Medical Microbiology I - Lecture10
50
MEDICAL MICROBIOLOGY I Lesson 10 Lesson 10 Neisseria and Diseases
-
Upload
carinatingee -
Category
Documents
-
view
23 -
download
3
description
Notes
Transcript of Medical Microbiology I - Lecture10
-
MEDICAL MICROBIOLOGY I
Lesson 10Lesson 10
Neisseria and Diseases
-
Neisseria
2 species, Neisseria gonorrhoeae and
Neisseria meningitidis are strictly human
pathogens
The remaining 8 species are commonly The remaining 8 species are commonly
present on mucosal surfaces of the
oropharynx and nasopharynx, and
occasionally colonise the anogenital mucosal
membranes
-
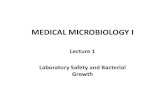
Neisseria
Characteristics:
Aerobic
Gram negative cocci (diplococci) with adjacent sides
flattened together (resembling coffee beans)flattened together (resembling coffee beans)
Non-motile
Do not form endospore
Oxidase-positive
Most produce catalase (combine with the Gram
stain morphology allow for a rapid, presumptive
identification of a clinical isolate)
-
Neisseria
-
Neisseria gonorrhoeae
-
Neisseria gonorrhoeae
1. Physiology and Structure
N. gonorrhoeae is a fastidious organism, requiring complex media for growth and adversely affected by drying and fatty acids
Optimal growth temperature: 35 - 37C Optimal growth temperature: 35 - 37C
A humid atmosphere supplemented with carbon dioxide is either required or enhances growth of N. gonorrhoeae
Cell wall: thin peptidoglycan layer sandwiched between the inner cytoplasmic membrane and the outer membrane
-
Neisseria gonorrhoeae
The outer membrane is not covered with a
true carbohydrate capsule, as is found in N.
meningitidis
Cell surface-capsule like negative charge Cell surface-capsule like negative charge
Fresh clinical isolates have pili (virulence
factor)
The pili are composed of repeating protein
subunits (pilins), whose expression is
controlled by pil gene complex
-
Neisseria gonorrhoeae
Pili mediate attachment to non-ciliated
epithelial cells as well as provide resistance to
killing neutrophils
The Por proteins (formerly protein I) are porin The Por proteins (formerly protein I) are porin
proteins that form pores or channels in the
outer membrane
2 classes: PorA (resistant to serum killing and
thus are commonly associated with
disseminated disease) and PorB
-
Neisseria gonorrhoeae
Opa proteins (opacity proteins; formerly
protein II) are family of membrane proteins
that mediate binding to epithelial cells
Bacteria expressing the Opa proteins appear Bacteria expressing the Opa proteins appear
opaque when grown in culture
These proteins facilitate bacterial adherence to
each other and to eukaryotic cells
-
Neisseria gonorrhoeae
RMP proteins - highly conserved; reduction-
modifiable proteins; formerly protein III
These protein stimulate antibodies that block
serum bacterial activity against N. gonorrhoeaeserum bacterial activity against N. gonorrhoeae
Others: lipooligosaccharide (LOS), lipid A, -
lactamase which degrades penicillin
-
Neisseria gonorrhoeae
2. Pathogenesis and Immunity
Gonococci attach to mucosal cells, penetrate into the cells and multiply, and then pass through the cells into the sub-epithelial space, where infection is establishedspace, where infection is established
Pili - virulence; non-piliated - avirulent
After the initial attachment, Opa protein directs first a tighter association with the host cell surface and then the migration of bacteria into the epithelial cell
-
Neisseria gonorrhoeae
-
Neisseria gonorrhoeae
It was believed that the Por protein protects
the phagocytosed bacteria from intracellular
killing by inhibiting phagolysosome fusion
The gonococcal LOS stimulates the The gonococcal LOS stimulates the
inflammatory response and release of tumour
necrosis factor- (TNF-), which causes most
of the symptoms associated with gonococcal
disease
-
Neisseria gonorrhoeae
IgG3 is the predominant IgG antibody formed in
response to gonococcal infection
Antibodies to LOS can activate complement,
releasing complement component C5a, which has releasing complement component C5a, which has
a chemotactic effect on neutrophils
IgG and secretory IgA1 antibodies directed against
Rmp protein can block this bacteridal antibody
response
People with inherited complement deficiencies are
at considerably greater risk for systemic disease
-
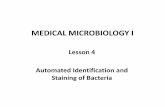
Clinical Diseases
Genital infection in men is primarily restricted to the urethra
A purulent urethral discharge and dysuria develop after a 2-5 days incubation perioddevelop after a 2-5 days incubation period
Approximately 95% of all infected men have acute symptoms
Although complications are rare, epididymitis, prostatitis, and periurethral abscesses can occur
-
Clinical Diseases
-
Clinical Diseases
The primary site of infection in women is the cervix because the bacteria infect the endocervical columnar epithelial cells
The organism cannot infect the squamous epithelial cellsepithelial cells
Symptoms: vaginal discharge, dysuria, and abdominal pain
Ascending genital infection: salpingitis, tuboovarian abscesses, and pelvic inflammatory disease (10 - 20% women)
-
Clinical Diseases
Disseminated infections with septicaemia and infection of skin and joints occur in 1 - 3% of infected women and in a much lower percentage of infected men
Clinical manifestations of disseminated disease: Clinical manifestations of disseminated disease: fever, migratory arthralgias, suppurative arthritis in the wrists, knees and ankles, and a pustular rash on a erythematous base over the extremities but not on the head and trunk
N. gonorrhoeae is a leading cause of purulent arthritis in adult
-
Clinical Diseases
-
Clinical Diseases
Other diseases associated with N.
gonorrhoeae:
Perihepatitis (Fitz-Hugh-Curtis syndrome)
Purulent conjunctivitis, particularly in Purulent conjunctivitis, particularly in
newborns infected during vaginal delivery
(opthalmia neonatorum)
Anorectal gonorrhoea in homosexual men and
pharyngitis
-
Laboratory Diagnosis
Microscopy: Gram stain
Culture: Thayer-Martin medium, chocolate agar
Identification: oxidase-positive (acid produced Identification: oxidase-positive (acid produced oxidatively from glucose but not from other sugars), Gram negative diplococci that grow on chocolate agar
Genetic probes: sensitive, rapid (2 - 4 hrs)
Serology: gonococcal antigen-antibody detected; not recommended
-
Neisseria gonorrhoeae
-
Neisseria meningitidis
1. Physiology and Structure
The meningococci form transparent, non-pigmented colonies on chocolate agar, and their growth is enhanced in a moist atmosphere with 5% carbon dioxideatmosphere with 5% carbon dioxide
Isolates with large polysaccharide capsules appear as mucoid colonies
Meningococci are oxidase-positive and are differentiated from other Neisseria species by the production of acid from oxidation of glucose and maltose but not sucrose or lactose
-
Neisseria meningitidis
-
Neisseria meningitidis
N. meningitidis is subdivided into serogroups and serotypes
13 serogroups, with antigenic differences in their polysaccharide capsule, have been describeddescribed
A, B, C, X, Y and W135
The serotype classification of isolates is based on differences in the proteins in the outer membrane and in the oligosaccharide component of LOS
-
Neisseria meningitidis
Serotype classification has proven useful for
epidemiologic classification and for the
characterisation of virulent strains
All group A meningococci have the same outer- All group A meningococci have the same outer-
membrane proteins and belong to a single
serotype, whereas the meningococci in group
B and C belong to multiple serotypes
-
Neisseria meningitidis
2. Pathogenesis and Immunity
The outcome in a person exposed to N. meningitidis depends on the following 4 factors:
Whether the bacteria are able to colonise the nasopharynx (mediated by pili)nasopharynx (mediated by pili)
Whether specific group- and serotype-specific antibodies are present
Whether systemic spread occurs without antibody-mediated phagocytosis (protection afforded by polysaccharide capsule)
Whether toxic effects (mediated by the LOS endotoxin) are expressed
-
Neisseria meningitidis
Experiments with nasopharyngeal tissue organ
cultures have shown that meningococci attach
selectively to specific receptors for
meningococcal pili on non-ciliated columnar meningococcal pili on non-ciliated columnar
cells of the nasopharynx
Meningococci without pili are less able to bind
these cells
-
Neisseria meningitidisMeningococcal disease occurs in the absence of
specific antibodies directed against the
polysaccharide capsule and other expressed
bacterial antigens
Infants are initially afforded protection by the
passive transfer of maternal antibodiespassive transfer of maternal antibodies
Immunity can be stimulated by colonisation with
N. meningitidis or other bacteria with cross-
reactive antigens (e.g. colonisation with N.
meningitidis sp; exposure to E. coli K1 antigen,
which cross-reacts with the group B capsular
polysaccharide)
-
Neisseria meningitidis
Bactericidal activity also requires the existence
of complement
Patients with deficiencies in C5, C6, C7, or C8 of
the complement system are estimated to be at a the complement system are estimated to be at a
6000-fold greater risk for meningococcal disease
Meningococci are internalised into phagocytic
vacuoles and are able to avoid intracellular
death, replicate, and then migrate to the sub-
epithelial spaces
Protection: anti-phagocytic capsule
-
Neisseria meningitidis
The vascular wall damage associated with meningococcal infection (e.g. endothelial damage, inflammation of vessel walls, thrombosis, disseminated intravascular coagulation) is largely attributed to the action coagulation) is largely attributed to the action of the LOS endotoxin present in the outer membrane
N. meningitidis produces excess membrane fragments that are released into the extracellular space
-
Neisseria meningitidis
This continuous hyper production and release
of endotoxin may cause the severe endotoxic
reaction seen in patients with meningococcal
diseasedisease
-
Clinical Diseases
Meningitidis
The disease usually begins abruptly with headache, meningeal signs, and fever
Very young children may have only non- Very young children may have only non-specific signs, such as fever and vomiting
Mortality approaches 100% in untreated patients but is less than 10% in patients in whom appropriate antibiotic therapy is instituted promptly
-
Clinical Diseases
The incidence of neurologic sequelae is low,
with hearing deficits and arthritis most
commonly
-
Clinical Diseases
Meningococcemia
Septicaemia with or without meningitis is a
life-threatening disease
Thrombosis of small blood vessels and multi- Thrombosis of small blood vessels and multi-
organ involvement are characteristic clinical
features
-
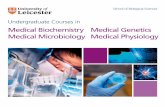
Clinical Diseases
-
Clinical Diseases
Small petechial skin lesions on the trunk and
lower extremities are common and may
coalesce to form larger haemorrhagic lesions
Overwhelming disseminated intravascular Overwhelming disseminated intravascular
coagulation with shock, together with the
bilateral destruction of the adrenal glands
(Waterhouse-Friderichsen syndrome), may
ensue
-
Clinical Diseases
A milder, chronic septicaemia has also been
observed
Bacteremia can persist for days or weeks, and
the only signs of infection are a low-grade the only signs of infection are a low-grade
fever, arthritis, and petechial skin lesions
The response to antibiotic therapy in patients
with this form of the disease is generally
excellent
-
Clinical Diseases
Other syndromes
Pneumonia, arthritis, and urethritis
Meningococcal pneumonia is usually preceded by a respiratory tract infection
Symptoms: cough, chest pain, rales, fever and Symptoms: cough, chest pain, rales, fever and chills
Evidence of pharyngitis is observed in most affected patients
Prognosis in patients with meningococcal pneumonia is good
-
Laboratory Diagnosis
Most useful specimens for the detection of
meningococci are blood and cerebrospinal
fluid (CSF)
Although the organism is present in the blood Although the organism is present in the blood
of most patients with systemic disease,
additives in blood culture broths can be toxic
for Neisseria and can therefore inhibit or delay
bacterial growth
-
Laboratory Diagnosis
Because the bacterial count in CSF is high, the Gram negative diplococci are readily seen within polymorphonuclear leukocytes on Gram stain
Counter-immunoelectrophoresis or the agglutination of latex particles used to detect soluble polysaccharide antigen
N. meningitidis is relatively non-immunogenic and does not react with the test antigens
-
Treatment, Prevention and Control
Antibiotic therapy and supportive management for the complications of meningococcal disease have significantly reduced the mortality associated with the diseasedisease
Sulfonamides - successful; however, widespread resistance to the agents has now negated their effectiveness
Penicillin - more common; resistancy also becoming common
-
Treatment, Prevention and Control
Because penicillin therapy remains effective
against most of these isolates, the clinical
significance of low-level resistance is unknown
Resistance to chloramphenicol and rifampin Resistance to chloramphenicol and rifampin
has been observed, so isolates from patients
whose does not respond to empirical therapy
should be evaluated carefully for antibiotic
resistance
-
Treatment, Prevention and Control
Eradication of the pool of healthy carriers of
N. meningitidis is unlikely
Therefore, efforts have been concentrated on
the prophylactic treatment of people exposed the prophylactic treatment of people exposed
to diseased patients and on the enhancement
of immunity to the serogroups most
commonly associated with the disease
-
Treatment, Prevention and Control
Sulfonamides were used for prophylaxis, but now
they are no longer considered reliable
Penicillin is ineffective in eliminating the carrier
statestate
Minocycline and rifampin have been effectively for
antibiotic-mediated chemoprophylaxis because
these antibiotics are secreted into the mucus
However, toxic effects have been associated with
minocycline, and rifampin-resistant N. meningitidis
can arise during treatment
-
Treatment, Prevention and Control
Prophylaxis with a sulfonamide is
recommended for people exposed to
susceptible strains, with rifampin used for
those with sulfonamide-resistant strainsthose with sulfonamide-resistant strains
Vaccines directed against the group-specific
capsular polysaccharides have been
developed for antibody-mediated
immunoprophylaxis
-
Treatment, Prevention and Control
A polyvalent vaccine effective against
serogroups A, C, Y, and W135, which can be
administered to children older than 2 years,
has been developedhas been developed
The vaccine cannot be administered to
children in younger age groups because they
do not respond to polysaccharide antigens
-
Treatment, Prevention and Control
The group B polysaccharide is a weak immunogen and cannot induce a protective antibody response
Thus, immunity to group B N. meningitidis must develop naturally after exposure to cross-develop naturally after exposure to cross-reacting antigens
Vaccination with a suspension containing serogroup A can be used for control of an outbreak of disease, for travelers to hyper-endemic areas, or for people at increased risk for disease
-
Other Neisseria Species
Neisseria species such as Neisseria sicca and
N. mucosa are commensal organisms in the
oropharynx
Implicated in isolated cases of meningitis, Implicated in isolated cases of meningitis,
osteomyelitis, and endocarditis as well as
bronchopulmonary infection, acute otitis
media, and acute sinusitis
-
Other Neisseria Species
The observation of many Gram negative
diplococci associated with inflammatory cells
in a well-collected respiratory specimen would
support the etiologic role of these organismssupport the etiologic role of these organisms
Most isolates of N. sicca and N. mucosa are
susceptible to penicillin, although low-level
resistance caused by altered penicillin-binding
protein has been observed