
Medicine Health RHODEI
32
UNDER THE JOINT EDITORIAL SPONSORSHIP OF: Brown Medical School Richard Besdine, MD, Dean of Medicine & Biological Sciences Rhode Island Department of Health Patricia Nolan, MD, MPH, Director Rhode Island Quality Partners Edward Westrick, MD, PhD, Chief Medical Officer Rhode Island Medical Society David B. Ettensohn, MD, President EDITORIAL STAFF Joseph H. Friedman, MD Editor-in-Chief Joan M. Retsinas, PhD Managing Editor Stanley M. Aronson, MD, MPH Editor Emeritus EDITORIAL BOARD Stanley M. Aronson, MD Edward M. Beiser, PhD, JD Jay S. Buechner, PhD John J. Cronan, MD James P. Crowley, MD Edward Feller, MD John P. Fulton, PhD Peter A. Hollmann, MD Anthony Mega, MD Marguerite A. Neill, MD Frank J. Schaberg, Jr., MD Fred J. Schiffman, MD Lawrence W. Vernaglia, JD, MPH Newell E. Warde, PhD William J. Waters, Jr., PhD OFFICERS David B. Ettensohn, MD President Fredric V. Christian, MD Vice President Tilak K. Verma, MD, MBA President-Elect Diane R. Siedlecki, MD Secretary Peter A. Hollmann, MD Treasurer Yul D. Ejnes, MD Immediate Past President DISTRICT & COUNTY PRESIDENTS Pamela A. Harrop, MD Bristol County Medical Society Gary A. L’Europa, MD Kent County Medical Society Jayanthi Parameswaran, MD Newport County Medical Society Stephen T. Conway, MD Pawtucket Medical Association Patrick J. Sweeney, MD, PhD, MPH Providence Medical Association R. Scott Hanson, MD Washington County Medical Society Naeem M. Siddiqi, MD Woonsocket District Medical Society R HODE I SLAND Medicine Health PUBLICATION OF THE RHODE ISLAND MEDICAL SOCIETY VOLUME 86, NO. 5 MAY, 2003 Medicine and Health\Rhode Island (USPS 464-820), a monthly publication, is owned and published by the Rhode Island Medical Society, 235 Promenade St., Suite 500, Providence, RI 02908, Phone: 401-331-3207. Single copies $5.00, individual subscriptions $50.00 per year, and $100 per year for institutional subscriptions. Published articles represent opinions of the authors and do not necessarily reflect the official policy of the Rhode Island Medical Society, unless clearly specified. Advertisements do not imply sponsorship or endorsement by the Rhode Island Medical Society. Periodicals postage paid at Providence, Rhode Island. ISSN 1086-5462. POSTMASTER: Send address changes to Medicine and Health\Rhode Island, 235 Promenade St., Suite 500, Providence, RI 02908. Classified Information: RI Medical Journal Marketing Department, 175 Mathewson Street, Providence, RI 02903, phone: (401) 331-4637, fax: (401) 331-3594 Cover: “Cyclist – Not Quite There Yet”, two-dimensional oil on canvas, with sand and wire, by Jeremy Ballard, originally from Tiverton, who is now a glassblower, painter and sculptor in Savannah, Georgia. COMMENTARIES 126 How Much Choice Does a Patient Have? Joseph H. Friedman, MD 127 A Medical Student Is Elected To the Presidency Stanley M. Aronson, MD, MPH POSITRON EMISSION TOMOGRAPHY (PET) IMAGING Guest Editor: John J. Cronan, MD 128 Imaging in the Second Century: The Introduction of Functional Imaging John J. Cronan, MD 129 Positron Emission Tomography (PET): The Basics Richard B. Noto, MD 132 PET: Oncological Applications Jac D. Scheiner, MD 136 Neurologic PET Anthony F. Posteraro, MD, and Richard B. Noto, MD 139 Cardiac Applications of Positron Emission Tomography (PET) Richard B. Noto, MD 143 Future Advances and Applications in Positron Emission Tomography Don Yoo, MD, and Richard B. Noto, MD 147 Certificate of Need Process: An Assessment of the Need for PET John X. Donahue, MPA COLUMNS 150 Quality Partners of Rhode Island - Notice 152 Health by Numbers DAMP HOUSING CONDITIONS AND ASTHMA IN RHODE ISLAND Leanne C. Chiaverini, Jana E. Hesser, PhD, and John P. Fulton, PhD 154 A Physician’s Lexicon THE VERBIAGE OF OBESITY Stanley M. Aronson, MD, MPH 154 Vital Statistics 156 Rhode Island Medical Journal Heritage ACKNOWLEDGEMENT: A grant from Philips has paid for the reproduction of images in this issue.
Transcript of Medicine Health RHODEI

UNDER THE JOINTEDITORIAL SPONSORSHIP OF:
Brown Medical SchoolRichard Besdine, MD, Dean of Medicine& Biological Sciences
Rhode Island Department of HealthPatricia Nolan, MD, MPH, Director
Rhode Island Quality PartnersEdward Westrick, MD, PhD, Chief MedicalOfficer
Rhode Island Medical SocietyDavid B. Ettensohn, MD, President
EDITORIAL STAFFJoseph H. Friedman, MD
Editor-in-ChiefJoan M. Retsinas, PhD
Managing EditorStanley M. Aronson, MD, MPH
Editor Emeritus
EDITORIAL BOARDStanley M. Aronson, MDEdward M. Beiser, PhD, JDJay S. Buechner, PhDJohn J. Cronan, MDJames P. Crowley, MDEdward Feller, MDJohn P. Fulton, PhDPeter A. Hollmann, MDAnthony Mega, MDMarguerite A. Neill, MDFrank J. Schaberg, Jr., MDFred J. Schiffman, MDLawrence W. Vernaglia, JD, MPHNewell E. Warde, PhDWilliam J. Waters, Jr., PhD
OFFICERSDavid B. Ettensohn, MD
PresidentFredric V. Christian, MD
Vice PresidentTilak K. Verma, MD, MBA
President-ElectDiane R. Siedlecki, MD
SecretaryPeter A. Hollmann, MD
TreasurerYul D. Ejnes, MD
Immediate Past President
DISTRICT & COUNTY PRESIDENTSPamela A. Harrop, MD
Bristol County Medical SocietyGary A. L’Europa, MD
Kent County Medical SocietyJayanthi Parameswaran, MD
Newport County Medical SocietyStephen T. Conway, MD
Pawtucket Medical AssociationPatrick J. Sweeney, MD, PhD, MPH
Providence Medical AssociationR. Scott Hanson, MD
Washington County Medical SocietyNaeem M. Siddiqi, MD
Woonsocket District Medical Society
RHODEISLANDMedicine Health�
PUBLICATION OF THE RHODE ISLAND MEDICAL SOCIETY
VOLUME 86, NO. 5 MAY, 2003
Medicine and Health\Rhode Island (USPS 464-820), a monthly publication, is owned and published by the Rhode Island Medical Society,235 Promenade St., Suite 500, Providence, RI 02908, Phone: 401-331-3207. Single copies $5.00, individual subscriptions $50.00 per year,and $100 per year for institutional subscriptions. Published articles represent opinions of the authors and do not necessarily reflect the officialpolicy of the Rhode Island Medical Society, unless clearly specified. Advertisements do not imply sponsorship or endorsement by the RhodeIsland Medical Society. Periodicals postage paid at Providence, Rhode Island. ISSN 1086-5462. POSTMASTER: Send address changes toMedicine and Health\Rhode Island, 235 Promenade St., Suite 500, Providence, RI 02908. Classified Information: RI Medical JournalMarketing Department, 175 Mathewson Street, Providence, RI 02903, phone: (401) 331-4637, fax: (401) 331-3594
Cover: “Cyclist – Not Quite There Yet”,two-dimensional oil on canvas, withsand and wire, by Jeremy Ballard,originally from Tiverton, who is now aglassblower, painter and sculptor inSavannah, Georgia.
COMMENTARIES
126 How Much Choice Does a Patient Have?Joseph H. Friedman, MD
127 A Medical Student Is Elected To the PresidencyStanley M. Aronson, MD, MPH
POSITRON EMISSION TOMOGRAPHY (PET) IMAGINGGuest Editor: John J. Cronan, MD
128 Imaging in the Second Century: The Introduction of Functional ImagingJohn J. Cronan, MD
129 Positron Emission Tomography (PET): The BasicsRichard B. Noto, MD
132 PET: Oncological ApplicationsJac D. Scheiner, MD
136 Neurologic PETAnthony F. Posteraro, MD, and Richard B. Noto, MD
139 Cardiac Applications of Positron Emission Tomography (PET)Richard B. Noto, MD
143 Future Advances and Applications in Positron Emission TomographyDon Yoo, MD, and Richard B. Noto, MD
147 Certificate of Need Process: An Assessment of the Need for PETJohn X. Donahue, MPA
COLUMNS
150 Quality Partners of Rhode Island - Notice
152 Health by NumbersDAMP HOUSING CONDITIONS AND ASTHMA IN RHODE ISLAND
Leanne C. Chiaverini, Jana E. Hesser, PhD, and John P. Fulton, PhD
154 A Physician’s LexiconTHE VERBIAGE OF OBESITY
Stanley M. Aronson, MD, MPH
154 Vital Statistics
156 Rhode Island Medical Journal Heritage
ACKNOWLEDGEMENT: A grant from Philips has paid for thereproduction of images in this issue.

126Medicine and Health / Rhode Island
COMMENTARIES� �
�How Much Choice Does
a Patient Have?
When I was a neurology residenta patient once kicked me out
of her room, or rather, her husbanddid. I wasn’t insulted. It was a smallplus for me actually. As a first year resi-dent one spent most time on the wardservice, seeing patients without privateattendings referred primarily from theemergency room and occasionally theclinics. The months on the private ser-vice were quite different. On the wardservice we’d admit three to five patientsevery fourth day usually, and tookcharge of the cases, formulating thedifferential, ordering and interpretingtests and generally caring for the pa-tients. An attending level neurologistsupervised but generally kept a lowprofile. On the private service, we’dadmit ten patients, write a history,document a detailed neurological examand conclude, “tests per Dr. X.” Onnon-admitting days, if interested, we’dstop by to see what was happening. Butgenerally, if one wasn’t admitting, onedidn’t have any in-patient work. Theteaching advantage of the private ser-vice was extraordinary. Patients camefrom far and wide to see the famousexperts. In those days patients wouldbe admitted sight unseen. In this par-ticular case, the patient came formOhio to see the famous Dr. X., a trueworld expert. Rather then seeing himin the office she was admitted directlyso that it would be easy to obtain anytests and also so that the fellows couldsee the patient on rounds. When Iwent to see the patient her husbandinformed me that his wife had seen aslew of neurologists in the Midwest,was here to see Dr. X., not me, and Ishould take a hike. I explained myneed to examine all patients because Iwas responsible when I was the onlydoctor in the hospital overnight, butthe man was adamant. I happily wroteup my admission note with a detailed
history and, in large letters, “patientrefused exam.” This saved a half-houror more. As I was leaving to go to an-other floor I met Dr. X. and told himwhat happened, expecting him to shakehis head and move on. He didn’t. “Shecan’t do that.” He marched me in tothe room and told the patient and hisspouse that I could examine her or shecould leave. Although not pleased, Iwas impressed.
Recently a colleague was similarlythrown out of a patient’s room and itbrought to mind the very complex is-sues surrounding medical care in hos-pitals, particularly teaching hospitals.In this case a patient, who was a uni-versity professor, asked a young Asian-born woman not to return. Dr. Asianwoman was brought in as a consult-ant. She was an assistant professor andattending for one particular consultingservice. Private doctors may also havebeen available but hers was the teach-ing service at the university hospital.The patient told her boss that he didn’twant a doctor who had trained at aforeign medical school. Her fellowshiptraining at the Harvard hospital theywere in didn’t seem to overcome his jin-goist inclination and her status as aHarvard assistant professor didn’t ei-ther. Perhaps he didn’t feel comfort-able with women. What was the“proper” response? What would theresponse have been if the doctor wasblack and the patient racist? Mostlikely the patient’s request would havebeen ignored. What if the patient wasfemale, the doctor male and the prob-lem gynecologic? Where do we draw aline between reasonable and unreason-able requests?
Should the service director havesaid, “Dr Asian woman has our com-plete confidence or we wouldn’t havehired her. If you don’t feel comfort-able with her despite her unimpeach-
able conduct then she will be taken offyour case and your primary doctor canfind another consultant?” I think so.Medical treatment is a service that hasseveral constraints. Patients cannotalways exercise free choice. There is aTV commercial in which a plumberenters a house to find it submergedwhile water is gushing out of a pipe.The young owner instead of lookingrelieved that his disaster is about to betaken care of, instead asks for an esti-mate to make sure he’s getting a goodprice. An emergency is an emergencyand generally if you’re in an Americanhospital in the 21st century it’s an emer-gency and there’s usually not time tocomparison shop. When the emer-gency resolves you can take time to findthe best and most compatible doctor.In the case of a hospitalized patient,the rejection of a service without jus-tifiable cause puts the onus on the pa-tient or the patient’s primary doctorto provide alternate care. If the pa-tients said, “I never heard of you butyour boss is famous, I want her,” therequest would have died immediately(unless the patient was a donor or aVIP).
Discrimination by doctors is un-acceptable and punishable. Discrimi-nation by patients, while notpunishable, is no more tolerable andshould not be supported.
– JOSEPH H. FRIEDMAN, MD

127Vol. 86 No. 5 May 2003
�A Medical Student Is Elected To the Presidency
His relatives described him as slim and of average height.His hair was said to be thin, beginning to grey at the
temples and was combed carelessly over his prominent fore-head. His face was of fair complexion, long and slim, with anelongated nose, strong jaw-line and thin lips. From a distancehe appeared to be a forbidding and unapproachable states-man; but in truth he was plain-spoken, affable, accessible andquite unpretentious.
William Henry Harrison may have seemed unpretentiousto his close friends, relatives and pastor, but to others his an-cestry alone would have made him a formidable and unap-proachable personage. His mother’s lineage, for example, wastraceable all the way back to Plantagenet England’s Henry III[1207-1272]. His father’s family had migrated from Englandto Virginia in 1632. The first of six successive William HenryHarrisons then became one of Virginia’s largest landowners.His son, the second William Henry Harrison, was elected tothe House of Burgesses, Virginia’s legislative council. The thirdWilliam Henry Harrison became Virginia’s Attorney General;the fourth William Henry Harrison was a colonel in the localmilitia as well as a member of the House of Burgesses. AndWilliam Henry Harrison’s father, the fifth bearing the name,was a member of the Continental Congress, a signatory of theDeclaration of Independence and governor of Virginia.
The sixth William Henry Harrison [1773-1841] was bornon February 9, 1773, at the family’s ancestral home, BerkleyPlantation, Virginia, the youngest of seven living children. Theplantation was attacked and partially destroyed by BenedictArnold and his troop of loyalist militia and the family, includ-ing four year-old William Henry, sought refuge elsewhere.Biographers claim that it was during this critical interval in hislife that he declared his intention to become a physician.
William Henry’s elementary education was in the handsof competent private tutors. At the age of 14, he was sent toVirginia’s Hampden-Sydney College for premedical studies.Records indicate that he successfully completed his classes inrhetoric, mathematics, geography, history and classical lan-guages. From early childhood William Henry was deeply reli-gious and committed to the verity of the Bible. He left collegewhen the institution’s formerly Episcopalian spirit was sup-planted by a “Methodist fervor.”
In 1790, at age 18, William Henry began his medicalapprenticeship with Dr. Andre Leiper of Richmond, Virginia,and in 1791 he transferred to the medical college of the Uni-versity of Pennsylvania to complete his final requirements forthe degree of Doctor of Medicine. His principal tutor was apolitical acquaintance of his father, Dr. Benjamin Rush, also asigner of the Declaration of Independence.
In August of 1791, William Henry’s father unexpectedlydied, leaving the family’s fiscal status in disarray. William Henry,with heavy heart, then left the medical school and enlisted inthe United States Army.
His military career was auspicious. He rose to the rank ofcaptain and later to the rank of major general in the infantry,playing a leadership role in the decisive battle of Tippecanoe
in 1811. William Henry participated in the Indian Wars withinthe Northwest Terrirtory and in the battles with the Britishduring the War of 1812, during which time he led the Ameri-can troops in the recapture of Detroit. He was appointed byPresident John Adams as Governor of the Indian Territoriesand he fashioned the treaty leading to unhindered white settle-ments in the states of Illinois, Indiana, and Ohio. He resignedfrom the Army in 1814 and in 1816 was elected to the Houseof Representatives in Washington. From this time onward hiscareer was solely in politics and government posts. In 1819 hewas elected to the United States Senate, representing Ohio[which had achieved statehood in 1803].
In 1836 the Whig party chose William Henry Harrison asits candidate for the Presidency. He lost to Martin van Buren,but ran again, this time successfully, in 1840, with John Tyler ashis Vice President and Daniel Webster as his Secretary of State.
William Henry Harrison, sometime medical student, vet-eran infantryman, governor and legislator, was inaugurated onMarch 4, 1841, as the ninth President of the United States.The weather on that day was bitterly raw, with intermittentrain and high winds. Despite the inclement weather, Harrisonchose to deliver an inaugural address lasting an hour and fortyminutes. And despite his age [at 68, he was the oldest newlyelected President until Ronald Reagan in 1980] he chose todeliver this closely reasoned speech with neither a coat, a hatnor even the partial protection of an umbrella.
Within a day he took to bed with a high fever and signs ofpulmonary involvement. His chest infection then seemed toabate but within a few more days his fever rose precipitously,associated now with severe chest pains made worse by a hack-ing cough. The President’s physicians diagnosed his mortalcondition as “bilious pleurisy.” And within a few weeks he died.John Tyler of Virginia, his vice president, assumed the Presi-dency.
William Henry Harrison served a total of 31 days as Presi-dent, the shortest tenure in office of any American Presidentand the first President to die in office. One of his sons had thedistinction of being both the son of the ninth President of thisnation and the father of the twenty-third President [BenjaminHarrison, 1833-1901]. Another son became a practicing phy-sician in Vincennes, Indiana.
There is little in Harrison’s career as military officer, legis-lator, governor or President that reflects his earlier training inclinical medicine. Most physicians, during their years of for-mal education, do learn the basic Hippocratic aphorisms, oneof which is: Primum non nocere [first, do no harm; do not in-tervene, in other words, unless you are certain that your inter-vention has some positive value]. One can speculate that a barehint of this aphorism emerges in one of Harrison’s more memo-rable quotations: “The people are the best guardian of theirown rights and it is the duty of their executive to abstain frominterfering or thwarting the sacred exercise of the lawmakingfunctions of their government.”
– STANLEY M. ARONSON, MD, MPH

128Medicine and Health / Rhode Island
�Imaging in the Second Century:
The Introduction of Functional Imaging
John J. Cronan, MD
A new era of imaging has arrived. Di-agnostic Imaging is no longer fo-
cused on morphology-lumps, bumps,masses, etc. We are now probing me-tabolism and cellular function, creatingan image based upon metabolic activitywithin the cell.
Positron Emission Tomography(PET) is our introduction to molecularimaging. The future of imaging dependsupon functional imaging because it willpermit “visualization in space and timeof normal as well as abnormal cellularprocesses at a molecular or genetic levelof function.” 1 The radiologist will use aprobe such as 18 fluoro dioxoglucose(FDG), directed to specific targetswithin the body, permitting imaging ofcellular function.
How is this image different fromthe CT or MRI images employing theiodinated contrast of CT or Gadoliniumin MRI? These latter agents are not spe-cific for a particular metabolic activity.Rather, the present contrast agents re-spond to distribution dynamics, such asextra cellular space, blood flow and thebreakdown of the blood brain barrier.They do not demonstrate cellular meta-bolic activity.
Today we hope to identify abnor-mal cellular processes before they createlumps or bumps in organs. We wish toimage abnormal pathophysiology whenit is only a metabolic process, not a mor-phologic process. Futuristically, theseprobes will be targeted specifically tomatch a patient’s tumor or metabolicdefect. We will be freed of the evalua-tion of tumor size as a criteria for che-motherapy success and instead evaluatethe molecules responsible for the tumor.Hitherto, we begin chemotherapy andwait months before determining if ourtherapeutic effort is effective. Tumor sizeis our barometer of success or failure oftreatment. Utilizing molecular imaging,we will soon evaluate the tumor’s abilityto replicate and express certain proteinsas soon as chemotherapy is initiated.
potential of PET and introduce the con-cept of functional imaging. Rhode Is-land is probably the last state in theunion to acquire this technology, so Icannot construe that it is extravagant,but rather an important service to beprovided to our patients. In this issuewe hope to review how PET was ac-quired in this state, how the Departmentof Health determined PET was readyfor clinical introduction and the mecha-nism they developed to ensure qualityreading when the examinations begin.In addition, we will review the physicsof PET, review the present indicationsfor PET, which although mainly onco-logic, do have some limited uses in neu-rologic and cardiac disease. And finally,we will explore the future potential forPET.
I trust you will find this issue use-ful and exciting as you look at cellularactivity. This is our first probe into as-sessing cellular function.
REFERENCES1. Ronald Blasbey, MD., Director of
Neuro-Oncology PET program atMemorial-Sloan Kettering CancerCenter, New York, New York.
John J. Cronan, MD, is Professor andChairman, Department of DiagnosticImaging, Rhode Island Hospital andBrown Medical School.
CORRESPONDENCE:John J. Cronan, MDDepartment of Diagnostic ImagingRhode Island Hospital593 Eddy St.Providence, RI 02903Phone: (401) 444-5184Fax: (401) 444-5017e-mail: [email protected]
�
We will be freed of theevaluation of tumor size
as a criteria forchemotherapy success and
instead evaluate themolecules which are
responsible for the tumor.
As we are introduced to molecularimaging, FDG is our initial probe. It isa marker of glucose, which is increasedin tumors because of increased cellularmetabolism. This increased cellular ac-tivity is a biomarker for the presence oftumors.
We seek more specific markers thatwill delineate specific molecular events,which are signatures of diseases – ova-rian cancer, Alzheimer’s disease, breastcancer.
Our initial focus in the use of PETwill be with oncology. The brake onthe development of PET, which hasbeen available for over twenty years, hasbeen the limited reimbursement byMedicare. Unfortunately, the penetra-tion of PET into other disease processeswill also be determined mainly on thebasis of approved indications, which ul-timately lead to reimbursement. Anexamination technique, lacking reim-bursement, will not be performed in theclinical arena.
Concern is continuously raised thatPET is just “another imaging tool” thatwill not replace any previous modality.This may well be true, but delineationof tumor extent will permit a markedlyimproved staging process, and hopefullyavoid unnecessary and non-therapeuticsurgical procedures.
We anxiously await the opportu-nity as radiologists to illuminate the

129Vol. 86 No. 5 May 2003
�Positron Emission Tomography (PET): The Basics
Richard B. Noto, MD
“Positron Emission Tomography(PET) is the most important advancein biomedical science since the inven-tion of the microscope.”1 While thismay sound like excessive praise for amodality that has only recently provenitself in the clinical arena, this quotefrom Henry N. Wagner, Jr., MD, Di-rector of the Division of RadiationHealth Services at the Johns HopkinsBloomberg School of Public Healthand former Chief of Nuclear Medicineat Johns Hopkins, gives a sense of thevast potential of PET in the twenty-first century. As a clinical and researchtool, PET has the capability of provid-ing the medical community physi-ologic and molecular information thathas heretofore not been available andthat may improve the management ofa wide variety of diseases. Already, PETis contributing new information to ourunderstanding of oncology, cardiology,and neurology. All who are involvedwith this modality would agree that wehave only begun to scratch the surfaceof the potential of PET imaging.
PET refers to the branch ofnuclear medicine where a radioactivepositron emitting radiopharmaceuticalis administered to a patient for thepurposes of producing tomographicimages of the distribution of the ra-diopharmaceutical. The radio-isotopesthat decay by positron emission includeFluorine-18, which is readily linked toa glucose analog to produce 2-(F-18)fluoro-2-deoxyglucose (FDG), andcarbon-11, nitrogen-13, and oxygen-15, which have the advantage of beingthe atoms that are the basic buildingblocks of all physiologic processes.
The history of PET dates back tothe discovery of the positron by Ander-son and the invention of the cyclo-tron by Lawrence in the 1930s. Thefirst positron-detecting camera wasproduced by Ter-Pogossian in the early1970s and this technology was refinedover the subsequent decades to themodern day PET camera.2 While re-search studies with PET imaging date
back almost 30 years, it was not untilthe advent of clinical studies with FDGin the late 1980s that the clinical po-tential of PET started to become ap-parent.3 Multiple studies in the 1990sindicated the efficacy of PET in on-cology and applications in cardiologyand neurology were refined for clini-cal use.4,5
While it was becoming clear thatPET was potentially a formidable clini-cal tool, its development was severelylimited until the late 1990s by issuesrelated to the production and availabil-
ity of positron emittingradiopharmaceuticals. Positron emit-ting radio-isotopes can only be pro-duced in sufficient quantity formedical use by a cyclotron: the highcost of purchasing and maintaining acyclotron limited this technology toonly a few sites in the country. Be-cause all medically useful positronemitters are short-lived (half-life of 109minutes for F-18, 20 minutes for C-11, 10 minutes for N-13, and 2 min-utes for O-15), it is necessary to have acyclotron in close proximity to the
TABLE 1. CURRENT MEDICARE APPROVEDAPPLICATIONS OF PET
Clinical Condition Coverage
Solitary Pulmonary Nodules Characterization
Lung Cancer (Non-small cell) Diagnosis, Staging, and Re-staging
Esophageal Cancer Diagnosis, Staging, and Re-staging
Colorectal Cancer Diagnosis, Staging, and Re-staging
Lymphoma Diagnosis, Staging, and Re-staging
Melanoma Diagnosis, Staging, and Re-stagingNot covered for evaluating regionalnodes
Head and Neck Cancer Diagnosis, Staging, and Re-stagingNot covered for CNS and thyroidcancers
Breast Cancer As an adjunct to standard imagingmodalities in staging (patients withdistant metastasis) and re-staging(patients with locoregional recurrenceor metastasis)As an adjunct to standard imagingmodalitiesfor monitoring tumorresponse to treatment for women withlocally advanced and metastaticbreast cancer when a change intherapy is anticipated.
Refractory Seizures Pre-surgical evaluation only
Myocardial Perfusion Noninvasive imaging of heart perfu-sion
Myocardial Viability Primary or initial diagnostic study, orfollowing an inconclusive SPECT,prior to revascularization (SPECTmay not be used following aninconclusive PET scan)
Specific conditions apply to some of the above coverage policies. Seethe Blue Cross Blue Shield of RI Policy RI-2002-100 for further details.

130Medicine and Health / Rhode Island
imaging device since the activity willrapidly decay to too low a level to beclinically useful. However, once it be-came apparent that FDG had poten-tially major applications in oncology,a variety of manufacturers set up re-gional cyclotrons that could produceFDG and ship it rapidly to sites in thatregion. Currently, FDG is readily avail-able in all urban areas throughout theUS and many more rural areas also nowhave FDG access as well. Unfortu-nately, the shorter lived isotopes likeC-11, N-13, and O-15 remain avail-able only to those locations that havean on-site cyclotron. Another positronemitting radio-isotope, rubidium-82,has been used for evaluating myocar-dial perfusion and has an extremelyshort half-life (76 seconds), but can beproduced from an on-site generator forimmediate use on an as-needed basis.
FDG has become such an impor-tant agent in recent years because itallows the imaging of sites of active glu-cose metabolism. It is transported intocells that consume glucose and thenundergoes phosphorylation to FDG-6-phosphate. In this form, it is retainedin the cell and can be imaged with PETscanners. Under normal circumstances,there is intense uptake in the brain,which is an obligate glucose user, andvariable degrees of normal uptake inthe myocardium depending on serumglucose levels. In addition, a varietyof pathologic processes lead to alter-ation of glucose metabolism. In thebrain, sites of decreased glucose me-tabolism may be seen in patients withAlzheimer’s disease and epilepsy. In theheart, areas of decreased perfusion thatshow increased glucose metabolism areindicative of viable myocardium thathas switched from aerobic to anaero-bic metabolism because of inadequateperfusion.
Because many cancers showmarkedly increased glucose metabo-lism, FDG can be utilized to visualizesites of active tumor. This is useful instaging because the whole body is vi-sualized and sites of malignancy showup as areas of increased activity. How-ever, PET with FDG is often even moreuseful in re-staging after treatment be-cause it can differentiate residual tu-
mor from scar tissue, which is often notpossible with anatomic imaging mo-dalities like CT and MR. Unfortu-nately, the downside of this ability toimage physiology is some non-speci-ficity; non-malignant processes such asinfection and inflammation may alsohave increased glucose metabolism andtherefore can show up as increased ac-tivity on an FDG PET scan.
All positron emitting radio-iso-topes produce emissions that are de-tectable by PET cameras through aprocess called annihilation. Thepositron that is emitted by the processof nuclear decay travels a very shortdistance in soft tissues before encoun-tering an electron. This distance is de-termined by the energy of the positronand should be as small as possible foraccurate localization and image pro-duction. For F-18, the energy of thepositron is relatively low and the meanpositron range in water is only 1.4 mmwhich is ideal for imaging purposes.When a positron of appropriate energyencounters an electron, the two anni-hilate, meaning that there is completeconversion of the positron-electronpair into energy in the form of twogamma photons. The two gamma pho-tons produced in annihilation each
have an energy of 511 keV and travelin opposite directions, 180 degreesfrom each other.
PET scanners are designed to de-tect these annihilation photons in ahighly efficient manner. Most mod-ern PET scanners consist of a ring ofdetectors which encircle the patient.For an event to be recorded, 511 keVphotons must strike detectors that are180 degrees opposed to each otherwithin a very brief time period; suchan event is called a coincidence eventand a line of response is drawn betweenthe two involved detectors. PET im-ages are produced by generation of alarge number of such lines of response,which are proportional to the concen-tration of the radiopharmaceutical inthat particular location. The line ofresponse data is then reconstructed intotransaxial, coronal, and sagittal planesas well as three dimensional volumerenderings using complex iterative re-construction algorithms.
Numerous variables in the con-struction of PET cameras have a majorimpact on the quality of images that areproduced. Probably the most impor-tant variable is the choice of a full ringdetector system versus a modified dualhead gamma camera. As PETradiopharmaceuticals began to becomereadily available, manufacturers devisedmethods for modifying conventionaldual head gamma cameras with a thickersodium iodide (NaI) crystal and com-puter improvements such that one coulduse these modified gamma cameras toimage both single photon and positronemitting radiopharmaceuticals. Whilethese cameras served as a first step intothe world of PET imaging for many in-stitutions, the resolution and sensitiv-ity of these modified dual head units isnot comparable to that of dedicatedPET scanners and CMS (Centers forMedicare and Medicaid Services, for-merly HCFA) has placed severe limita-tions on their reimbursement of studiesperformed on these cameras in the fu-ture.
Modern dedicated PET systemsuse one of four types of crystal materialfor their detectors. Bismuth germanate(BGO) has been the most commonlyused detector material in large part due
�
FDG has become suchan important agent inrecent years because itallows the imaging ofsites of active glucose
metabolism.
�
While FDG is anextremely useful
radiopharmaceutical, itis just the first in whatwill be a long line ofPET imaging agents.

131Vol. 86 No. 5 May 2003
to its very high density which is good atstopping and registering the high energyphotons produced in PET. More re-cently, two new detector materials havereached the market which may eventu-ally replace BGO. Both gadoliniumoxyorthosilicate (GSO) and lutetiumoxyorthosilicate (LSO) have character-istics that allow faster acquisitions withno loss of resolution compared withBGO. The fourth crystal material thatis currently available is NaI, which is theleast expensive but also the least effec-tive choice for PET detectors. The reso-lution of modern BGO, GSO, or LSOPET cameras is approximately 4 mm.
The most recent innovation inPET systems is the hybrid PET/CTscanners. These units, which includeboth a dedicated ring detector PETsystem and a multi-slice CT scannerplaced back-to-back in the same orimmediately adjacent gantries, mayeventually become the standard forPET imaging. These units have theadvantage of superior attenuation cor-rection algorithms by using the CTacquisition to correct the PET imageand also allow near perfect co-registra-tion of the PET and CT images. Thismeans that the anatomic informationfrom CT and the physiologic informa-tion available from PET can be viewedon a single image which has major ad-vantages in confirming and localizingPET findings.
When PET was first utilized clini-cally, the potential applications wereprimarily neurologic and includedevaluation of complex partial seizuresprior to surgical therapy and evalua-tion of brain tumors, especially to dif-
ferentiate recurrent tumor from radia-tion therapy. It was also apparent inthe 1980’s that PET could be usefulfor detection and evaluation of coro-nary artery disease and determinationof myocardial viability. However, it hasbeen the burgeoning oncologic appli-cations for PET that have brought themodality to the forefront in the pastfew years and which continue to evolverapidly at this time. The current listof applications for PET that are ap-proved for reimbursement by CMSand the local Medicare carrier are listedin Table 1.6
The potential of PET is limitless.While FDG is an extremely useful ra-diopharmaceutical, it is just the firstin what will be a long line of PET im-aging agents. Because of the possibil-ity of distribution through regionalpharmacies as with FDG, a variety ofF-18 labeled agents are under devel-opment, primarily for oncologic appli-cations. Potentially even moreintriguing are the C-11 agents whichcan be used to image various receptorand transporter systems in the brain aswell as fatty acid metabolism in theheart. Further in the future, it is withinthe capabilities of PET to image DNAsynthesis mechanisms and cellular pro-liferation as well as enzymes that maybe important tumor targets.
In summary, the PET applicationsthat we are seeing in 2003 are just asmall sampling of the future directionsof this technology which will be an es-sential tool in the imaging armamen-tarium available to clinicians andresearchers now and in the future.
REFERENCES1. Wagner HN. Historical Outline. In:
Wahl, RL, ed. Principles and Practiceof Positron Emission Tomography. Phila-delphia: Lippincott, Williams &Wilkins, 2002: xiii.
2. Ter-Pogossian MM. The origins ofpositron emission tomography. SeminNucl Med 1992; 22:140-9.
3. Kessler RM, Partain CL, Price RR,James, AE. Positron emission tomog-raphy: prospects for clinical utility.Invest Radiol 1987; 22:529-37.
4. Coleman RE. Clinical PET in oncol-ogy. Clinical Positron Imaging 1998;1:15-30.
5. Bar-Shalom R, Valdivia AY, BlaufoxMD. PET imaging in oncology. SeminNucl Med 2000; 30:150-85.
6. www.rimedicare.org/files/RI-2002-100.htm.
Richard B. Noto, MD, is Directorof Nuclear Medicine, Department ofDiagnostic Imaging, Rhode Island Hos-pital, and Clinical Assistant Professor ofRadioloty, Brown Medical School.
CORRESPONDENCE:Richard B. Noto, MDDepartment of Diagnostic ImagingRhode Island Hospital593 Eddy St.Providence, RI 02903Phone: (401) 444-5184Fax: (401) 444-5017e-mail: [email protected]

132Medicine and Health / Rhode Island
Positron Emission Tomography(PET) has many clinical applica-
tions. Most are in the oncologic arena.There are currently seven Medicare-re-imbursable oncologic indications forperforming PET scans; i.e., stagingand restaging for cancer of the colon,head and neck (excluding CNS andthyroid), esophagus, lung, lymphoma,breast (distant to the axilla) and mela-noma. PET has also been approvedfor evaluating the response of breastcancer to therapy, as well as to evalu-ate for the presence of malignancy in apulmonary nodule.
PET is effective in cancer imag-ing because it is able to image radio-labelled glucose. Many types of cancerselaborate an increased amount of glu-cose receptors to obtain sufficient glu-cose to maintain their high metabolicrates. 18-Fluoro-deoxyglucose [FDG]is thus taken up by cancer cells in highamounts. FDG is thenphosphorolated, which results in itstaying in the cell without undergoingglycolysis. A PET camera images thisphosphorylated version of FDG.
Intracellular FDG provides severaladvantages in oncologic imaging over‘morphologic’ imaging modalities such
�PET: Oncological Applications
Jac D. Scheiner, MD
as computed tomography (CT). WithCT, the possibility of a lymph nodebeing involved with malignancy is typi-cally not suggested unless it is enlarged(i.e. greater than 1 cm). Of course,there can be malignant involvementwith smaller lymph nodes. However,to raise suspicion for malignancy inthese smaller nodes would result in sig-nificantly decreased specificity, becausethese nodes are common even in nor-mal patients. Freed of morphologiccriteria, small nodes involved withmalignancy can be detected on FDGPET scans.
There are other advantages ofFDG PET over CT or MRI. FDGPET can detect malignancy in tumorsites that have the same appearance asadjacent normal structures on CT.FDG PET also has the ability to dif-ferentiate post-therapeutic/surgical
changes (such asscar, which is notmetabolically active)from residual/recur-rent neoplasm(which is metaboli-cally active).
LIMITATIONS OF PET IN ONCOL-OGY
Despite the widespread oncologicapplications of FDG PET, several cau-tions should be noted.
1. Some common cancers whichare either not as metabolically active,do not elaborate significant amountsof glucose receptors, or are unable toretain FDG - Prostate cancer,BronchoAlveolar Lung Cancer, andHepatocellular Carcinoma - are notwell seen on FDG PET scans. In ad-dition, small amounts of tumor [suchas malignancy in <5 mm lung nodulesor nodes] are not so easily detectableon FDG PET.
2. FDG PET scans tend to havedecreased sensitivity in patients withdiabetes. FDG PET scans can be per-formed in diabetic patients, althoughit more active tumors may need to bepresent before imaging is abnormal.
3. The brain typically takes up asignificant amount of FDG on PETscans. This increased backgroundmakes it difficult to discern a focus ofmetastatic disease. MRI of the brainwith i.v. contrast is thus superior toPET for detecting brain metastases.
4. CT of the chest is more sensi-tive for detecting very small lung me-tastases (especially those less than 5mm) than FDG PET.
5. In addition to being taken upby sites of malignancy, FDG is alsotaken up by active granulomatous dis-ease such as sarcoidosis and tuberculo-sis, as well as pneumonia. Thus, FDG
�
PET is effective in cancerimaging because it is ableto image radio-labelled
glucose.
Case 1a - Patient with known right upper lobe lung cancer. CTdemonstrates patients known lung cancer. No enlarged lymph nodes
were noted on CT.
Case 1b - PET scan demonstrates increased metabolic activity in theright upper lobe, consistent with known lung cancer. No other areas ofabnormal activity are seen. There is normal activity in the urinary tract
and heart. The findings are consistent with a resectable lung cancer.
133Vol. 86 No. 5 May 2003
PET should not be used to distinguishmalignancy from inflammatory dis-ease.
6. As is true with all imagingstudies, FDG PET scans should not beperformed unless they can potentiallychange patient management. For ex-ample, if a patient with lung cancer hasknown diffuse metastatic disease to thebone, finding a few more sites of tu-mor on FDG PET will not change pa-tient management. However, if apatient has potentially resectable lungcancer by CT and other modalities,FDG PET should be performed toensure correct staging.
PET AND PUBLISHED ONCOLOGIC
STUDIES
1. Lung Cancera. Lung Nodules – Approxi-
mately 80% of lung nodules will bebenign granulomas or malignancies.The standard work-up of a nodule seenon a chest radiograph is to identify cen-tral calcification within the nodule in-dicating with benignity. If this findingcan not be ascertained, the next step isto compare the chest radiograph toprior radiographs to document ap-proximately 2-3 years of stability, con-sistent with benignity. If the possibilityof malignancy persists, the next step isCT of the chest, which can detect be-nign central calcification within thenodule with a higher sensitivity thanconventional radiographs.
If the possibility of malignancypersists after CT evaluation, the nextstep is to decide whether to biopsy thenodule or perform short term follow-up imaging with CT. FDG PET is apowerful triage tool. A nodule whichdemonstrates FDG uptake on PETtypically warrants a biopsy. Alternately,
a nodule withoutPET activity is evalu-ated with short termfollow-up imagingwith CT.
FDG PET isnot recommendedto evaluate nodulesless than 5mm or atumor that is notvery metabolicallyactive, such asbronchoalveolar cellcarcinoma.1 Thus, a negative PETscan should not stop the work-up oflung nodule. However, it providesgreater confidence for triaging the pa-tient to the ‘follow-up imaging’ armof the lung nodule work-up, as op-posed to biopsy.
A meta-analysis of PET studies of1474 lung nodules/masses publishedfrom 1966-2000 showed that PET hadan impressive 97% sensitivity for ma-lignancy. 2 The specificity was 78%,thus emphasizing the importance ofutilizing PET in the appropriate clini-cal context, such as not using this mo-dality to distinguish malignancy frompneumonia.
b. Staging/Restaging of Non-Small Cell Lung Cancer (NSCLC) –A recent study of 102 patients whounderwent invasive surgical staging ofthe mediastinal lymph nodes, chest CTand FDG PET, showed that the sensi-tivity/specificity for malignant lymphnodes was 95%/86% for FDG PET,vs. 75%/66% for CT.3 Often, theFDG PET scan reveals previously un-known sites of metastatic disease thatwill obviate the need for a thoracotomy.A recent randomized controlled trial of188 patients with NSCLC demon-strated that the futile thoracotomy rate(ie. those patients that underwent lungcancer resection and then demon-strated recurrence within 1 year) was41% in patients who underwent non-PET staging vs. 21% for those stagedwith PET.4
When lung cancer is treated viaradiation therapy and/or chemotherapy,post-treatment CT often cannot distin-guish scar tissue from persistent cancerin residual masses. PET is an ideal solu-tion in this situation becauses live can-cer cells usually take up FDG, whereasscar tissue does not. In a study of 126patients with stage I – IIIb NSCLC, ofwhom 60 had persistent or recurrenttumor, the sensitivity/specificity for per-sistent or recurrent tumor was 100%/92% for FDG PET vs. 71%/95% forCT.5 In addition, PET correctly pre-dicted response to therapy in 96% ofthese 126 patients.
2. Esophageal CancerThe main advantage of PET in
staging esophageal cancer is its abilityto accurately detect malignancy in non-regional lymph nodes which are notenlarged on CT or endoscopic ultra-
Approved Oncologic Indications – PET
• Staging and restaging of - colon cancer – head and neck– esophagus– lung– lymphoma– breast (distal and axial)– melanoma
• Evaluating response to therapy of beast CA
�
When lung cancer istreated via radiation
therapy and/orchemotherapy, post-treatment CT often
cannot distinguish scartissue from persistent
cancer in residual masses.
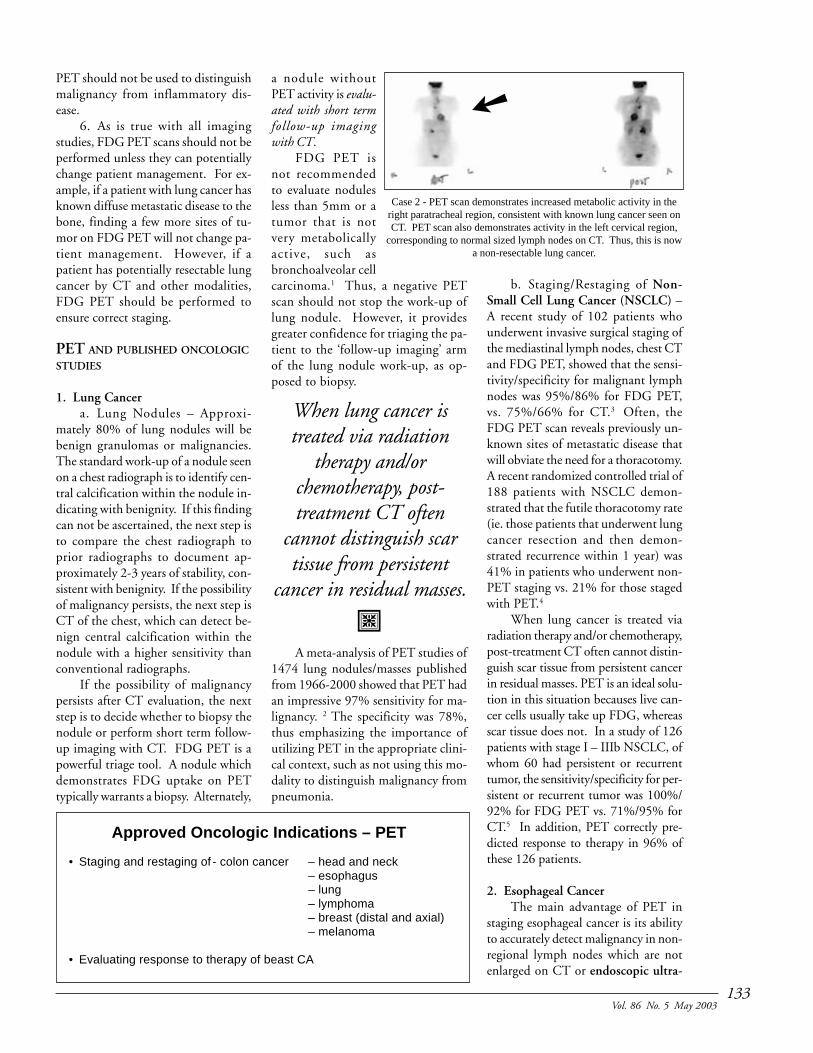
Case 2 - PET scan demonstrates increased metabolic activity in theright paratracheal region, consistent with known lung cancer seen onCT. PET scan also demonstrates activity in the left cervical region,
corresponding to normal sized lymph nodes on CT. Thus, this is nowa non-resectable lung cancer.
➙

134Medicine and Health / Rhode Island
sound (EUS). A recent prospectivestudy was performed in which 42 pa-tients all underwent PET, CT and EUSbefore surgical staging of espophagealcancer.6 PET was less accurate fordetecting malignancy in local regionallymph nodes (N1, N2) compared tocombined CT and EUS, 48% vs. 69%.This was likely due to the higher sen-sitivity of EUS for detecting small re-gional nodes. However, the accuracyfor distant nodal metastatic disease wasgreater for PET, 86% vs. 62%. Thiswas mostly due to greater specificity ofPET uptake, 90% vs. 69%.
3. Colorectal CancerA prospective, blinded study was
performed on 115 patients with a his-tory of colon cancer.7 All had a clini-cal suspicion for persistent/recurrentcolon cancer and underwent CT andPET. Compared to a gold standard of
follow-up imaging and/or findings at surgery,the sensitivity/specific-ity of PET was 93%/98% vs. 69%/96% forCT. Impressively, PETscans were true positivein 12 (67%) of 18 pa-tients with elevated se-rum carcinoembryonicantigen levels and nega-tive CT findings.
4. Head and NeckCancer
When a patientpresents with malignantcervical lymph nodes,conventional forms ofdiagnostic imaging suchas CT often fail to iden-tify the primary tumor.As a result, patients mayneed to undergo neckdissection or radiationof both sides of the neckwith random biopsies.PET scanning can re-veal the site of the pri-mary tumor preventingthe adverse effects ofrandom biopsies or un-needed radiation. Inpooled data from 4
studies, which included 76 patientswith malignant cervical lymph nodesand unknown primary despite CT,FDG PET correctly demonstrated theprimary site in 30% of these patients.8
[The review paper did not cite the per-centage of false positives.]
In patients with malignant cervi-cal lymph nodes, FDG PET allows formore accurate staging, which is essen-tial for determining whether to per-form dissection or radiation. Aprospective, blinded study of 19 pa-tients with malignant cervical lymphnodes was performed. 9 CT alone cor-rectly staged 69% of patients, whereasCT and FDG PET combined correctlystaged 92%.
5. MelanomaFDG PET is useful in detecting
sites of melanoma, but not in definingregional draining lymph nodes. Sen-
tinel node biopsy is superior in thesecases. A prospective, blinded study of74 patients with melanoma (70 ofwhom had melanoma > 1mm in depth)was performed.10 All had FDG PETscans followed by sentinel node biopsyas the gold standard. The sensitivity/specificity of FDG PET for malignancyin regional lymph nodes was 17%/96%.
For assessing sites of melanomaelsewhere, however, FDG PET hasbeen shown to be superior to conven-tional imaging such as CT. A prospec-tive study of 100 patients with high risk(>1.5 mm depth) melanoma was per-formed.10 All underwent conventionalimaging (which included CT) alongwith FDG PET. For sites of malig-nancy in the 52 patients who presentedfor initial staging, the sensitivity/speci-ficity for FDG PET was 100%/94%,whereas conventional imaging did notdetect any of the 9 sites of lymph nodesmetastases. Among the 48 patientsassessed for melanoma recurrence, thesensitivity/specificity for patients withrecurrence was 100%/96% for FDGPET vs. 85%/68% for conventionalimaging. For sites of recurrence, FDGPET was more sensitive to conven-tional imaging for detecting melanomain the neck and abdomen (100% vs.67% and 100% vs. 27% respectively),although CT was more sensitive fordetecting small lung metastases (87%vs. 70%).
6. LymphomaTraditionally, patients with lym-
phoma underwent both CT and Gal-lium Scintigraphy [GS] at initialstaging. The purpose of GS was two-fold. GS allows true whole body im-aging, from head to toe, and thus alarger field of view for detecting sitesof active lymphoma than on CT. Moreimportantly, most post-therapy lym-phoma patients will have residualmasses at original lymphoma sites onCT. The initial follow-up CT is un-able to differentiate residual masses dueto scar tissue vs. active lymphoma.However, if the initial GS demon-strated that the lymphoma is of a typethat takes up Gallium, the GS can berepeated, with a lack of uptake indi-
Case 3b - PET scan demonstrates increased activity in the region ofthe gastrohepatic ligament, consistent with a site of recurrent tumor
[arrow]. In retrospect, this mass was present on CT, although itsappearance was similar to a non-distended gastric fundus.
Case 3a - CT scan performed on patient with history of resectedcolon cancer and rising CEA was originaly read as negative.

135Vol. 86 No. 5 May 2003
cating scar tissue.A number of studies have recently
been published showing that not onlycan FDG PET be used for the samepurposes that GS had been used inlymphoma patients, but also that FDGPET was more accurate than GS. Astudy was performed on 51 patientswith lymphoma (38 non-Hodgkins, 13Hodgkins).11 All had FDG PET andGS (including single photo emissioncomputed tomography), and the sig-nificance of discordant sites were de-termined via correlation with CT andother clinical exams (including follow-up imaging). FDG PET detected all51 patients with active lymphoma, aswell as all 158 known sites of diseasein these patients. GS detected 72% ofsites and 80% of patients with activelymphoma.
7. BreastFDG PET at the current time
does not play a role in differentiatingbenign from malignant breast lesions.There are no significant studies onFDG PET playing a discriminatingrole in populations with a < 50% preva-lence of breast cancer who have lesionsreferred for biopsy. However, a meta-analysis of pooled data of 13 studies(n=606) with a >50% prevalence ofbreast cancer showed the sensitivity/specificity of FDG PET to be 89%/80% for primary breast malignancy.12
Given the high costs of FDG PETcompared to the less expensive, moreaccurate results of biopsy, FDG PETdoes not play a role in this realm.
Sentinel node biopsy is superiorto FDG PET for staging the axilla. Ameta-analysis was performed on 4 stud-ies with a pooled patient populationof 203 patients with breast cancer andnon-palpable axillary lymph nodes.12
All underwent FDG PET and sentinelnode biopsy (as the gold standard).The sensitivity/specificity of FDG PETfor detecting malignancy in the axillawas 80%/89%.
FDG PET has been approved forthe staging/restaging of distant spreadof breast cancer (beyond the axilla). Astudy was performed in which 48breast cancer patients underwent bothFDG PET and Tc-99m Bone Scans.13
The accuracy of FDG PET for detect-ing metastatic lesions to bone was 95%vs. 79% for Bone Scans. This waslikely related to the greater specificityof FDG PET for malignancy.
In another study, 57 breast cancerpatients with suspicion of recurrenceunderwent whole body FDG PET.14
Results were compared to a gold stan-dard of biopsy, follow-up imaging ofup to 2 years, and other diagnostictests. The sensitivity/specificity fordetecting patients with recurrence was93%/79%.
FDG PET has also been approvedfor evaluating tumor response to treat-ment. A prospective study was per-formed on 40 patients with estrogenreceptor positive breast cancer that wasat least locally advanced.15 Compar-ing the pre-therapy FDG PET to oneobtained 7-10 days after the start oftherapy, the sensitivity/specificity ofFDG PET for predicting responders totherapy was 95%/89%.
The oncologic indications forPET continue to evolve. This is an areain evolution and formal indications areconstantly changing
REFERENCES:1. Kim BT, Kim Y, Lee KS, et al. Local-
ized form of bronchioloalveolar carci-noma: FDG PET findings. AJR 1998;170:935-9.
2. Gould MK, Maclean CC, KuschnerWG , et al. Accuracy of positron emis-sion tomography for diagnosis of pul-monary nodules and mass lesions: ameta-analysis. JAMA 2001; 285:914-24.
3. Pieterman RM, van Putten JW,Meuzelaar JJ, et al. Preoperative stag-ing of non-small-cell lung cancer withpositron-emission tomography. NEJM2000; 343:254-61.
4. van Tinteren H, Hoekstra OS, SmitEF, et al. Effectiveness of positronemission tomography in the preopera-tive assessment of patients with sus-pected non-small-cell lung cancer: thePLUS multicentre randomised trial.Lancet 2002; 359:1388-93.
5. Bury T, Corhay JL, Duysinx B, et al.Value of FDG-PET in detecting re-sidual or recurrent nonsmall cell lungcancer. Eur Respir J 1999; 14:1376-80.
6. Lerut T, Flamen P, Ectors N, et al.Histopathologic validation of lymphnode staging with FDG-PET scan in
cancer of the esophagus and gastroe-sophageal junction: A prospectivestudy based on primary surgery withextensive lymphadenectomy. Ann Surg2000; 232:743-52.
7. Valk PE, Abella-Columna E, HasemanMK, et al. Whole-body PET imagingwith [18F]fluorodeoxyglucose in man-agement of recurrent colorectal can-cer. Arch Surg 1999; 134:503-11.
8. http://cms.hhs.gov/coverage/8b3-hh2.asp
9. Myers LL, Wax MK. Positron emissiontomography in the evaluation of thenegative neck in patients with oral cav-ity cancer. J Otolaryngol 1998; 27:342-7.
10. Rinne D, Baum RP, Hor G, et al. Pri-mary staging and follow-up of highrisk melanoma patients with whole-body 18F-fluorodeoxyglucose positronemission tomography: results of a pro-spective study of 100 patients. Cancer1998; 82:1664-71.
11. Kostakoglu L, Leonard JP, Kuji I, etal. Comparison of fluorine-18fluorodeoxyglucose positron emissiontomography and Ga-67 scintigraphyin evaluation of lymphoma. Cancer2002; 94:879-88.
12. http://www.cms.hhs.gov/coverage/download/8b1-g1.pdf
13. Yang SN, Liang JA, Lin FJ, et al. Com-paring whole body (18)F-2-deoxyglucose positron emissiontomography and technetium-99m me-thylene diphosphonate bone scan todetect bone metastases in patients withbreast cancer. J Cancer Res Clin Oncol2002; 128:325-8.
14. Moon DH, Maddahi J, SilvermanDH, et al. Accuracy of whole-bodyfluorine-18-FDG PET for the detec-tion of recurrent or metastatic breastcarcinoma. J Nucl Med 1998; 39:431-5.
15. Mortimer JE, Dehdashti F, Siegel BA,et al. Metabolic flare: indicator of hor-mone responsiveness in advancedbreast cancer. J Clin Oncol 2001;19:2797-803.
CORRESPONDENCE:Jac D. Scheiner, MDDepartment of Diagnostic ImagingRhode Island Hospital593 Eddy St.Providence, RI 02903Phone: (401) 444-5184Fax: (401) 444-5017e-mail: [email protected]

136Medicine and Health / Rhode Island
�Neurologic PET
Anthony F. Posteraro, MD, and Richard B. Noto, MD
Since the 1960s, functional brainimaging, using a variety of
radiopharmaceuticals, has been utilizedto non-invasively study neurologicaldiseases in vivo. The initial pharma-ceuticals used were labeled with vari-ous isotopes of radioiodine andtechnetium, allowing the pharmaceu-tical distribution to be localized usingsingle photon emission computed to-mography (SPECT).
Positron emission tomography(PET) has become a clinical realitywith recent advances in instrumenta-tion and radiopharmaceutical develop-ment. PET imaging offers markedlyimproved spatial resolution comparedto standard SPECT imaging of thebrain (4-5mm compared with 8-10mm) as well as the ability to directlyimage metabolism.1 Positron-emittingradionuclides (18F, 15O, 13N, 11C) canbe used to synthesize a variety of bio-logically important radiotracers be-cause the elements used for labelingoccur naturally in such compounds.The most widely used radiotracer, 18F-Fluorodeoxyglucose (FDG), is a glu-cose analogue that images metabolism,providing a direct evaluation of thecerebral metabolic rate for glucose. Incomparison to SPECT imaging, meta-bolic imaging combined with betterinherent spatial resolution compared toconventional SPECT perfusion scanshas revealed some extraordinary find-ings which may influence the manage-ment of patients with seizures, braintumors, dementia, movement disor-ders, and other neuropsychiatric dis-eases. In the following discussion,various applications ofPET will be reviewed withan emphasis on applica-tions useful in clinicalpractice.
TECHNIQUE
Neurologic PET re-quires some special prepa-ration and attention todetail compared to imag-
ing other areas of the body. For themajority of applications, 18F-FDG isthe primary radiopharmaceutical used.FDG is taken up in proportion to theregional cerebral metabolic rate for glu-cose, thus providing a map of cerebralmetabolic activity. Following intrave-nous administration of FDG, the pa-tient is allowed to rest quietly in a dimlylit room for 30 minutes during theuptake phase. External stimulationand cognitive processes will result inpatterns of uptake corresponding toareas of neural activity. By minimiz-ing external stimulation, the “back-ground noise” of various areas ofcortical activation can be eliminated,providing a uniform baseline for com-parison. Typically an ‘eyes and ears’open technique is used as uptake val-ues are less variable under such circum-stances.2
Other techniques used for cerebralPET imaging include perfusion imag-ing with 15O-H
2O and imaging with
radiolabeled neurotransmitters and re-
ceptor ligands. 15O-H2O is a freely dif-
fusible radiotracer and can provide im-aging of cerebral perfusion. In addition,15O has a half-life of 2 minutes, so thetracer is rapidly cleared from the patientby positron decay, allowing multiplescans to be obtained in a short periodof time. While beneficial for researchpurposes, the short half life requires anon site cyclotron and limits clinical ap-plications.3 Radiolabeled neurotrans-mitters are mostly used for researchapplications, though 18F Fluorodopa hasshown great clinical promise in its abil-ity to image the dopaminergic neu-rotransmitter system.
DEMENTIA
Dementia is usually defined as adecline in multiple cognitive functionssuch as memory, language andvisuospatial ability sufficiently severe tointerfere with daily life. There are sev-eral distinct clinical dementia and de-mentia like syndromes; the mostcommon is Alzheimer disease. PETcan be used to help distinguish differ-ent types of dementias, which may beparticularly helpful early in the course.
Alzheimer’s disease has become amajor problem as our population ages.About 8% of the population over 65will have Alzheimer disease; this rises toover 30% for people older than 85.4
Therapy tends to work best and prolongindependent living the longest whenstarted early in the course of the disease,when the clinical diagnosis is most chal-lenging. PET offers an accurate meansof evaluating patients for Alzheimer dis-ease. A recent report by the members of
Fig. 1. There is decreased interictal FDG uptake within the left temporal lobe of this patient with medicallyrefractory epilepsy (arrows). No other foci of abnormal cortical activity were localized. The patient subsequently
underwent successful left temporal lobectomy for treatment.
�
Neurologic PETimaging, used for avariety of research
applications over the lasttwo decades, is now
emerging as a powerfulclinical tool.

137Vol. 86 No. 5 May 2003
the Quality Standards Subcommittee ofthe American Academy of Neurologyconcluded that “PET scanning appearsto have promise for use as an adjunct toclinical diagnosis of Alzheimer disease.”Their review of published studies showeddiagnostic specificity of 86%-100% forF18 FDG PET.6
PET imaging in Alzheimer diseasedemonstrates decreased metabolic ac-tivity in the mesial temporal lobes aswell as the posterior temporal and pa-rietal lobes. With time this progres-sively worsens and also involves thefrontal lobes. This contrasts with the“frontal lobe dementias” such as Pickdisease, which presents with decreasedmetabolic activity in the frontal lobes,followed by decreased metabolic activ-ity in the temporal and parietal lobes.End stage Alzheimer disease and fron-tal lobe dementias have overlappingfindings, which is why brain PET ismost sensitive and specific for evaluat-ing dementia early in the disease.
BRAIN TUMORS
Primary malignant brain tumorsare mostly gliomas, with histologic graderanging from low grade astrocytomas tohigh grade tumors such as glioblastomamultiforme. In general, patients withlower grade tumors live longer whilepatients with higher grade tumors havea dismal prognosis (2% 5 year survivalfor glioblastoma multiforme).7 Gliomastend to be infiltrating heterogeneoustumors with areas of varying gradespread within the tumor mass. In addi-tion, the distribution of the tumor doesnot always correspond to the area of en-hancement or T2 abnormality seen onMRI. FDG PET, in conjunction withconventional MRI, can accurately im-age the spatial distribution of the tumoras well as determine areas of higher andlower grade tumor for better localiza-
tion at the time ofbiopsy.8
The degree ofFDG uptake withinbrain tumors is di-rectly related to tu-mor grade asdescribed by theWorld Health Orga-nization (WHO)
grades I-IV. Measurements of tumorto white matter (T:WM) and tumorto grey matter activity (T:GM) can dis-tinguish low grade (WHO grade I andII) from high grade tumors (WHOgrade III and IV). High grade tumorsare detected by a T:WM ratio greaterthan 1.5 and T:GM ratio greater than0.6 with a sensitivity of 94% and speci-ficity of 77%.9 In addition, FDG PEThas proven useful for differentiating re-current tumor from radiation necro-sis in patients with treated gliomas.
In general, high grade tumors tendto mimic the intensity of grey matteruptake while low grade tumors mimicthe intensity of white matter uptake,making co registration of images withMRI for anatomic localization necessaryfor accurate staging of brain tumorswith FDG PET. Because of the highbackground activity within the brainobserved with FDG PET, detection ofmetastatic disease to the brain is diffi-cult with recent literature giving brainPET a sensitivity of 61% for detectingcerebral metastatic disease.10 The onlyexceptions include lymphoma andmelanoma. These tumors have greaterspecific uptake than grey matter and canbe readily discerned from backgroundbrain activity.11 PET can be used to stageprimary brain lymphoma and has beenused to differentiate cerebral toxoplas-mosis from lymphoma in patients withAIDS. For most applications, contrastenhanced MRI remains a more sensi-tive screen of the CNS for metastaticlesions in patients with a primary neo-plasm elsewhere.
EPILEPSY
Epilepsy has a prevalence of 0.5%to 1.0% with rare patients having fre-quent seizures unresponsive to medi-cations. In patients with focal EEGabnormalities, a single hypometabolic
region can be identified in 55% to 80%of patients interictally using FDGPET.12 During a seizure these regionsare hyperactive. In those patients whohave medically refractory focal onsetseizures, surgical removal of the epilep-tic focus can be effective in controllingthe seizure disorder. Interictal PETand ictal perfusion SPECT imaginghave similar sensitivity and specificityfor localizing seizure foci; however,interictal imaging is easier to performand eliminates the need for hospital-ization and monitoring while waitingfor a seizure to occur.13 Because of theshort-half life of FDG, ictal PET im-aging is logistically impractical.
Pre-surgical ealuation for epilepsysurgery is the only neurologic applica-tion approved by the Centers forMedicare and Medicaid Servces(CMS) (formerly the HCFA, theHealth Care Financing Administra-tion).
MOVEMENT DISORDERS
Recently, 18F-Fluorodopa has be-come clinically available for evaluatingParkinson disease. Fluorodopa imagesthe dopaminergic neurons in the stria-tum allowing accurate objective quan-tification of nigrostriatal function.With time there is progressive loss ofdopaminergic activity within the stria-tum as Parkinson disease progresses.Findings on Fluorodopa PET imaginghave been shown to correlate with dis-ease progression as well as the likeli-hood of treatment response.14
Fluorodopa PET will likely find clini-cal utility in differentiating Parkinson-like disorders from Parkinson’s disease,as well as monitoring progression.
PET has a role only in research onHuntington’s Disease at this time.15
CONCLUSIONS
Neurologic PET imaging, used fora variety of research applications overthe last two decades, is now emergingas a powerful clinical tool. Currentlythe only CMS approved indication forPET imaging of the brain is pre-surgi-cal seizure evaluation. There is, how-ever, a body of evidence demonstratingPET’s utility in accurately evaluatingearly dementia and Parkinson disease,
Fig. 2. Transaxial, sagittal and coronal FDG PET images in a patientwith Alzheimer’s Disease showing bilateral temporo-parietal defects
(arrows). Images courtesy of Abass Alavi, MD, Hospital of theUniversity of Pennsylvania.
138Medicine and Health / Rhode Island
as well as staging and restaging braintumors. Acceptance of PET by CMSfor reimbursement has revolved notabout PET’s accuracy but whether PETdiagnosis is cost-effective and improvesclinical management compared withclinical diagnosis alone. Recent deci-sion analysis supports such a role forneurologic PET imaging and as thera-pies for dementia and other neurologicdiseases improve, PET’s role will likelyincrease as an accurate, non-invasivemeans of evaluating various neurologicdisorders.16
Anthony F. Posteraro, MD, is SeniorResident, Department of Diagnostic Im-aging, Rhode Island Hospital.
Richard B. Noto, MD, is Directorof Nuclear Medicine, Department ofDiagnostic Imaging, Rhode Island Hos-pital, and Clinical Assistant Professor ofRadiology, Brown Medical School.
REFERENCES1. Budinger TF. Future developments in
poitron emission tomography for in-corporation into the clinical sphere.Invest Radiol 1993; 28 (suppl 3): S142-3.
2. Mazziotta JC, Phelps ME, Carson RE,Kuhl DE. Tomographic mapping ofhuman cerebral metabolism: sensorydeprivation. Arch Neurol 1976; 33:523-6.
3. Van Heertum RL, Tikofsky RS. Func-tional cerebral SPECT and PET imag-ing, 3rd ed. Philedelphia PA:Lippincott Willims & Wilkins, 2000.
4. Bachman DL, Wolf PA, Linn RT. In-cidence of dementia and probablealzheimer’s disease in a general popu-lace: the Framingham study. Neurol1993; 43: 515-9.
5. Knopman DS, DeKosky ST,Cummings JL. Practice parameter:diagnosis of dementia (an evidence-based review) – report of the qualitystandards subcommittee of the Ameri-can academy of neurology. Neurol2001; 56: 1143-53.
6. Hagge RJ, Wong TZ, Coleman, RE.Positron emission tomography braintumors and lung cancer. Radiol ClinN Amer 2001; 39: 871-81.
7. Pirotte B, Goleman S, Bidaut LM. Useof positron emission tomography(PET) in stereotactic conditions forbrain biopsy. Acta Neurochir1995;134: 79-82.
8. Delbeke D, Meyerowitz C, LapidusRL. Optimal cutoff levels of F-18fluorodeoxyglucose uptake in the dif-ferentiation of low-grade from highgrade brain tumors with PET. Radiol1995; 195: 47-52.
9. Rohren EM, Provenzale JM, BarboriakDP, Coleman RE. Screening for cere-bral metastases with FDG PET in pa-tients undergoning whole-bodystaging of non-central nervous systemmalignancy. Radiol 2003; 226: 181-7.
10. Roelcke U, Leenders KL. Positronemission tomography in patients withprimary CNS lymphomas. J Neuro-Oncol 1999; 43: 231-6.
11. Henry TR, Sutherling WW, Engel JJr. Interictal cerebral metabolism inpartial epilepsies of neocortical origin.Epilepsy Res 1991; 10: 174-82.
12. Ho SS, Berkovic SF, Berlangieri SU,et al. Comparison of ictal SPECT andinterictal PET in the presurgical evalu-ation of temporal lobe epilepsy. AnnNeurol 1995; 37: 738-45.
13. Brooks DJ. PET studies and motorcomplications in Parkinson’s. TrendsNeurosci 2000; 23(10 Suppl): S101-8.
14. Hayden MR, HewittK, Stoessl AJ.The combined use of positron emis-sion tomography and DNA polymor-phisms for preclinical detection ofHuntington’s disease. NEJM 1987;317: 3823.
15. Silverman DHS, Gambhir SS, HuangHW. Evaluating early dementia withand without assessment of regionalcerebral metabolism by PET: A com-parison of predicted costs and benefits.J Nuc Med 2002; 43: 253-66.
CORRESPONDENCE:Anthony F. Posteraro, MDDepartment of Diagnostic ImagingRhode Island Hospital593 Eddy St.Providence, RI 02903Phone: (401) 444-5184Fax: (401) 444-5017e-mail: [email protected]

139Vol. 86 No. 5 May 2003
�Cardiac Applications of Positron Emission Tomography (PET)
Richard B. Noto, MD
One of the first clear clinical indi-cations for Positron Emission
Tomography (PET) imaging was inthe evaluation of cardiac disease. PETtechniques to evaluate both myocardialperfusion and myocardial viability havebeen available for several years and havebeen proven to be accurate and reli-able. While cardiac PET has not seenthe growth in volume that has occurredin oncologic PET, there is tremendouspotential for future applications of car-diac PET and it is likely that PET willplay a role in the evaluation of a vari-ety of cardiac disease processes in thefuture.
Coronary blood flow can be evalu-ated by PET with a variety of tracers.In research applications, both O-15water and N-13 ammonia have beenused for many years to evaluate myo-cardial perfusion. O-15 water is prob-ably the most accurate tracer availablefor quantifying myocardial perfusion.This radiopharmaceutical freely dif-fuses across cell membranes in themyocardium giving a highly accuratereflection of myocardial blood flow.However, because of rapid equilibra-tion of the tracer between tissue andvascular spaces, sophisticated tech-niques to separate myocardial fromblood pool activity are necessary.1
N-13 ammonia is an excellenttracer for imaging myocardial bloodflow and, after passively diffusing intothe myocardium in proportion to per-fusion, is incorporated in myocardialcells in the form of glutamine. Becauseof its high extraction and target to back-ground ratio, N-13 ammonia yields thebest imaging quality of the agents avail-able for PET myocardial perfusion im-aging and can also be used to quantifymyocardial blood flow.1 However, bothO-15 water and N-13 ammonia arerarely utilized in the clinical setting be-cause of their short half-life and needfor cyclotron production. The half-lifeof O-15 is only 110 seconds and thehalf-life of N-13 is 10 minutes, mean-ing that they decay very quickly to lev-
els that are too low for imaging pur-poses. These very short half-lives limitthe utilization of these tracers to facili-ties that have on-site cyclotrons imme-diately adjacent to their PET scanners.
Because of the logistical issues re-lated to the short half-lives, the mostcommonly used tracer for PET myocar-dial perfusion imaging is neither O-15water nor N-13 ammonia. Instead, ru-bidium-82 is the agent that has provenmost practical in some centers. Whilerubidium-82 also has a very short half-life of 76 seconds, it is produced fromstrontium-82 via a commercially avail-able generator which can be purchasedand kept on site. Each generator canproduce adequate doses of rubidium-82for about a month. Therefore, there isno need for an on-site cyclotron. Ru-bidium-82 is approved by the FDA.While the generators are expensive, theymay prove cost-effective for sites that areperforming high volumes of myocardialperfusion studies.2
Like thallium-201, rubidium-82 isan analogue of potassium. It is rapidlyand efficiently extracted from the bloodpool by the myocardium and localizesin the myocardium in proportion to re-gional coronary blood flow. Because ofits extremely short half-life, it is possibleto give large doses (50-60 mCi) of ru-bidium-82 for each portion of the study.Combining this with the high imagingquality of PET cameras, excellent myo-cardial perfusion images can be obtainedin very short acquisition times.2 Becauseof the rapid acquisition time and the factthat the rubidium-82 activity decays sorapidly, it is possible to perform a rou-tine rest/stress myocardial perfusion scanin less than one hour (Figure 1).
In most studies, PET myocardialperfusion imaging has demonstrated ahigh sensitivity for coronary artery dis-ease in the range of 85-95% as well asspecificity in the range of 80-90%.3,4
In studies that have compared PET andSPECT myocardial perfusion imaging,PET has usually been shown to bemore accurate, especially with regard
to specificity, although the differencesare not great.5 Advantages of PETimaging over SPECT include highercount rates and better image quality,superior attenuation correction algo-rithms, and greater ability to quantifymyocardial blood flow and flow re-serve. Studies have also shown moreaccurate localization of coronary arterydisease and greater interpreter confi-dence with PET.
While PET has some advantagesover SPECT for myocardial perfusionimaging and is probably the best non-invasive study to evaluate myocardialperfusion, the use of PET for this pur-pose has not been widespread. Thishas clearly been because of cost con-siderations; in addition to the cost ofthe PET camera, the radiopharmaceu-tical costs are significant even if oneuses a rubidium generator. However,recent studies have indicated that PET,with its high specificity for coronaryartery disease, can be cost-effective, es-pecially in those with an intermediatepre-test probability. For those withhigh pre-test likelihood of coronary ar-tery disease, coronary angiography re-mains the most cost-effective choice.6
The other primary application ofPET in cardiac disease is the evalua-tion of myocardial viability. In patientswith coronary artery disease leading toleft ventricular dysfunction and heartfailure, the decision as to whether toattempt revascularization can be a dif-ficult one. Patients with severe left ven-tricular dysfunction have increasedmorbidity and mortality, but these pa-tients are also at higher risk of compli-cation from surgical revascularizationprocedures. Therefore, it is importantto have a non-invasive study that canaccurately predict which patients willhave significant improvement in leftventricular function afterrevascularization. At the present time,PET is the most accurate non-invasiveprocedure available for this purpose.
The PET evaluation of myocardialviability is dependent on the varying

140Medicine and Health / Rhode Island
�
The positron emittingradiopharmaceutical F-18 fluorodeoxyglucose
(FDG) is ideal forevaluating glucosemetabolism in the
myocardium.
methods of energy metabolism in theheart in different circumstances. Innormally perfused myocardium, oxida-tive metabolism of fatty acids is thepredominant means of energy produc-tion in the fasting state. In patientsrecently fed, glucose becomes the pre-dominant metabolic substrate. If myo-cardial ischemia is present, oxidativemetabolism is reduced and anaerobicglycolysis of glucose is the primarymeans of energy production.
The positron emitting radiophar-maceutical F-18 fluorodeoxyglucose(FDG) is ideal for evaluating glucosemetabolism in the myocardium. FDGis transported into myocytes by glucosetransporters, GLUT-4 and GLUT-1. Inthe myocyte, FDG undergoes phos-phorylation by hexokinase to FDG-6-phosphate. The FDG-6-phosphateundergoes little further metabolismand effectively becomes trapped in themyocyte in proportion to glucose up-take.7
The main purpose of FDG imag-ing in the heart is to identify dysfunc-tional but viable myocardium. Theterm “hibernating myocardium” ap-plies to areas of the myocardium that
have chronically reduced blood flow atrest and impaired contractile function,but maintain viability. The term “myo-cardial stunning” refers to episodes ofacute decreased myocardial blood flowand ischemia that may lead to myo-cardial dysfunction due to reperfusioninjury. Repeated episodes of myocar-dial stunning may also cause abnor-malities of contractile function despitethe presence of viable myocardium andmay represent a continuum with “hi-bernating myocardium.” These viableareas will often return to normal func-tional status if a revascularization pro-cedure is performed and therefore it is
very important to differentiatepatients with dysfunctionalbut viable myocardium fromthose with scar that will notimprove despiterevascularization.
While cardiac PET withFDG is probably the most use-ful non-invasive tool for mak-ing this distinction, logisticalissues make performance andinterpretation of cardiac FDGstudies difficult. In particu-lar, the myocardial uptake ofFDG is very dependent on theserum glucose level. In thefasting state, there is little over-all uptake of FDG in the myo-cardium because of thepredominant fatty acid me-tabolism and the uptake thatis present is often heteroge-neous with relatively less nor-mal uptake in the septum thanin the lateral wall. To combatthis problem, an oral load ofglucose can be administered to
the patient before the FDG to increaseinsulin levels; insulin stimulates themyocardial uptake of FDG which usu-ally improves image quality. However,excessive levels of serum glucose maycompete with FDG for myocardialuptake and thereby decrease myocar-dial FDG uptake. In an ideal case, theserum glucose should be maintainedbelow 140 mg/dL and it may be nec-essary to administer insulin intrave-nously to titrate the glucose to thecorrect level. Even with these mea-sures, it is often difficult to achievemaximal cardiac FDG uptake and im-age quality in diabetic patients. Otherapproaches to maximizing myocardialFDG uptake include the use of thehyperinsulinemic-euglycemic clampand, more recently, the use of nicotinicacid derivatives.8
Imaging techniques for myocar-dial viability PET usually include ascan to evaluate myocardial perfusionas well as a myocardial FDG scan. Theperfusion scan is usually a resting studyperformed either with SPECT agentslike Tc-99m sestamibi or Thallium-201 chloride or a perfusion PET scanperformed with one of the
Figure 1. Stress-Rest rubidium-82 perfusion images in a 69 year old male with known CAD and chest pain. Imagesreveal reversible perfusion defects in the apex, inferior wall, septum and lateral wall indicative of ischemia.

141Vol. 86 No. 5 May 2003
radiopharmaceuticals described abovelike rubidium-82. The perfusion im-ages are then compared with the FDGimages to evaluate the amount of glu-cose uptake in regions of decreasedmyocardial perfusion.
The classic pattern described in thecase of viable, but hibernating myocar-dium is the “perfusion-metabolism mis-match” (Figure 2). In this circumstance,the resting perfusion to a segment of themyocardium is reduced, but there is pre-served FDG uptake. The FDG uptakein this segment may be equal to the restof the myocardium or greater than themyocardial uptake elsewhere in theheart, but in either case is indicative ofviable myocardium. The relatively in-creased FDG uptake is felt to be due togreater glucose metabolism in the hiber-nating segment. Areas of “perfusion-metabolism mismatch” usually showimprovement in contractility afterrevascularization procedures.
In the case of scarring, the perfu-
sion and the FDG areboth reduced, result-ing in a “perfusion-me-tabolism match”. Thereduction in uptake ofthese tracers may ei-ther be severe in thecase of transmuralinfarctions or mild inthe case of non-trans-mural MIs. In general,segments that showeda “perfusion-metabo-lism match” do notshow significant im-provement in functionafter revascularization.It is also possible tohave a “partial mis-match” where FDGuptake is decreased butnot as much as perfu-sion and this likely rep-resents a combinationof scar and hibernatingmyocardium .7,9
Many studieshave looked at the ac-curacy of PET in pre-dicting functionalimprovement afterrevascularization pro-
cedures. Overall, the positive predic-tive value for significant functionalrecovery with a “mismatch” pattern isabout 75%, the negative predictivevalue of a “match” pattern is about85%, and the accuracy of PET in pre-dicting functional recovery is about80% .9-14 Improvement afterrevascularization sometimes takemonths to occur. In comparison toresting thallium-201 scintigraphy,which is also used to determine viablemyocardium, PET shows viability inapproximately 30-45% of segmentsthat show fixed thallium defects.1
In addition, PET evidence of vi-ability has been shown in several stud-ies to be an excellent indicator of eventrate post-revascularization.7,10,14 Inthose with PET evidence of significantviable, but dysfunctional myocardium,the rate of serious cardiac events wasmuch lower in patients who were sub-sequently treated with revascularizationrather than medical therapy. In those
without viable, but dysfunctional myo-cardium by PET, there was no signifi-cant difference between the cardiacevent rate between the revascularizationand the medical therapy groups. Thissuggests that PET can be accuratelyused to suggest which patients wouldbe amenable to revascularizationtherapy.
In summary, PET has tremendouspotential for cardiac applications in thenear future. While it has already beenshown to be very useful as a perfusiontracer, costs associated with the studyhave limited the use of PET in myo-cardial perfusion imaging. In deter-mining myocardial viability, FDG PETappears to be an accurate, non-inva-sive predictor of improvement afterrevascularization and should play anincreasingly important role in decid-ing which patients undergorevascularization procedures in the fu-ture.
ACKNOWLEDGEMENT: Figures 1 and 2were provided by Dr. Josef Machac,New York University–Mt. Sinai Medi-cal Center.
REFERENCES1. Schwaiger, M, Hutchins, GD. Evalu-
ation of coronary artery disease withpositron emission tomography. SeminNucl Med 1992; 22:210-23.
2. Tamaki, N, Ruddy, TD, deKamp, R,Beanlands, RSB. Myocardial perfu-sion. In: Wahl, RL, ed. Principles andPractice of Positron Emission Tomogra-phy. Philadelphia: Lippincott, Will-iams & Wilkins, 2002: 320-33.
3. Schelbert H, Wisenberg G, Phelps M,et al. Noninvasive assessment of coro-nary stenoses by myocardial imagingduring pharmacologic coronary va-sodilation. VI: Detection of coronaryartery disease in man with intravenous13-NH3 and positron computed to-mography. Am J Cardiol 1982;49:1197-207.
4. Williams BR, Mullani NA, JansenDE, Anderson BA. A retrospectivestudy of the diagnostic accuracy of acommunity hospital-based PET cen-ter for the detection of coronary ar-tery disease using rubidium-82. J NuclMed 1994; 35:1586-92.
5. Go RT, Marwick TH, MacIntyre WJ,et al. A prospective comparison of ru-bidium-82 PET and thallium-201SPECT myocardial perfusion imaging
Figure 2 - Stress and rest rubidium-82 PET myocardial perfusionimages and FDG PET images in the same patient. The perfusion
images show extensive partially reversible perfusion defects in theseptal, inferior, lateral, and antero-apical regions. The FDG
images show areas of perfusion-metabolism mismatch in thelateral and infero-basal regions (arrows) indicating hibernating but
viable myocardium

142Medicine and Health / Rhode Island
utilizing a single dipyridamole stressin the diagnosis of coronary artery dis-ease. J Nucl Med 1990; 31:1899-905.
6. Patterson RP, Eisner RL, Horowitz SF.Comparison of cost-effectiveness andutility of exercise ECG, single photonemission computed tomography,positron emission tomography, andcoronary angiography for diagnosis ofcoronary artery disease. Circulation1995; 91:54-65.
7. Beanlands RSB, Ruddy TD, MaddahiJ. Myocardial viability. In: Wahl, RL,ed. Principles and Practice of PositronEmission Tomography. Philadelphia:Lippincott, Williams & Wilkins,2002:334-50.
8. Parker JA. Cardiac nuclear medicinein monitoring patients with coronaryheart disease. Semin Nucl Med 2001;31: 223-37.
9. Bax JJ, Visser FC, Elhendy A, et al.Prediction of improvement of regionalleft ventricular function after
revascularization using different per-fusion-metabolic criteria. J Nucl Med1999; 40:1866-73.
10. Di Carli MF, Asgarzadie F, SchelbertHR, et al. Quantitative relation be-tween myocardial viability and im-provement in heart failure symptomsafter revascularization in patients withischemic cardiomyopathy. Circulation1995; 92:3436-44.
11. Shivalkar B, Maes A, Borgers M, et al.Only hibernating myocardium invari-ably shows early recovery after coro-nary revascularization. Circulation1996; 94:308-15.
12. Vom Dahl J, Altehoefer C, SheehanFH, et al. Effect of myocardial viabil-ity assessed by technetium-99m-sestamibi SPECT andfluorine-18-FDG PET on clinical out-come in coronary artery disease. J NuclMed 1997; 38:742-8.
13. Gambhir SS, Czernin J, SchwimmerJ, et al. A tabulated summary of theFDG PET literature. Cardiac applica-tions: Myocardial viability. J Nucl Med2001; 42:70S-1S.
14. Schelbert HR. 18-F-Deoxyglucose andthe assessment of myocardial viability.Semin Nucl Med 2002; 32:60-9.
Richard B. Noto, MD, is Directorof Nuclear Medicine, Department ofDiagnostic Imaging, Rhode Island Hos-pital, and Clinical Assistant Professor,Brown Medical School.
CORRESPONDENCE:Richard B. Noto, MDDepartment of Diagnostic ImagingRhode Island Hospital593 Eddy St.Providence, RI 02903Phone: (401) 444-5184Fax: (401) 444-5017e-mail: [email protected]

143Vol. 86 No. 5 May 2003
�Future Advances and Applications in Positron
Emission Tomography
Don Yoo, MD, and Richard B. Noto, MD
While positron emission tomog-raphy (PET) is already a useful
clinical tool in a variety of areas, manyadvances are on the horizon which willfurther improve this technology, in-cluding PET/CT (positron emissiontomography/computed tomography)technology, better imaging, and newradiotracer agents.
PET/CT is one of the most excit-ing technologic advances in radiology.PET alone gives physiologic informa-tion but is limited by spatial resolutionand anatomic landmarks. CT alonegives anatomic information but can-not give functional or metabolic infor-mation. PET/CT is often describedas fusion or hybrid imaging because itcombines the advantages of these twodifferent imaging modalities and incor-porates their features into a new com-posite imaging modality. Thecomposite image, containing overlayedvoxels of data, produces an image re-flecting both biologic and anatomicprocesses occurring at the molecularlevel in internal structures .1,2
A whole-body PET/CT scan takesabout thirty minutes to perform. Thedata are integrated to produce a com-posite image. The quality of the im-ages is higher than a conventional PETscan alone because the incorporationof CT improves attenuation correctionresulting in a more accurate image.The study is also performed faster be-cause the use of CT algorithms allowsfor faster attenuation correction.1
Because this is a new technology,research directly comparing the sensi-tivity and specificity of PET/CT withPET and CT performed separately (in-terpretation performed with both PETand CT images) is not yet available.The costs of a combined scanner costmore than each purchased separately.
New crystal technology has beencrucial to the advancement of PETimaging. Crystals convert high-energyphotons into flashes of light that are
recorded, transmitted, and assembledinto images. In order for a PET scanimage to be produced, an incident pho-ton has to interact with a detector caus-ing a light flash detected by aphotomultiplier tube behind the crys-tal. Smaller crystals allow a greaternumber of detectors, increasing theresolution. The most commonly usedcrystals have been NaI (sodium iodide)or bismuth germinate oxide (BGO).BGO crystal based PET scanners arecurrently the most common. The ad-vantage of the BGO crystal is that ithas the best efficiency in stopping theincident photon (stopping power) butit suffers from poor light output, longphotoflourescent decay times and poorenergy resolution. New LSO (lutetiumoxyorthosilicate) and GSO (gado-linium oxyorthosilicate) crystals havebeen developed which, while havingslightly poorer stopping power, morethan compensate with better light out-put, markedly shorter photoflourescentdecay times, and superior energy reso-lution, producing a better image in lesstime.3-5
New radiotracers have emergedthat will increase the use of PET. 11C-methionine has shown encouragingresults in a variety of tumors becauseamino acid metabolism is increased dueto an increased protein synthesis rate.11Carbon labeled tracers have shownsome promise. The limitation is thehalf-life of 20 minutes, requiring anon-site cyclotron. Another 11C labeledagent, 11C-choline has shown promisein prostate and bladder cancer. 11C-choline is a component of phosphati-dylcholine, one of the essentialphospholipids in the cell membrane.The advantage of 11C–choline is thatit is taken up by cancer cells by activetransport, retained by phosphorylationand has minimal urinary excretion.
Until on-site cyclotrons becomemore economically feasible, tracersbased on 18fluorine are the ligands of
choice dues to the relatively long half-life of 110 minutes. Recently a new flu-orinated choline derivative,18F-fluorocholine (FCH), should bevery useful in oncology applications.FCH has been shown to mimic 11C-choline in cultured human prostate cells.FCH also has potential for imagingbrain tumors. FCH may be more use-ful than FDG in the brain because FCHhas much less uptake in normal braincortex. FCH will have the potential toevaluate many other tumors such aslung, colon, and esophageal cancers inwhich 11C-methionine has been shownto be effective. Other new promisingtracers such as fluoroethyl tyrosine(FET) and fluorodeoxythymidine(FLT) have been studied. FLT has beenshown in studies to accumulate morespecifically in tumor cells than FDG.6-9
Medicare reimburses PET forseven types of cancers: lung, lym-phoma, head and neck (excluding thy-roid), colorectal, melanoma,esophageal and breast. It also reim-burses PET for two non-oncologicuses: myocardial viability and seizurefocus. However, the use of PET is be-ing studied for many more tumors andnon-oncologic applications. Futureapplications include oncologic imag-ing applications in urology, endocrinol-ogy, and gynecology. Futurenon-oncologic applications includeAlzheimer’s disease (AD), psychiatricdisorders, inflammatory diseases, infec-tions, and, finally, gene expression.
GU CANCER
The genitourinary system will beone of the new frontiers for PET. Interms of metastatic prostate cancer, PEThas shown great promise in the preop-erative evaluation of distant lymph nodeinvolvement. FCH has shown abouttwice the sensitivity of FDG, 70% vs.34%.10 In a recent study, in which 10patients were undergoing androgen ab-lation for metastatic prostate cancer, the

144Medicine and Health / Rhode Island
decrease in size of tumor on CT andPSA levels corresponded to a decreasein PET uptake in the primary tumorand metastatic sites.11 In the future, PETmay be most helpful in evaluating thetumor response to treatment and deter-mining the prognosis of the patient earlyin treatment, especially with new trac-ers .10-14
For patients with renal cell carci-noma, in a few recent studies, FDG-PET has been shown to be as accurateas CT (the current gold standard) inthe primary diagnosis and better thanCT in monitoring the response oftreated renal cell carcinoma. In theprimary diagnosis of renal cell carci-noma in two different studies, FDG-PET had a sensitivity of 77% (20/26patients) and 94% (15/16 patients) inhistologically proven renal cell carcino-mas .15 In 21 patients with renal cellcarcinoma who were treated withinterleukin-2 based therapy, PET wasable to identify progression in 100%(10/10 patients) while CT only cor-rectly identified progression in 70% (7/10 patients).16 One of the main ad-vantages of PET was its ability to dif-ferentiate between recurrent tumor inthe renal fossa and radiation necrosis.In the future, PET especially withPET/CT fusion will have an expand-ing role in the diagnosis and manage-ment of renal cell carcinoma.
FDG-PET has also been shown tobe useful in the diagnosis and manage-ment of testicular cancer. PET has beenshown to be more sensitive than CT indiagnosing retroperitoneal disease inpatients initially diagnosed with testicu-lar cancers. In a study of 37 patientsinitially diagnosed with stage I or IIseminomas and nonseminomas, PETwas more accurate in staging than CT,92% vs. 78% respectively.17 PET canhave an important role in monitoringthe response to treatment. PET allowsthe differentiation between involutingtissue and residual or recurrent tumor.
THYROID
In endocrinology, the largest em-phasis has been on the use of PET forthyroid cancer. PET has shown to beeffective in imaging patients with dif-ferentiated thyroid cancer who present
with elevated thyroglobulin levels anda negative 131Iodine scan. Progressionin differentiated thyroid cancer occursslowly with relatively good prognosiseven after metastatic disease has beendiscovered provided that appropriatetreatment is rendered. Patients withmetastatic disease and negative 131I scanare usually not treated with high-doseradioiodine. Usually thyroid cancermetastases that are not iodine avidhave to be removed surgically if theycan be localized. That is where PETcan prove valuable for detection of bothlocal recurrence and distant metastases.One recent study showed that out of64 patients with histologically provendifferentiated thyroid cancer who hadnegative 131I scans and elevated thyro-globulin levels, 44 had positive abnor-mal PET uptake. 34 out of 44 patientswere shown to have a true positive PETstudy. Treatment was changed in 19out of the 34 patients with additionalsurgery performed in 18 patients. PETcan be valuable in patients with differ-entiated thyroid cancer who presentwith increased thyroglobulin levels andnegative 131I scan because it allows sur-gical treatment for select patients,which is often curative.18
In the future, PET and 131I scanmay play complementary roles in thedetection of recurrent or metastaticdifferentiated thyroid cancer. The rea-son for this is that recent studies haveshown that poorly differentiated thy-roid cancer is often negative for 131Iscan and positive for PET while highlydifferentiated thyroid cancer is positivefor 131I scan and negative for PET.Glucose metabolism is more likely tobe increased in poorly differentiatedthan in well differentiated thyroid can-cer, whereas radioactive iodine uptakeis more likely to be preserved in welldifferentiated thyroid cancer. Onestudy has shown that PET has a distri-bution pattern similar to 201thallium
even though they have different mecha-nisms of uptake. PET has much bet-ter image quality and sensitivity than201Tl scan. Thus for metastatic diseaseafter total thyroidectomy, PET and 131Iscan will likely play complementaryroles, while a 201Tl scan may not benecessary as it has the same distribu-tion of uptake as in PET.19
GYNIn terms of gynecologic tumors,
FDG-PET has been examined forevaluating cervical and ovarian cancer.Studies comparing PET with CT andMRI have been performed. A recentstudy examined 35 cervical cancer pa-tients with stage IB or II based onFIGO (International Federation ofGynecology and Obstetrics) staging,comparing MRI and PET with histo-logic findings after radical hysterec-tomy. Sensitivity and specificity was91% and 100% with PET comparedto 73% and 83% with MRI.20 Similarresults have been shown on studiescomparing PET and CT.21
In patients with rising serummarkers such as CA 125 where ovariancancer is suspected, PET has beenshown to be of some benefit. In onerecent study, PET results were com-pared with the results of conventionalimaging and CA125 levels as well assurgical findings and clinical 6 monthfollow-up. PET showed a sensitivityof 80% (16/20 patients), a specificityof 100% (5/5 patients) and an accu-racy of 84% (21/25 patients) for thediagnosis of recurrent ovarian cancer.CT had a sensitivity of 55% (11/20patients), specificity of 100% (5/5 pa-tients) and accuracy of 64% (16/25patients). PET detected recurrent le-sions in seven of nine patients in whomconventional imaging was falsely nor-mal.22
NEUROLOGY
PET has shown promise in diag-nosing Alzheimer’s disease (AD.Clinically diagnosing dementia early inpatients who exhibit some cognitivedecline is extremely challenging. PEThas been shown in studies to have sen-sitivity of 83-96% and specificity of55–70% based on autopsy. PET is
�
New radiotracers haveemerged that will
increase the use of PET.

145Vol. 86 No. 5 May 2003
superior to conventional SPECT tech-niques for the early diagnosis of AD.Currently, PET is not reimbursed byMedicare for the diagnosis of AD, butthis will likely change, with the devel-opment of better treatments for AD.
Psychiatric disorders have been afertile ground for PET research, butPET has not yet been proven clinicallyeffective in evaluating psychiatric con-ditions. This may in part be due tothe clinical heterogeneity of many psy-chiatric disorders. With various dif-ferent experimental PET tracers, it ispossible to evaluate a variety of neu-rotransmitter systems with the dopam-ine, serotonin, gamma-aminobutyricacid (GABA), and opiate systems mostextensively studied to this point. PETresearch has shown abnormalities ofneuroreceptor uptake in a variety ofdiseases and it is anticipated that PETstudies of receptors and transporterswill demonstrate valuable informationin the years ahead. One promising areaof PET research in psychiatry is antip-sychotic drug occupancy studies whichmay be useful in better defining effec-tive and patient-specific medicationdoses with fewer side effects based onreceptor occupancy levels.
MISCELLANEOUS
PET has also shown potential forimaging inflammation and infection.FDG not only collects in tumors butin activated white blood cells such asgranulocytes and macrophages thatconsume a lot of glucose to fight in-fection. New studies are being per-formed for using PET to diagnosis andmonitor inflammatory bowel disease .23
In contrast to other agents for imag-ing infection, FDG has no normalbone marrow uptake. This is particu-larly useful in evaluating hip prosthe-ses for infection versus loosening.24 Inthe future, PET may replace 111indiumwhite blood cell and 67gallium scans forinfection. In patients with fever ofunknown origin or unknown sites ofinfection, PET/CT may be used to findand accurately localize an infection inany part of the body.
One of the most exciting futureapplications of PET may be in genetherapy. Currently more than 200 gene
therapy trials are being performedworldwide. Many of these trials arestudying herpes simplex virus thymi-dine kinase (HSV1-tk) marker gene.In these trials HSV1-tk marker gene isplaced into tumors by retroviral or ad-enoviral gene transfer. HSV1-tkmarker gene has been used as a targetfor nucleoside prodrug activation forherpes infection. PET has the uniqueability to noninvasively demonstrate invivo gene expression. 18F labelednucleoside analogs such as acyclovir,ganciclovir, and penciclovir allow PETto image HSV1-tk marker gene. There-fore as a clinical tool, PET may be usedin the future to safely monitor the effi-cacy of clinical gene therapy trials. Thefuture in gene therapy is limitless. Forexample gene therapy in prostate can-cer has been studied. In a recent study,PET was able to successfully demon-strate the expression of HSV1-tkmarker gene in severe combined im-munodeficient mice with prostate tu-mor xenograft using fluorinatedpenciclovir as a radiotracer .25-27
The future of imaging will be acombination of functional and ana-tomic imaging.
PET and PET/CT will have manynew oncologic and non-oncologic ap-plications. PET is in its infancy withunlimited potential for growth due tofuture advances in PET technology andnew radiopharmaceuticals.
REFERENCES1. Hany TF, Steinert HC, Goerres GW,
et al. PET diagnostic accuracy: im-provement with in-line PET-CT sys-tem: initial results. Radiol 2002;225:575-81.
2. Sandrick K. Hybrid PET/CT capturesbest of both modalities. Supplementto Diagnostic Imaging 2002; 2-4.
3. Melcher CL. Scintillation crystals forPET. J Nucl Med 2000 41;1051-5.
4. New developments in PET instrumen-tation: quo vadis PET? J Nucl Med2001 42:1831-2.
5. Chatziioannou AF, Cherry SR, Shao Y,et al. Performance evaluation ofmicroPET: A high-resolution lutetiumoxyorthosilicate PET scanner for ani-mal imaging. J Nucl Med 1999;40:1164-75.
6. Roivainen A, Forsback S, Gronroos T,et al. Blood metabolism of [methyl-11C]choline: implications for in vivo
imaging with positron emission tomog-raphy. Eur J Nucl Med 2000; 27:25-32.
7. Price DT, Coleman RE, Liao RP, et al.Comparison of [18 F]fluorocholine and[18 F]fluorodeoxyglucose for positronemission tomography of androgen de-pendent and androgen independentprostate cancer. J Urol 2002; 168:273-80.
8. DeGrado TR, Baldwin SW, Wang S, etal. Synthesis and evaluation of (18)F-labeled choline analogs as oncologicPET tracers. J Nucl Med 2001;42:1805-14.
9. Hara T, Kosaka N, Kishi H. Develop-ment of (18)F-fluoroethylcholine forcancer imaging with PET: synthesis,biochemistry, and prostate cancer im-aging. J Nucl Med 2002; 43:187-99.
10. Hoh CK, Seltzer MA, Franklin FJ, etal. Positron emission tomography inurologic oncology. J Urol 1998;159:347-56.
11. Oyama N, Akino H, Suzuki Y, et al.PET for evaluating the change of glu-cose metabolism in prostate cancer af-ter androgen ablation. Nucl MedCommun 2001; 22:963-9.
12. Effert PJ, Bares R, Handt S, et al. Meta-bolic imaging of untreated prostate can-cer by positron emission tomographywith 18fluorine-labeled deoxyglucose.J Urol 1996; 155:994-8.
13. Nunez R, Macapinlac HA, Yeung HW,et al. Combined 18F-FDG and 11C-methionine PET scans in patients withnewly progressive metastatic prostatecancer. J Nucl Med 2002; 43:46-55.
14. Hara T, Kosaka N, Kishi H. PET im-aging of prostate cancer using carbon-11-choline. J Nucl Med 1998;39:990-5.
15. Bachor R, Kotzerke J, Gottfried HW.Positron emission tomography in diag-nosis of renal cell carcinoma [German].Urologe A 1996; 35:146-50.
16. Hoh C, Figlin R, Belldegrun A. Evalu-ation of renal cell carcinoma with wholebody PET. J Nucl Med 1996; 37:141P.
17. Albers P, Bender H, Yilmaz H, et al.Positron emission tomography in theclinical staging of patients with stage Iand II testicular germ cell tumors. Urol1999;53:808-11.
18. Schluter B, Bohuslavizki KH, Beyer W,et al. Impact of PET on patients withdifferentiated thyroid cancer whopresent with elevated thyroglobulin andnegative 131I scan. J Nucl Med 2001;42:71-6.
19. Shiga T, Tsukamoto E, Nakada K,Morita K. Comparison of (18)F-FDG,(131)I-Na, and (201)Tl in diagnosisof recurrent or metastatic thyroid car-

146Medicine and Health / Rhode Island
cinoma. J Nucl Med 2001; 42:414-9.20. Reinhardt MJ, Ehritt-Braun C,
Vogelgesang D, et al. Metastaticlymph nodes in patients with cervicalcancer: detection with MR imagingand PET. Radiol 2001; 218:776-82.
21. Sugawara Y, Eisbruch A, Kosuda S, etal. Evaluation of PET in patients withcervical cancer. J Nucl Med 1999;40:1125-31.
22. Torizuka T, Nobezawa S, Kanno T, etal. Ovarian cancer recurrence: role ofwhole-body positron emission tomog-raphy using 2-[fluorine-18]-fluoro-2-deoxy- D-glucose. Eur J Nucl Med MolImaging 2002; 29:797-803.
23. Kresnik E, Gallowitsch HJ, MikoschP, et al. (18)F-FDG positron emissiontomography in the early diagnosis ofenterocolitis: preliminary results. EurJ Nucl Med Mol Imaging 2002;29:1389-92.
24. Manthey N, Reinhard P, Moog F, et al.The use of [18 F]fluorodeoxyglucosepositron emission tomography to dif-ferentiate between synovitis, looseningand infection of hip and knee prosthe-ses. Nucl Med Commun 2002; 23:645-53.
25. Blasberg R. PET imaging of gene ex-pression. Eur J Cancer 2002; 38:2137-46.
26. Nichol C, Kim EE. Molecular imag-ing and gene therapy. J Nucl Med2001; 42:1368-74.
27. Boerman OC, Oyen WJ, CorstensFH. Progress in gene therapy: Seeingis believing. J Nucl Med 2001;42:1235-7.
Don Yoo, MD, is Senior ResidentDepartment of Diagnostic Imaging,Rhode Island Hospital.
Richard B. Noto, MD, is Directorof Nuclear Medicine, Rhode Island Hos-pital, and Assistant Professor (Clinical),Department of Diagnostic Imaging,Brown Medical School.
CORRESPONDENCE:Richard B. Noto, MDDepartment of Diagnostic ImagingRhode Island Hospital593 Eddy St.Providence, RI 02903Phone: (401) 444-5184Fax: (401) 444-5017e-mail: [email protected]
ForthcomingBlood-Borne Pathogens
A CME Issue
The June 2003 Medicine & Health/Rhode Island will feature Blood-Borne Pathogens, an issue guest-edited by Marguerite Neill, MD
Brown Medical School is accredited by the Accreditation Council forCommunity Medical Education (ACCME) to provide ContinuingMedical Education for Physicians.
Brown Medical School designated this educational activity for amaximum of 2 hours in Category 1 credit towards the AMAPhysicians⤙ Recognition Award.
Each physician should claim only those hours of credit that he/sheactually spent in the educational activity.

147Vol. 86 No. 5 May 2003
In Rhode Island, health care provid-ers and health care facilities propos-
ing to undertake major capital invest-ment for new high-cost medicalequipment must receive certificate ofneed approval (CON).1 CON is apublic review process that assesses thecommunity need and affordability ofthe proposed investment. One of thepurposes of the CON is to avoid thecostly duplication of high-cost medicalequipment. For tertiary care services,assuring the quality of the new serviceis a key purpose of CON review.
Positron Emisson Tomography(PET) is a capital-intensive diagnosticprocedure in which very small amountsof radiotracers are injected and sensi-tive imaging equipment is used to de-tect biochemical and physiologicalreactions in the human body. A majorapplication of this technology is for thedetection, staging, and monitoring ofcancer because tumor cells show highuptake of some radiotracers.2 Whenthe Department of Health reviewedPET, it looked at machines costing ap-proximately $1.7 million, and consid-ered $1700 the average insurancereimbursement per scan.
PET is subject to CON review fortwo reasons: (1) the total costs exceedthe capital cost review threshold of $1million, and; (2) PET is classified as atertiary care service and is reviewableregardless of capital or operating costs.
In general, the CON process in-volves a formal application, publiccomment period, review by the HealthServices Council (HSC), an assessmentof public need and affordability, a rec-ommendation by the HSC and, a fi-nal determination by the Director ofRhode Island Department of Health(HEALTH). For tertiary care services,the due process steps remain the same,but greater scrutiny is applied to issuesrelated to quality of care including,programmatic oversight, staffing, effi-cacy, access and cost effectiveness.
�Certificate of Need Process: An Assessment of the
Need for PET
John X. Donahue, MPA
HISTORICAL BACKGROUND
PET is not a new medical tech-nology, but its capabilities and appli-cations in clinical practice have beenrefined and expanded over the last fewyears. Limitations on PET marketingand diffusion have included high costsand reimbursement constraints. Forexample, until recent developments inisotope production, PET required on-site capacity of cyclotrons (approxi-mately $2 million alone). Also, inDecember 2000, Medicare finally ap-proved for reimbursement an expandedlist of diagnostic categories for PETscanning services3
In Rhode Island, a number ofhospitals had, for many years, identi-fied PET as a potential CON projectin their individual hospital annualshort and long range plans but neverfiled for review. In 1991, Eastern Bio-Medical, Inc. submitted a CON to es-tablish PET scanning services. Thecapital costs were in excess of $5.5million and included a cyclotron. Theproposal was not approved, but it gen-erated much discussion on costs, or-ganizational structure, research,medical education and efficacy particu-larly within the medical community.
RECENT DEVELOPMENTS
Following the December 15,2000, Medicare decision to expandreimbursement, local interest in pro-viding PET services rapidly changed.In January 2001, three separate CONapplications were filed. Two proposalswere submitted by physician practicesspecializing in diagnostic imaging, andthe third application was a joint ven-ture between a for-profit entity and ahospital. The capital costs of the dif-ferent proposals ranged from $1.3 mil-lion to just under $2 million.
The CON applications were re-ferred to the HSC for review. Giventhe evolving nature of PET, the HSC/HEALTH requested that an indepen-
dent consultant undertake a need as-sessment for this tertiary service inRhode Island. Spectrum Research per-formed an in-depth analysis of PETand, in May 2001, presented its Re-port, “An Assessment of the Need forPositron Emission Tomography Scan-ners in Rhode Island,” to the HSC andthe applicants. The Report highlightedthe annual predicted patient volume tobe 2,806 scans while the annualthrough-put per scanner was estimatedto be 1,500. Important factors for sit-ing PET scanners included: 1) prox-imity to inpatient services; 2)availability for research; 3) access forteaching residents and medical schoolstudents; 4) board certification andexperience requirements for PET pro-gram directors and PET physicianreaders; 5) co-location with other clini-cal services; 6) radiation safety issuesfor PET staff; 7) state-of-the-art equip-ment capabilities; and, 8) cost effective-ness factors.4
The HSC was cognizant of thevalue that PET would contribute to thehealth care system in Rhode Island.The HSC weighed each applicationand recognized that each proposal hadcertain strengths and weaknesses. Inthe final analysis, however, the HSCwas not convinced that those propos-als then under review satisfied the fac-tors identified above for siting thistertiary care service in RI, particularlywith reference to the equipment, train-ing, co-location of services and the or-ganization/delivery of PET services asproposed.
The HSC recommended denial ofapplications, but also recommendedthat the HEALTH prepare a Requestfor Proposal (RFP) for PET Servicesincorporating the most recent researchand standards for PET services deliv-ery. In taking this position, the HSCsought to establish a high quality stan-dard for the initial deployment anddiffusion of this tertiary level technol-

148Medicine and Health / Rhode Island
ogy in RI. This approach has been uti-lized previously by the HSC andHEALTH in the case of other tertiarycare services.
REQUEST FOR PROPOSALS
After circulating a draft RFP tointerested parties, HEALTH, in De-cember 2001, issued the formal PETRFP with a February 1, 2002, sub-mission date. The RFP contained anumber of factors, standards and mea-sures that each applicant was requiredto address including: 1) planning pro-cess; 2) demonstrated demand; 3)teaching hospital role for medical edu-cation and research; 4) physician quali-fication and experience; 5) location andorganizational relationship to existingdiagnostic and medical services; 6)quality assurance standards; 7) state ofthe art equipment, and; 8) access forall patients regardless of ability to pay.
On February 1, 2002, two appli-cants responded to the RFP. RhodeIsland Hospital proposed to establishthe PET service on its campus adja-cent to its nuclear medicine depart-ment. Rhode Island PET Services,LLC (RIPS) proposed to offer a mo-bile PET service involving six hospi-tals statewide (Landmark MedicalCenter, Memorial Hospital of RhodeIsland, Roger Williams Medical Cen-ter, St. Joseph Health Services, KentCounty Memorial Hospital and SouthCounty Hospital Healthcare System).
Overall, there were several notice-able differences between the 2002 RFPproposals compared to the 2001 PETproposals. These included: 1) provisionfor state-of- the-art equipment (LSO/GSO); 2) identification of the meansto satisfy the professional competencerequirements of PET directors, PETreaders, and PET trainers; 3) hospital-based service to address the issue of co-location to other diagnostic andmedical services; 4) the role of teach-ing hospitals for medical education andresearch, and; 5) health facility licen-sure, quality assurance and access pro-visions.
The proposals were referred to theHSC for review. The HSC/HEALTHrequested that Spectrum Research up-date its 2001 Needs Analysis. The
2002 Update noted that recent reim-bursement changes in coverage for PETresulted in an estimated doubling ofpotential scan volume for Rhode Is-land. Spectrum Research now esti-mated the annual volume of scans tobe 5,600. The 2002 Update also fac-tored into account the more efficientnature of the equipment (LSO/GSO)proposed, resulting in greater annualthru-put of 3,000 PET scans. Finally,the Update continued to confirm theprofessional competence requirementsand other siting considerations for PEToriginally identified in the 2001 NeedsAssessment Report and as reflected inthe RFP standards. 5
Beyond the hardware issues of thenumber of scanners needed andequipment capabilities, the HSC/HEALTH were also concerned aboutthe professional componen t to oper-ate the PET service. The Departmentretained an out-of-state expert, R. Ed-ward Coleman, MD, Director of PETServices at Duke University MedicalSchool, to evaluate the RFP responsesand to review physician credentials forthe positions of PET directors, PETreaders, and PET trainers for both ap-plicants. The RFP requirements foreach were as follows: PET director –
board-certified in nuclear medicine/nuclear radiology and completed aPET fellowship or nuclear medicinefellowship and having read at least 600PET scans; PET reader – board-certi-fied in nuclear medicine with specialtyPET training or experience as demon-strated by having read at least 600 PETscans; PET trainer – board-certified innuclear medicine and having read over2,000 PET scans.
Dr. Coleman also reviewed theRIPS proposed 6-month PET trainingand education program (4 hours persession) for physicians to be sponsoredby Alan Fischman, MD, Director ofPET Services for Massachusetts Gen-eral Hospital. In addition, he advisedon volume standards for maintainingproficiency and competency in PETreadings. Dr. Coleman provided awritten Report which: 1) evaluated thequalifications of each proposed physi-cian against the RFP standards; 2)commented on the adequacy of theproposed RIPS training program; and3) recommended that any physicianwith limited PET experience (600 in-terpretations via a training program)needs to read a minimum of 5 scansper week (250 annually) to maintainproficiency.
CON DECISIONS
After consideration of all of thematerials including the RFP applica-tions, the 2002 Needs AssessmentUpdate Report and the Report of themedical consultant, the HSC recom-mended to the Director of Health thatthe RIH and the RIPS PET proposalsbe approved. The recommendationsincluded the standard CON conditionsof approval regarding cost, access andregulatory compliance. The HSC in-cluded an additional condition to theRIPS proposal that required that eachphysician have his/her scans over-readby the RIPS medical director (Dr.Fischman) until such time that physi-cian has read five scan per week on aconsistent basis.
In June 2002, the Director ofHealth accepted the HSC recommen-dations and approved the proposalswith the inclusion of conditions forPET site accreditation for both appli-
�
The Departmentretained an out-of-state
expert, R. EdwardColeman, MD, Directorof PET Services at Duke
University MedicalSchool, to evaluate theRFP responses and to
review physiciancredentials for thepositions of PET
directors, PET readers,and PET trainers for
both applicants.

149Vol. 86 No. 5 May 2003
cants and certain physician certifica-tions to the RFP requirements be forth-coming primarily from the RIPSproposals.
DISCUSSION
As a result of the RFP, the HSC/HEALTH have established a high stan-dard for the introduction and initialdeployment of PET services in RI. Theframework of the RFP required theapplicants to address quality consider-ations pertinent to tertiary care servicesin general and to PET services in par-ticular. For example, both RIH andRIPS have committed to acquiringstate of the art equipment and both willbe using professional staff that havemet or will meet the physician stan-dards for rendering PET services. Inaddition to quality of care factors, pa-
tients will also experience enhancedaccess and choice of location and PETservice provider.
In summary, current needs assess-ment and reimbursement policies in-dicate that patient demand for PETwill be more than adequately served byRIH and RIPS, at least in the nearterm. As PET becomes operationalearly in 2003, quality oversight activi-ties should be an integral componentof the service on an ongoing basis andpublic need for additional PET capac-ity will be periodically assessed.
REFERENCES1. Rhode Island General Assembly.
Chapter 23-15 Determination of Needfor New Health Care Equipment andNew Institutional Health Services.
2. Balk E, Lau J. PET scans and technologyassessment. JAMA 2001;285:936-7.
3. Medicare coverage policy decisionsmemorandum: FDG positron emis-sion tomography (CAG-00065); De-cember 15, 2000.
4. Zimmerman H. An Assessment of theNeed for Positron Emission Tomog-raphy Scanners in Rhode Island; May2001.
5. Zimmerman H. An Assessment of theNeed for Positron Emission Tomog-raphy Scanners in Rhode Island; Re-vised May 2002.
John X. Donahue, MPA, is Chiefof the Office of Health Systems Develop-ment, Rhode Island Department ofHealth.
CORRESPONDENCE:John X. Donahue, MPARhode Island Department of Health3 Capitol HillProvidence, RI 02908Phone: (401) 222-2788Fax: (401) 273-4350e-mail: [email protected]
20 Years ExperienceReferences
508-336-5066
Healthcare ProviderAHA CPR Training
in Your Building
AED & AMBU bag training,Barrier Device for each
person included. Best CPRclass, Certification good for2 years. $35 per person,
minimum of 5.

150Medicine and Health / Rhode Island

151Vol. 86 No. 5 May 2003
Edited by Jay S. Buechner, PhD
Damp Housing Conditions and Asthma in Rhode IslandLeanne C. Chiaverini, Jana E. Hesser, PhD, and John P. Fulton, PhD
Rhode Island Department of Health
Patricia A. Nolan, MD, MPH, Director of Health
Health by Numbers
Exposure to environmental agents can play an impor-tant role in the development and exacerbation of
asthma, a condition that affects an estimated 84,000 per-sons in Rhode Island (RI).1 Considering the amount oftime spent indoors, housing conditions are of particularinterest. More specifically, several studies in the U.S. andelsewhere have found that the prevalence of asthma andother respiratory symptoms among both children andadults are higher in homes with reported dampness ormold.2-5 Mildew (mold in early stage) and molds are fungithat grow on organic materials almost anywhere indoorsand outdoors.6 They thrive in moist environments—mold
growths or colonies can develop on damp surfaces within24 to 48 hours—and reproduce by making small, lightweightspores that travel through the air.6 The work presented hereexamines the relationship between home dampness/mildewodor and asthma in RI.
At the national level, Healthy People 2010 includes thefollowing objective relevant to environmental risk factors:increase the number of “persons with asthma who receiveassistance with assessing and reducing exposure to environ-mental risk factors in their home, school, and work envi-ronments.7”
MethodsData on persons reported with
asthma, dampness in the home, and mil-dew odor in the home were obtained fromthe RI Health Interview Survey,1 a peri-odic telephone survey of approximately2,600 households including 6,500 indi-viduals per iteration. Percentages and es-timated populations are based on weighteddata for 2001.
Prevalence of asthma is defined as per-sons who answered “yes” to “Does anyonein the household have asthma?” and “Dida doctor say that you/he/she have/hasasthma?” Dampness in the home is deter-mined from two questions as shown inTable 1: (a) “During the past 12 months,has there been water or dampness in theapartment/house where you live caused bybroken pipes, leaks, heavy rain, or floods?”and (b) “Has this happened more than oncein the past 12 months?” Mildew odor inthe home is defined as persons who an-swered “yes” to “Does the apartment/housewhere you live frequently have a mildewodor or musty smell?” All data exclude re-spondents who answered “I don’t know” orwho refused to answer the question.
ResultsAmong all persons in RI, 18% re-
port the presence of any dampness (9%
Figure 1. Prevalence of dampness and mildew odor in housing, Rhode Island, 2001.
Figure 2. Prevalence of asthma, by presence of dampness and mildew odor in housing,Rhode Island, 2001.

152Medicine and Health / Rhode Island
report one time dampness; 9% report repeated dampness),10% report mildew odor, and 23% report either any damp-ness or mildew odor in the home. (Figure 1) The percentof Rhode Islanders who report dampness and mildew odorin the home varies by several demographic variables. Damphousing/mildew odor was reported less among homeowners(versus renters), Hispanics, and persons of older age. Theobserved relationship between demographic variables andhome dampness/mildew odor was independent of genderand income.
According to this study, 8.6% of Rhode Islanders arereported to have a doctor’s diagnosis of asthma. The bur-den of asthma varies according to dampness/mildew odorhousing conditions. (Figure 2) The percent of persons inRI who have asthma is 7.9% among those with no damp-ness in the home, 8.4% among those with one-time damp-
ness in the home, and 12.6% amongthose with repeated dampness in thehome. The percent of persons in RI withasthma is 7.9% among those with nomildew odor in the home. This num-ber jumps to 12.1% among persons whoreport mildew odor in the home. Oddsratios (ratio of event occuring with riskcondition to event occuring without riskcondition) for associations betweenasthma and home dampness/mildewodor range from 1.14 to 1.60. (Table 2)
Age is a significant variable whenconsidering the relationship betweenasthma and home dampness/mildewodor. (Figure 3) Among persons whoreport no dampness or mildew odor inthe home, the burden of asthma is dis-tributed evenly across all age groups
(about 8%) except for those 65 years and over (asthma preva-lence of 5.5%). Among persons who report any dampnessor mildew odor in the home, the percent with asthma de-creases as age increases. The strongest association betweenasthma and any dampness or mildew odor is among 0-17year-olds. In this age group, the percent of persons withasthma is 8.2% among those with no dampness or mildewodor, and 14.6% among those with any dampness or mil-dew odor in the home. A smaller association is seen amongpersons ages 18-44 (7.9 versus 10.1%). No difference isobserved among persons ages 45-64 (8.3% for both nodampness/mildew odor and any dampness/mildew odor),and there is a small inverse relationship among those 65years and over (5.5 versus 4.2%).
AssessmentPublished research2-5
has demonstrated thatdampness and mildew odorin the home are potentialrisk factors for asthma. Wehave observed a similar as-sociation in RI survey data.The prevalence of asthma inRI is elevated among per-sons who report one time orrepeated dampness or mil-dew odor in the home com-pared with those who report
no dampness or mildew odor in the home. This relation-ship between home asthma and dampness/mildew odor wasstrongest among persons ages 0-17. The burden of asthmain this age group was disproportionately higher than in otherage groups. Results suggest that children and young adultsare more susceptible than adults to developing asthma as aresult of exposure to home dampness/mildew odor.
Future investigations may want to examine other ex-posures in the home environment, such as environmental
Figure 3. Prevalence of asthma, by age group and presence of dampness and mildew odorin housing, Rhode Island, 2001.

153Vol. 86 No. 5 May 2003
tobacco smoke or the presence of adequate ventilation, aswell as the relationship between asthma and dampness/mil-dew odor in other indoor environments such as workplacesand schools.
This and future studies will be instrumental in design-ing public health interventions to reduce exposure to envi-ronmental triggers of asthma in order to reduce asthmamorbidity. Asthmatic patients should be encouraged todeal with mold problems effectively and efficiently, and totake the following steps to prevent mold and mildew prob-lems in their homes:6
• Fix leaks in pipes or other sources of water.• Be sure the home has adequate ventilation.• Use dehumidifiers during humid months.ª Clean bathrooms with mold killing products.
Leanne C. Chiaverini is Research Associate, Division ofDisease Prevention and Control, Rhode Island Department ofHealth.
Jana E. Hesser, PhD, is Program Manager for Health Sur-veys, Office of Health Statistics, Rhode Island Department ofHealth, and Clinical Teaching Associate in Community Health,Brown Medical School.
John P. Fulton, PhD, is Associate Director, Division ofDisease Prevention and Control, Rhode Island Department ofHealth, and Clinical Associate Professor of Community Health,Brown Medical School.
REFERENCES1. Rhode Island Health Interview Survey, Office of Health Sta-
tistics, RI Department of Health, 2001.2. Thorn J, Brisman J, Toren K. Adult-onset asthma is associ-
ated with self-reported mold or environmental tobacco smokeexposures in the home. Allergy 2001;56:287-92.
3. Hu FB, Persky V, Flay BR, Richardson J. An epidemiologicalstudy of asthma prevalence and related factors among youngadults. J Asthma 1997;34:67-76.
4. Kilpelainen M, Terho EO, Helenius H, Koskenvuo M. Homedampness, current allergic diseases, and respiratory infectionsamong young adults. Thorax 2001;56:462-7.
5. Yang CY, Chiu JF, Chiu HF, Kao WY. Damp housing condi-tions and respiratory symptoms in primary school children.Pediatr Pulmonol 1997;24:73-7.
6. Federal Emergency Management Association, Mitigation Di-vision. Dealing with Mold and Mildew in your DamagedHome. http://www.fema.gov/pdf/reg-x/mold_mildew.pdf
7. US Department of Health and Human Services. Healthy People2010. 2nd ed. With Understanding and Improving Health andObjectives for Improving Health. 2 vols. Washington, DC: USGovernment Printing Office, 2000.

154Medicine and Health / Rhode Island
– A Physician’s Lexicon –
The Verbiage of Obesity
(a) Cause of death statistics were derived from theunderlying cause of death reported by physicians ondeath certificates.
(b) Rates per 100,000 estimated population of1,048,319
(c) Years of Potential Life Lost (YPLL)
Note: Totals represent vital events which occurred in Rhode Is-land for the reporting periods listed above. Monthly provisionaltotals should be analyzed with caution because the numbersmay be small and subject to seasonal variation.
Rhode Island MonthlyVital Statistics Report
Provisional Occurrence Datafrom the
Division of Vital Records
Vital StatisticsEdited by Roberta A. Chevoya
Rhode Island Department of Health
Patricia A. Nolan, MD, MPH, Director of Health
Number (a) Number (a) Rates (b) YPLL (c)Diseases of the Heart 243 3,069 292.8 3,894.0**Malignant Neoplasms 188 2,403 229.2 7,483.0 *Cerebrovascular Diseases 40 529 50.5 720.0**Injuries (Accident/Suicide/Homicide) 21 400 38.2 7,385.0***COPD 32 517 49.3 462.5
Reporting PeriodUnderlyingCause of Death 12 Months Ending with May 2002
Number Number RatesLive Births 1,120 13,649 13.0*Deaths 821 10,289 9.8*
Infant Deaths (6) (101) 7.4#Neonatal deaths (5) (71) 5.2#
Marriages 557 8,306 7.9*Divorces 248 3,389 3.2*Induced Terminations 416 5,563 407.6#Spontaneous Fetal Deaths 89 1,123 82.3#
Under 20 weeks gestation (86) (1,052) 77.1#20+ weeks gestation (3) (71) 5.2#
Reporting PeriodNovember
2002Vital Events
* Rates per 1,000 estimated population # Rates per 1,000 live births** Excludes one death of unknown age.*** Excludes two deaths of unknown age.
12 Months Ending withNovember 2002
May2002
The word epidemic, by custom if not byetymology, is generally applied to any
disorder, infectious or otherwise, originat-ing elsewhere, newly attacking large num-bers of humans living in a geographicallydefined area, and coming down with thedisease within a restricted time interval. TheUnited States is currently experiencing un-precedented increases in overweightednessand obesity. And so, in the words of theRhode Island Department of Health, thedisorder of obesity has reached “epidemicproportions in the United States.” To illus-trate, in 1991 no state had an obesity rateof 20% or more involving its overall popu-lation. By 2000, 22 states reported obesityrates of 20% or higher in their populations,and in the past decade, the adult obesitypopulation in Rhode Island has almostdoubled.
Obese individuals are now defined ashaving a Body Mass Index [calculated by aperson’s height and weight] equaling or ex-ceeding 30. The synonyms of the word,obese, are numerous.
The word obesity is derived from a
Latin word, obesus, which in turn is a con-traction of two Latin words, ob- and edere,meaning to devour, to eat away. The edereroot also produces such current Englishwords as edible. Adipose, and similar wordssuch as adiposity, come from a Latin wordadeps, meaning fat. The anatomic phrase,panniculus adiposus [the superficial ab-dominal fascia with much incorporated fattytissue] is also derived from the Latin pan-nus, meaning sheet or layer.
The word corpulent comes directlyfrom the Latin corpulentia, meaning anaugmentation of the body [corpus]. Andwith an added diminutive ending one ar-rives at the Latin word, corpusculum, mean-ing little body as in its English derivative,corpuscle. Portly, from the Latin portare,meaning to carry, has, as in English wordssuch as comport, gradually evolved to meanhow one carries or conducts oneself, as inthe sentence, “He comported himself withdignity.” Portly has then come to mean dig-nified, imposing, stout.
The word stout [an old German wordoriginally meaning courageous or dauntless,
as in stout-hearted] has now gradually come to meanfleshy or corpulent.
And the word weight comes from anAnglo-Saxon word gewiht, meaning fatty.The word fat is similarly of Anglo-Saxonorigin, taken from the word, faet.
Words such as lipid, lipase, lipoma andlipemia are all derived from a Greek wordmeaning greasy or fatty. In general, whenthere is both a Latin as well as a Greek termavailable to define a specific anatomic struc-ture, the pathologic states tend to use theGreek rather than the Latin root. Thus wehave the word pulmonary, from the Latin,but pneumonitis from the Greek; or renal,from the Latin, but nephritis from theGreek; or vascular from the Latin, but an-giitis, from the Greek. This pattern of as-signing pathologic states or lesions solely toGreek-derived words is diminishing sincewords such as pu;monitis or vasculitis nowappear occasionally.
– STANLEY M. ARONSON, MD, MPH

155Vol. 86 No. 5 May 2003
William M. AllenTroy, Pires & AllenPawtucket • 401-728-2060
Sidney BaileyAON Risk Services of RIProvidence • 401-331-7700
Nat CalamisStarkweather & ShepleyEast Providence • 401-435-3600
John H. Lathrop Lathrop Ins. AgencyWesterly • 888-596-2530
Bill Mende Mastors & ServantEast Greenwich • 800-335-5701
Anthony Paolino, Jr.Paolino Ins. AgencyProvidence • 401-421-2588
John TicknerBabcock & HelliwellWakefield • 401-782-1800
ith important purchases, the lowest price isn’t always the best buy. Quality is more critical in the purchase of a home,
car, medical equipment and that all-important purchase: medical malpractice insurance. With the future of your practice and your reputation on-the-line you can’t afford second best.
Take a look at ProMutual Group:
• The largest provider of medical malpractice insurance in New England.
• Nearly 30 years experience.
• Insures more than 16,000 healthcare professionals.
• Financial strength that has earned us an A- (Excellent) rating from A.M. Best, the nation’s leading independent insurance rating organization.
• Over $1.3 billion in total assets with $364 million in surplus.*
• Outstanding risk management service from thelargest staff in New England.
• Experienced claim professionals close a majority of claims without payment and win in excess of 90% of those that go to verdict.
Isn’t it time you got the best protection from one of the largest providers of medical malpractice insurance in New England? Call or visit our web site today.
www.promutualgroup.com
101 Arch Street, Boston, Massachusetts 02110888-776-6888 www.promutualgroup.com
Connecticut • Maine • Massachusetts • New Hampshire • New Jersey • Rhode Island • Vermont
* As reported in our 2001 Annual Report.
Not all products are available in all states.

156Medicine and Health / Rhode Island
�
�
�
�
PROVIDENCE, R.I., JANUARY, 1917VOLUME 1NUMBER 1
PER YEAR $2.00SINGLE COPY, 25 CENTS
The Official Organ of the Rhode Island Medical SocietyIssued Monthly under the direction of the Publications Committee
THE RHODE ISLAND MEDICAL JOURNAL
� �FIFTY YEARS AGO
[MAY, 1953]
� �NINETY YEARS AGO
[MAY, 1913]
TWENTY FIVE YEARS AGO
[MAY, 1978]� �
An editorial explained the Medical Society’s reluctant decision toexpel two members. The first, Dr. J.B. Archambault, of
Woonsocket, “although a graduate of Laval [and] a licensed practi-tioner of this state,” had “publicly lent his name and the professionto a …quack medicine.” Dr. Archambault had placed an advertise-ment in a local newspaper for his elixir, a “Long Life Tonic for Dys-pepsia and all Female Disturbances, also a Wonderful Cough Syrupfor Tuberculosis, Bronchitis, Pneumonia, Whooping Cough.” TheSociety also expelled Dr. George M. Bailey, MD, LLB, President ofthe Rhode Island College of Nursing. Dr. Bailey had advertised theschool in JAMA. This correspondence course (the time could rangefrom a few months to a year) was replacing the Rhode Island Train-ing School for Nursing and Allied Sciences. Dr. Bailey proposed togive physicians stock in the school, in exchange for sending “fullypaid students.” The advertisement promised physician-investors thatthey might also gain some free labor from the students.
Governor Pothier had invited Dr. Friedrich F. Friedmann ofGerman to demonstrate at public clinics (Woonsocket Hospital, St.Joseph’s Hospital, City Hospital, and an improvised laboratory atthe Narragansett Hotel) his treatment for tuberculosis. Dr. Friedmannrefused to publish details of his cure. The Journal decried the visit:“That he has infected others with his sensationalism is evidenced bythe hectic and perfervid comparison of his coming to America by alocal minister to that of the coming of Jesus Christ.”
Henry C. Hall, MD, President, Providence Medical Associa-tion, gave the Annual Address, “Practical Aspects of Psychotherapy.”He wrote: “In the present era of medical science . . . may it not bewell to pause and seriously question whether some of the old-timemethods of cure are not neglected?” Specifically, he cited “sugges-tion” (as in faith healing, mesmerism, animal magnetism), but con-ceded that modern medicine was “antagonistic” to these treatments.
Henry W. Kimball, MD, in “Carbon Dioxide and its Uses inDermatology,” noted that in 1905 Julius Berg of Breslow sprayedcarbon dioxide on body parts; later Pusey of Chicago used the solidform. He described the technique of collecting and molding thesnow, using a chamois sheet and a test tube. He recommended car-bon dioxide for congenital deformities of the skin, abnormal over-growth, small epithelomata, hypertropic scars, lupus vulgaris, eventattoo marks.
Arthur E. O’Dea, MD, Research Fellow in Pathology and LegalMedicine, Harvard Medical School, presented “Medicolegal and
Pathological Aspects of Suicide,” at the Providence Medical Associa-tion annual meeting. He cited the duties of a forensic pathologist:“He not only documents homicide but also guards the public inter-est by removing unwarranted suspicion arising over a given deathand assists law enforcement officers acting as an impartial arbiter in
In “Message from the Dean,” Stanley M. Aronson, MD, MPH,described the 63 students from the Class of 1978, Brown Medical
School’s fourth group. The journal featured photographs of gradu-ates, with their residency destinations.
In “Medicine in the Year 2000 : A Symposium,” Stanley M.Aronson, MD, Paul Calabresi, MD, Pierre M. Galletti, MD, PhD,Henry T. Randall, MD, Leo Stern, MD, Albert F. Wessen, PhD, andRobert J. Westlake, MD, peered into the crystal ball two years hence.[They did not foresee managed care.]
Milton W. Hamolsky, MD, gave a eulogy for Marshall Fulton,MD [1899-1977], an Iowa-born Brown graduate and Rhodes Scholarwho went on to become Brown’s first University Professor of Medi-cine in Brown’s new program in medicine.
The Journal reprinted from the Harvard Medical Alumni Bulle-tin “Sir William Osler’s Better Half,” which Dr. Fulton wrote for theAmerican Osler Society.
investigating sudden and apparently unexplainable deaths.” Identify-ing suicide was a challenge because the pathologist rarely had a cor-rect family history. Instead, the family would try to make the cause ofdeath seem natural or accidental.
Norman L. Loux, MD, Clinical Director, Butler Hospital, in“Some Clinical Aspects of Suicide,” said that men were more likely touse firearms and hanging; women, poison and gas.
Anthony Caputi, MD, and Louis E. Burns, MD, in “CoronaryOcclusion and Myocardial Infarction,” reviewed 188 cases of coro-nary occlusion seen at Newport Hospital from January 1, 1946, toDecember 31, 1950. Only 12 patients received anticoagulant therapy.The mortality rate was 40.5 %; 76.3% of them died within two weeksafter onset of the occlusion.
Barry B. Mangillo, MD, contributed “Videotherapy as an Of-fice Procedure.” For example, the cartoon film, “Johnny Learns HisManners,” was “of great value in treating children with behavior prob-lems.” The film featured “Badself,” “nasty imp whose mission is toget Johnny into trouble”, versus “Goodself.” One scene, promotingneatness, showed Johnny in the room of a West Point cadet.
An editorial praised the Providence Tuberculosis League, whichprovided chest x-rays and advice to 6,341 individuals at facilities andtook 22,214 small films at the trailer.
An editorial on Foreign Medical Graduates noted, on the onehand, that state licensing boards had found the foreign training defi-cient, on the other hand, that hospitals needed these staff. The edito-rial saw “no easy solution.”


















