Medical Error Sept 08 2.ppt
45
Managing Medical Error in the New Medical Home • A review of two residency processes aimed at reducing medical error: • A variation on the Morbidity and Mortality Conference • “Unusual Occurrence Reporting” in the Family Medicine Residency Clinic Jessica Burness MD and Elizabeth Klein MD Providence Milwaukie Family Medicine Residency Milwaukie Oregon
-
Upload
jikko-verra-garcia -
Category
Documents
-
view
76 -
download
3
description
medical
Transcript of Medical Error Sept 08 2.ppt

Managing Medical Error in the New Medical Home
• A review of two residency processes aimed at reducing medical error:
• A variation on the Morbidity and Mortality Conference
• “Unusual Occurrence Reporting” in the Family Medicine Residency Clinic Jessica Burness MD and Elizabeth Klein MD
Providence Milwaukie Family Medicine Residency Milwaukie Oregon

Introduction of Participants
• Who are you? Where are you from? What do you hope to learn?
• Destiny by William Bryan:
“Destiny is not a matter of chance, it is a matter of choice. It is not a thing to be waited for- it is a thing to be achieved.”
So it is with Managing Medical Error in 2008

Objectives for participants
• Discuss the importance of having a system to report and investigate medical error
• Understand the development and use of our medical error system
• Be able to develop you own process and form for reporting and investigating medical error
• Be able to implement physician friendly Morbidity and Mortality Rounds

Medical Mistakes Happen
• At least 44,000 and as many as 98,000 people die in hospitals each year as a result of medical errors that could have been prevented, according to estimates from two major studies.
Institute of Medicine. To Err is Human: Building a Safer Health System.” Washington, DC: National Academy Press, 1999.

Medical Mistakes Happen
• 100-200k people die each year due to medical error in the USA -2X MVA
• Errors happen 1 in 4 patient visits
• Increased medical complexity and uncertainty leads to increased errors
• Residents Errors differ from Practicing Physician Errors

Error Definition
• IOM “Failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim”
• AAFP Past President Dr Bruce Bagley “ A medical error is anything that happens in my office that shouldn’t have happened and I absolutely do not want to happen again”

Resident vs Practicing MD
• 35-50 % of Resident Errors due to misdiagnosis or delay in care
• Practicing Physician Errors are more likely related to process errors, results lost, not acted on, lost specimen, lost or incomplete records

Errors in Family Practice
• According to AAFP Policy analyst Susan Dovey, MPH- examined error in office
• 24% Communication problems
• 20% Discontinuity of care
• 19% Lab results- timing, fu
• 13% Missing values, charting errors

Errors in Family Practice cont
• 8% Clinical Mistakes (knowledge/skill)
• 8% Prescribing Errors (dosage, choice, allergy or interaction)
• 8% other
• Medical errors in family practice are a result of multiple conditions rather then just prescribing error or “bad doctors”

Truths about Medical Errors
• Errors will happen
• Since errors happen, systems must be designed to prevent and absorb them
• Errors are not the same as negligence, therefore need to look at systems not just individuals
• Must have culture of safety for error reporting

Intense feelings common when medical errors occur
• Anxiety, humiliation, fears of being sued or professionally censured
• Resident evaluation and promotion also a concern
• However, recent reports show declines in malpractice claims and costs occur when disclosure and apology are implemented.

3 Main Reasons for Lawsuits
• 1) Matter of justice and fairness
• 2) Financial compensation for harms and setbacks
• 3) Out of need for explanation, accountability and concern for care standards and needs not being met

Need Systematic Program for Medical Error Evaluation
• Medical error must be disclosed and discussed in a systematic fashion in order for effective change to occur to reduce medical error. Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press, 1999.
??? Remains- How do you implement a systematic program for error evaluation and disclosure in the family medicine office??

Future of Family Medicine
• New Medical Home is “Patient Centered with Integrated Care where Quality is measured and improved and Safety becomes systematic instead of just assumed”
• Quite a challenge…..

New model and our office
• New Model includes Goal of Systematic Safety in the new Medical Home
• I wanted to create a culture of safety in our Family Medicine Center and Residency
• I wanted to look at systems, not individuals• View adverse events as OPPORTUNITIES
to make our office safer and better for our patients and our staff

Culture of Safety
• Empower everyone to point out errors
• Look for weak links
• Look for root causes
• Review and update polices and procedures
• Avoid punishing those who commit errors, within reason

PLANNING
• Innovative Director- Dr Bill Gillanders• Our faculty are adventuresome and idealistic• Our program is young and willing to pilot
new projects- Ex EHR, Electronic Billing, Electronic Orders, Depression Screening in the waiting room etc.
• We value and ask for input from staff, residents and faculty

Unusual Occurrence ReportingPlanning for office use
• Hospital UORs have been used for years
• The hospital form needed revision to be useful in the office
• Discussions regarding who would fill them out, who would review them and who would follow through on the changes that we wanted to implement

Implementation of UOR process
• Bumpy start
• Lack of consistent follow through
• Loss of Office Manager
• Loss of UORs by Medical Director
• Revised form several times
• Culture of safety prevailed

Implementation of UOR process continued
• UORs reviewed and discussed at all provider and staff meetings- On the agenda at both meetings
• Encourage staff, residents and faculty to fill out the UOR form
• Faculty, new office manager and staff like our process

Examples of UORs
• Narcotic prescribing, lack of contracts, need for compliance by docs, especially faculty
• Visual acuity on every patient with eye complaint• Steroid injection depigmentation- Didactic and
better PARQ Form for steroid injections• Missed ischemia on EKG- New form and process
for EKG reporting and faculty sign off• IUD Perforation- Didactic on IUD PARQ and
insertion-new IUD consent form

Examples of UORs continued
• Direct hospital admission policies
• Immunization Errors
• Medication Errors
• Test Notification Errors- delay, wrong pt
• Falls- Children and adults- Fall Prevention
• TM Perforation with Ear Lavage- better training of Medical Assistants

Lessons Learned
• Innovative director and enthusiastic clinic manager really helps
• Emphasis on improving systems to protect patients and staff is important
• Promotes good role modeling by faculty
• Empowers staff because they see results
• Promotes Culture of Safety

Share your experience
• Medical Error Reporting in your clinic or residency
• Unusual Occurrence Reporting
• What were your challenges and successes?
• What were some unexpected outcomes?

Morbidity and Mortality Conference: A Revised Model
Jessica Burness MD

Outline
1. Background and Rationale
2. Core Concepts for Revised Model
3. Pilot
4. Our Experience
5. Future Directions

Background and Rationale
• Learning to appropriately and effectively address error is an important part of resident education.
• The Morbidity and Mortality conference is a tool for addressing medical error.

Background and Rationale
• The emotional consequences of committing medical errors are not slight.Douglas, S., Crook, E., Stellini, M. et al. Medical Errors and the Trainee: Ethical Concerns. American Journal of Medical Sciences. 2004; 327: 33-37.
• There is evidence that exposure of error in Morbidity and Mortality conferences can cause stress, anxiety and blaming which may lead to future non-disclosure of medical errors.Wu, A., Folkman, S., McPhee, s., et al. Do House Officers Learn from their Mistakes? JAMA. 1991: 265: 2089-2094.

Background and Rationale
• Undue stress and anxiety is not conducive to education.
• In order to address medical error and be educationally valuable, a Morbidity and Mortality conference must be structured such that it creates a supportive, safe, and non-persecutory environment.

Background and Rationale
• There is no consensus or single standard on the appropriate structure of a Morbidity and Mortality conference within a department of Family Medicine or Internal Medicine.Orlander, J., Fincke, G. Morbidity and Mortality Conference; A Survey of Academic Medicine Departments. Journal of General Internal Medicine. 2003; 18: 656-658.

Background and Rationale
• There are suggestions in the medical literature for frameworks for Morbidity and Mortality conferences that might foster a supportive, safe, and non-persecutory environment.Orlander, J., Barber, T., Fincke, G. The Morbidity and Mortality Conference: The Delicate Nature of Learning from Error. Academic Medicine. 2002; 77: 1001-1006.

Background and Rationale
• There is no literature to suggest that any Morbidity and Mortality conference format is effective at simultaneously systematically addressing medical error and being perceived as educational, supportive, safe, and non-persecutory.

Core Concepts
• All adverse patient outcomes should be identified on a continuous basis.
• Cases should be generated from the entire practice population.
• Error and adverse events should be classified and defined according to a basic taxonomy of error.
• Moderator(s) should ensure the conference environment is supportive and non-persecutory, and that it does not stray from the format.

Core Concepts
• Faculty and residents should both participate in generation of cases and discussion of cases.
• If systems problems or generic mistakes are identified, discussion should be facilitated on how to prevent future similar adverse events. An action plan should be identified and subsequent practice changes should be communicated and implemented.

Pilot Study Model
• 2 Moderators, faculty member and chief resident
• Conference begins with brief standard intro about confidentiality, universality of human error, and learning from mistakes.

Pilot Study Model
• Brief numerical review of all adverse outcomes for the month and taxonomy of error. Chief resident.
• Two to three 10 minute case presentations of adverse outcomes or near-misses with clarifying questions only.

Pilot Study Model
• Moderators lead discussion after full presentations. Discussion centers on error type, factors leading or contributing to adverse outcome, and/or barriers to good outcome. All discussions end with brainstorming and choosing action ideas to reduce similar future errors or adverse outcomes.
• Final portion of conference to review actions taken (and results?) from previous conferences.

Goals
• Can a Morbidity and Mortality conference be structured such that it simultaneously systematically evaluates medical error and is perceived by residents as being educational, supportive, safe and non-persecutory?
• Surveys before and after pilot study implementation to attempt to answer the question for this Morbidity and Mortality conference design.

Limitation
• The only computerized database currently available to cull data on adverse outcomes is the inpatient database. Ideally, we would have similar ability to access data for outpatient care.

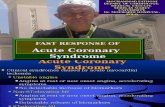
% Respondents answering STRONGLY agree
0
10
20
30
40
50
60
70
1 2 3 4 5 7
BeforeAfter

% Respondents answering STRONLY disagree
0
10
20
30
40
50
60
70
6
EastWest

Modifications for Providence Milwaukie residency
• Half-hour time slot limits us to 1 case
• Cases presented every 2 months instead of monthly
• 1 moderator
• Follow-up process “Managing Medical Error Committee” for M&M cases and UOR cases

Sample Case
• From selection, through presentation and discussion, to follow-up

Call for M and M Cases
• Cases (inpatient or outpatient, from our practice) should involve:
• 1. a poor or unintended outcome which might have been due to or worsened by error or system problems, or
• 2. “near-misses,” where there was an error or misstep in care delivery that could have led to a poor patient outcome
• The goals of the conference are • 1. to learn from each other in a supportive
environment and • 2. to improve patient care in our practice.

Future Directions
• Incorporating ideas from –• Matrix Process at Cedars Sinai• Patient Healthcare Matrix• Creation of system to query outpatient data
for markers• Greater number of cases, rely on databases,
not solely volunteers• Your ideas?????