
It’s Complicated: Methods to assess medication nonadherence and regimen complexity
Upload
shana-chandlerCategory
view
214download
0
Medication Nonadherence Is Associated With Increased Health
Care Utilization in Pediatric Patients With Chronic Diseases

Background The systematic review
Methods and included studies Results Conclusions
More information about medication nonadherence
Approaches and tools to promote medication adherence
Outline

In 2010, the United States spent $2.6 trillion on health care.
The two largest components of health care spending: Hospital care Physician and clinical services (i.e., emergency
department visits, hospitalizations, office visits) About 10 percent of the population consumes about
64 percent of health care expenditures. Patients with chronic conditions often incur high
levels of health care costs and use about 83 percent of health care services.
Overview of Health Care Utilization in the United States
Emanuel EJ. JAMA. 2012 Jan 4;307(1):39–40. PMID: 22214161.Haber S, McCall N, Cromwell G. RTI Project No. 0208491.018. Available at http://www.rti.org/pubs/0208490-018_siv-draft.pdf.Martin AB, Lassman D, Washington B, et al. Health Aff (Millwood). 2012 Jan;31(1):208-19. PMID: 22232112.Schoenman J, Chockley N. NIHCM Data Brief. Available at http://www.nihcm.org/images/stories/NIHCM-CostBrief-Email.pdf.Stanton MW. AHRQ Pub. No. 06-0060. Available at http://www.ahrq.gov/research/ria19/expendria.pdf.

Improving tertiary prevention may reduce unnecessary medical care for chronically ill patients including: Decision support tools to increase patient
engagement, and potentially, medication adherence Establishing interventions to increase medication
adherence Targeting modifiable factors related to patients with
chronic conditions, specifically medication adherence, may reduce health care use and associated costs.
Reducing Health Care Use and Costs Related to Chronic Conditions
Anderson G. Chronic conditions: making the case for ongoing care. 2010. Available at http://www.rwjf.org/content/dam/farm/reports/reports/2010/rwjf54583.De Brantes F, Rosenthal MD, Painter M. N Engl J Med. 2009 Sep 10;361(11):1033-6. PMID: 19692682.Emanuel EJ. JAMA. 2012 Jan 4;307(1):39–40. PMID: 22215161.

Adherence can be defined as “the extent to which a person’s behavior coincides with medical or health advice.”
Adherence depends on interactions between patients and health care providers and refers to behavioral correspondence with: Prescriptions Medical recommendations Advice from health care providers
According to the World Health Organization (WHO), adherence is the most important modifiable factor that can compromise treatment outcomes.
Defining Medication Adherence
Modi AC, Pai AL, Hommel KA, et al. Pediatrics. 2012;129(2):e473-85. PMID: 22218838.Sabate E. Adherence to long-term therapies: evidence for action. 2003. Available at http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?ua=1.
Self-management is “the interaction of health behaviors and related processes that children and/or family members engage in to care for a chronic condition.”
Self-management and adherence are interrelated—nonadherence can be a result of poor self-management.
Self-management behaviors occur across four domains: Individual Family Community Health care systems
Poor self-management reduces treatment benefits and increases the risks of adverse health outcomes.
Defining Self-management
Modi AC, Pai AL, Hommel KA, et al. Pediatrics. 2012;129(2):e473-85. PMID: 22218838.

The rate of chronic conditions among children has doubled in the past 2 decades.
About 13 to 27 percent of children have an existing chronic condition that requires ongoing multidisciplinary treatment and self-management.
Chronically ill pediatric patients who require ongoing treatment and self-management may represent a population that can seriously impact health care costs.
Pediatric Chronic Conditions in the United States
Modi AC, Pai AL, Hommel KA, et al. Pediatrics. 2012 Feb;129(2):e473-85. PMID: 22218838.Newacheck PW, Halfon N. Am J Public Health. 1998 Apr;88(4):610–7. PMID: 9551003.Newacheck PW, McManus MA, Fox HB. Am J Dis Child. 1991 Dec;145(12):1367–73. PMID: 1669662. Newacheck PW, Taylor WR. Am J Public Health. 1992 Mar;82(3):364–71. PMID: 1536351.Van Cleave J, Gortmaker SL, Perrin JM. JAMA. 2010 Feb 17;303(7):623–30. PMID: 20159870.van Dyck PC, Kogan MD, McPherson MG, et al. Arch Pediatr Adolesc Med. 2004 Sep;158(9):884–90. PMID: 15351754.

Based on 2009–2010 data, approximately 86 percent of children and adolescents with chronic illnesses are prescribed medication.
Nonadherence to prescribed medication regimens affects 50 to 88 percent of children and adolescents with chronic conditions.
As with adults, nonadherence in pediatric populations may be a modifiable factor that can help reduce health care use and costs.
Efforts to contain pediatric health care costs have not yet been examined despite the widespread nature of nonadherence in pediatric patients.
Poor Self-management and Nonadherence in Chronically Ill Pediatric Patients
Hommel KA, Davis CM, Baldassano RN. Inflamm Bowel Dis. 2009 Apr;15(4):589-93. PMID: 18985746.Logan D, Zelikovsky N, Labay L, Spergel J. J Pediatr Psychol. 2003 Sep;28(6):383-92. PMID: 12904450.Modi AC, Pai AL, Hommel KA, et al. Pediatrics. 2012 Feb;129(2):e473-85. PMID: 22218838.

McGrady and Hommel1,2 published a systematic review in Pediatrics (2013) to examine the relationship between medication nonadherence and health care use in children and adolescents who have a chronic medical condition.
Articles published before April 2013 were identified using PubMed®, PsycINFO®, and CINAHL® and searching reference lists of relevant articles.
Inclusion criteria: Tested the relationship between medication nonadherence
and health care use (i.e., hospitalizations, emergency department visits, or outpatient visits) or cost
Children and adolescents (mean age ≤ 18 years) with a chronic medical condition
Data were extracted to predefined data fields.
A Systematic Review of Medication Adherence and Health Care Utilization in Pediatric Chronic Illness
1 McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953. 2 Dr. Kevin Hommel is a member of the Cincinnati Children’s Center for Education and Research on Therapeutics (CERT).

Systematic Review Study Selection Flow Diagram
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.
Records identified through database searching (n = 4,519)
Additional records identified through other searches (n=12)
Records after duplicates removed (n = 4,346)
Records screened (n = 4,346) Inclusion criteria:1. Pediatric sample with a chronic illness2. Original research article3. Adherence and health care utilization or
cost referenced
Full-text articles assessed for eligibility (n = 73)
Studies included in qualitative synthesis (n = 10)
Records excluded (n = 4,273)
Articles excluded (n = 63)• No examination of
relationship between adherence and health care utilization (n=2)
• Mean age of sample > 18 years (n = 3)
• No health care utilization (n = 25)
• No adherence (n = 32)• Use of same sample (n = 1)

Medication nonadherence measures: Self-report questionnaires Self-report structured interviews Electronic monitoring devices Prescription refill history Biochemical assays
Health care use data classifications: Emergency department (ED) visits Outpatient visits Hospitalizations Other (e.g., combined number of ED visits, outpatient
visits, and hospitalizations)
Measures and Outcomes Used in the Systematic Review
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.Quittner AL, et al. J Pediatr Psychol. 2008 Oct;33(9):916–36; discussion 937–8. PMID: 17846042.

Ten studies met the inclusion criteria. The chronic illness in nine studies was asthma, and type
I diabetes was the chronic illness in the 10th study. Mean age range was from 6.2 to 16 years. Study designs:
Prospective observational cohort (n = 4) Cross-sectional analyses (n = 3) Retrospective observational cohort (n = 2) Randomized-controlled trials (n = 1)
Measures of adherence in included studies: Pharmacy refill records (n = 5) Self-report measures (n = 3) Electronic monitors (n = 2)
Description of the Studies Included in the Systematic Review
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.
Six studies show that greater nonadherence is related to a higher risk for emergency department visits in children and adolescents with asthma.
Nonadherence in these studies is measured as: Not filling any anti-inflammatory prescriptions versus
filling at least one A lower percentage of time in possession of anti-
inflammatory medications A lower percentage of dosages taken, as measured
by electronic monitoring
Results of the Systematic Review: Emergency Department Visits and Medication Nonadherence
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.

Two studies found that nonadherence is related to fewer asthma-related office or primary care physician visits. The fewer the number of days a child possessed
asthma-related medications, the less often they made asthma-related office visits.
Primary care physician visits were less likely for a child whose controller medication prescription had not been filled in the last 3 months.
Results of the Systematic Review: Outpatient Visits and Medication Nonadherence
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.

Results were mixed and dependent on the method of adherence measurement.
For children with asthma, these measures were associated with increased risk for hospitalization: Failing to fill any anti-inflammatory prescriptions Caregiver self-reports of nonadherence to corticosteroids
In other studies, medication adherence was not associated with fewer hospital admissions. Anti-inflammatory medication possession ratios (MPRs) of 20 to 49
percent had increased odds of hospitalization versus those with MPRs of 0 to 19 percent.
Leukotriene MPRs were not associated with hospitalizations. Adherence behaviors as assessed in a sample of questionnaires
had no relationship to hospitalizations rates.
Results of the Systematic Review: Asthma-Related Hospitalizations and Medication Nonadherence
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.

For children with type 1 diabetes, who were younger than 10 years of age, nonadherence was associated with increased odds for: Hospital admission for diabetic ketoacidosis
(OR = 24.57; 95% CI, 4.66 to 129.49; p-value = 0.001)
Hospital admission for acute diabetic-associated complications (OR = 10.86; 95% CI, 1.60 to 73.48; p-value = 0.02)
Results of the Systematic Review: Type 1 Diabetes-Related Hospitalizations and Medication Nonadherence
Abbreviations: 95% CI = 95-percent confidence interval; OR = odds ratio
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.
Caregiver self-reported nonadherence was related to more frequent unscheduled asthma visits (provider and emergency department visits).
Nonadherence may be associated with changes in health care use patterns. Nonadherence was associated with greater health
care use over time in a sample of African-American children with asthma versus health care use patterns of children with better adherence.
Results of the Systematic Review: Other Measures of Health Care Use and Medication Nonadherence
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.

Medication nonadherence is usually related to increased health care use in children and adolescents who have a chronic illness.
Nonadherence may be associated with more emergency department visits and hospitalizations. Children and adolescents who are nonadherent may suffer
from more exacerbations and complications requiring medication attention and more emergency department visits or hospitalizations.
Nonadherence may be associated with fewer outpatient visits. It is likely that patients who are nonadherent to their
medication regimens are also nonadherent to scheduled office visits.
Conclusions From the Systematic Review
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.

The relationship between nonadherence and increased health care utilization is consistent with findings in adults samples.
Addressing medication nonadherence in the pediatric population may reduce the $1,800/child spent on hospital care, according to a study by Encinosa et al. published in 2010.
This issue can be addressed in the clinical care of chronically ill pediatric patients to promote shared decisionmaking.
Clinical Implications From the Systematic Review
Agency for Healthcare Research and Quality. 2010 Medical Expenditure Panel Survey Household Component Data. Available at http://meps.ahrq.gov/mepsweb. Accessed July 8, 2013.Encinosa WE, Bernard D, Dor A. Adv Health Econ Health Serv Res. 2010;22:151–73. PMID: 20575232.Roebuck MC, Liberman JN, Gemmill-Toyama M, et al. Health Aff (Millwood). 2011 Jan;30(1):91–9. PMID: 20575232.Valenti WM. AIDS Read. 2001 Feb;11(2):77–80. PMID: 11279875.

Unintentional Intending to take a medication as instructed but failing to
do so for some reason (e.g., forgetfulness, carelessness) Influenced by patient characteristics, treatment factors,
and patient-provider issues Intentional
Making a reasoned decision not to take a medication as instructed based on perceptions, feelings, or beliefs
A rational decisionmaking process whereby the patient weighs the benefits of treatment against any adverse effects of the treatment
Mitigating nonadherence requires different types of interventions.
Understanding the Types of Nonadherence
Dayer L, Heldenbrand S, Anderson P, et al. J Am Pharm Assoc. 2013 Mar-Apr;53(2); 172-81. PMID: 23571625.
Sabate E. Adherence to long-term therapies: evidence for action. 2003. Available at http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?ua=1.

Behavioral Modifying the environment to encourage adherence
or providing positive and negative consequences Educational
Providing information on physician orders or how to use medical equipment
Organizational Decreasing barriers to medical care by improving
communication with medical staff or reducing the complexity of medical regimens
Combinations of these
General Categories of Adherence Intervention Strategies
Graves M, Roberts M, Rapoff M, et al. J Pediatr Psychol. 2010 May;34(4);368-82. PMID: 19710248.Sabate E. Adherence to long-term therapies: evidence for action. 2003. Available at http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?ua=1.

Adherence interventions can effectively increase adherence and improve health outcomes.
Educational interventions alone are insufficient to promote adherence in children and adolescents.
Behavioral and multicomponent interventions may have stronger effects on adherence behaviors than those that only employ educational techniques.
Combination behavioral and educational strategies may improve health outcomes better than either strategy used alone.
There is considerable heterogeneity in the available data highlighting the need for future research.
Results of Recent Meta-analyses on Adherence Interventions in Chronically Ill Pediatric Patients
Dean AJ, Walters J, Hall A. Arch Dis Child. 2010 Sep;95(9):717-23. PMID: 20522463.Graves MM, Roberts MC, Rapoff M, et al. J Pediatr Psychol. 2010 May;35(4):368-82. PMID: 19710248. Kahana S, Drotar D, Frazier T. J Pediatr Psychol. 2008 Jul;33(6):590-611. PMID: 18192300.

Modi et al. (2012) described a patient self-management model accounting for multiple factors in medication adherence: Individual, family, community, health care system factors Treatment type (e.g., medication route, manual therapy) Lifestyle issues (e.g., diet, exercise) Clinic appointment attendance Symptom monitoring (e.g., glucose measures, inhaler use) Outcome measures (e.g., symptom control, quality of life) System issues (e.g., financial costs, treatment efficacy)
The model is described in a copyrighted publication available at no cost at www.pediatrics.org/cgi/content/full/129/2/e473.
Pediatric Self-management Model
Modi AC, Pai AL, Hommel KA, et al. Pediatrics. 2012 Feb;129(2):e473-85. PMID: 22218838.

The next four slides provide information on tools and resources that clinicians and caregivers can use to promote prescription medication adherence in children and adolescents with chronic health conditions.
Links to these tools and resources are provided here, and CME/CE participants are encouraged to: Peruse these resources Identify those relevant to their patients’ needs Apply relevant tools and resources in their practice setting
to enhance medication adherence among children and adolescents challenged by chronic health problems
These resources have been developed into a handout available at chainonline.org/practice-tools/medication-adherence-handout/.
Practical Implications for Chronically Ill Pediatric Patients

The Cincinnati Children’s Center for Education and Research on Therapeutics (CERT) offers these patient-friendly tools to help patients and caregivers manage behaviors related to medication adherence: Helping your child manage medication treatment effectively (tip
sheet) Adherence strategies tip sheet Keeping track of your child's medication taking (medication calendar) Problem solving guide for family members Helping your child swallow pills (tip sheet) Helping your child with eczema and other skin conditions (Behavior
Change Plan and Habit Reversal Training) Helping your child with sickle cell disease (Pain Management Plan and
Self Management Program)
The tools are available at www.cincinnatichildrens.org/research/divisions/c/adherence/parents/.
Practical Implications for Chronically Ill Pediatric Patients: Resources for Patients and Caregivers
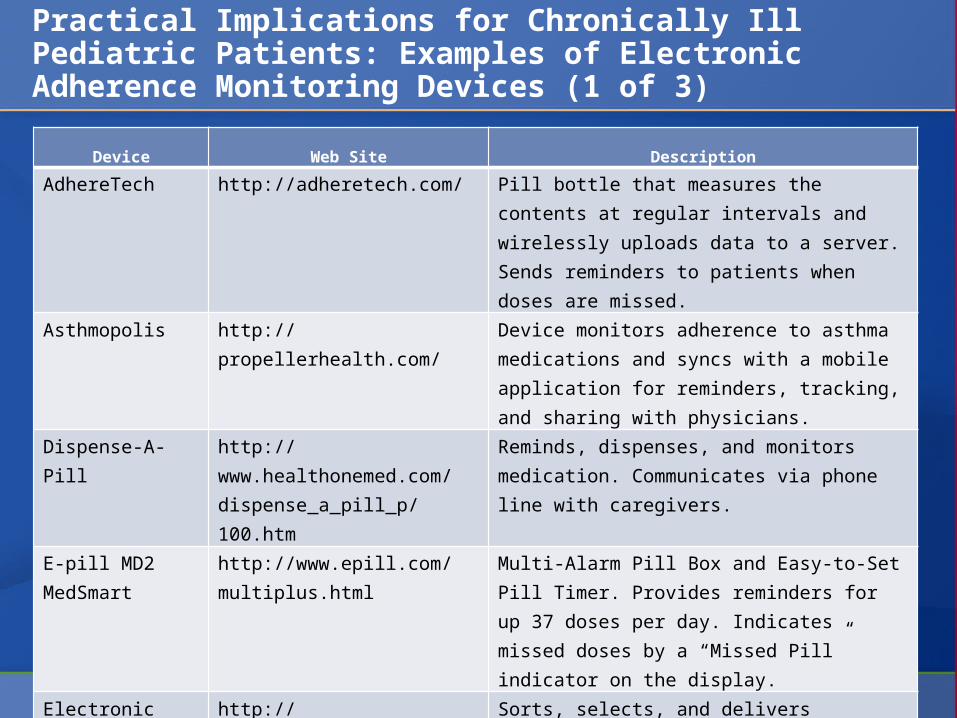
Device Web Site Description
AdhereTech http://adheretech.com/ Pill bottle that measures the contents at regular intervals and wirelessly uploads data to a server. Sends reminders to patients when doses are missed.
Asthmopolis http://propellerhealth.com/ Device monitors adherence to asthma medications and syncs with a mobile application for reminders, tracking, and sharing with physicians.
Dispense-A-Pill http://www.healthonemed.com/dispense_a_pill_p/100.htm
Reminds, dispenses, and monitors medication. Communicates via phone line with caregivers.
E-pill MD2 MedSmart
http://www.epill.com/multiplus.html
Multi-Alarm Pill Box and Easy-to-Set Pill Timer. Provides reminders for up 37 doses per day. Indicates missed doses by a “Missed Pill” indicator on the display.
Electronic Medication Management Assistant
http://www.inrangesystems.com/#1
Sorts, selects, and delivers medication.Remotely controlled by pharmacist or nurse. Provides reminders and alarms.
Practical Implications for Chronically Ill Pediatric Patients: Examples of Electronic Adherence Monitoring Devices (1 of 3)
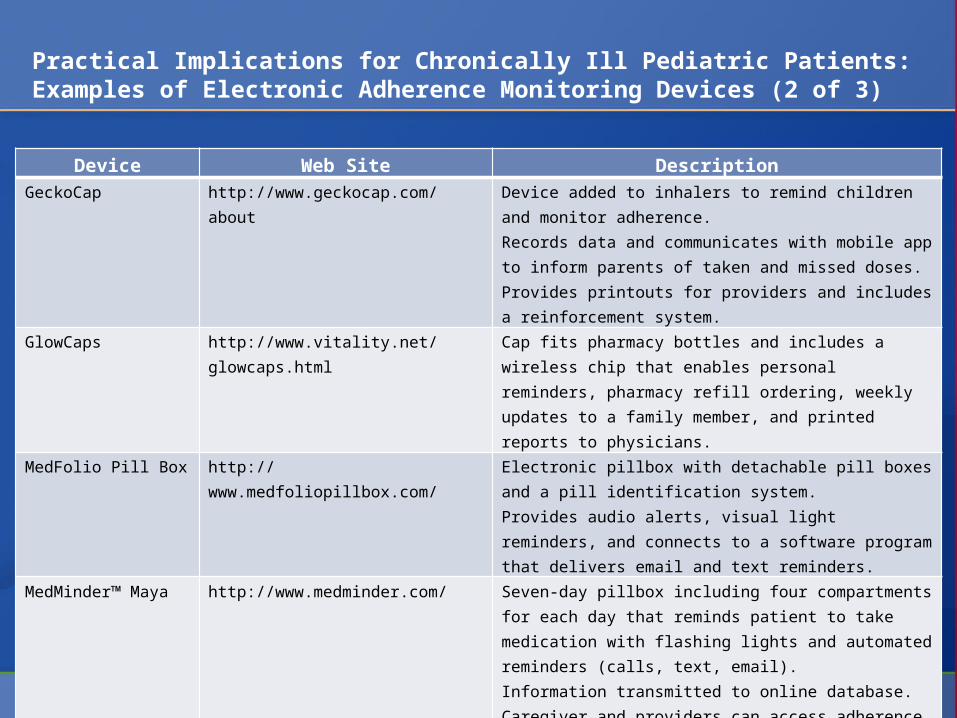
Device Web Site DescriptionGeckoCap http://www.geckocap.com/about Device added to inhalers to remind children and
monitor adherence.Records data and communicates with mobile app to inform parents of taken and missed doses. Provides printouts for providers and includes a reinforcement system.
GlowCaps http://www.vitality.net/glowcaps.html
Cap fits pharmacy bottles and includes a wireless chip that enables personal reminders, pharmacy refill ordering, weekly updates to a family member, and printed reports to physicians.
MedFolio Pill Box http://www.medfoliopillbox.com/ Electronic pillbox with detachable pill boxes and a pill identification system.Provides audio alerts, visual light reminders, and connects to a software program that delivers email and text reminders.
MedMinder™ Maya http://www.medminder.com/ Seven-day pillbox including four compartments for each day that reminds patient to take medication with flashing lights and automated reminders (calls, text, email).Information transmitted to online database.Caregiver and providers can access adherence data.
MEMS http://www.mwvaardex.com/Products/DataCollection/MEMSCap/index.htm
Medication bottles with caps that record the time and date of each opening and closing.
Practical Implications for Chronically Ill Pediatric Patients:Examples of Electronic Adherence Monitoring Devices (2 of 3)
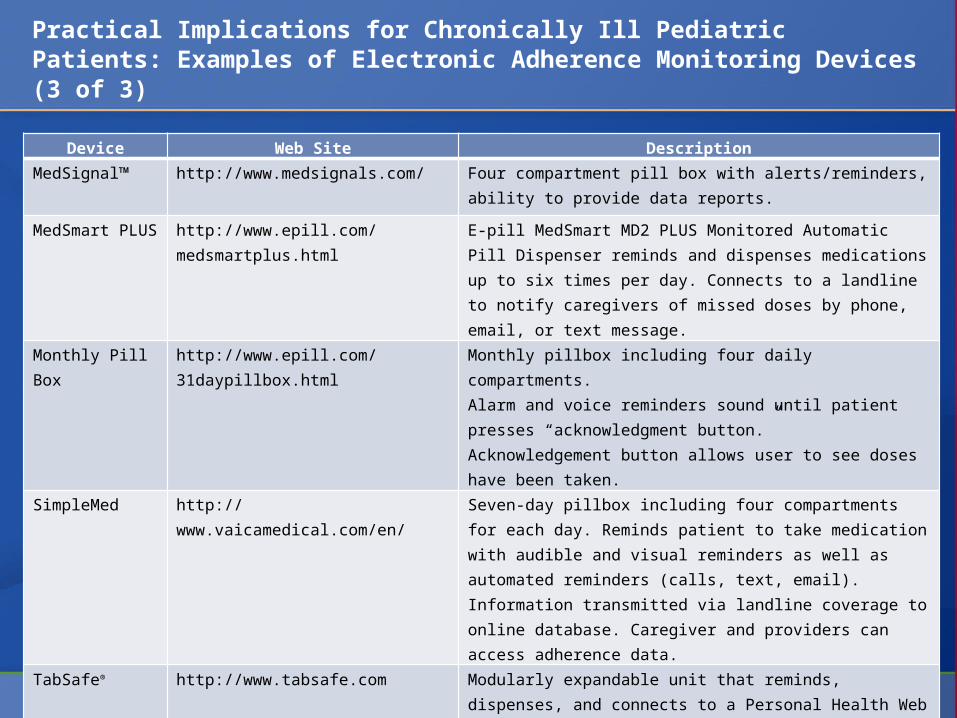
Device Web Site DescriptionMedSignal™ http://www.medsignals.com/ Four compartment pill box with alerts/reminders, ability
to provide data reports.
MedSmart PLUS
http://www.epill.com/medsmartplus.html
E-pill MedSmart MD2 PLUS Monitored Automatic Pill Dispenser reminds and dispenses medications up to six times per day. Connects to a landline to notify caregivers of missed doses by phone, email, or text message.
Monthly Pill Box
http://www.epill.com/31daypillbox.html
Monthly pillbox including four daily compartments.Alarm and voice reminders sound until patient presses “acknowledgment button.”Acknowledgement button allows user to see doses have been taken.
SimpleMed http://www.vaicamedical.com/en/ Seven-day pillbox including four compartments for each day. Reminds patient to take medication with audible and visual reminders as well as automated reminders (calls, text, email). Information transmitted via landline coverage to online database. Caregiver and providers can access adherence data.
TabSafe® http://www.tabsafe.com Modularly expandable unit that reminds, dispenses, and connects to a Personal Health Web site.Programmed on the Web site by patient, caregiver, or health professional.
Practical Implications for Chronically Ill Pediatric Patients: Examples of Electronic Adherence Monitoring Devices (3 of 3)

Inclusion of additional pediatric chronic illness populations in studies focusing on health care use and cost analyses
Randomized controlled trials that use longitudinal data
Evidence-based methods to assess adherence across trials
Studies with a sufficient amount of follow-up time to allow for the realization of long-term consequences from nonadherence
Future Research Needs
McGrady ME, Hommel KA. Pediatrics. 2013 Oct;132(4):730-40. PMID: 23999953.


















