

Medical Necessity Documentation, Challenges and...
79
The audio portion of the conference may be accessed via the telephone or by using your computer's speakers. Please refer to the instructions emailed to registrants for additional information. If you have any questions, please contact Customer Service at 1-800-926-7926 ext. 10. Presenting a live 90-minute webinar with interactive Q&A Medical Necessity Documentation, Challenges and Defense Complying With Federal and State Regulatory Requirements, Demonstrating Reasonable and Necessary Healthcare Services Today’s faculty features: 1pm Eastern | 12pm Central | 11am Mountain | 10am Pacific WEDNESDAY, MARCH 22, 2017 Linda Fotheringill, Co-Founder and Partner, Fotheringill & Wade, Baltimore Sarah Mendiola, Esq., Fotheringill & Wade, Baltimore
Transcript of Medical Necessity Documentation, Challenges and...

The audio portion of the conference may be accessed via the telephone or by using your computer's
speakers. Please refer to the instructions emailed to registrants for additional information. If you
have any questions, please contact Customer Service at 1-800-926-7926 ext. 10.
Presenting a live 90-minute webinar with interactive Q&A
Medical Necessity Documentation,
Challenges and Defense Complying With Federal and State Regulatory Requirements,
Demonstrating Reasonable and Necessary Healthcare Services
Today’s faculty features:
1pm Eastern | 12pm Central | 11am Mountain | 10am Pacific
WEDNESDAY, MARCH 22, 2017
Linda Fotheringill, Co-Founder and Partner, Fotheringill & Wade, Baltimore
Sarah Mendiola, Esq., Fotheringill & Wade, Baltimore

Tips for Optimal Quality
Sound Quality
If you are listening via your computer speakers, please note that the quality
of your sound will vary depending on the speed and quality of your internet
connection.
If the sound quality is not satisfactory, you may listen via the phone: dial
1-866-927-5568 and enter your PIN when prompted. Otherwise, please
send us a chat or e-mail [email protected] immediately so we can
address the problem.
If you dialed in and have any difficulties during the call, press *0 for assistance.
Viewing Quality
To maximize your screen, press the F11 key on your keyboard. To exit full screen,
press the F11 key again.
FOR LIVE EVENT ONLY
Continuing Education Credits
In order for us to process your continuing education credit, you must confirm your
participation in this webinar by completing and submitting the Attendance
Affirmation/Evaluation after the webinar.
A link to the Attendance Affirmation/Evaluation will be in the thank you email
that you will receive immediately following the program.
For additional information about continuing education, call us at 1-800-926-7926
ext. 35.
FOR LIVE EVENT ONLY

Program Materials
If you have not printed the conference materials for this program, please
complete the following steps:
• Click on the ^ symbol next to “Conference Materials” in the middle of the left-
hand column on your screen.
• Click on the tab labeled “Handouts” that appears, and there you will see a
PDF of the slides for today's program.
• Double click on the PDF and a separate page will open.
• Print the slides by clicking on the printer icon.
FOR LIVE EVENT ONLY
March 22, 2017 Strafford Webinar Panel
Presented by: Linda Fotheringill, Esq. Sarah Mendiola, Esq., LPN, CPC
Complying With Federal and State Regulatory Requirements, Demonstrating Reasonable and
Necessary Healthcare Services

Fotheringill & Wade, LLC. Presenters
Linda Fotheringill, Esq. Co-Founder and Principal
Sarah Mendiola, Esq., LPN, CPC Senior Attorney | Director of Clinical Services
6

Overview
Appropriate Documentation of Medical Necessity
Identifying Risks Understanding government’s legal theories in medical
necessity investigations
Recent Cases, Legal Actions and Settlements Defenses available to providers
Best Practices for Ensuring Compliance with Regulations Ensuring appropriate documentation
7
Medical
Necessity
8

How is “Medical Necessity” Defined?
SSA Section 1862 (a) (1) (A) “Notwithstanding any other
provision of this title, no payment may be made under part A or part B for any expenses incurred for items or services— (1)(A) which, except for items
and services described in a succeeding subparagraph, are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member…”
Definitions vary from state to state, but are typically similar regarding current care standards and cost-effectiveness.
Subjective Example - Georgia
“care based upon generally accepted medical practices in light of conditions at the time of treatment… ”
State Federal/Medicare
9

Federal/Medicare: Medical Necessity Layers
Social Security Act
Federal Register IPPS and OPPS Proposed & Final Rules
Code of Federal Regulations
Medicare Manuals CMS' program issuances, day-to-day operating instructions, policies, and
procedures that are based on statutes, regulations, guidelines, models, and directives.
National and Local Coverage Determinations
Medicare Learning Network MLN Matters Articles
10
CMS presumes a healthcare provider’s knowledge of every word of every statute, rule, NCD/LCD, manual, transmittal, etc.
Administrative Law Judge comment in an Unfavorable ALJ Decision: “The Provider was unquestionably aware of the CMS regulations,
manuals and rulings, CMS bulletins, past unfavorable CMS contractor actions and the lack of substantiating medical records. See 42 CFR Section 411.406(e) (knowledge presumed from experience and constructive notice of CMS publications).”
Federal/Medicare: Medical Necessity Layers, cont.
11

Determining Medicare Medical
Necessity Example: Total Knee
Replacement
12

Can the Entire Inpatient Claim be Denied as Not Medically Necessary?
“When a procedure was not medically necessary, the contractor shall follow these guidelines: If the admission was for the sole purpose of the performance
of the non-covered procedure, and the beneficiary never developed the need for a covered level of service, deny the admission;
If the admission was appropriate, and not for the sole purpose of performing the procedure, deny the procedure (i.e., remove from the DRG calculation), but approve the admission…”(MPIM, Ch. 6, Section 6.5.4)
13

Example Medical Record Documentation: Total Knee Replacement
Mr. Smith is a 69 y/o male with a hx of osteoarthritis of the right knee, becoming increasingly severe. His pain has been worsening over the last 6 years to the point that he is no longer able to climb the stairs in his home. NSAIDs have not been effective. He has participated in a therapy program for the last 2 months and is not exhibiting any improvement. The pt has received a series of injections to the knee over the past 6 years which were helpful at first, but have not been helpful as of late. Risks and benefits to TKA discussed, patient voiced understanding.
14
Federal/Medicare: Medical Necessity Layers
SSA? “…reasonable and necessary for the diagnosis or treatment of
illness or injury or to improve the functioning of a malformed body member…”
Federal Register/Final Rule? Consider that this is an inpatient only procedure according to the
CMS-1656-FC-2017 OPPS FR, Addendum E.
CFR?
Medicare Manuals?
NCD/LCD?
MLN Matters Article?
15

16

MLN Matters Number: SE 1236
https://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnmattersarticles/downloads/se1236.pdf
17
Document Medical Necessity to Avoid Denial of Claims CMS recognizes that joint replacement surgery is reserved for patients whose symptoms have not responded to other treatments. To avoid denial of claims for major joint replacement surgery, the medical records should contain enough detailed information to support the determination that major joint replacement surgery was reasonable and necessary for the patient. Progress notes consisting of only conclusive statements should be avoided. Consequently, the medical record must specifically document a complete description of the patients’ historical and clinical findings. Examples of such information may include: History: • Description of the pain (onset, duration, character,
aggravating, and relieving factors); • Limitation of Activities of Daily Living (ADLs) – specify; • Safety issues (e.g. falls); • Contraindications to non-surgical treatments; • Listing and description of failed non-surgical treatments such
as: • Trial of medications (for example, NSAIDs); • Weight loss; • Physical therapy; • Intra-articular injections; • Braces, orthotics or assistive devices.
Physical Examination: • Deformity; • Range of motion; • Crepitus; • Effusions; • Tenderness; • Gait description (with/without mobility aides). Investigations: • Results of applicable investigations (e.g. plain radiographs). Clinical Judgment: • Reasons for deviating from a stepped-care approach.

MLN Matters Number: SE 1236, cont.
https://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnmattersarticles/downloads/se1236.pdf
Example of a medical record that may result in a DENIED claim Mrs. Smith is a female, age 70, with chronic right knee pain. She states she is unable to walk without pain and pain meds do not work. Therefore, she needs a total right knee replacement. Example of a medical record with more detail and support of medical necessity History: Mrs. Smith is a 70-year-old female who is suffering from end-stage Osteoarthritis (OA) of her right knee, worsening gradually over the past 10 years. Treatment has included NSAIDs which have not effectively relieved her pain/inflammation and which have recently begun to cause her gastric distress. She has also participated in an exercise program/physical therapy for the past 3 months without functional improvement. Sometimes the pain keeps her awake at night. She is using a cane and is no longer able to climb the five steps to her front door. Personal safety is compromised as she had falls x 3 in attempting the stairs to her home entrance. Her knee pain and stiffness limit her ability to perform ADLs. She cannot walk from her bedroom to her kitchen without stopping to rest. Investigations: X-ray (7/2/11): right knee shows joint space narrowing along with marginal osteophytes. Impression: Total Knee Arthroplasty (TKA) indicated.
18
Is this Surgical Procedure Medically Necessary?
SSA? “…reasonable and necessary for the diagnosis or treatment of
illness or injury or to improve the functioning of a malformed body member…”
Federal Register/Final Rule? Was the patient appropriately admitted as an inpatient?
Is there an active LCD for the state in which the service was performed?
Does the documentation meet the suggested guidance outlined in SE 1236?
19
What Defenses Do We Have if the Claim is Denied as Not Medically Necessary?
Clinical Arguments
Documentation should be reviewed by a clinician familiar with CMS’s specific requirements.
Obtain physician records for appeal and/or an affidavit to support medical necessity.
Inpatient Only Procedure
20

What Defenses Do We Have if the Claim is Denied as Not Medically Necessary?, cont.
Legal Arguments LCD
42 CFR §405.1060 and 42 CFR §405.1062 require the ALJ to apply an NCD to the facts of a specific claim, but permit the ALJ discretion when reviewing a denial based on an LCD or “other program memoranda” - LCDs and other policies are not binding on the ALJ and MAC, but must be given “substantial deference”.
MLN Matters Article
SE 1236 states: “The Centers for Medicare & Medicaid Services (CMS) is publishing this article as an educational guide to improve compliance with documentation requirements for major joint replacement surgery. The article presents suggestions for documenting medical necessity to avoid denial of Medicare Fee-For-Service (FFS) claims. The use of this guide is not mandatory and does not guarantee payment.”
21

Medical Necessity & Level of Care Determinations
Inpatient vs. Observation
22

How is an “Inpatient” Defined? Federal/Medicare 42 CFR §412.3
(a) “…an individual is considered an inpatient of a hospital, including a critical access hospital, if formally admitted as an inpatient pursuant to an order for inpatient admission by a physician or other qualified practitioner…”
(d)(1) “…an inpatient admission is generally appropriate for payment under Medicare Part A when the admitting physician expects the patient to require hospital care that crosses two midnights.”
Medicare Benefit Policy Manual, Chapter 1, Section 10 Factors to be considered when making the decision to admit include such things
as: The severity of the signs and symptoms exhibited by the patient;
The medical predictability of something adverse happening to the patient;
The need for diagnostic studies that appropriately are outpatient services (i.e., their performance does not ordinarily require the patient to remain at the hospital for 24 hours or more) to assist in assessing whether the patient should be admitted; and
The availability of diagnostic procedures at the time when and at the location where the patient presents.
23

How is an “Inpatient” Defined?, cont.
State Examples
Georgia Rules and Regulations for Hospitals 111-8-40-.02 (g) “Inpatient means a person admitted to a hospital for an intended length of
stay of twenty-four (24) hours or longer.”
Montana Administrative Rule 37.86.2901 (26) “‘Inpatient’ means a person who has been admitted to a hospital for bed
occupancy for purposes of receiving inpatient hospital services. A person generally is considered an inpatient if formally admitted as an inpatient with an expectation that the client will remain more than 24 hours. The physician or other practitioner is responsible for deciding whether the client should be admitted as an inpatient.”
24
How is an “Inpatient” Defined?, cont 2.
Georgia Medicaid Manual 904.7
Inpatient admissions of less than twenty-four hour’s duration are subject to review for medical necessity of admission. A length of stay less than twenty-four hours may be considered inpatient if the services can be provided only on an inpatient basis. Outpatient services billed as inpatient are subject to recoupment after review for medical necessity and cannot be re-billed as outpatient.
25

Current Rules for Inpatient Status
Payor Inpatient Rule
Medicare Two Midnight Rule
Medicaid State regulatory definitions for medical necessity
Medicaid MCOs Typically use evidence based, clinical guidance such as MCG or InterQual, HOWEVER contract governs
Commercial Typically use evidence based, clinical guidance such as MCG or InterQual, HOWEVER contract governs
Medicare Advantage Two Midnight Rule (?); HOWEVER contract governs
26

Current Rules for Observation Status
Payor Pay 1 – 48 hours of observation?
Pay > 48 hours of observation?
Authorization required?
Medicare Yes – But See “MOON” Regulation.
Not > 48 hours unless “rare and exceptional” (Auto Edit!)
No
Maryland Medicaid Yes No -may only reimburse up to 24 hours in an outpatient setting; applies to MD
Medicaid, MCOs, and Behavioral Health.
Med review used to be needed for > 24 hours, now won’t be paid
UHC Community Plan
Yes – up to 24 hours No See above
Carefirst BlueChoice requires authorization
Aetna Yes – up to 24 hours; then MN review
No established maximum –May pay
Medical necessity review for > 24 hours
27

Medicare & the Two-Midnight
Rule
28

Two-Midnight Rule
Effective for DOS on or after 10/01/13
Has undergone several modifications/updates since its inception.
Requirements
Inpatient Order
Expectation of hospitalization spanning two midnights Exceptions:
Inpatient Only Procedures
“Unforeseen circumstances”
“Case by case” review
29

Updates to the Two-Midnight Rule
CMS issued a revised policy regarding exceptions to the 2 Midnight rule in CMS-1633-F
For admissions not meeting the two midnight benchmark, Part A payment is appropriate on a case-by-case basis where the medical record supports the admitting physician’s determination that the patient requires inpatient care, despite the lack of a 2 midnight expectation.
The QIOs will consider complex medical factors such as history and comorbidities, the severity of signs and symptoms, current medical needs, and the risk of an adverse event to determine whether the medical record supports the need for inpatient hospital care. These cases will be approved by the QIOs when the other requirements are met. 30
Updates to the Two-Midnight Rule, cont.
This update is codified in 42 CFR 412.3 (d)(3) as of November 13, 2015
(d) (3) Where the admitting physician expects a patient to require hospital care for only a limited period of time that does not cross 2 midnights, an inpatient admission may be appropriate for payment under Medicare Part A based on the clinical judgment of the admitting physician and medical record support for that determination. The physician's decision should be based on such complex medical factors as patient history and comorbidities, the severity of signs and symptoms, current medical needs, and the risk of an adverse event. In these cases, the factors that lead to the decision to admit the patient as an inpatient must be supported by the medical record in order to be granted consideration.
31
Two-Midnight Rule: Example of Achievable Best Practice Documentation
This is an 84 year old patient admitted for treatment of a COPD exacerbation. She has multiple comorbid conditions including diabetes, CHF, and coronary artery disease. She is at risk for rapid deterioration, respiratory failure, and cardiac ischemia and requires IV antibiotics, frequent nebulizer treatments, and frequent vital signs. I expect that she will require at least two midnights of hospitalization this episode because she typically requires 2-3 days of IV steroids and has increased oxygen needs during these exacerbations.
32
Two-Midnight Rule: Current Audits QIO review
Two Midnight initial patient status reviews resumed on 09/12/16.
MAC review Reviews unrelated to patient status (e.g., coding reviews, reviews to
determine the medical necessity of procedures, diagnostic studies, etc.).
RAC review May conduct patient status reviews only for those providers that have been
referred by the QIO as exhibiting persistent noncompliance with Medicare payment policies. CMS awarded new contracts on 10/31/16.
Probe reviews Conducted for stays > 2 midnights to monitor for evidence of gaming,
abuse, or delays in an effort to meet the Two Midnight presumption of medical necessity (CERT, FATHOM, PEPPER).
33
Two-Midnight Rule: Audits
KEPRO, one of the the BFCC-QIOs states on its website: “KEPRO utilizes both non-physician and physician reviewers for its
review process. It has chosen to utilize a commercial screening tool, InterQual, to aid its nonphysician reviewers with the medical necessity review portion of these reviews. Should the documentation fail the initial utilization review screening, the medical record will be provided to a physician reviewer for his/her clinical review.”
“NOTE: CMS considers the use of screening criteria as only one tool that should be utilized by contractors to assist them in making an inpatient hospital claim determination.” (MLN Matters Number: SE 1037)
35
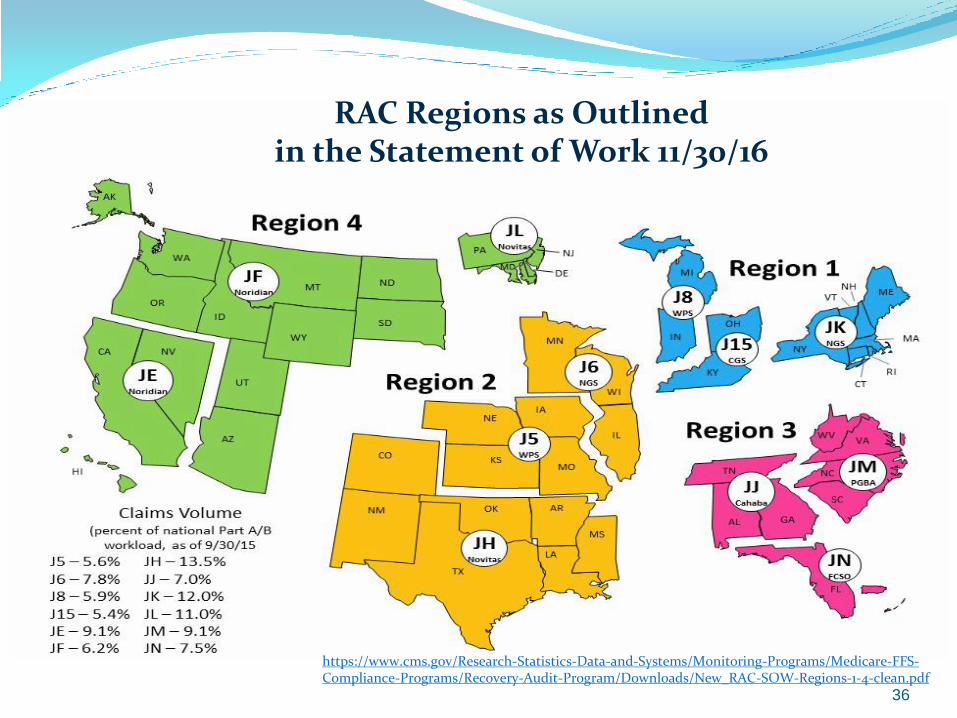
RAC Regions as Outlined in the Statement of Work 11/30/16
https://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medicare-FFS-Compliance-Programs/Recovery-Audit-Program/Downloads/New_RAC-SOW-Regions-1-4-clean.pdf 36
Two-Midnight Rule: Benchmark Presumption that the claim is appropriately payable as a Part
A claim if admission is 2+ midnights.
The clock starts when treatment starts: Triage excluded
Waiting room excluded
Still not actually an inpatient until admission is ordered by a physician Claims reflecting one day of treatment will likely be chosen for audit or pre-pay denial,
but may still be appropriate for Part A reimbursement.
The potential for denials still exists in a two midnight stay Delay in services
Delay in discharge
Hospitalization not medically necessary Care guidelines can be useful to support the need for hospitalization vs. outpatient
care
37

Two-Midnight Rule: General Rule for Expected 2+ Midnight Stays If an unforeseen circumstance results in a shorter length of stay
than expected, Part A payment may still be made. The circumstances must be documented in the medical record. Examples: Death
Transfer to another facility
AMA departure
Hospice election
Unexpected recovery
QIOs will consider “complex medical factors” that support a reasonable expectation of the needed duration of the stay.
38

Two-Midnight Rule: General Rule for Expected 0-1 Midnight Stays
Previously CMS indicated that these claims should be billed as outpatient claims.
Procedures defined as “inpatient only” are an exception.
Revised exceptions policy pursuant to CMS-1633-F: “… for admissions not meeting the two midnight benchmark, Part A
payment is appropriate on a case by case basis where the medical record supports the admitting physician’s determination that the patient requires inpatient care, despite the lack of a 2 midnight expectation.”
QIOs will consider “complex medical factors.”
39

Keys to a Successful Defense
Review the record for:
Inpatient Order
Documentation as to WHY inpatient care is required
Complex medical factors
Or, is this an inpatient only procedure or newly initiated mechanical ventilation?
Review the record for:
Inpatient order
Documentation as to WHY admission is appropriate
Documentation to support the expectation of the needed duration
Or, were there “unforeseen circumstances” that occurred?
Inpatient Stay Expected
0-1 Midnight
Inpatient Stay Expected
2 Midnights or More
40
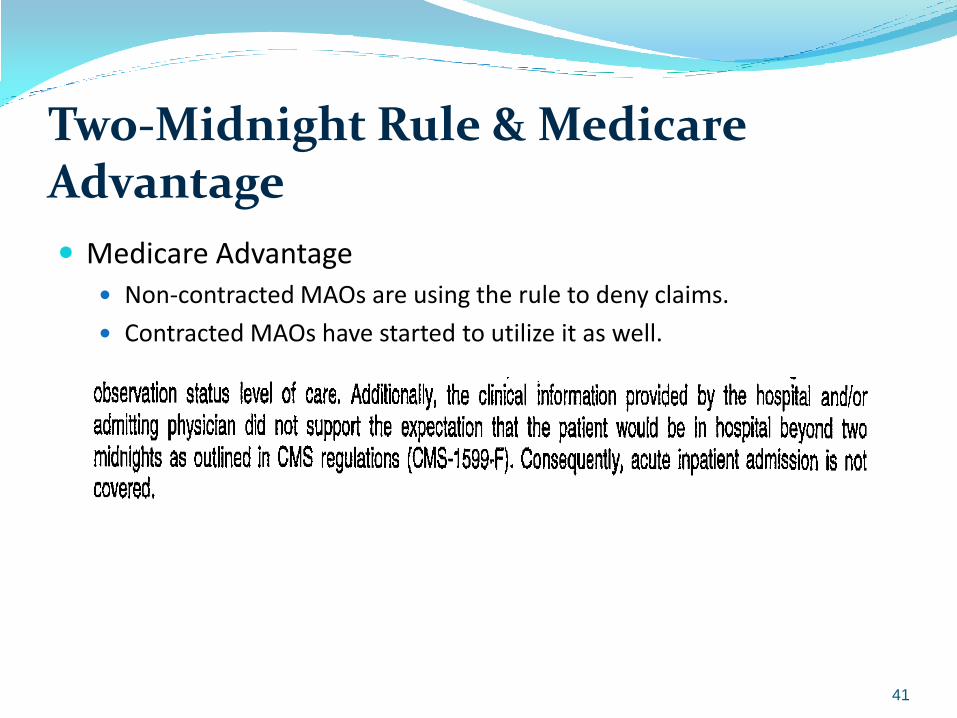
Two-Midnight Rule & Medicare Advantage
Medicare Advantage Non-contracted MAOs are using the rule to deny claims.
Contracted MAOs have started to utilize it as well.
41

Challenges & Risks
42

Testimony of Gloria Jarmon, Deputy Inspector General for Audit Services, OIG – April 30, 2014 Hearing before House Committee on Ways and Means:
“Ideas to Improve Medicare Oversight To Reduce Waste, Fraud, and Abuse”
“Fighting waste, fraud, and abuse in Medicare and other Department programs is a top priority. We use a range of tools in this fight, including audits, evaluations, investigations, enforcement authorities, and educational outreach.”
“The key takeaway from my testimony today is that more action is needed from (CMS), its contractors, and the Department to reduce improper Medicare payments and billings and improve oversight of its Medicare contractors. Reducing improper payments and improving the oversight of contractors are two of the Department’s top management and performance challenges and are critical to reducing Medicare waste, fraud, and abuse.”
43

Center for Program Integrity
Created in 2010 to strategically combat fraud, waste and abuse with a coordinated approach in Medicare and Medicaid.
Accomplished through:
Enhanced provider enrollment activities;
Proactive data analysis;
Close collaboration among law enforcement;
Subject matter experts and program integrity contractors; and/or
The investigation of complaints from various sources; provider on-site visits; and beneficiary interviews.
44

Multiple Entities/Contractors Federal Medicare Administrative Contractors
(MAC)
Recovery Audit Contractors (RAC)
Comprehensive Error Rate Testing (CERT)
Quality Improvement Organizations (QIO)
Unified Program Integrity Contractors (UPIC) Zone Program Integrity Contractors (ZPIC)
Supplemental Medical Review Contractors (SMRC)
Office of Inspector General (OIG)
Health Care Fraud Prevention and Enforcement Action Team (HEAT) Joint effort between HHS & DOJ
Medicare Fraud Strike Force
State
Medicaid RACs
Medicaid Integrity Contractors (MIC) https://www.cms.gov/Medicare-
Medicaid-Coordination/Fraud-Prevention/FraudAbuseforProfs/State-Program-Integrity-Review-Reports-List.html
Office of Inspector General (OIG) Medicaid Fraud Control Units
45
ZPIC: Medical Review Function An investigation is the expanded analysis performed on leads
once such lead is vetted and approved by CMS to be opened as an investigation. The ZPIC shall focus its investigation in an effort to establish the facts and the magnitude of the alleged fraud, waste, or abuse and take any appropriate action to protect Medicare Trust Fund dollars. (MPIM, Chapter 4 Section 4.7)
Reactive Referrals from MACs/CMS, HHS OIG tipline, law enforcement,
whistleblowers
Proactive Data-mining across years of claims data
Fraud Prevention System (FPS) CMS-operated analytical and predictive tool
46

ZPIC: Extrapolation
Other reviewers—from MACs to HHS OIG—can use extrapolation, but they are a key feature of the ZPIC program.
The purpose of extrapolation is to save the administrative costs that would be necessary to investigate each claim.
When a ZPIC finds what it believes is a “sustained or high level of payment error,” it can use sampling and extrapolation.
CMS has not defined a sustained or high level.
The determination of a sustained or high level of error is not subject to judicial review.
(MPIM, Ch. 8, Section 8.4) 47

ZPIC: Case Study
PSC conducted proactive data analysis.
In 2010, PSC sent written request to Medical Records Administrator for medical records associated with claim sample
Three years later, ZPIC sent “Post Payment Review Results & Overpayment Determination” to CEO Alleged insufficient documentation to justify medical necessity
Denial premised on non-compliance with LCD’s detailed service and documentation requirements
Extrapolation Universe of 500 claims
Sample of 50 claims, all denied post-payment
$250,000.00 at issue on sample claims
$2,250,000.00 “lower limit” (total estimate $2,500,000.00)
48

ZPIC: Case Study, cont.
Worked quickly to put recoupment on hold
Within 30 days under the provisions of Section 935 of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (“MMA”)
Developed arguments on both the audit process and the claim details
Analyzed LCD at issue, applied it to facts of each claim
Attacked quality & promptness of notice
Sent appeals—one for each claim and one for the extrapolation
49

ZPIC: Responding to a ZPIC Audit
Assemble all medical records and other pertinent documentation.
Review all relevant Medicare criteria and regulations
Have properly trained team and/or attorney evaluate the cases The key skill is experience interpreting medical records in light of complex
regulations & often fuzzy criteria and formulating a clear, targeted response.
Ordinary denial management processes are likely under-prepared for the scope of a ZPIC audit and under-skilled for what’s at stake.
50

LCD Language
51

LCD Language, cont.
52

Fraud, Waste & Abuse
53

The False Claims Act, 31 U.S.C. §§ 3729-3733
Knowingly submitting a false or fraudulent claim for payment can lead to:
Treble damages; and
Fines of $5,500-$11,000 per claim
For purposes of this regulation, the terms “knowing” and “knowingly” mean that a person, with respect to information:
(1) has actual knowledge of the information;
(2) acts in deliberate ignorance of the truth or falsity of the information; or
(3) acts in reckless disregard of the truth or falsity of the information, and no proof of specific intent to defraud is required.
54

The False Claims Act, Statute of Limitations
A civil action under section 3730 may not be brought — more than six years after the date on which the violation of
section 3729 is committed, or
more than three years after the date when facts material to the
right of action are known or reasonably should have been known by the official of the United States charged with responsibility to act in the circumstances, but in no event more than 10 years after the date on which the violation is committed, whichever occurs last.
55

What is Medicare Fraud? In general, fraud is defined as making false statements or
representations of material facts to obtain some benefit or payment for which no entitlement would otherwise exist. These acts may be committed either for the person’s own benefit or for the benefit of some other party.
Examples of Medicare fraud may include: Knowingly billing for services that were not furnished and/or
supplies not provided, including billing Medicare for appointments that the patient failed to keep; and
Knowingly altering claims forms and/or receipts to receive a higher payment amount.
56
What is Medicare Abuse? Practices that, either directly or indirectly, result in unnecessary costs to the
Medicare program.
“Abuse appears quite similar to fraud except that it is not possible to establish that abusive acts were committed knowingly, willfully, and intentionally.”
Examples of Medicare abuse may include:
Misusing codes on a claim;
Charging excessively for services or supplies; and
Billing for services that were not medically necessary or services that do not meet professionally recognized standards.
Both fraud and abuse can expose providers to criminal and civil liability.
57
Per Medicare Learning Network: “…there is no precise measure of health care fraud…”
Fraud?
Abuse?
Improper Payment?
Reasonable Minds can Differ?
58

Question:
Can billing Medicare for [insert almost any service you provide here] when the documentation does not support medical necessity per CMS criteria be considered fraud or abuse? What about when the denial is not appealed?
What about where there are many cases with this issue?
59
The False Claims Act and Enforcement
If such activity is considered fraud or abuse, Providers are exposed to civil and criminal liability.
Exclusion from Federal Healthcare Programs
Loss of Licensure
Corporate Integrity Agreement
Civil monetary penalties
Criminal penalties
Imprisonment
Criminal fines
60

OIG Semi-Annual Reports to Congress
OIG Semi-Annual Report Period
Criminal
Actions
Civil Actions
Investigative Receivables Due to
HHS
Investigative Receivables for
Non-HHS
April 1 – Sept 30, 2016
381 311 $1.62 Billion + $607.4 Million +
Oct 1 – March 31, 2015
384 379 $1.68 Billion + $332.6 Million +
April 1 – Sept 30, 2015
378 347 $756.9 Million + $139.4 Million +
61

Qui Tam Provision Anyone may initiate the law suit on behalf of the
government! (31 U.S.C. § 3730)
USA ex rel. Karin Berntsen v. Prime Healthcare Services, Inc. The Relator was a registered nurse employed by Defendant
Alvarado Hospital when Prime acquired it in 2010.
The suit alleges that Prime Healthcare defrauded the federal government of millions of dollars by billing Medicare for medically unnecessary inpatient short-stay admissions, which should have been classified as outpatient or observation cases. Complaint alleged that the hospital “engaged in a systematic practice of maximizing revenues by, among other things, inducing physicians who work at Prime hospitals to increase the number of inpatient care admissions of Medicare beneficiaries who visit the Emergency Department (ED) at a Prime hospital, without regard to whether inpatient admission is medically necessary.”
62

OIG Transcript for Audio Podcast: False Claims Act
“False Claims Act cases are in the news and many involve large companies, such as drug and device manufacturers or pharmaceutical companies. But there also are many cases involving smaller entities and individuals. For example, a recent FCA case involved a cardiologist who allegedly submitted claims to the Federal health care programs for services that were not supported by patient medical records and did not meet the billing criteria. Additionally, the physician allegedly billed separately for services that the government had already paid for as part of a bundled payment for a group of services. To resolve these allegations the doctor paid $435,000 and entered into a 5-year Integrity Agreement.”
63

A Corporate Integrity Agreement (CIA) outlines the obligations an entity agrees to as part of a civil settlement. The organization agrees to the CIA in exchange for the OIG’s
agreement that it will not seek to exclude the entity from participation in Medicare, Medicaid or other Federal healthcare programs.
Often paired with a “Deferred Prosecution Agreement” or “Settlement Agreement.”
Monetary penalties can result from failure to comply with a CIA; a material breach of the CIA constitutes an independent basis for exclusion.
https://oig.hhs.gov/compliance/corporate-integrity-agreements/cia-documents.asp
Corporate Integrity Agreements
64

Recent OIG Civil Monetary Penalties
At least 13 separate settlement agreements during 2016 between the OIG and physician practices/groups for HCPCS code G0452 (molecular pathology procedure; physician interpretation and report) .
Settlements spanned between $10,000 - $66,000!
Allegations were: (1) no consultation request had been made;
(2) no written narrative report by a consultant physician was produced that went beyond the report of the laboratory results; and
(3) no exercise of medical judgment by a consultant physician was required.
65

Recent OIG Criminal and Civil Enforcement March 6, 2017; U.S. Department of Justice
California Clinic Owner Sentenced to 63 Months in Prison
for Role in Occupational Therapy Fraud Scheme
A rehabilitation clinic operator in Los Angeles County was
sentenced to 63 months in prison for his role in a $3.4 million
Medicare fraud scheme that involved billing for occupational
therapy services that were not medically necessary and not
provided.
He was also ordered to pay $2,407,857 in restitution after pleading
guilty on Dec. 15, 2016, to one count of conspiracy to commit
health care fraud.
66
Recent OIG Criminal and Civil Enforcement, cont. February 10, 2017; U.S. Attorney; Southern District of Florida
Plantation Physician and Physician Practice to Pay $750,000 to Resolve False Claims Act Allegations Involving Medically Unnecessary Sinus and Throat Procedures Dr. Paul B. Tartell, an ENT physician practicing in Plantation, Florida and his practice
Paul B. Tartell, M.D., P.L., d/b/a South Florida Sinus & Allergy Center, have agreed to pay $750,000 to resolve allegations that he violated the False Claims Act by billing for surgical endoscopies with debridement and laryngeal stroboscopies that were not provided or not medically necessary.
February 1, 2017; U.S. Attorney; Eastern District of Kentucky Pain Management Physician Resolves False Claims Act Allegations Pain management physician Dr. Robert Windsor has agreed to the entry of a $20
million consent judgment to resolve allegations that he violated the False Claims Act by billing federal health care programs for surgical monitoring services that he did not perform and for medically unnecessary diagnostic tests. Dr. Windsor owned pain management clinics in Georgia and Kentucky that operated under the umbrella of National Pain Care, Inc., including clinics in Lexington, London, Somerset, Hazard, Prestonsburg, and Pikeville, Kentucky.
67

Compliance
68

OIG’s Voluntary Guidance 1998 OIG Compliance Program Guidance (CPG)
2005 Supplemental OIG CPG Should be considered collectively when evaluating or developing a
program
Focus expected to be on areas of potential concern most relevant to the organization
Benefits:
Early detection & reporting minimizes financial loss to Hospital
Demonstrates good faith effort to comply with federal requirements
69
Fraud & Abuse Risk Areas
Submission of accurate claims & information considered “single biggest risk area” for hospitals
Inaccurate or incorrect coding
Upcoding
Unbundling of services
Billing for medically unnecessary services or services not covered
Insufficient documentation
70

Specific Risk Areas for Incorrect Outpatient Procedure Coding
Billing on an outpatient basis for ‘‘inpatient-only’’ procedures
Submitting claims for medically unnecessary services by failing to follow the FI’s local policies
Submitting duplicate claims or otherwise not following the National Correct Coding Initiative guidelines
Submitting incorrect claims for ancillary services because of outdated Charge Description Masters
Improperly billing for observation services—
Improper E&M codes
Same day discharge & Readmissions
Etc., Etc. Etc.
71

Formal Commitment by Hospital’s Governing Body for All Recommended Compliance Program Elements Should be Evident
1. Written standards of conduct, policies & procedures
2. Designation of chief compliance officer & committees that report to CEO & governing body
3. Regular, effective education & training for all affected employees
4. Maintenance of process to receive anonymous complaints
5. System to respond to allegations & enforcement of disciplinary action
6. Use of audits and/or other evaluation techniques
7. Remediation of identified systemic problems
72

Auditing & Monitoring
Regular compliance audits by internal or external auditors with expertise in Federal & State requirements recommended
Pepper (Program for Evaluating Payment Patterns Electronic Report) considered a guide for hospital’s auditing & monitoring activities PEPPER contains a hospital’s data for DRGs & discharges at risk for
improper payment
Three comparison groups: nation, MAC Jurisdiction, & state
Outliers command attention!
73

Responding to an Audit
1. Anticipate the issues that are of concern.
2. Ensure that your response contains a complete medical record.
3. Paginate the documentation you intend to provide.
4. Create index/table of contents to assist the reviewers with finding critical documentation
5. If appropriate, provide a narrative that pulls together the story in association with the relevant regulations.
6. Consider affidavits or attestations to supplement when appropriate.
74

Mandatory Requirements: Self-Identified Overpayments Section 6402(a) of the Affordable Care Act established a new
section 1128J(d) of the Act. Section 1128J(d)(1) of the Act requires a person who has received an
overpayment to report and return the overpayment to the Secretary, the state, an intermediary, a carrier, or a contractor, as appropriate, at the correct address, and to notify the Secretary, state, intermediary, carrier, or contractor to whom the overpayment was returned in writing of the reason for the overpayment.
Section 1128J(d)(2) of the Act requires that an overpayment be reported and returned by the later of: (A) the date which is 60 days after the date on which the overpayment was identified; or (B) the date any corresponding cost report is due, if applicable.
Query: At what point does an overpayment identification occur?
75

Thank You For Your
Attention! Questions? Comments?
76

Linda Fotheringill, Esq. Linda Fotheringill is a nationally recognized expert on Medicare denials and Managed Care/Commercial denials, and is a founding member of Washington & West, LLC and a partner in the law firm of Fotheringill & Wade, LLC. Ms. Fotheringill successfully assists hospitals across the country in overturning “hopeless” denials and generating millions of dollars in revenue that would otherwise be lost for Commercial, Medicare Advantage, or Government payers. Ms. Fotheringill began her career as a hospital-based Physician Assistant. She also had fourteen years of experience in the medical malpractice insurance industry as a claims representative with Medical Mutual Liability Insurance Society of Maryland. Ms. Fotheringill graduated cum laude from the University of Baltimore School of Law and is a member of the Health Care Financial Management Association, American Association of Healthcare Administrative Management, and American and American Association for Justice. In addition, she has presented for numerous professional organizations such as HFMA National and HFMA Regional Chapters, as well as for the American Hospital Association, AAHAM, and NAHAM. Ms. Fotheringill is also a lead developer of Quantum Appeals, a state-of–the art RAC Tracking and Denial Management software application.
77
Sarah Mendiola, Esq., LPN, CPC Sarah Mendiola is a Senior Associate and Director of Clinical Services for the Baltimore, MD-based law firm of Fotheringill & Wade, LLC, and denial Defense Company of Washington & West, LLC. Ms. Mendiola has extensive experience overturning various Medicare, Medicaid, and Commercial plan denials. She has a comprehensive understanding of the Medicare appeals process and has successfully represented numerous clients at Administrative Law Judge hearings; and has obtained favorable results for claim denials from Zone Program Integrity Contractor (ZPIC) audits. She has also represented Maryland providers at administrative hearings for claim denials by Maryland Medicaid and is intimately familiar with the myriad issues surrounding commercial claims as well. Ms. Mendiola graduated from the University of Baltimore School of Law Magna Cum Laude, and holds a Bachelor of Arts in Jurisprudence from the University of Baltimore where she graduated Summa Cum Laude. Ms. Mendiola is also a Licensed Practical Nurse (LPN) in the State of Maryland and is certified as a Certified Professional Coder (CPC) as well. She is admitted to the Maryland Bar and is a member of the American Bar Association.
78

Disclaimer: Please Note The information conveyed in this presentation is for general educational purposes and is not legal advice. The application and impact of laws can vary widely, based on the specific facts involved. Given the constantly changing nature of state and federal laws, there may be omissions or inaccuracies in the information you receive during this program. Accordingly, any information is provided with the understanding that the presenter is not rendering legal, accounting, or other professional advice and services. As such, any information obtained in this presentation should not be used as a substitute for consultation with legal counsel or other professional advisors specifically retained for that purpose. While Fotheringill & Wade, LLC has made every attempt to ensure that the information contained in these materials is generally useful for educational purposes, Fotheringill & Wade, LLC and its agents & employees are not responsible for any errors or omissions or for the results obtained through the use of any information herein.
79


















