Medical Eye Care Management and ICD-10...
157
Medical Eye Care Management and ICD-10 Implementation Jason R. Miller, OD, MBA, FAAO
Transcript of Medical Eye Care Management and ICD-10...

Medical Eye Care Management and
ICD-10 Implementation
Jason R. Miller, OD, MBA, FAAO

Professional Disclosures
! Does not have financial interest in any of the products mentioned. The speaker has received honoraria for writing, lecturing, acting in an advisory capacity or research from: Alcon Laboratories, Allergan, Aton Pharma, Bausch+ Lomb, CooperVision, Hoya, Ista, Revolution EHR, Synergeyes, Valeant and Vistakon
! Consults with PMI, LLC and Chuck Brownlow for Billing and Coding
! Consults with RevolutionEHR

! http://www.cms.gov/
! http://www.medicare.gov/default.aspx
! https://www.vsp.com/
! http://aoacodingtoday.prsnetwork.com/
! http://www.pmi-eyes.com
! http://www.ReimbursementPlus.com/
Resources

National Resources ! Current Procedural Terminology, CPT© American
Medical Association
! Only nationally accepted source for definitions and codes for choosing and reporting visits and procedures
! International Classification of Diseases, 9th Edition
! Only nationally accepted source for diagnosis codes
! Healthcare Common Procedure Coding System (HCPCS)
! Level I = CPT codes
! Level II = products, supplies, services not in CPT


! Beginning – Case History
! Middle – Examination
! End – Assessment / Plan
Tell the Story / Document It!

The ‘Logic’ of Documentation
! Every record must include
! The site of service
! The medical necessity of services provided
! Accurate, thorough, legible record of all that happened during the encounter
! Case History
! Physical Examination
! Medical Decision Making
! Subjective/Objective/Assessment & Plan (SOAP)
! Date and legible identity of the observer

! Reason for visit (eg chief complaint) must be clearly stated on the record, and
! All care provided and all contents of the record must be driven by the reason for visit, not by wishes for higher income (or by the ease of recording in EHR)
Basics for Providing Care Form Basics for Medical
Records

! Keys to a ‘No Worries’ audit
! Do what the patient needs, no more, no less,
! Keep good records,
! Choose codes based on the content of each record are the
! Choose all codes based on definitions and rules in
! Current Procedural Technology (© American Medical Association),
! ICD-9, and
! The Documentation Guidelines for the Evaluation and Management Services (99000)
Best Antidote for the “Rash” of Audits?

Poll Everywhere:

Reason for the Visit!
! Reason for Visit—No grade, but no record is complete without a reason!
! Drives the Bus!
! Additionally, Does the RFV support the extent of the history / examination performed?

! “It should detail the primary reason(s) the patient scheduled the examination. Ideally, it should be recorded in the patient’s own words. The chief complaint also suggests what tests you’ll need to perform and the possible CPT codes to use for the encounter.”
! Note: this could also be “Doctor driven” – tests ordered at completion of last visit.
Woodworth, Kenneth E. Jr. www.revophth.com
The RFV / Chief Complaint

! Be an Investigator…
! What is the best way to treat this condition?
! i.e. RFV or Chief Complaint (cc:):
! If Refractive – generally refractive carrier is responsible (VSP, Vision Plus, etc.)
! If Medical – generally medical carrier is responsible (UHC, Medical Mutual, etc.)
Evidence Based Medicine

! However:
! “When a beneficiary goes to his/her physician for an eye examination with no specific complaint, the expenses for the examination are Not covered even though as a result of such examination the doctor discovered a pathologic condition.”
! “…my wife sent me in” or CEE, no probs. Centers for Medicare and Medicaid Services
The Chief Complaint

Throw out Old RFV Habits…
! Pt. here for comp. exam
! CEENP or CEEEP
! Eye health check
! Annual Exam
! Etc.
! Sometimes, even filled out before they come in!

Reason for the Visit: ! May be an Order from their LEE:
! RTC in 3 months to evaluate ocular surface
! Determine if OTC medications have improved OSD. Consider Rx products or punctal plugs if condition worsens or no improvement
! Order: Dry Eye Evaluation and Anterior Segment photos at that visit to monitor condition.

Poll Everywhere:

Key Reminders… ! Auditors may reject a claim if they feel the reason for visit
does not support the level of code chosen, even if all the components of the record support the choice.
! Doctors must follow the rules and be ready to defend
! Their decisions relative to the case history and physical examination
! The diagnoses and management options
! The content of their medical record and
! Their choice of CPT and ICD codes

Key Reminders… ! Medicare does not intend to pay for:
1. Routine Services
2. Screenings for Medical Conditions

! Jim, 47yo NP
IDDM – VSP, UHC
! Poor control
! BS > 200
! Does not check
! Wants new glasses
! (+) Diabetic Ret
! IOP’s 23mmHg OU
Physician-Patient Encounter

Poll Everywhere:

! Jim, 47yo NP
IDDM
Is there a Right
or Wrong??
Physician-Patient Encounter

! Auditors will have limited knowledge and will focus on what they expect to find, e.g.
! Does the reason for visit support coverage?
! Medical reason = medical insurance
! Vision/non medical reason = vision plan/patient pay
! Does the reason for visit support the extent of the history/examination provided?
Audit Realities – Reminder…

" Billed Vision for Exam
" Ordered testing for Diabetic Retinopathy and POAG Suspect
" Maybe Fundus Photos to Medical on same day
" Returned 4 wks later for:
" Office visit / DFE (99---)
" 24-2 Threshold VF (92083)
" GDx / OCT (92133)
" Ordered close monitoring – RTC in 6 months for Office visit / DFE, Retinal Photos and Repeat TVF’s
Billing Vision / RTC for Medical

" When back for next full exam 1 year later – was ordered previously, bill medical 1st:
" Paid:
" $xx.xx from UHC for exam, balance billed to Vision as Secondary coverage
" $xx.xx from Vision
" Ordered Medical Testing:
" 24-2 Threshold VF
" GDx / OCT
Billing Medical / Vision Next Visit

• Don’t do Medical Testing at Vision Exam
• Follow-Up for Medical Pearls
• Exponential Growth • Paid for Intellect Business
Impact
Take Home

! What do you do when a patient complains?
! What about if they have a high deductible?
! What if their wife has the HSA card?
Easier said than done sometimes…

Coordination of Benefits – Why Make the Effort?
! Are you confused about how to bill your Diabetic
patients? Especially your Diabetic patients who also have VSP?
! Many health care payers have sent notices to many eye care providers asking for the claim when their member is Diabetic.
! Kind of a blessing and curse when 2 different carriers are asking for the claim with these specific patients


Coordination with VSP 1. In order to coordinate this claim to VSP, there must be a
refraction done on the same date as well.
2. The exam can be either a 99xxx or 92xxx CPT, whichever you deem appropriate. The medical exam needs to be pointed to the medical diagnosis (choose a Diabetic code in this scenario – 250.xx) listed in position 1 on the HCFA form.
3. The refraction (92015) must be pointed towards a refractive diagnosis.
4. The claim, in its entirety, with the exam, refraction and any special testing if applicable (92250 Fundus photos if medically necessary), will be filed to the health insurance carrier for consideration.

Coordination with VSP ! The health insurance is going to process the claim as
primary and they are going to pay based on the patient’s coverage for that service.
! Once the health insurance processes the claim, you will receive the explanation of payment (EOP).
! After the health insurance company processes the claim as primary, the claim can then be filed to VSP under their coordination policy.
**This secondary claim to VSP, must mirror the primary claim exactly. This is not just sending the refraction code to VSP. CPT codes and diagnosis order cannot be altered.

Discuss Vision vs. Medical with your Patients (Dr. Gailmard tip 12/5/12)
! Explaining this to the patient can also be a challenging situation, but Dr. Neil Gailmard had a very practice management explanation of this situation along with a handout to use with patients:
! http://www.optometricmanagement.com/om_mtotw.aspx

! Insurers, including Medicare, will see increased payouts due to higher coding
! Insurers will audit more to try to control those increases
Audit Concerns with EHR:

EHR Coding: ! Great tools, meant to be impartial choice of
code based on what is in medical record
! Confirm your software is coding accurately – Audit yourself.
! “Friendly Audits” or “Self Audits” will shed some light on how confident you are in the coding features

Ask the coding email: ! My question is that I heard we should never code a level 5
as it is an immediate red flag for Medicare.
! Is that true? If my system ever does that I immediately put it down to a level 4. Should I not be doing that?
! Ans: Codes are chosen by comparing the content of the medical record to the CPT definitions for the codes. Eye doctors do visits that qualify as 99214, 99215, 99204 and even 99205. 99205 is rare in eye care, but if the content of the record matches the definition, 92005 is the code that should be reported.

EHR ‘Guided’ Coding Can Be Problematic
This encounter is one Exam Element short of a 99214
We do tests because the doctor and patients need them, not in order to
code higher!

EHR Code Triggers… ! Be Careful with this! Remember:
“Auditors may reject a claim if they feel the Reason for Visit does not support the level of code chosen, even if all the components of the record support the choice.”
! Can be useful to double check you have recorded all your information in the EHR

! Keep really good records purely because the information will…
! Assist you in arriving at diagnoses related to the visit
! Assist you in communicating with patient and staff
! Assist you in remembering what you did (and why) when the patient returns
A ‘Fresh Look’ at Patient Care:

Which Code to Use…

! Best defense is: ! Knowledge of payers’ requirements regarding patient
care and medical record keeping
! Knowledge of national rules for medical records]
! Current Procedural Terminology
! International Classification of Diseases
! Documentation Guidelines for the Evaluation and Management Services (99000 series office visit codes)
! Excellent patient records, including all information that is germane to the needs of the patient
! Accurate choices of codes, based upon contract requirements and the national rules
Best Defense = Good Offense

! Being reimbursed for a submitted claim means I filed the claim correctly…
True or False?

Auditors are ‘Focused’ on the 92000 Codes??
! Many ODs and OMDs use them almost exclusively
! 15-20% of the charts we review are missing at least one required element of the 92000 codes
! Most ODs and OMDS have never read the CPT definitions for the codes
! Auditors love to challenge doctor’s ‘initiation of diagnostic and treatment program’

Current Challenges

http://www.washingtonpost.com/blogs/ezra-klein/post/our-skyrocketing-health-care-costs-in-one-chart/2011/11/09/gIQANUPJ6M_blog.html

! Access to patients
! Increasing overhead costs and decreased reimbursement rates
! Third party denials
! Importance of correct coding
! Changing third party environment (HSA’s vs. HMO vs. PPO)
! Working harder for less
Current Challenges

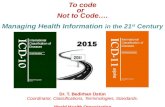
44%
21%
17%
16%
2%
Percentage
Prescription Eyewear Eye Exams Medical Eye Care
Contact Lenses Other
Optometric Practices Sources of Revenue
Source: MBA Practice Profile

! Efficient
! Delegate effectively
! Service centric
! Patient centric
! Medical necessity
! Highly modernized & automated
! Electronic Medical Records (EMR) and Practice Management Systems (PMS)
The Office of the Future

Improving the Bottom Line

Challenges Relative To Fees
! Federal Law Prohibits Talking About Fees
! Third Parties Won’t Divulge Their Methods For Determining Fees
! Fee Data (Surveys, etc.) Tightly Controlled
! Unfortunately, Doctors Base Fees On Payers’ Schedules

! Q: How much of a discount can I give to my private pay patients?
! A: Prompt pay discounts are legal and must be given in exchange for payment on the same day of service (not just for patients without insurance or for patients that you are afraid to tell what you would like to charge).
! The discount should not be more than 20% of the usual fee. No clear rules exist for this, but it believed that discounts up to 20% are all right and discounts greater than 20% should be avoided.
! The discount may be just for services or just for materials or for both.
! The discount is available to all patients, even if they have insurance.
Ask the Coding Email:

! Verify both vision and medical prior to visit
! Inform patient about
! Eligibility
! Deductibles
! Co-payments
! Collect patient balance after each visit
Best Practices

! Limit the number of insurance/3rd party plans on which you take assignment (review chair cost, lowest reimbursements)
! Integrated Electronic Medical Records with electronic claims filing
! Outsource?
Reducing Processing Costs

Poll Everywhere:

! What will they do and is it cost effective?
! Filing claims is the easy part…
! Follow-up is crucial and most time consuming
! Seek a full service provider that is paid on what is collected (5-8% usually), NOT per claim filed, etc.
Outsourcing

! Ocular surface disease
! Cataract comanagement
! LASIK comanagement
! Glaucoma
! Retina
! Red eyes
! Urgent / Emergency eye care
! On-call services
Implement the Medical Model

! Look at your “Business Model”
! Vision Care vs. Medical Care
! Efficiency will be key:
! Multiple Exam Lanes
! Instrumentation / Diagnostic equipment
! Staffing / Scribe
! Revamp Record Keeping and Billing Systems (e-Rx)
! Disease Protocols
! Full-scope Optometry
The Medical Model

What you told me…
The tests revealed…
I recommend…
Patient Education

Take the time… ! There are lots of things to learn with respect to medical
record keeping, coding, claims submission, Medicare and other payer rules.
! There is no alternative to learning, carefully doing, and properly reporting
! It takes effort, but it’s not that tough and it is well worth the effort, both in enhanced revenues for the practice, in better relationships with the payers, and in improved peace of mind.

Where to start? -ICD-10-

Poll Everywhere…

ICD-10 ! International Classification of Disease (ICD) codes
are used in virtually every healthcare setting, including inpatient and outpatient hospital settings and physician offices as well as in professional, medical services
" The 10th edition, ICD-10, will replace the current ICD-9 code set

Change… ! ICD-10 is the biggest change in the healthcare industry
in close to three decades!
! Due to the expanded ICD-10 code set, physicians will be responsible for providing greater specificity in their clinical documentation.
! There may be a 20% increase in the time required for physician documentation to produce the specificity required in ICD-10

Starts with the Why? ! 1. Why the transition from ICD-9 to ICD-10?
! The transition to ICD-10 is occurring because ICD-9 codes have limited data about patients' medical conditions. ICD-9 codes are 30 years old, many of the codes are obsolete and have outdated terms.
! In addition, because of the structure of ICD-9 codes, they are limiting in nature. In effect, conversion to ICD-10 codes is critical to transforming our nation's health care system.

! The transition to ICD-10 is occurring because ICD-9 codes have limited data about patients' medical conditions and severity of disease
! In effect, conversion to ICD-10 codes is critical to transforming our nation's health care system.
ICD-10

Start with Good Medical Records

Evaluate Your Current Documentation
! Take a look at your current records to see how your clinical documentation would be graded in ICD-10
! Is your history comprehensive enough to fully describe the encounter which will go along with your findings?
! Practice and improve on your everyday documentation which is driven by each clinical condition.
(Online Demo)

For Example ! You may have just referred to someone as a POAG
suspect, but that is not specific enough when it comes to coding.

Practice Coding ! Improve documentation skills.
! Take a number of charts by provider to review the documentation to see if it codes to ICD-10.
! The increased specificity of the codes require greater detail in the documentation.
! Provider will be given feedback about the documentation. This will allow us to see if training is needed in this area.

More Practice ! The next training recommendation is for the providers
to code a half day of charts using ICD -10 codes.
! The Billing Department will chart audit the codes & give feedback to the providers.
! This process should continue on a schedule until the deadline date of 10/1/2014. This will allow plenty of “practice” for both providers, techs & billing to learn the ICD-10 codes.

Documentation!! ! If you think ICD-10 is all about new codes, you are dead
wrong. ICD-10 is really about “documentation” � we clinicians have learned from day one that, “If it’s not documented, it wasn’t done.” This situation is even truer in the ICD-10 world, where the coder must build the ICD-10 code based on the presenting story of that patient’s visit from admissions to discharge. With all the new code options, you never know what code will be built.
! Resource: Why ICD-10 is not just a coding project (EHR Intelligence) - http://ehrintelligence.com/2014/01/27/why-icd-10-is-not-just-a-coding-project/

Be Specific ! Site of condition
! Laterality
! Location
! External Cause (injury?)
! Place of Occurrence
! Activity Code (sport?)

Coding Question:

Properly Demonstrate Medical Necessity
1. List the 1st Diagnosis, condition or problem as the reason for the medical service or procedure
2. Assign the code with the highest level of specificity
3. Never code a “rule-out”, “probable”, or “possible” statement (this could label a patient with a problem they really don’t have)
4. Be specific in describing the patient’s condition, illness or disease
5. Distinguish b/w acute and chronic when possible
6. Identify chronic complaints or secondary diagnoses only when treatment is provided for them or if they impact the overall management of the patient’s care.

Building Block of Health Information
! ICD-10, Data, and Patient Care
! Improved diagnosis of chronic illness and identifies
! Underlying causes
! Complications of disease
! Identifies:
! Conditions that contribute to the complexity of a disease
! Current stage of a disease (chronic kidney disease, dementia, asthma)
! Expands – types of diabetes and its severity

ICD-10 Supports ! Advances in Health Care
! Captures innovations in Medicine
! Administrative Transactions for Claims Processing
! Claims processing for provider services
! Improved Data for Quality
! Enhanced patient data
! Improved public health research, reporting and surveillance

Increasing Demand for High-Quality Documentation
! Better clinical documentation promotes better patient care and more accurate capture of acuity and severity
! Quality measures
! Reimbursement
! Severity-level profiles
! Risk adjustment profiles
! Present on admission reporting
! Hospital-acquired conditions
! High-quality documentation can help to:
! Avoid misinterpretation by third parties (auditors, payers, attorneys, etc.)
! Justify medical necessity

Then the What! ! 2. What should providers be doing to prepare for
ICD-10 conversion?
! Providers should plan to test their ICD-10 system early in order to ensure compliance. This will be internal and coordinated with payers, software vendors, clearinghouses and third-party billing services.
! http://cms.gov/Medicare/Coding/ICD10/Downloads/ICD10FAQs.pdf

ICD-10 Implementation

ICD-10 Implementation ! Compliance date is October 1, 2014
! ODs continue to use: ! Current Procedural Terminology from the American
Medical Association
! Healthcare Common Procedural Coding System (HCPCS II)
! ICD-10-CM (diagnoses) will be used by all providers in every health care setting
! ICD-10-PCS (procedures) will be used only for hospital claims for inpatient hospital procedures

ICD-10 Implementation ! CMS has stated the date will not be extended.
! The compliance date is based on Date of Service for Outpatient/Professional services and Date of Discharge for Inpatient services.
! **But, there is a slim chance for delay through Congress:http://m.govhealthit.com/news/congress-vote-icd-10-delay-Thursday

ICD-10 Implementation ! There is no transition period – 10/1/14 is a hard date
for compliance. However, because of timely filing rules ICD-9 codes will continue to be accepted after go-live but ONLY for claims with Dates of Service/Dates of Discharge prior to 10/1/14.
! Resubmitted claims will follow the Date of Service/Date of Discharge. If the claim was originally filed with ICD-9 codes and the Date of Service/Date of Discharge was prior to 10/1/14 we will continue to accept that claim through the appeal process with ICD-9 coding.

ICD-10 Implementation ! ICD-10 Diagnosis codes must be used for all health
care services providers in the U.S.
! ICD-10 Procedure codes must be used for all hospital inpatient procedures.
! Claims with ICD-9 codes for services provided on or after the compliance deadline cannot be paid!
! Note: For other Managed Care Plans, contact the specific plan for their ICD 10 implementation plans.

ICD-10 Implementation ! Testing is underway now
! End-to-End testing is necessary and critical to avoid any issues and fix any problems
! Will begin with a small sample group of cross-sectional providers in Summer 2014
! http://cms.gov/Outreach-and-Education/Medicare-Learning -Network-MLN/MLNMattersArticles/Downloads/SE1409.pdf

End-to-End Testing ! In late July 2014, CMS will offer end-to-end testing to
a small group of providers
! It will include the submission of test claims to CMS with ICD-10 codes and the provider’s receipt of a Remittance Advice (RA).
! Providers, suppliers and other submitters able to participate
! Volunteer Registration

FAQ’s ! During the transition period, can both codes appear on
the same claim?
! CMS has stated that there cannot be both ICD-9 and ICD-10 codes on the same claim
! Deciding which code set to use is driven by the date of service/date of discharge
! If the incorrect code set is reported on a claim, the claim will be denied

Challenges? ! Clinical
! Common language across specialties
! Operational
! Impact on practice productivity
! Financial
! Implementation issues
! Perception of cash flow / financial impacts of ICD-10 implementation

! Review changes in clinical documentation requirements and educate staff by using Internet-based programs for converting commonly used ICD-9 codes to ICD-10
! Each health care practice is unique, so your ICD-10 implementation plan will be unique, too.
! Begin using staff meetings to gradually raise awareness of the required changes in diagnosis coding.
! Watch AOA NEWS and other AOA and AOAExcel communications for more on this very important subject.

Preparation: ! To help you prepare for the transition from ICD-9 to
ICD-10, CMS has developed several implementation handbooks, with each guide providing detailed information for planning and executing the transition
! To view the guides, please visit: cms.gov/Medicare/Coding/ICD10/ProviderResources.html

Preparation: Poten&al)resources)to)assist)you)" WEDI)(Workgroup)for)Electronic)Data)Interchange))advises)
the)U.S.)Department)of)Health)and)Human)Services)on)all)things)health)IT)related)and)has)taken)a)lead)in)assis&ng)in)ICDD10)implementa&on.))Their)ICDD10)Roadmap)Tool)Kit)is)here:)wedi.org/knowledgeDcenter/resourceDview/resources/2013/07/02/icdD10DroadmapDtoolDkit))
" CMS)has)developed)Transi&on)Checklists)and)Implementa&on)Guides)specific)to)small)prac&ces,)large)prac&ces,)small)hospitals,)and)payers:)cms.gov/Medicare/Coding/ICD10/ProviderResources.html))

Go to the Centers of Medicare and Medicaid Services website ! Up-to-date information on ICD-10
! E-mail updates
! Webinars
! Links for specific provider information
! Timelines for implementation.
! http://cms.gov/Medicare/Coding/ICD10/index.html

Create a Team

Determine Who Will be Affected
! Evaluate all aspects of your practice where ICD-9 is currently used
! Authorizations
! Pre-certifications
! Physician orders
! Medical records
! Superbills
! EHR systems
! Coding manuals
! Public health reports.
! Establish a training timeline.

Create a Team / Ask Questions ! Create an ICD-10 project management team for your
practice, including doctors and staff ! Begin to discuss how ICD-10 will affect your practice ! Start working on an ICD-10 project plan for your
organization, including scheduling staff training for choosing ICD-10 codes for diagnosis codes common to your practice
! Ask your payers and vendor (software/systems, clearinghouses, billing services) about ICD-10 readiness; review contracts/proposals ! Ask about systems changes, a timeline, costs, and
testing plans ! Ask when they will start testing, how long they will
need, and what they suggest your office should be doing to smooth the transition to ICD-10

What Providers Need to Do… 1. Stay Updated on ICD-10 Information – lots of
resources
2. Train your Staff
3. Ensure your Vendors are compliant and up-to-date
4. Update your Claim forms - Claim Documentation - HCFA 1500 form will have space for (12) ICD-10 codes compared to prior form that allowed space for (4) ICD-9 codes
5. Practice Coding Cases with ICD-10 - Providers who have done this indicate that coding staff discovered that practitioners need to include more detailed information in the medical record in order for the coder to properly code the claim.
# Be cautious regarding where you receive your ICD-10 information!

How Can Providers Prepare for ICD-10?
! Understand)which)processes)use)ICDD9)codes)today)that)will)need)updated?)! Billing)soVware/)trading)partners)! Management)soVware)(electronic)health)record)system))
! Reports

Know your top codes ! There are several programs, websites and services
available to help navigate the new ICD-10 codes and allowing a comparison to ICD-9.
! Take a look at your current top 25 ICD-9 codes for your practice to see examples of what the ICD-10 codes will be. These same programs will also allow you to compares ICD-10 codes to their previous classification.
! Document these codes as a guide to improve accuracy when ICD-10 comes around.

General Equivalence Mapping (GEM)
! The purpose of the GEMs is to create a useful, practical, code to code translation reference dictionary for both code sets, and to offer acceptable translation alternatives wherever possible.
! The target codes included for a given source code are selected, to the greatest extent possible, according to the same principle as that articulated by the National Library of Medicine (NLM)
**Note: Mappings from specific concepts to more general concepts are possible; however, it is not possible to use mappings to add specificity when the original information is general.

Useful Aids ! There are good websites by AAPC and ICD10data.
! The GEMS file and other CMS information is available on their site at wwww.cms.gov/ICD10/
! www.icd10data.com
! There is a great quick way to search for codes
! It will also have a link to see tabular break down of codes within that class
! http://myicd10.advancedmd.com/post/code-search-icd-9-to-icd-10-mapping-tool
! Green button leads you to an online tool that uses GEM from ICD-9 to ICD-10 as CMS has mapped them.



ICD-10 Coding Lessons

General Equivalence Mapping (GEM’s)
! Crosswalk between ICD-9, ICD-10 and SNOMED
! Over time, ICD-9 will be shelved and GEM will need to identify ICD-10 for historical ICD-9 diagnoses
! No Match: 3%
! 1-1 match: 24%
! 1-1 approximate match with 1 choice: 49%
! 1-1 approximate match with multiple choices: 19%
! 1 to many match with 1 or many scenarios: 5%

103

ICD$9) ICD$10)
3D5)characters)in)length) 3D7)characters)in)length)
Approx.)14,000)codes) Approx.)79,000)available)codes)
First)digit)may)be)alpha)(E)or)V))or)numeric;))Digits)2D5)are)numeric)
Digit)1)is)alpha;))Digits)2D7)are)alpha)or)numeric)
Limited)space)for)adding)new)codes) Flexible)for)adding)new)codes)
Lacks)detail) Very)specific)
Lacks)laterality) Has)laterality))
NonDspecific)codes) Specificity)improves)coding)accuracy)
Difficult)to)analyze)data)due)to)nonDspecific)codes)
Specificity)improves)coding)accuracy)and)depth)of)data)analysis)
Codes)are)nonDspecific)and)do)not)adequately)define)diagnosis)for)medical)research)
Detail)improves)the)accuracy)of)data)used)in)medical)research)

OD not as bad as OB/GYN Gesta&onal)week)diagnosis)codes)will)be)required)on)every)claim)a)delivery)procedure)code)is)billed)
105
ICD-10 Diagnosis Codes(Z3A.00 not specified Z3A.
16)16 weeks gestation of pregnancy)
Z3A.26
26 Weeks gestation of pregnancy
Z3A.36
36 Weeks gestation of pregnancy
Z3A.01 Less than 8 weeks gestation of pregnancy
Z3A.17)
17 weeks gestation of pregnancy)
Z3A.27
27 Weeks gestation of pregnancy
Z3A.37
37 Weeks gestation of pregnancy
Z3A.08 8 weeks gestation of pregnancy
Z3A.18)
18 weeks gestation of pregnancy)
Z3A.28
28 Weeks gestation of pregnancy
Z3A.38
38 Weeks gestation of pregnancy
Z3A.09) 9 weeks gestation of pregnancy)
Z3A.19)
19 weeks gestation of pregnancy)
Z3A.29
29 Weeks gestation of pregnancy
Z3A.39
39 Weeks gestation of pregnancy
Z3A.10) 10 weeks gestation of pregnancy)
Z3A.20)
20 weeks gestation of pregnancy)
Z3A.30
30 Weeks gestation of pregnancy
Z3A.40
40 Weeks gestation of pregnancy
Z3A.11) 11 weeks gestation of pregnancy)
Z3A.21)
21 weeks gestation of pregnancy)
Z3A.31
31 Weeks gestation of pregnancy
Z3A.41
41 Weeks gestation of pregnancy
Z3A.12) 12 weeks gestation of pregnancy)
Z3A.22
22 Weeks gestation of pregnancy
Z3A.32
32 Weeks gestation of pregnancy
Z3A.42
42 Weeks gestation of pregnancy
Z3A.13) 13 weeks gestation of pregnancy)
Z3A.23
23 Weeks gestation of pregnancy
Z3A.33
33 Weeks gestation of pregnancy
Z3A.49
Greater than 42 weeks gestation of pregnancy
Z3A.14) 14 weeks gestation of pregnancy)
Z3A.24
24 Weeks gestation of pregnancy
Z3A.34
34 Weeks gestation of pregnancy
) )
Z3A.15) 15 weeks gestation of pregnancy)
Z3A.25
25 Weeks gestation of pregnancy
Z3A.35
35 Weeks gestation of pregnancy
) )

SNOMED ! The core terminology of EHR’s
! Over 300,000 concepts
! Multinational and multilingual
! All numeric coding
! Maintained and distributed by ISTSDO, an international non-profit standards developed by an organization in Denmark

Not too far down the line… ! ICD-11
! World Health Organization (WHO) developing a plan to endorse by 2015
! Will align with SNOMED terminology
! Expanded multilinguality
! Enhanced Content Model will guide the users:
! Each disease will have definitions that give key descriptions and guidance on the meaning of the code in human readable terms

FYI – SNOMED Implementation
! 2014 Certified EHR’s will include SNOMED
! Standards require documentation of a wide variety of data through SNOMED
! SNOMED is an option for Diagnosis listing and for documentation of treatment plans, but will not be accepted for claim payment

! Your EHR will need to have a plan and align with the new ICD-10 code sets
! ICD-10 is critical to get paid
! SNOMED is critical in provider’s ability to properly document and share data

ICD-10 ! Sense organs (eye and ear) separated from Nervous
System chapter
! Laterality has been added to relevant codes
! Certain conditions and associated manifestations in combo codes:
! E11.311 = Type2 DM with unspecified diabetic retinopathy with macular edema
! 7th character in some conditions (musculoskeletal, obstetrics, injuries, external causes)

ICD-10 ! A dummy placeholder “x” is used in cases where
future code expansion may be necessary.
! Excludes 1 note indicates a code used when 2 conditions cannot occur together
! Excludes 2 note identifies codes that may be reported together if the patient has both conditions

ICD-10 ! Example of laterality expressed in ICD-10: H01.111
Allergic dermatitis, right upper eyelid

! Billy, 15 year old, NP:
! Presents with complaints of “burning, itching and redness”; going on for the past 4 weeks, on/off, has not used any eye drops
! Wears glasses full-time, thinks vision has progressively worsened, is considering contact lenses this time.
! Has seasonal ocular allergies – taking Zyrtec
! Online Demo
ICD-10 Case Example

Ask your EHR? ! Their implementation plan
! Mapping between ICD-9 to ICD-10 and SNOMED
! How are they addressing ICD-10
! Will there be a “crosswalk” for today’s diagnoses and what about the Master List of Diagnoses



Code Examples ! Myopia
! ICD-9: Myopia = 367.1
! ICD-10: Myopia Bilateral = H52.13
! SNOMED:
! 57190000 – Myopia
! 232133000 – Simple Myopia
! 408757002 – Axial Myopia

Dry Eyes ! ICD-9: 375.15 = tear film insufficiency
! ICD-10: H04.123 = Dry Eye syndrome of both lacrimal glands
! SNOMED:
! 1249004 – Dry Eyes
! 24689001 – lack of tear production

Nuclear Sclerotic Cataract
! ICD-9: 366.16 = cataract, senile nuclear sclerosis
! ICD-10: H25.13 = age-related nuclear cataract, bilateral
! SNOMED:
! 53889007 – nuclear cataract
! 193589009 – nuclear senile cataract

Age-related Macular Degeneration
! ICD-9: 362.51 = non-exudative senile macular degeneration
! ICD-10: H35.31 = non-exudative AMD
! SNOMED:
! 267718000 – AMD
! 414875008 – non-exudative AMD
! 264633009 – drusen stage AMD

Glaucoma ! ICD-9: 365.11 – primary open angle glaucoma
! 365.71 – mild stage glaucoma
! ICD-10: H40.11X1 – primary open angle glaucoma, mild stage
! SNOMED:
! 77075001 – primary open angle glaucoma

Type 2 DM with Mild NPDR
! ICD-9: 250.52 = Type2 DM with ophthalmic manifestations
! 362.04 = Mild Non-proliferative DR
! ICD-10 = E11.329 = Type2 DM with Mild NPDR and No DME

! Susan, 44 year old (IT Manager) PP;
! Pt here c/o some dryness at the end of the day and occasional tearing OU.
! Myopic OU and would like to update SCL Rx
! Ocular / Medical history is negative.
! (+) Family history of glaucoma.
ICD-10 Case Example

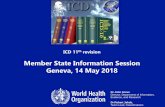
Crosswalk from ICD-9 to ICD-10 ICD-9 ICD-10
Acute conjunctivitis, unspecified
372.00 Unspecified Acute Conjunctivitis
H10.33
Nuclear sclerosis 366.16 Age-related nuclear cataract
H25.10
Diabetic Retinopathy, Proliferative
362.02 Type 2 diabetes mellitus with proliferative
diabetic retinopathy
without macular edema
E11.359
Glaucoma, Primary open-angle
365.11 Primary open-angle glaucoma,
severe stage
H4Ø.11X3
X is a placeholder which allows for future expansion

Road to ICD-10 October 1, 2014

Develop and Work the Plan!
! It starts with education!
! Visit the site: http://cms.gov/Medicare/Coding/ICD10/index.html for a variety of important documents.
! Create a communication and awareness plan. This is where each office opens the lines of communication about ICD-10. Assess training needs and develop a training plan. Meet with the staff and discuss the effects of ICD-10, why the conversion is important and assign responsibilities.


Provider Preparation 1. Plan the Journey
2. Train your Team
3. Update your Processes
4. Engage your Vendors & Payers
5. Test your Systems and Processes


Plan the Journey ! Understand where your are currently with ICD-10
compliance
! Develop the Action Plan
! Pinpoint common Diagnosis Codes
! Identify a transition team
! Prepare a budget
! Arrange for training

Front Desk ! We’ll need to educate the Front Desk staff to the new
routine & medical codes so that they can collect the correct copays for visits.
! The ICD-10 codes will also be listed on all of the referral slips.

Billing ! This transition will require a new chart audit protocol for reviewing
all ICD – 10 on claims. This will increase staff time spent on coding leading up to & during the transition period. This will also increase posting time for claims.
! Work on a testing schedule for ICD-10 codes with our practice management system, our clearinghouse & payers.
! There will be additional staff time needed to appeal denials on the back end. Even if our coding is correct, we must expect that there will be systems issues with payers that will cause denials, delays in processing and reimbursements.
! Billing Books must be updated.
! Local Coverage Determination of codes will change – need education for billing, providers & clinical staff.
! Need to find out what our involvement will be in customizing diagnosis tables with new codes.

Route Slips ! Route Slips as we know them will no longer exist. The
full list of diagnoses codes will be impossible to list on the route slips because of the expansion of the number of codes. We’ll need to develop a new route slip system to allow proper communication of information to Front Desk, Clinical, Providers & Billing.
! Maybe include Top 25 Codes and will have to look up others if needed.

Creating your List… ! Development of a list of the most common diagnoses
codes used by our providers.
! All providers will receive a list of ICD-9 diagnosis codes & the corresponding ICD-10 codes from the new ICD-10 Ophthalmology Coding book.
! This list will be reviewed by all providers to highlight the codes which they frequently use. We’ll take the feedback to create our own master list of most frequently used codes. Again, this list will be too large to fit on route slips.

Clinical ! We’ll need to determine how the transition will impact the
clinical daily process & slow the work flow.
! Providers will require increased time to document & select ICD-10 codes leading up to & during the transition period.
! We’ll need to determine if the current level of documentation support the new detail of the ICD-10 codes-may require training for increased level of documentation.
! We must update protocols, processes, forms, paperwork that are related to any diagnosis codes.
! We need to develop a training schedule for staff.

Financial ! Every article and website states that the cash flow for
practices will be disrupted. There will be transmittal & systems problems, claim appeals & denials and slow down of payments.
! Plans should be put into place in preparation for the change in cash flow.

2. Train your Team ! Support staff is huge!!
! Meetings
! Training resources
! CMS website

Provider Implementation Touch Points
! Educate and Train Staff
! Coder Training:
1. Ensure Coder Implementation Training
2. Explore Coding Exercises and Scenarios
3. Determine use of 3rd party or Outsourced coders

3. Update your Processes ! Review current clinical documentation and identify
gaps related to ICD-10
! Update forms and templates

Provider Implementation Touch Points
! Review Internal Policies
! Internal Operations
1. Contact Clearinghouses, Trading Partners, etc.
2. Forms
3. Review Clinical Documentation Practices

4. Engage your Vendors & Payers
! Collaborate with technology vendors
! Ensure system updates
! Address any compliance risks

Payers ! Review payment policies since the transition to
ICD-10 will involve new coding rules
! Testing End-to-End

Provider Implementation Touch Points
! Systems Software & Systems
! Upgrade and remediate systems as needed (EHR, PM)
! Test internally and externally
! Identify alternative ways to submit your ICD-10 ready claims if your system isn’t ready:
1. CMS Billing software
2. CMS Claims submission portals
3. Paper Claims

Software Vendors ! Clearinghouses
! 3rd Party Billers
! EHR systems
! ALL need to work with provider to install and test ICD-10 ready products.
! http://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD10_Introduction_060413%5B1%5D.pdf

Clearinghouse ! Contact our clearinghouse to see what the timeframe
is for converting their electronic claim systems to ICD-10.
! What do we need to do from our end for the system upgrades?
! What we’ll we need to know when we can start testing claims through the new system?

EHR / PMS ! We need to convert to latest practice management software
version which incorporates ICD-10, need to find out when this version will be available.
! We need to find out the schedule for running the dual systems for ICD-9 & ICD-10.
! We’ll need to know if the EHR will completely change for ICD-10 & how our customized screens will be impacted.
! The diagnoses tables will be all new, what will be the set up & what role will we play in customized them.
! The new HCFA 1500 may have space for up to 12 diagnosis codes. How will we submit claims without the older, resolved diagnoses showing on the claims?
! Will the changes to the practice management system impact our disc space?



Test your Systems and Processes
! Testing is a critical process of the ICD-10 transition
! Internal and External testing
! Practice Coding Cases with ICD-10
! Validate clinical documentation processes


CMS Testing Tools and Information
! Available Now:
! General Equivalence Mappings are available for public use
! ICD-10 Mappings
! National Coverage Determinations
! Coming Soon:
! April, 2014 – Local Coverage Determinations will become available

Resources ! CMS Email Updates
1. Go to www.cms.gov/icd10
2. Select “CMS ICD-10 Industry Email Updates” from navigation bar
3. Click on “Sign up for update messages”




More Resources ! CMS Provider Resources http://www.cms.gov/Medicare/
Coding/ICD10/ProviderResources.html
! FAQ: ICD-10 Transition Basics
! ICD-10 Transition: An Introduction Fact Sheet
! ICD-10 Basics for Medical Practices
! ICD-10 Basics for Payers
! The ICD-10 Transition: Focus on Non-Covered Entities
! Checklists, Timelines, and Implementation
! Implementation Planning
! Communicating About ICD-10
! Medscape Education: Webinar and Articles Available
! American Association of Professional Coders - www.aapc.com
! American Health Information Management Association (AHIMA)
! www.ahima.org

Thank You!! [email protected]