MENA CAB Report
30
-
Upload
association-de-lutte-contre-le-sida -
Category
Healthcare
-
view
153 -
download
0
Transcript of MENA CAB Report


Community Participants
Hussein Zahid Sustainable Resource Foundation, Pakistan
Souhaila Ben Said Association Tunisienne de Lutte contre les MST et le
Sida,Tunisia
HebaWanis Egyptian Initiative for Personal Rights, Egypt
Khaled Omer Sudanese people living with HIV care association, Sudan
Fatiha Razik Association de protection contre le sida (APCS), Algeria
Mohamed Mazen Affiliation? Jordan
Fatimata Ball Secrétariat Exécutif National de Lutte contre le SIDA,
Mauritania
SanyKozman Middle East and North Africa network of harm reduction,
Egypt
Rita Wahab Soins Infirmiers et Développement Communautaire &
Vivre Positif, Lebanon
Mohammed Dadsi Association de lute contre le sida (ALCS), Morocco
Habachi Abderrahim Association de lute contre le sida (ALCS), Morocco
Zakaria Bahtout ITPC-MENA, Morocco
My Ahmed Douraidi Association de lute contre le sida (ALCS), Morocco
Othman Mellouk ITPC-MENA, Morocco
Pauline Londeix MENA-CAB Consultant
Amal Ben Moussa MENA-CAB Coordinator,Association de lute contre le
sida(ALCS), Morocco
First meeting of Middle East and North Africa
Community Advisory Board

Industries and organizations Participants
ViiV Healthcare Scott Purdon. Director Access and Government Affairs
Gudrun Maechler. Director Medical Affairs
Medicine Patent Pool Esteban Burrone. Head of Policy

Abbreviations
ABC: abacavir
ARV: Antiretroviral (class of drug)
CAB: Community Advisory Board
DTG: Dolutegravir
FDA: United States Food and Drug Administration
IP: intellectual property
NGO: nongovernmental organization
PLHIV: person or people living with HIV/AIDS
TRIPS: Trade related aspects of intellectual property rights (World Trade Organization)
WHO: World Health Organization
MPP Medicines Patent Pool
Background
Despite the fact that HIV prevalence in the countries of the Middle East and North Africa is
believed to be low at least among the General Population, the rate of increase of new cases
since 2001 makes this region home to one of the most fastest-growing epidemic in the World.
The annual number of new cases continues to increase in the MENA region unlike other
regions of the world, like in sub-Saharan Africa, where the number of new cases have been
significantly decreasing(34% decrease) or in the Caribbean region (49% decrease). In parallel,
MENA Region is reported to be the region with the lowest access to care and treatment in the
World (11%)
Pharmaceutical companies use the World Bank classification, which is based on the income
of countries, to define their access policy in the world. According to this classification the
majority of countries in the MENA region are considered as middle-income countries.
However, the United Nations Committee for Development Policy uses three criteria for
identifying countries as least developed countries: gross national income per capita, the
human asset index, and the economic vulnerability index. This results in a larger number of
poor people living in middle-income countries than in low-income countries.
Because pharmaceutical companies consider the countries in the MENA region as
intermediary countries, the price of their products are much more expensive than in low-
income countries. Another consequence is that the countries in the MENA region are
excluded from voluntary licenses, which means they can’t have access to generic drugs which
usually propose the same molecules, but for affordable prices compared with prices provided
by originators. Also the originators often use different strategies, like “evergreening”, abusing
their rights related to the intellectual propriety to block generic manufacturers for as long as
possible. As a result, the access to new generation ARVs in these countries stays limited.
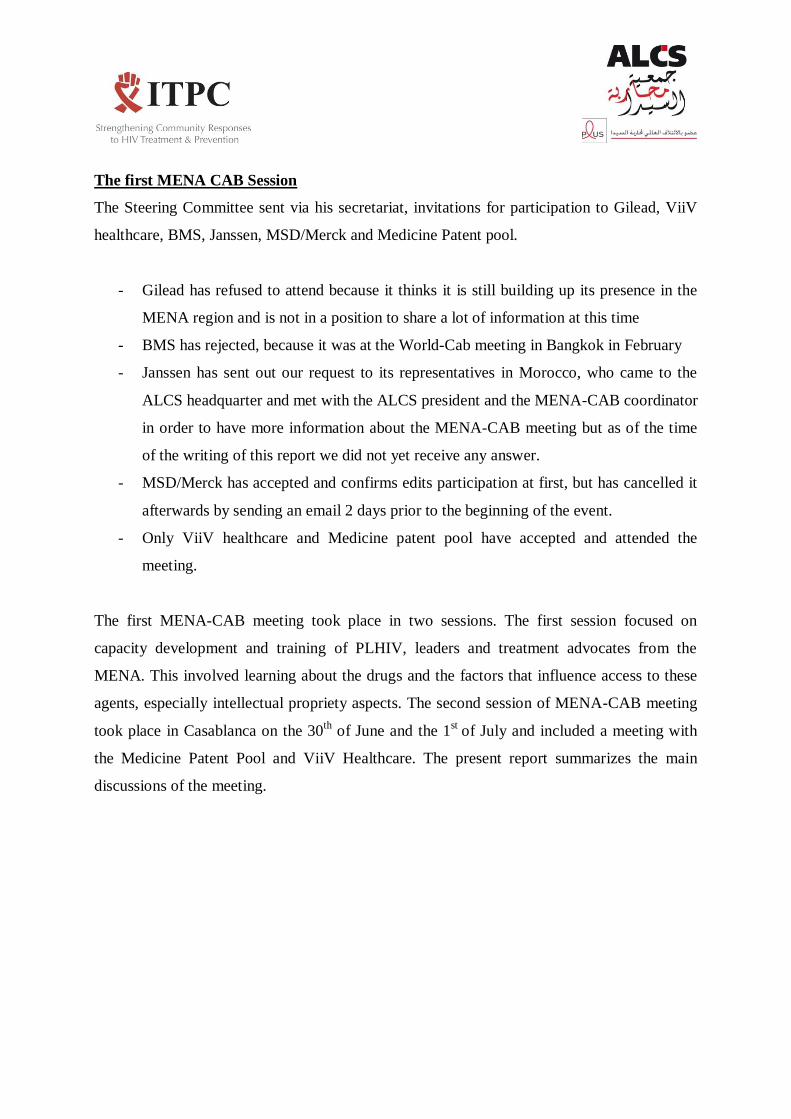
Actually the third-line treatment in these countries is too expensive. For example, in Morocco,
where there are 5500 people on treatment, the amount spent on the procurement of third-line
treatment for 20 people (at US$ 1700 per patient per month, or US$ 20 400 per patient per
year) is equivalent to the amount required for treating 1700 people on first-line medicines (at
US$ 240 per patient per year).

The Middle East and North Africa Community Advisory Board (MENA-CAB)
The creation in September 2013 of a Community Advisory Board for the first time in the
MENA region was a regional initiative of the Association de Lutte Contre le Sida (ALCS) in
Morocco in collaboration with ITPC-MENA.
The main objective of the MENA-CAB is to ensure a dialogue at the regional level among all
of people living with HIV and / or hepatitis C, treatment advocates, and representatives of the
pharmaceutical industry and policy makers in order to ensure improved access to treatment,
care, and support for patients. The MENA-CAB is managed by a Steering Committee
composed of 6 members from 5 different countries (Table 1)selected to reflect geographical
representation, sexual orientation and gender identity, knowledge, community credibility, and
honesty as much as possible.
This committee decides on the program and participants in meetings and activities of the
MENA-CAB while the legal and financial control is provided by ALCS.
Before the Steering Committee, an ad hoc Experts Committee was constituted ad hoc and was
temporary; its role was in agreeing the terms if reference for the full time elected Steering
Committee and preparing and agreeing the criteria for selection, process of invitation, self-
nomination process, timescales and process of acceptance of self-nomination of individuals to
be Steering Committee members. This was fully achieved by the Experts Committee which
was then terminated leaving the floor for the Steering Committee (SC).
The role of the Steering Committee is to:
Decide the work plan, in consultation with members
Agree the programme for CAB meetings
Approve participants to the meeting
Set and monitors the budget, in consultation with the secretariat
Seek funds, in consultation with the secretariat
Update the administrative and governance procedures for the CAB, in consultation with
the secretariat
Select a Chair and Deputy Chair for CAB from among Steering committee members
Appoint other voluntary officers as needed from among its number or the members.
Adjudicate on the participants to be invited to the CAB.
The first MENA CAB Session
The Steering Committee sent via his secretariat, invitations for participation to Gilead, ViiV
healthcare, BMS, Janssen, MSD/Merck and Medicine Patent pool.
- Gilead has refused to attend because it thinks it is still building up its presence in the
MENA region and is not in a position to share a lot of information at this time
- BMS has rejected, because it was at the World-Cab meeting in Bangkok in February
- Janssen has sent out our request to its representatives in Morocco, who came to the
ALCS headquarter and met with the ALCS president and the MENA-CAB coordinator
in order to have more information about the MENA-CAB meeting but as of the time
of the writing of this report we did not yet receive any answer.
- MSD/Merck has accepted and confirms edits participation at first, but has cancelled it
afterwards by sending an email 2 days prior to the beginning of the event.
- Only ViiV healthcare and Medicine patent pool have accepted and attended the
meeting.
The first MENA-CAB meeting took place in two sessions. The first session focused on
capacity development and training of PLHIV, leaders and treatment advocates from the
MENA. This involved learning about the drugs and the factors that influence access to these
agents, especially intellectual propriety aspects. The second session of MENA-CAB meeting
took place in Casablanca on the 30th
of June and the 1st
of July and included a meeting with
the Medicine Patent Pool and ViiV Healthcare. The present report summarizes the main
discussions of the meeting.

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
COUNTRY N° people
with HIV
Atazanavir
TDF COBI EVG, QUAD
Abacabir Dolutegravir Abacabir pediatric
Dolutegravir pediatric
Pakistan 87000
Morocco 30000
Yemen 19000
Mauritania 10000
Egypt 6500 Royalties Royalties
Tunisia 2300
Algeria N/A
Jordan N/A
Lebanon N/A
Libya N/A
Palestine (west bank &Gaza)
N/A
Sudan N/A
Syrian Rep N/A
Licenses of Atazanvir, TDF, COBI, EVG & QUAD, Abacavir,
Dolutegravir, Abacabir pediatric and Dolutegravir pediatric in countries of the MENA region

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
AGENDA OF THE MEETING
June 28th 2014 - Day 1
8h30-09h00 - Welcome and Logistic issues
9h00-10h00 - Opening session of the MENA-CAB meeting
- Welcome speech to the MENA-CAB
- Participants introduction: Situation in each country
- MENA-CAB creation, Principles of the CAB, Agenda
10h15-11:45- Session 1
- Course of the drug from the discovery of a molecule to its placing on the market and Propriety
intellectual issues
- General Discussion
BREAK (15mn)
12H00- 13H30- Session 2
- Discussion on HIV & HCV pipelines. Which therapeutic priorities for people affected with HIV &
HCV in the MENA region?
- Pharmaceutical companies pipelines presentation. Focus on HIV & HCV medicines patented by
ViiV Healthcare & Merck
- Discussion on the current main or specific identified needs by the participants in each country of the
MENA region
BREAK 45 mn
14h15-15h45 - Session 3
- HIV & HCV treatments, what commercial strategies for pharmaceutical companies?
- Main strategies from pharmaceutical companies for their HIV & HCV medicines (standardized
prices, tiered pricing, voluntary licencing, and merger and acquisition)
- Discussion: what consequences of these strategies for the access to HIV & HCV treatments in
MENA region countries?
15h45-16h00 Day 1 closing session & logistic issues

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
June 29th 2014 - Day 2
9h00-11h00 - Session 4
- Using TRIPS flexibilities in MENA countries, as a strategy to stimulate competition & to
improve the access to treatments
- Focus & discussions on TRIPS flexibilities and to oppose patents in MENA.
BREAK (15mn)
11h15-13h15- Session 5&6
- Patent landscape in the MENA region
- Voluntary mechanisms, including the Medicines Patent Pool, and the access to medicines in MENA
- Group work: Best strategies for access in some countries
BREAK (45mn)
14:00-16:00 - Session 7
- General presentation and focus on the Medicines Patent Pool & the MENA region
- Specific discussion for the meeting with the Medicines Patent Pool
15h45-16h00 Day 2 closing session

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
June 29th 2014 - Day 3
8h30-9h00 - Final discussions before the meeting with the Medicines Patent Pool
9h0-11h00- Meeting with the Medicines Patent Pool (MPP)
- Presentation from the Medicines Patent Pool
- Questions, comments &discussion
BREAK (15mn)
- Plenary debriefing of the meeting with the Medicines Patent Pool ; Lessons learned & next
steps
12:15-13h- Session 8
- The generic industry in the MENA region
- The generic industry in India
- Specific discussion on the issue of registration of medicines in each country. Strategy of the
pharmaceutical companies to block generics
BREAK (45mn)
14:15-16:00 – session 9
- General capacity building session for the meeting with ViiV Healthcare
- Discussion

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
July 1st 2014 - Day 4
9h-11h Capacity building session for the meeting with ViiV Healthcare
BREAK (15mn)
11h15-13h15- Meeting with ViiV Healthcare
- Presentation from ViiV Healthcare
- Questions & discussion
BREAK (45mn)
- 14h- 16h: Debriefing of the CAB
Day 4 closing of the MENA-CAB

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
Minutes of the meeting
1. Fatiha: During a negotiation with pharmaceutical companies, based on which criteria do you
decide the geographical scope of the license?
A license is a piece of paper, what you actually want is an impact to make sure that these
medications are available and accessible throughout the country.
We start from the basis of what is a company doing right now, what is their current policy?
We try to push the limit, with a country that would not normally be able to buy the generic.
The negotiation takes a long time for this reason; this is why it takes a couple of years
because we are working very hard to get all of the conditions that benefit the country that
these other companies cannot do. When we reach the moment when we know that is as
much as we can get, then we agree on the negotiation – we want it to be a significant
improvement over the status quo including certain conditions that would not otherwise be
available.
2. Heba: Are governments involved in the negotiation process? If yes, how? If not, why?
I have to be very frank and open with, we’ve never done this before, a patent pool of this
kind does not exist in any other field. About a year and a half ago we started interacting with
the governments that we wanted to work with, meetings and phone calls. The first thing that
we need to do is connect data, we have to make a solid case using current information about
1st line, 2nd line and the epidemic in the country. You will make the moral case, the access to
treatment case but often you also need to include the data in order to solidify your
argument. The second step is to try and see if they need that drug and how we can interact
very closely in order to bring the license to fruition. What we want is to convince the
companies that you want access to this drug and to this generic for the lower price. We’ve
been doing this a lot lately, especially with Atazanavir and it was disappointing. The reply we
are getting is that the drug is not registered there so how can they be procuring this drug? In
most countries if the originator company has not registered the product it becomes very
difficult for generics to produce the product. This should be an easy win because the
company is making zero money in this country, because they’re not selling the product. But
the governments are telling us that it’s difficult and they aren’t getting to it right now.
Dolutegravir is also not being sold because it is so new and people don’t know if it will work.
What we’re trying to say is we want to get them in now. We were trying to see how we can
get the Ministry of Health interested in moving.
A license can be amended as many times as the parties agree. We don’t want the companies
to say that you’re putting pressure on the countries to do this.
Meeting with Medicine patent pool

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
3. ZAKARIA: Given the scope of your licenses, it appears clearly that you are failing to include
MENA countries, why?
I’ll give an example with Dolutegravir. We managed to get Egypt, we couldn’t get Morocco or
Algeria. ViiV says that actually they have a strategy to make this product available in Morocco
and Algeria. There are commercial countries, where they expect to make a profit. So we push
and push in order to bring it here. ViiV originally had 67 countries benefiting and we got to a
stage where 120 countries could benefit. So do we drop this because of your region and not
allow all of these other countries to benefit? I wouldn’t call it a failure, it’s one of the biggest
challenges we have. We are going to be able to help some people and I think something is
better than nothing.
4. Douraidi: The main part of the work of the Patent Pool is based on negotiations. We know
that to negotiate you need to have leverage. What are your means to pressure
pharmaceutical companies during the negotiation process in order to accept your
conditions?
They have also been granted by the countries an exclusive right, which makes it difficult.
What do we have as pressure points? Not enough to be honest. There is strong pressure
from the government, social society and the global fund finance to do more. The royalties do
something but that is essentially it. In HIV there is a lot of pressure on the companies to try
and do more. We have to show them, we have to make a case for them in order to convince
them to do more.
5. Med Dadsi: What is the place of people living with HIV in the governance of the Patent Pool?
So we have people living with HIV in our governance structure, one of our board and three
people living with HIV in our expert advisory group (3/11). There is no person from the MENA
region right now and I think we should include someone. We have people from Kenya, from
Bolivia, from South Africa that are in our governance structures right now. I think even
beyond this we need to do a lot with communication.
6. Zahid: Do you think that you are adequately consulting with civil society?
Originally we were consulting more with the international groups, which was our key access
to civil society. We realized over time that we needed to talk to people more at the national
level of these countries in order to provide a better forum for communication and discussion
between people. There is lots of work to be done. What we are doing is discussing a lot with
civil society during the negotiation process but we cannot go public during that process.
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
7. Fatimata: In your media statements, you are claiming that thanks to the Patent Pool,
Subsaharan countries, including my country Mauritania, have access to treatments. How do
you make sure that these drugs are effectively available in my country and when?
The challenge we have is the following, when we are discussing with a pharmaceutical
company, we try to tell them low and middle income countries. Sometimes they say
Subsaharan Africa and sometimes they don’t include all of the countries. So far we haven’t
had much trouble with Mauritania. Our focus is countries with a higher disease burden and a
lower income. We have been going to every regional conference, international conference
and every CAB that I can go to in order to have these conversations. We are not doing
enough but gradually we are trying to do more and the licenses are getting better and better.
It’s still not enough and the mechanism, as it is a voluntary mechanism, is making it very
difficult for this to happen.
We have to be humble about what we do. We’re an organization of 14 people and we’re
trying to address hundreds of thousands of people. If the drug has a patent, it will be very
expensive, if there is no patent but a license, the generic country tries to come in and tender
the license. We have to be careful what we do as we are not the Global Fund or any other
giant international company. To the extent that there is a patent barrier, we are trying to
remove that barrier but there is an immense process we must work through to achieve this
goal.
8. Fatimata: Concretely, when are we going to access these medicines and at what price? As for
Tenofovir, it existed in Mauritania before your license, so nothing has changed. My husband
just died, 255 days ago, from lack of availability of 3rd line treatment. When are we going to
access Dolutgravir in Mauritania? And when will it be available in other MENA countries so
that what happened to him does not happen to others?
For the moment the products for the 3rd line are in negotiation with the other countries.
Perhaps in your region the access is not licensed for Dolutegravir. There is a lot of interest in
the generic form of Dolutegravir but there is the issue of time to put it on the market.
Without the license from the originators, it is difficult for the generic brands to commence
producing the product. We would think that the time would take between two and half to
three years. Sadly, it is the time that rests as the problem.
9. Othman: In Johannesburg, November 2012, you committed to disclosedata regarding the
impact of your Gilead license. Could you share this data with us?
For the patent in 2006 for Tenofovir, 106 countries that are in the process of buying the
access to these medications. The license is in the process of existing in 75 or 80 countries and
we working with our partners to try and bring this many other countries. Right now, we are
negotiating with our partners to bring these to about 140 countries.

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
The updated data is still in the process of being recorded and documented and we have true
data on this for very few countries.
10. Heba: (So) how do you measure your impact? Do you see yourself as a successful initiative?
Our generic licenses starting producing Tenofovir and many of them already had it. They are
producing it in more countries and don’t have to pay royalties there. We took the countries
with data, very few above the 95 and we are looking at the prices in these countries actually
paid, in some countries they bought from the originator and from others they bought them
from Cipla. The countries got the licenses in 2012 and started registering, which takes time.
The impact is now low but it is starting to go up, trimester by trimester. There are savings on
royalties for those countries. The Dolutegravir impact probably won’t come for three years.
The impact estimation is based on certain assumptions, until the end of the patent. I will
focus on making the drugs available sooner, better terms with the companies and putting
pressure on these companies.
11. Sany: Who sets the price of generic products developed through your licenses? How can we
be sure that the products will be actually significantly cheaper and affordable and thus
increase access? For instance, could you intervene if you realize that the prices are still too
high and not affordable to countries?
We don’t decide price. Every time they tried to decide a price it was wrong. It went down
with the market and the generic competition. When there is a patent that doesn’t allow that
to happen, we try to remove that barrier and to allow that competition to happen to give a
better price. If we start fixing the price, that’s not going to give you a good price. If I put a
ceiling price, they’ll all charge up to that price. The ceiling price is the originator price
because that price is already available in the market. So if the generics want to sell they have
to sell cheaper than that. Fortunately, the market price competition has brought the ARV
price down significantly.
A tiered pricing approach allows the originator price to be lowered very much and allows the
competition between the generic brands. When competition happens, the generic price goes
down but the originator prices stay the same, that is to say the price in the US stays the
same. That is why we want differentiated pricing structure, to increase the competition and
lower the overall prices.
12. Abderrahim: Actually, all that you have been doing is supposed to be on our behalf, people
living with HIV, our countries! Who gave you the mandate to speak on our behalf?
This is the message we’d like you to bring back to your company, we know that we do not
have time to answer this right now.
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
13. Sany: If excluded countries want to issue a compulsory license, will you publicly support
these countries? For example, Egypt is one of the rare MENA countries who want access to
Atazanavir because a patent has been granted. If Egypt decides to issue a compulsory license,
will the MPP publicly support us?
14. Rita: I am from Lebanon. I don’t see any difference between my country and other MENA
countries that are included in your license in terms of income or epidemiology. Could you
explain to me the rationale behind our exclusion? Furthermore, with flows of refugees from
Palestine and now Syria, the situation is even worse.
For some of the licenses it is included but for some others there is no patent for Lebanon so
Lebanon would be able to buy from the generic. Because the companies allow the countries
with no patent to buy the product generically, Lebanon can do this. That is the information
that we have (referring to the orange and green slides). In terms of having those for us, my
understanding is that Dolutegravir is a product that is very exciting in terms of its
characteristics, little side-effects and only 50 mg.
The key point is whether or not Lebanon will be able to benefit from the products.
15. Rita: Otherwise, I am really shocked to see that a country such as Palestine, which relies
100% on the international aid, is excluded from your licenses. Do you or your partner
companies consider that the government has the ability to pay?
I’ve looked at the data for West Bank and Palestine and often they are paying the highest
amount for generics and other drugs. I think that this has a lot to do with how the drugs are
transported to them. I don’t think that we are necessarily the right company to talk to about
this. As the MPP we would like to work to figure out how we can help and fix the prices that
they are playing.
16. Mohamed: Just like Rita, I have been really surprised to see that Jordan is the only country
excluded from the pediatric Abacavir license, knowing that we only have a few children on
treatments. Frankly, I can understand that a company defends its commercial interests in a
country. Do you really think that 20 children in Jordan represent a strategic market for ViiV?
I apologize that is my mistake here. I’ll re-look at the slides and send you the slides with the
right data. I couldn’t imagine a country that is only 20 children. We just announced that we
are expanding the countries that are including Abacavir in pediatrics.
17. Fatimata: Excuse me, before M. Burroneanswers; I am really concerned about the
knowledge of people who are negotiating on behalf of our region. M. Burrone, would you be
able to locate Jordan on a map?
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
In the negotiation, we try to get all the low and middle income countries in. That is the
starting point. Then the company will tell us which country that we can include. We tried to
get Jordan included, that is a given. Is it a commercial market? I can’t believe that any of
these countries are really a commercial market. You should discuss with ViiV about the
specific reasons for this. I really don’t believe that pediatric HIV is a commercial market
anyway. A lot of what they do is really about the precedent; they are trying to set a
precedent.
18. Zahid: I am from Pakistan and personally, I am getting more and more confused. Looking at
your licenses, I don’t understand if I am living in a poor country, in a rich country or in a
middle income country. Is Pakistan a high prevalence country or a low prevalence country?
As sometimes I am in the country and sometimes I am not, I would be grateful if you could
help me out in my ignorance.
Pakistan was in the first license and out of the second license and in the third and out of the
fourth. Sometimes they are included and sometimes they are excluded. The key challenge is
we will try to say to a company, this is who you have included now, and push them to include
Pakistan. But it is a voluntary process so it is ultimately up to the company. Pakistan is
fortunately a country that we have been able to include in most of our licenses, and if it is
not included there are provisions that allow it to buy from generic brands. We are faced with
countries that are increasingly starting to see these countries as commercial markets. That’s
what we’re facing and we’re trying to push back.
19. Zakaria: I am from Morocco and I can understand that Morocco is less poor than Yemen,
Mauritania and Sudan, however, just like Rita, Mohamed and Zahid I am lost. Could you
explain how our countries are considered poor enough to access Abacavir and not poor
enough to access Dolutegravir? Can you explain why Egypt can only access Dolutegravir and
why we Moroccans, Algerians, Tunisians, Lebanese, Jordanians, etc. are excluded? What
does Egypt have different from us apart from the pyramids?
The license for Abacavir is a pediatric license, which means that it is easier to include more
countries in this license. This is not seen as a commercial license as the adult products are.
On the other hand, this is not finished. A license can been modified many times, just because
it is signed does not mean that it is finished. It can be modified in 2 or 3 years. Right now, the
license is publically published and people can reference them and demand why are we not
included? Additionally, a country can demand this and question what is in the license in
order to make the enterprise move and adjust.
20. Heba: What are the Medicines Patent Pool criteria for determining whether a country is
paying royalties or not? For countries that are paying royalties; how did you decide on the
tier? What makes you say that it’s acceptable this way?
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
For countries in low income status like those in Subsaharan Africa, there are no royalties; we
do not take royalties there. There are 67 countries where there are no royalties and there
are many countries where there is no patent outside of those 67. So then you’re left with a
list of about 15 countries, maybe more, where there are patents. So the challenge was to
convince ViiV to include these countries in the patent. ViiV was saying that their board only
allows those 67 countries in their patent. So then they were saying what can we use as
features to try and get these new countries in. There are two things we can do, the first one
is market fragmentation. We would like to be able to get more data on this. We were saying
that at the very least allow the generic brands to be in the public sector. We also proposed
royalties based on the level of disease. So they said we could have six additional countries
with adjusted royalties and it was very necessary that we convinced them of the success of
this. In the end we settled for the income approach linked with GDP level. The original would
be available for about 400 dollars; the generic brand around 100 dollars and then that will go
down with competition. In these six additional countries, the royalties will only be payable if
the patent is granted.
21. Heba: What do you do with companies with whom you don’t reach an agreement? Do you
denounce them publicly?
No, publically we would never denounce a company that we do not reach an agreement
with. In order to manage this, we use complementary strategies in order to continue to urge
the companies. We cite publically the companies that we work with and those that we do
not work with. We write to every company to negotiate with. If they do not negotiate with
us, we will state that we do not have a license with them.
22. Fathia: During the negotiations, do you have any redlines you can’t go beyond that
determine what is acceptable for your or not? Can you share this?
All of the licenses that we have right now came from negotiations that we’ve had with these
companies. We push the companies to the maximum point in order to obtain everything that
we can for these countries. If there are royalties made at the base of the patents, we work to
lower those as much as we can. After discussing with different companies, there are many
different ways to negotiate this. There are certain things that are absolutely essential to
contain in the negotiations and those are what we are working on right now. The generics
should be able to challenge the patents; there shouldn’t be any no-challenge clauses in the
licenses.
23. Douraidi: Given what has been said, it appears clearly that the Patent Pool is failing to
address the issue of access in MENA and middle income countries more generally, and that
the few results that have been achieved are limited to the least developed countries, which
by the way don’t need a Medicine Patent Pool and can simply use the transition period to
implement TRIPS.
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
Looking at your slide, it appears clearly that the issue of patents is concentrated in the
middle income countries and until now, you haven’t done anything for most of these
countries. Between us, isn’t that a statement of failure?
I fully share that opinion. About 75% of countries that we are working with concerning
licensing products regarding HIV are voluntary licenses. However, it is necessary that we
work and push the laboratories to commit to our negotiations and give more voluntary
licenses.
24. Sany: We have been hearing that the Patent Pool is considering extending its mandate to
Hepatitis C. Is that true? In Egypt, we have been working closely with the government, on
invalidating the patent and on developing the local production. We really would not like to
see the MPP jumping with a voluntary license which we believe won’t bring the needed
competition leading to significant decrease of prices and increasing access.
For the moment we only have the mandate to work with HIV. We have been asked by
UNITAID to explore the options and what we could do with Hepatitis C. This is interesting
what you are asking me. No country is worse because of a patent license, and I want to make
that point very strongly. I don’t think that there is patent in Jordan for Abacavir, going back
to that, we can recertify the data to make sure. With Hepatitis C, we are in a phase where
there is a lot happening. From the MPP perspective, some people think it would be great and
other think it would be the worst thing. Right now we won’t do Hepatitis C unless there is a
full feasibility study that shows us that it would be a successful process.
25. Khaled: I am from Sudan. Even if my country has been included in the previous licenses, I feel
in solidarity with my colleagues. Given all of what has been said, can you tell us how you are
planning to deal with the MENA region in the future?
There is no license right now. Because there no patent in India, generics can produce in India
and sell at a cheaper price. We are trying to expand this to other countries to ensure the
availability of the drugs in other countries. That’s the context in which we’re trying to get as
many countries in the MENA region included. I think it would be great if we can consider
strategies to tell these companies that these generics are important and that they need to be
able to be sold.
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
1. Khammas: So far, Abacavir has been used very little in our region because of the fear of
prescribers of hypersensibility reaction. Question in two parts: Do you have studies/data on
the frequency of such mutation in the MENA region? Or in any other resource limited
country? As part of your promotion for access to Abacavir, what efforts do you do to make
the hypersensibility test available?
We work with diagnostic companies so we make sure that HLA testing is available on request
by physicians. The test is an expensive test but we are very interested in working with
countries that are interested in launching the product and make in available for those who
need it. Regarding the affordability, for example, in Kenya the HLA test is not available right
now in the public sector due to cost issues. So the patient that would go on this testing is
outside of the public sector. At the moment the countries I have information on are Saudi
Arabia and Turkey because they are very interested in the product so we are working to
make it available to them. Our commitment is when we launch the product in the country,
the test is available. The testing still needs to be carefully monitored.
2. Khammas: WHO just added ABC as a potential interesting 1st line for pediatric use. Do you
have any data on the risks of reaction to hypersensibility for children? Is the hypersensibility
test compulsory/recommended before the treatment initiation? And if so, how do we make
it available in resource-limited countries, especially as the demand is going to increase
following to the new guidelines?
As a company, we recommend the use of the test but in reality the governments decided
where to use the test. The patient can decide not to pay for the test and instead immediately
start treatment but we recommend the initial testing of the patient before treatment is
given. This is then the decision of the prescribing physician and the government.
Commercially, the test is recommended for children under 10 years of age and there is an
increasing demand for the drug. The rate of HSR in children and pediatrics is very low, not
nearly the same as adults. My information is that there is no request from the WHO to
supply children with the drugs. Thus commercially they do not specifically supply pediatric
drugs but they include an enormous amount of information. This excess of information will
give you some comfort as a clinician It is recognized very quickly. Where it is commercial, we
Meeting with ViiV healthcare
ARVs: Production & Pipeline

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
are very committed to working with the governments to ensure that everything goes well, by
setting up reference labs and working very closely with the government. We signed an
agreement with Clinton Health and Mylan Pharmaceuticals. . Abacavir is and will be a very
good drug for pediatric use, it is very dispersable and taste masked. In 2013, Abacavir was for
ten year olds, we knew that other medications were toxic for children. We used Abacavir 3TC
30 mg and 60 mg, we made it fully dispersable and we taste masked it. The last few months
we have been working in partnership with them in order to ensure the highest quality of this
pediatric drug. Mylan filed a pre-qualification with WHO last year and we are in the process
of answering their questions now. There is not a lack of commitment and we aim to make
this drug affordable.
3. Othman: Could you explain to us what is the therapeutic value added of Maraviroc for
patient in virological treatment failure in comparison to competitor products such as
Raltegravir or Darunavir? How do you analyze the fact that you do not have the same
commercial success with Maraviroc than Merck and Janssen and Raltegravir and Darunavir?
There is one observational study that saw an increase in cardiovascular events. It was an
observational study where all the confounding factors were not taken into consideration.
The other risk factors were not accounted for. Because of this, we and the FDA took this very
seriously and looked to see if we had a signal in our clinical trial. We assessed the signal of
cardiovascular side effects in our clinical trials. The analysis done by the FDA concluded that
there were no identifiable risk factors that affected the cardiovascular system. Several
international guidelines changed the importance of Caivexor for the initiation of ARV
therapy.
4. Othman: At what stage are the clinical trials for Drug 744, including on the “long action”
form (1 injection per month)? Will it be more for treatment? Or prep?
For this we work in partnership with other companies. The trials will start soon and this is
very early for a study this small. The study includes young women in particular there is an
epidemic for young women in Africa plus prevention development. The study is not
technically in our hands, we have passed on the study to our partner at the clinical site in
South Africa. There is only one drug in the prevention study that is not shared in the
partnership.
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
5. Zahid: In which countries have you registered your product? As for the countries where you
have not registered your product, what are the reasons for this?
We as a company are committed to submit the dossier in every country of the world,
everywhere. The main countries in North Africa need European approval (was approved in
January of this year) and these will be submitted in three waves as we do not have the
capacity to do it all at once. What we committed with DTG is to bring to all countries with a
regulatory authority. We have committed to filing these dossiers in March, June and
September of 2014. DTG needs to be registered in all countries with a regulatory body in
order for the patent to be successful. The other countries we hope to register in North Africa
include Algeria, Egypt, Jordan, Lebanon, Mauritania, Morocco, Tunisia and Pakistan. We are
having trouble with the regulatory capacity in Palestine, Sudan and South Sudan. I have
information that I am not comfortable sharing, but there are three countries where the
dossiers have already been filed. We cannot share a more precise list at the moment of the
countries we have already registered in and those that are in the process due to legal issues.
I would rather come back with a full list concerning the countries and DTG as well as ABC.
6. Souhaila: A few months ago, you met with the Ministry of Health of several countries in the
Maghreb (in Morocco at the end of 2013). What was the purpose of these visits? Is there any
link with the registration/marketing of DTG and pediatric ABC? What has come of these
meetings?
We came to Morocco over a year ago and participated in a series of informal meetings to
discuss the clinical trial as well as how to make the drug accessible to MENA countries. The
HLA trial is already ongoing in Morocco in comparison with everywhere else in North Africa,
where it is new. We have colleagues that are fully dedicated to this region that spend time
visiting mainly physicians to understand what they need. We felt that the Moroccan
government had a strong interest in the drug DTG. Overall I was really impressed by this
country to make antiretroviral medications available.
7. Fatiha: In some countries, you have filed patent applications. Do you systematically register
in countries where you file patent applications? As you know, because a patent exists, this
can prevent the appearance of a generic brand on the market. We find it unacceptable to
block a generic brand when the patented medication is not accessible!
Registration

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
We need to first complete our clinical trials in order to demonstrate that DTG is as safe as
current drugs used. There is no direct link between whether the drug is registered and or
whether it has a patent thus we have committed to registering the drug everywhere. For
example, Algeria was one of the first countries that we registered in.
8. Fatimata: What will your marketing strategy for DTG be in resource limited countries,
including those from the MENA region? Will you position DTG as a first line to compete with
Tenofovir-based 1st lines (as you do in rich countries), which would imply a considerable
effort on prices (as the TDF-based regiment is off-patent), or will you rather place DTG as a
part of 2nd and 3rd line regiments?
The way in which the drugs are positioned depends on where drugs are approved and which
indications we get. In Europe and North America we have indications with both the naïve and
experienced groups. Commercially, one aims to sell to those markets or those indications
where there is a need for the drug, whether naïve or experienced. The drugs that are
restricted to 2nd and 3rd line regiments are often those that are more expensive and difficult
to make. Very often that is because of the volumes of those drugs, they are produced at such
low volumes. DTG is 50 mg and my expectation is that the price will be affordable in naïve
and experienced groups. For example, we hope to communicate an access price in Kenya in
the next month or so. The pricing of these drugs depends on the specific country taking into
account the international region (Latin America, North Africa, Europe and Asia Pacific), the
size of the country, GDP and GNI, the size of the epidemic. We need to price our products at
a competitive level; if not there is no sense in producing them.

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
9. Fatimata: In the countries covered by the MPP licenses (Egypt, Yemen, Mauritania and
Sudan), who is going to register? Will ViiV do it or will the generic producers have to do it?
Will you work with the generic producer to make sure that the product will be effectively
registered?
We will register in all countries to enable the generic companies to cross reference our files. I
don’t know the current registration status in this part of the world but I will come back to
this. But the goal to have this dossier registered in all countries where this is possible. We are
working to make the available in one year as the average availability is seven to ten years.
10. Othman: In countries where you don’t have any patent, will you use data exclusivity to
prevent the registration of the generic version?
In the past companies have been slow to register with no sales and no pressure to register.
What we are saying is that we want to register this in every single country in this room that
has never been done before. We only got FDA approval in October of last year and the day
we did that we signed a voluntary license with Orabindel. Additionally, we only got European
Union approval in January of this year, and here we are putting dossiers in countries only 5
months later. The company is fully committed to registering DTG in every country.
The dossier has such a robust data package and file that we barely have any questions on the
regulatory authority so the approval is coming faster in these countries. We are trying to
make it as efficient as we can.
11. Souhaila: What are the countries where you have filed/granted patents vis-à-vis DTG,
specifically Tunisia?
Any country with a patent is linked with ViiV healthcare. Given the license, we will compete
globally in patented and non-patented countries. With generic companies and tiered
structures we will carry out the same policy. We are not going to walk away from this
commitment; we are committed to the supply of these products at a competitive price.
Ultimately, this will help medically and reputationally for ViiV healthcare.
12. Abdelrahim: What is your patent policy in MENA? Will you file patents everywhere or only in
several countries? What will be your criteria?
Patents & Intellectual Property

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
You would expect a pharmaceutical company to patent everywhere but they do not. I don’t
know the reason why this is not true but I can try to find out and get back to you with a
concrete answer. I know that it has to do with intellectual property rights. My guess is that
whoever made the decision probably thought that HIV wasn’t a problem in this region and
decided commercially they couldn’t make much revenue.
13. Mohamed: Looking at the patent landscape, we have noticed that you use a lot of
evergreening practice: patents on the original compound, the hemisulfate salt, the pediatric
use and on various combinations with older drugs. This process only aims to extend your
monopoly in order to delay legitimate generic competition. Don’t you find it immoral in
resource-limited countries such as ours?
There is a difference in the way that ViiV is trying to operate. From the perspective of the
company, the patent is valid. The morality of multiple combinations of the drug is much
more specific and individual to each brand and not contained in the patent that ViiV
healthcare holds.
14. Zakaria: If an excluded country from your DTG license (i.e. Morocco or Algeria) issues a
compulsory license, how would you react? Will you pressure the country or respect the right
of this country to use the TRIPS flexibilities?
Any country with a patent and grants a compulsory license is discussed on a case-by-case
basis. There are some good examples; Indonesia issued a compulsory license with Tenoflevir
as a political message. We would need to discuss the reasons for giving Morocco a
compulsory license. With the Ministry of Health we would need to discuss the effect of DTG
on the country and what we can do about it. It is a difficult position for countries with
unstable relationships linked with their governing bodies. Even if the country expresses
extreme interest in the drug, the government could have no intention of following through
and supporting access to the drug. My experience is that we would also discuss with CAB or
ITCP in order to better ensure the support of the drug. If we disagree with access policies, we
may take action with the country but again, that is decided on a country-by-country basis.
There have been three or four countries where compulsory license have been issued,
included Brazil and Indonesia. TRIPS flexibility says that if you do compulsory licenses you
need to negotiate, each country can set the price of the drugs and whether if they are set on
the market or not.
15. Mohamed: Linked with question 14, we heard that two years ago you sued PWHIV in Ukraine
(all Ukrainian networks of PLWHIV for introducing a generic version of Abacavir and
breaching your intellectual property rights)? If we do the same, are you going to sue us?
My personal view is that will not happen with ViiV healthcare. There must have been a clear
problem in Ukraine. It is highly unlikely that we would launch litigation for pediatric
medicines.

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
16. Regarding the presentation, can you go back to the criteria for the access strategy?
You’re asking us to give you the criteria that we are currently defining. I can’t share those
with you specifically right now as they are still being finalized. In general it will be based on
the GDP, GNI (humanitarian index), and size of the epidemic, size of the country and the
income level of the country. There are some missing factors and that is why there is a gap in
pricing in your region which we are trying to work out right now.
17. Othman: Patent pool license: Why did you negotiate two different licenses on ABC (with the
MPP)? One is wider with respect to pediatrics and the other more limited for adults? Outside
of the patent pool licenses, are you considering signing parallel voluntary licenses with the
generic producers (outside the MPP)?
The voluntary licensing policy has been in place for 13 years. MPP is very important as well,
they signed an agreement to accelerate the accessibility of DTG. The policy now exists so that
we will not seek to sign any voluntary license outside the patent pool. Additional licenses will
destroy the value of the patent pool and we are very adamant that this does not happen.
There will be an announcement of two or three other licenses but no others outside of those.
We signed an agreement with Orabindel giving them commercial license, meaning that it will
probably be one of the first companies with the drug on the market.
18. Sany: How do you explain that Gilead, the first firm who made the highest profits on HIV,
covers 112 countries with licenses while you only cover 73 countries?
For us, it is not solely the number of countries but the coverage. ViiV covers almost the same
area as Gilead but we are trying to get away from listing the number of countries and gear
towards coverage. Just because a country does not have a license does not mean that it has
denied access. The two should not be compared as Gilead is a totally different operating
model that takes royalties.
19. Heba: On what criteria have you decided on the included and excluded countries for these
licenses? Could you explain to us why a country such as Egypt who has the same level of
income as Morocco, Algeria or Tunisia is included and not the others?
When the voluntary licensing was created in 2001 they focused on developing countries.
These definitions were given by the World Bank and the UN not just based on geography and
boundaries but by also including low income countries. When we managed to get into the
MPP we added six additional countries that we thought that we could seriously make an
impact in. This depends on a vast array of conditions. How do you generate commercial
revenue as well as increase the availability of the drug?
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
This is the big question in the public health sphere. We don’t include some of these countries
because it is faster as ViiV healthcare. We only charge a royalty where the patent is approved
or granted, Egypt is the exception. The size of the epidemic in Egypt is large but with no good
commercial presence in the country, working with the patent pool in Egypt could be very
successful. We wanted to see the impact in Egypt so that is why it is included. We cannot
include some of the countries because of certain regions of the world, such as the case with
Ukraine and Russia. Directed by my legal colleagues, I am not allowed to disclose patent
information or my head will be on the block as that would be a breach of my employee
contract.
20. Mohamed: We are surprised to see that on the pediatric licenses the only country excluded
from the MENA region for Abacavir is Jordan, and for Dolutegravir, Jordan and Libya. How do
you explain these exclusions?
We will take this message back with us. That seems to be an oversight. The impact of
reference pricing leads to the exclusion of certain countries such as Mexico or Russia but I
agree, the exclusion of Jordan makes no sense.
21. Rita: Given the socio-economical and political context, we are shocked that a country such as
Palestine is excluded from your licenses. Furthermore, this country mostly relies on the
international aid and the number of PLWHIV is weak in this country. Could you explain to us
why this is?
In terms of patents and company policy, we are not here as a commercial wall that is not
listening to you. Which country cannot pay the price that we have negotiated? If you can give
me definite details I can take that straight to the CEO. I understand what you are saying that
there is no government in Lebanon to sign or help so if you can write to me and help me
understand who to provide the drugs to and the other additional barriers to access that
would be extremely useful. I need to hear that there are problems in Lebanon with influx and
refugees to fill in the blanks about what/who/where/how we can help concerning these
drugs.
22. Douraidi: For countries excluded from the licenses, what is your price policy? What are the
criteria to define prices? Will there be a unique price for all countries of the region, or will
the prices differ in each country?
This is information they are currently finalizing and defining more specifically to explain the
parameters by which a country prices a product. In general, we look at GDP, GNI, governing
bodies, the size of the country, the size of the epidemic and other competitive drugs. The
price is set by the market and by the countries, is it a national tender? It all depends on the
specifics of the country. We want to act as a transparent mechanism on the way in which
things are priced the way they are.
Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
23. Douraidi: Could you please define the “country commitment”?
We are not pricing by region but by country. There are private sector prices, public sector
prices and NGO prices. There are certain challenges with each country that need to be sorted
out. We are trying to work with the civil society and government of each country to have
differential pricing strategy. This has not yet been finalized but when it is, the information
will be available to you.
24. M. Dadsi: Now that the price of Dolutegravir is public in the UK and in the US (between
10,000 and 14,000 dollars paid per year in the US), what will the price of DTG be in MENA
countries?
Wholesale prices are what you would normally find in North America. The way companies
tend to work is they generate commercial income from North America or Europe then North
Africa and South America. After that, the region with the lowest pricing in the lowest income
regions. Thus in this area, the price will be between the lowest price in Africa and the highest
price in North America, and from my perspective it will be at the lower end. The UK is coming
in at a price that is the same as the previous products and the price will ultimately be set by
the governments but it still needs to be affordable. I have no price answer now but with
registration coming in the next few months we will see a scale of pricing. We will not price
highly as we are working to establish a balance between commercial and public access. I
cannot comment on the prices of these countries yet without the approval of the
governments in the countries. Morocco will probably have a higher price than Kenya but this
depends on the generic brands that already exist. The prices are set by the market and the
government. We cannot share the prices yet because none of the countries have national
guidelines for the drugs but in the next coming months we will see the Brazil approval and
the Kenya approval.

Association de lutte contre le sida (ALCS) : Rue Salim Cherkaoui. Quartier des Hôpitaux. 20360 Casablanca. MAROC
Tél : 00 212 5 22 20 94 90, Web : www.alcsmaroc.ma
First MENA-CAB, Casablanca, 28 June-1 July 2014