Medical Complications of Eating Disorders Complications of Eating Disorders ... • Define anorexia...
52
Medical Complications of Eating Disorders Margherita Mascolo, MD Assistant Professor of Medicine Ui i f C l d Sh l f M di i University of Colorado School of Medicine Lead Physician, ACUTE Center for Eating Disorder at Denver Health
Transcript of Medical Complications of Eating Disorders Complications of Eating Disorders ... • Define anorexia...
Medical Complications of Eating Disorders
Margherita Mascolo, MDAssistant Professor of Medicine
U i i f C l d S h l f M di iUniversity of Colorado School of MedicineLead Physician, ACUTE Center for Eating Disorder at
Denver Health
Learning Objectives:Learning Objectives:
• Define anorexia nervosa and bulimia nervosa
• How to identify at risk patientsy p
• Appropriate work up
• When to transfer patients to a higher level of • When to transfer patients to a higher level of care
C di l li i f i• Common medical complications of anorexia nervosa and bulimia nervosa
Epidemiology of Anorexia Nervosa
• In Western industrialized countries, the prevalence is 0.3 - 4% of the female population and 0.1% of the male population
• Mortality is the highest of any psychiatric diagnosis
– 0.56% per year
12 times higher than the annual death rate for women 15 24 – 12 times higher than the annual death rate for women 15-24 years of age
– Roughly one third are due to cardiac complications; g y p ;average age of death is 34 years
– Up to 30% of affected patients do not achieve sustainable recovery

What is Anorexia Nervosa?What is Anorexia Nervosa?
• Defined by four criteria from DSM IV• Defined by four criteria from DSM-IV
– Refusal to maintain body weight at or above 85% of that expected for heightp g
– Intense fear of gaining weight or becoming fat, even though underweight
b h f b d h f– Disturbance in the perception of one’s body weight for shape
– In postmenarchal women the absence of three consecutive In postmenarchal women, the absence of three consecutive menstrual periods
– Subtypes: restrictive or binge/purge
Anorexia NervosaAnorexia Nervosa
Epidemiology of Bulimia Epidemiology of Bulimia Nervosa
• Prevalence is between 1-2% of the female population
• Lifetime prevalence for females is between 1.1 and et e p e a e ce o e a es s betwee . a d 4.2%
• Onset between 13 and 20 years of agey g
• Ten times more common in females than males
What is Bulimia Nervosa?What is Bulimia Nervosa?
• Defined by the DSM IV as:Defined by the DSM IV as:
– Recurrent episodes of binge eating
– Recurrent, inappropriate compensatory behavior to Recurrent, inappropriate compensatory behavior to prevent weight gain
– These behaviors occur an average of twice a week for gthree months
– Self evaluation is influenced by body shape and weight
– The disturbance does not only occur during periods f i of anorexia nervosa

Risk Factors for Eating Risk Factors for Eating Disorders
• Female > male (2-3:1)
• Peaks at ages 13-14 and 17-18 – By age 14, 60-70% of girls are trying to reduce y g , g y g
weight
• Highest incidence in Western societiesg– Independent of race or ethnicity
Risk Factors for Eating Risk Factors for Eating Disorders
• Personal history of DM type I, cystic fibrosis, d i i di d ADHD PTSD depression, anxiety disorder, ADHD, PTSD, and OCD
• Family history positive for: obesity, depression, anxiety, other eating disorders
• Social history: dancers, body builders, models, actors
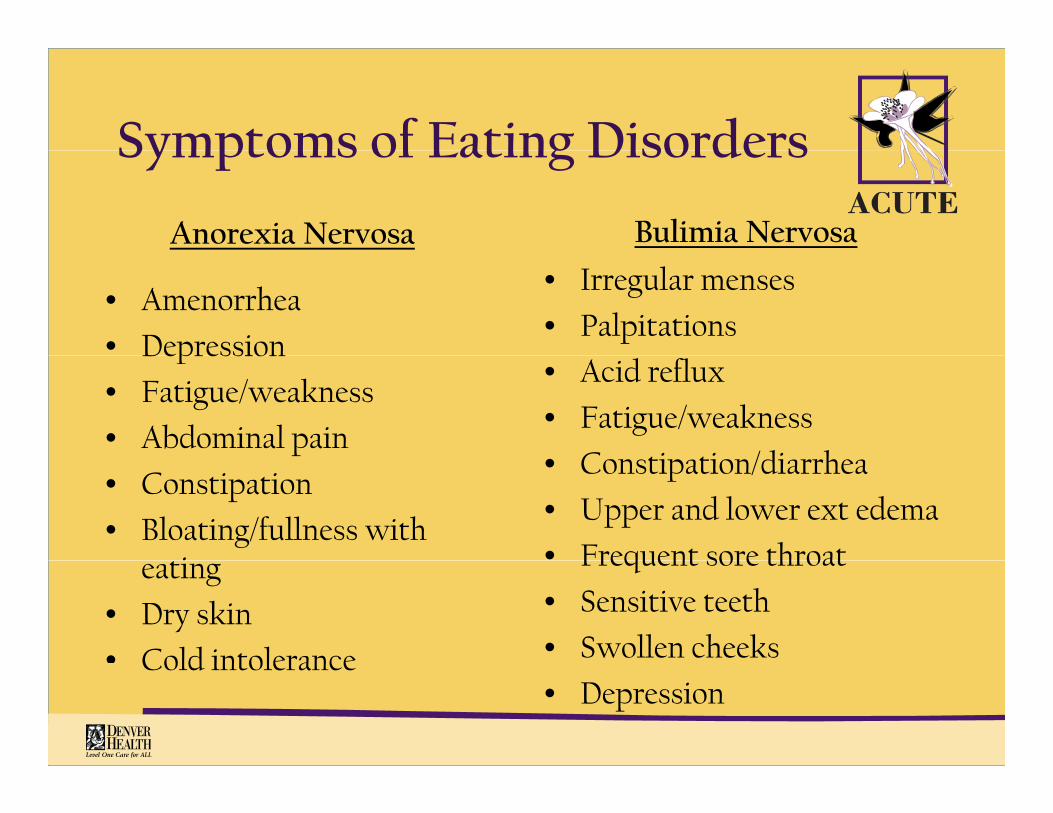
Symptoms of Eating DisordersSymptoms of Eating Disorders
Anorexia Nervosa Bulimia Nervosa
• Amenorrhea
• Depression
• Irregular menses
• PalpitationsDepression
• Fatigue/weakness
• Abdominal pain
• Acid reflux
• Fatigue/weakness
C ti ti /di h• Constipation
• Bloating/fullness with i
• Constipation/diarrhea
• Upper and lower ext edema
• Frequent sore throateating
• Dry skin
• Cold intolerance
Frequent sore throat
• Sensitive teeth
• Swollen cheeks Cold intolerance• Depression
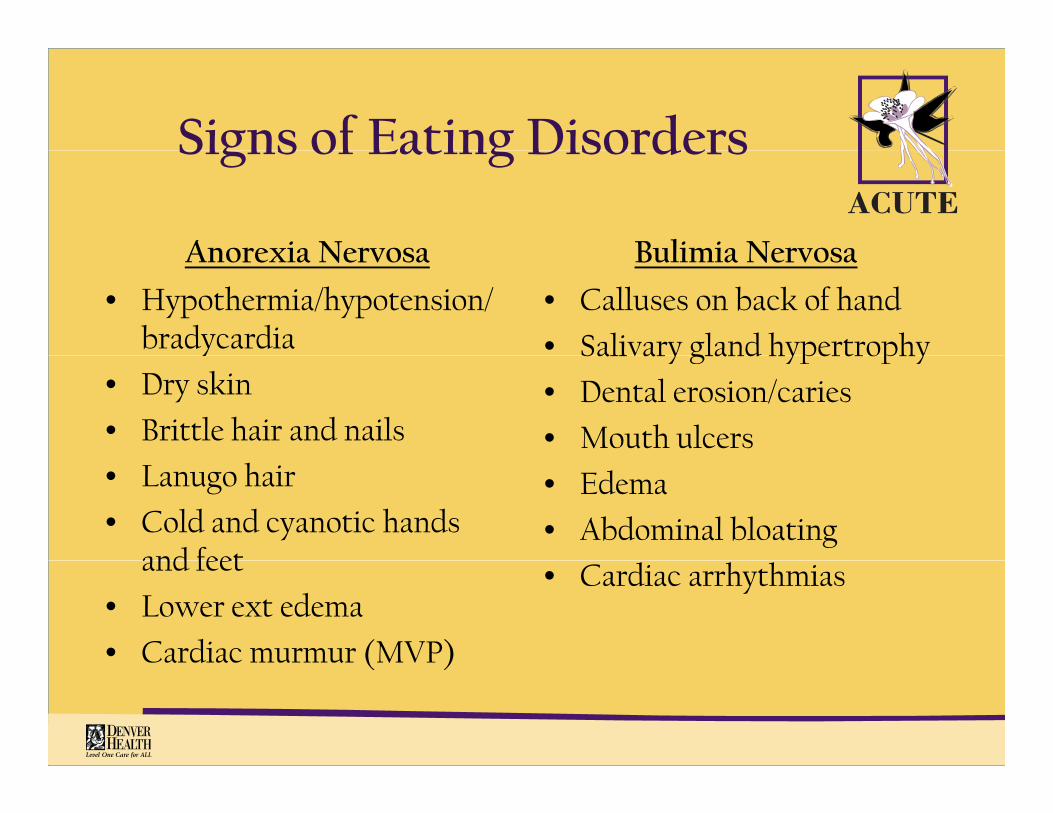
Signs of Eating DisordersSigns of Eating Disorders
Anorexia Nervosa Bulimia NervosaAnorexia Nervosa
• Hypothermia/hypotension/bradycardia
Bulimia Nervosa
• Calluses on back of hand
• Salivary gland hypertrophyy
• Dry skin
• Brittle hair and nails
Salivary gland hypertrophy
• Dental erosion/caries
• Mouth ulcers• Lanugo hair
• Cold and cyanotic hands and feet
• Edema
• Abdominal bloatingand feet
• Lower ext edema
• Cardiac murmur (MVP)
• Cardiac arrhythmias
( )
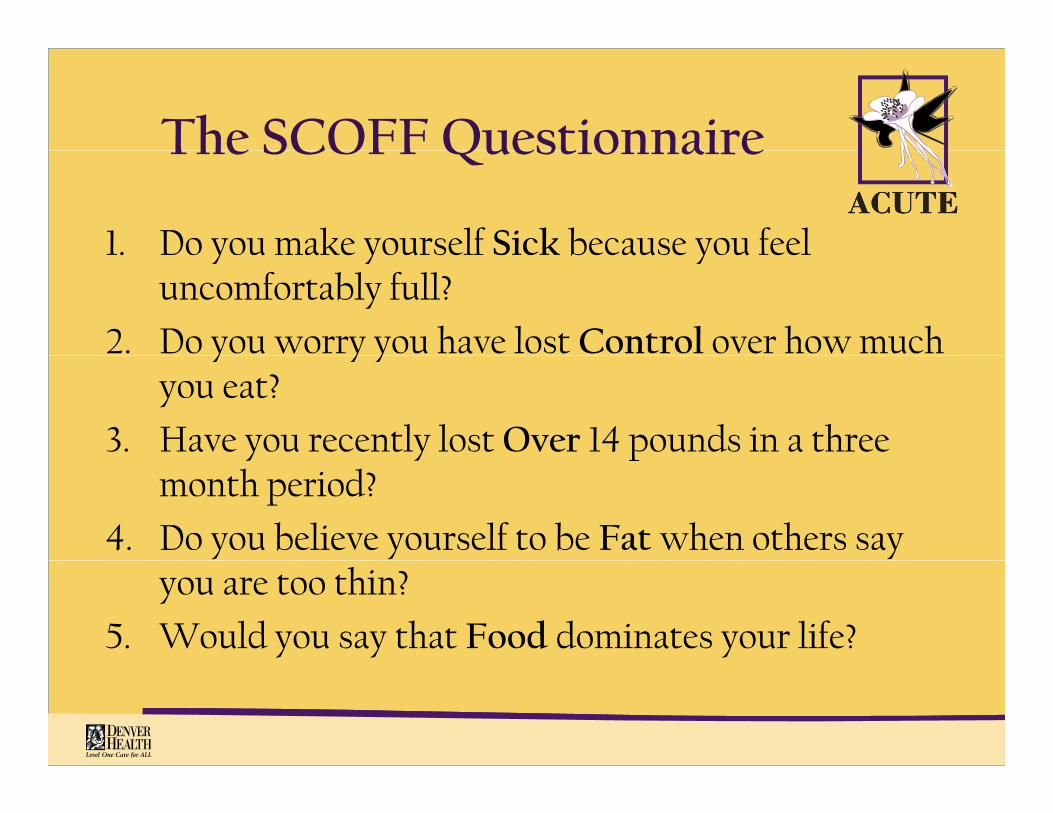
The SCOFF QuestionnaireThe SCOFF Questionnaire
1. Do you make yourself Sick because you feel 1. Do you make yourself Sick because you feel uncomfortably full?
2. Do you worry you have lost Control over how much y y yyou eat?
3. Have you recently lost Over 14 pounds in a three y y pmonth period?
4. Do you believe yourself to be Fat when others say you are too thin?
5. Would you say that Food dominates your life?
The SCOFF QuestionnaireThe SCOFF Questionnaire
• Ask all patients 10 – 40 years old in high risk groupsgroups
• Count one point for every “yes” answer
• Score of ≥ 2 likely anorexia nervosa or bulimia nervosa
Work-upWork up
• Height and weightHeight and weight
• CBC with diff
• Chem 7 with mag and phosphChem 7 with mag and phosph
• LFT’s
• TSH• TSH
• UA
• FOBT• FOBT
• EKG
DEXA if di f 6 h• DEXA if disease for ≥ 6 months

When to Hospitalize?When to Hospitalize?
For Anorexia Nervosa: For Bulimia Nervosa:For Anorexia Nervosa:
– Inpatient care below 75% of
For Bulimia Nervosa:
– Potassium <2.2 mmol/Lideal body weight
– Severe organ dysfunction: cardiac (arrhythmias),
l l l
– Bicarbonate > 40 mmol/L
– Excessive edema
– History of edema with gastrointestinal, electrolyte, hematologic
– Worsening weight loss with l d l
History of edema with cessation of purging behaviors
severely restricted caloric intake (at risk for refeeding syndrome)
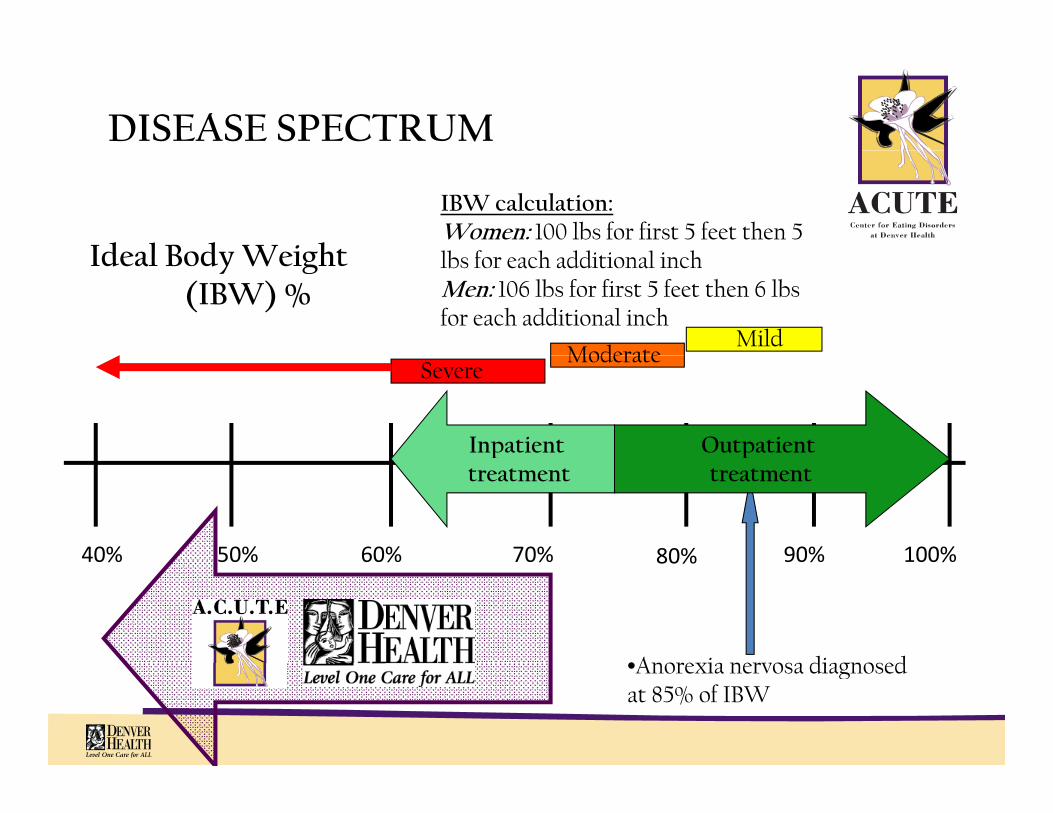
DISEASE SPECTRUM
Ideal Body Weight
IBW calculation:Women: 100 lbs for first 5 feet then 5 lb f h ddi i l i hIdeal Body Weight
(IBW) %
ModerateMild
lbs for each additional inchMen: 106 lbs for first 5 feet then 6 lbs for each additional inch
SevereModerate
Outpatient Inpatient
90%80%70% 100%60%50%
ptreatment
ptreatment
40% 90%80%70% 100%60%50%
•Anorexia nervosa diagnosed
40%
•Anorexia nervosa diagnosed at 85% of IBW
Medical ComplicationsMedical Complications
• Differ depending on the type of eating disorder
– In anorexia, the medical complications are the direct result of starvation and weight lossdirect result of starvation and weight loss
– In bulimia, they correlate with the mode and frequency of purgingfrequency of purging

Medical Complications of AAnorexia Nervosa
• Metabolic • Cardiac• Metabolic– Refeeding syndrome– Plateau effect– Hypercortisolemia
Cardiac– Bradycardia– Tachycardia– The QT question
C ti h t f il• Gastrointestinal– Gastroparesis– Constipation– Hepatitis
– Congestive heart failure– Hypotension
• Endocrine– AmenorrheaHepatitis
– Hypoglycemia– Superior mesenteric artery
syndromeP titi
– Osteoporosis– Cortisol and “the belly”– Thyroid function
• Hematologic– Pancreatitis• Electrolyte dysfunction
– Hyponatremia– Volume contraction
• Hematologic– Pancytopenia

Refeeding SyndromeRefeeding Syndrome
• Caused by life-threatening shifts in fluid and electrolytes as a starved person begins to eaty p g
• Seen initially in unintentional refeeding of WWII victims who died of cardiovascular complicationsp
• Replicated in Keys’ “Minnesota Experiment”
• Rediscovered with the introduction of TPN
Refeeding SyndromeRefeeding Syndrome
• As a starving person is being fed, the body shifts from a g p g , ycatabolic to an anabolic state
– From fat to carbohydrate metabolism
• Glucose in the food stimulates insulin release which drives phosphate and potassium intracellularly
– Lowers serum levels of both K and PhosphLowers serum levels of both K and Phosph
– In addition, insulin decreases sodium excretion in the distal tubule leading to edema
• Newly synthesized cells use these electrolytes as well as magnesium as building blocks thus further depleting serum levelslevels

Refeeding SyndromeRefeeding Syndrome
• Hypophosphatemia causes depletion of ATP and 2,3-DPG which lead to
– Diaphragmatic muscle fatigue
Respiratory failure– Respiratory failure
– Rhabdomyolysis
– Seizure
– CHF (depressed myocardial contractility)
• Fall is seen in the first 2-3 days of refeeding and may last up to 1-2 k2 weeks
• Aggressive replacement of phosphorus is crucial
• Po route is the best absorbed and patients may need up to 3 Po route is the best absorbed and patients may need up to 3 gm per day of potassium acid phosphate
Refeeding SyndromeRefeeding Syndrome
• Hypokalemia may lead to
– Rhabdomyolysis
– Seizures
– Cardiac arrhythmias
ll l h f 4 4• Fall in potassium is seen more acutely over the first 24-48 hours of refeeding and also corrects much faster (over the first 2-3 days)y )
– May replace IV or po
Refeeding SyndromeRefeeding Syndrome
• Edema
– Insulin mediated, NOT related to albumin/oncotic pressure
• Causes increased retention of sodium and thus water in the distal tubule
– Occurs within the first few days of refeeding and resolves Occurs within the first few days of refeeding and resolves within a few weeks
– Treatment consists of low sodium diet, leg elevation, and slow increase of calories
Refeeding SyndromeWh i Ri k?Who is at Risk?
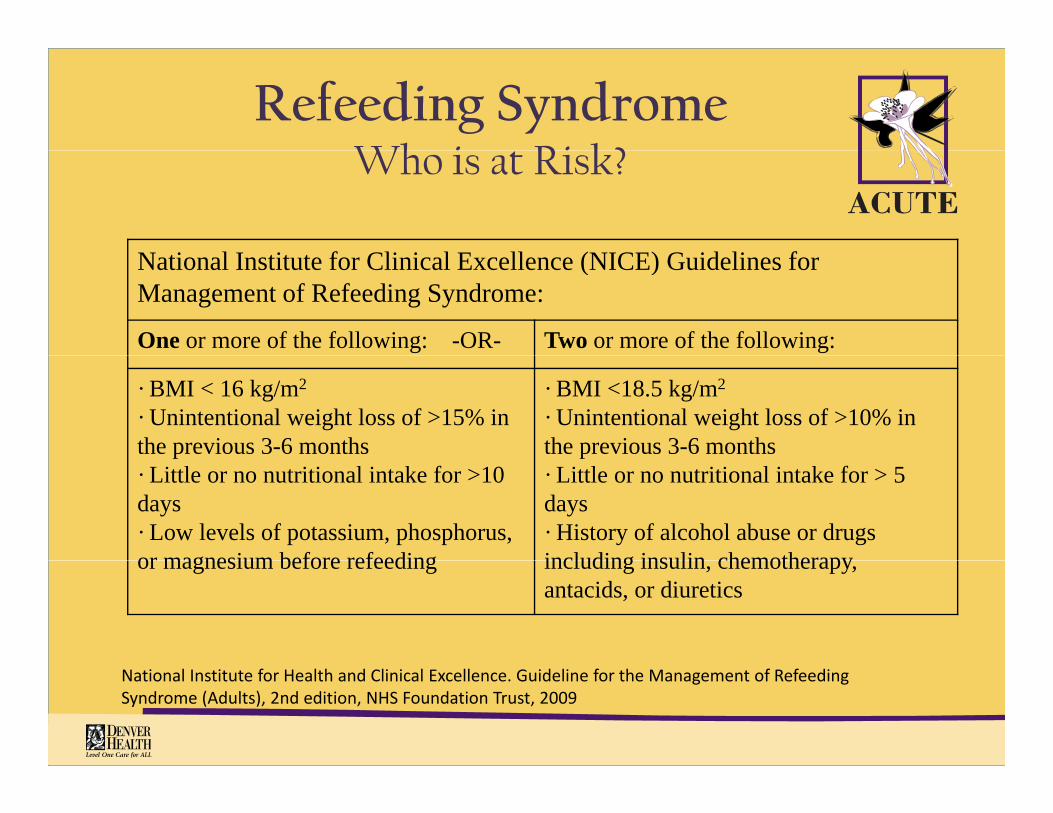
N i l I i f Cli i l E ll (NICE) G id li fNational Institute for Clinical Excellence (NICE) Guidelines for Management of Refeeding Syndrome:
One or more of the following: -OR- Two or more of the following:
· BMI < 16 kg/m2
· Unintentional weight loss of >15% in the previous 3-6 months
· BMI <18.5 kg/m2
· Unintentional weight loss of >10% in the previous 3-6 monthsp
· Little or no nutritional intake for >10 days· Low levels of potassium, phosphorus, or magnesium before refeeding
p· Little or no nutritional intake for > 5 days· History of alcohol abuse or drugs including insulin chemotherapyor magnesium before refeeding including insulin, chemotherapy, antacids, or diuretics
National Institute for Health and Clinical Excellence. Guideline for the Management of Refeeding Syndrome (Adults), 2nd edition, NHS Foundation Trust, 2009
Refeeding SyndromeRefeeding Syndrome
• How to prevent?p
– Recognize at risk patients
– Correct electrolyte disturbances prior to initiating nutritional support
– “Start low and go slow” with kcals based on pt’s basal energy expenditure (BEE)energy expenditure (BEE)
– Increase kcals slowly (by 300-400kcals) every three days and check daily chem 10 for the first week of refeeding
– Low salt diet and leg elevation to prevent/treat edema

HypoglycemiaHypoglycemia
• Maybe due starvation or refeeding
• In starvation:
– Due to depleted glycogen stores in the liver and lack of substrates for gluconeogenesis
• In refeeding:• In refeeding:
– Due to glucose load stimulating insulin secretion and overwhelming the already depleted hepatic glycogen storesg y p p g y g
• Can be life-threatening if not recognized

HypoglycemiaHypoglycemia
• Treatment:
– Nutritional support (i.e. KCALS!!!)
– Check FSBG q 4 hours for the first 24-48 hours of refeeding
+/ D5NS in order to maintain serum glucose above 70– +/- D5NS in order to maintain serum glucose above 70
• May need dextrose for up to 24- 48 hours
Cardiac ComplicationsCardiac Complications
• The heart in the severely malnourished patients loses mass y pwhich leads to decreased cardiac output
– May lead to acute heart failure if overwhelmed with the i d i l ti bl d l t d i increased circulating blood volume present during refeeding
– Hypokalemia and hypophosphatemia may lead to yp yp p p yarrhythmias and decreased contractility
– Cardiac mortality is likely due to QT dispersion and low h i bili heart rate variability
• All hospitalized patients should have a baseline EKG and be kept on telemetrykept on telemetry

HepatitisHepatitis
• Abnormalites in LFT’s are common in the severely malnourished state and maybe due to starvation or refeeding
• The mechanism for hepatitis of starvation is apotosis or autophagy
– May see transaminases up to 30 x upper limit of normalMay see transaminases up to 30 x upper limit of normal
– Treatment is continued nutritional support and normalization of liver function returns within 1-2 weeks into refeeding
HepatitisHepatitis
• Steatohepatitis of refeeding is manifested by increasing p g y gAST/ALT during the initial phases of refeeding
– Likely due to dextrose causing fat accumulation
– Treatment for this is decreased feeding rate/kcals
• Serial liver ultrasounds can aid in differentiation
Normal sized liver is indicative of starvation hepatitis– Normal sized liver is indicative of starvation hepatitis
• CONTINUE pushing kcals
– Enlarging liver is indicative of refeeding hepatitisEnlarging liver is indicative of refeeding hepatitis
• SLOW down kcal intake
Bone Marrow Suppression Bone Marrow Suppression
• Severe malnutrition causes suppression of the bone marrow and replacement of its matrix with one that does not produce
llcells– Serous fat atrophy
• Trilinear hypoplasia: anemia, leukopenia, and yp p , p ,thrombocytopenia are very common
• Bone marrow function fully recovers with weight restoration
AmenorrheaAmenorrhea
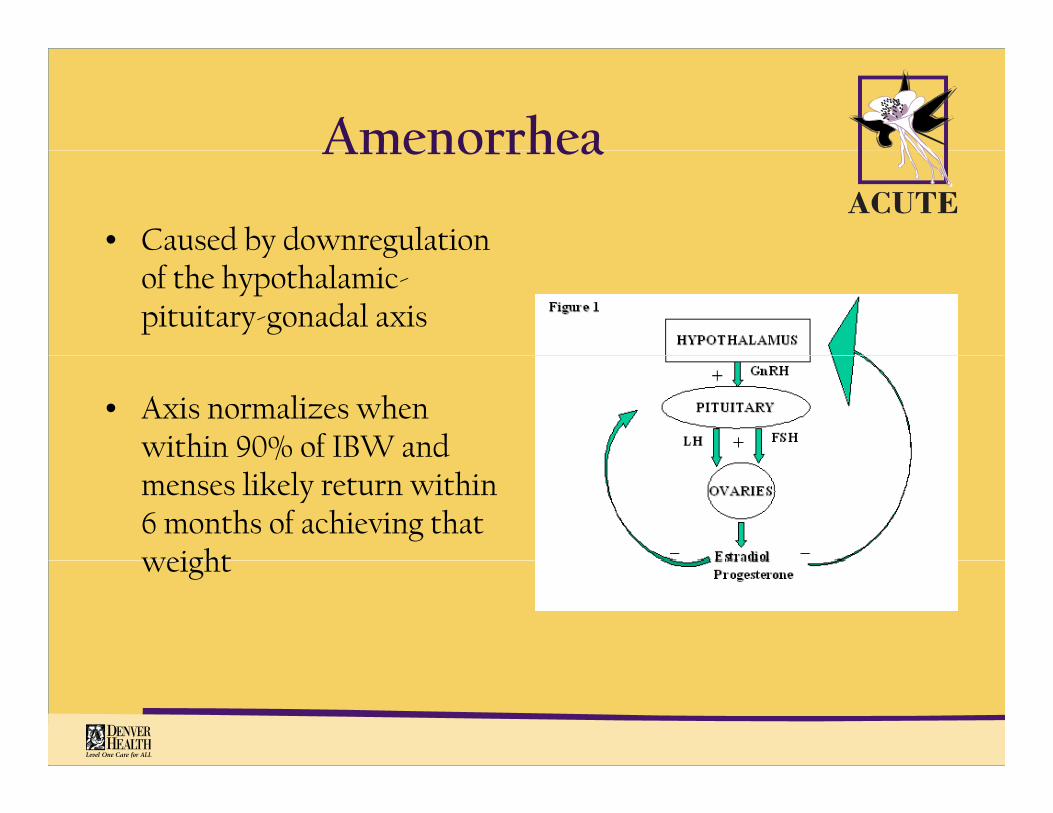
• Caused by downregulation y gof the hypothalamic-pituitary-gonadal axis
• Axis normalizes when within 90% of IBW and %menses likely return within 6 months of achieving that weightweight
GastroparesisGastroparesis
• Occurs as a consequence of kcal restriction and loss of at least 10 Occurs as a consequence of kcal restriction and loss of at least 10 to 20 pounds
• Symptoms include bloating, nausea, flatus, and abdominal pain h ’ d f lthat’s more pronounced after meals
• Treatment:
– Avoidance of high fiber dietAvoidance of high fiber diet
– Weight restoration (resolves when within 80% of IBW)
– Small, more frequent meals with kcals in liquid form
– Use of reglan 30 minutes prior to meals helps speed up transit time through the GI tract and alleviate symptoms
• 2 5 to 5 mg prior to meals• 2.5 to 5 mg prior to meals
OsteoporosisOsteoporosis
• Occurs solely in anorexia and usually begins early in disease d i klcourse and progresses quickly
• Peak bone mass is achieved by the end of the second decade which is the time when anorexia manifests itselfwhich is the time when anorexia manifests itself
• These patients never reach peak bone mass thus their osteoporosis is severe and resistant to treatment– Trabecular bone is affected more than cortical
• Duration of amenorrhea is the best predictor of bone density
A baseline DEXA should be performed 6 months after the – A baseline DEXA should be performed 6 months after the cessation of menses
• Weight restoration leading to activation of the hypothalamic-g g yppituitary-gonadal axis is the best treatment
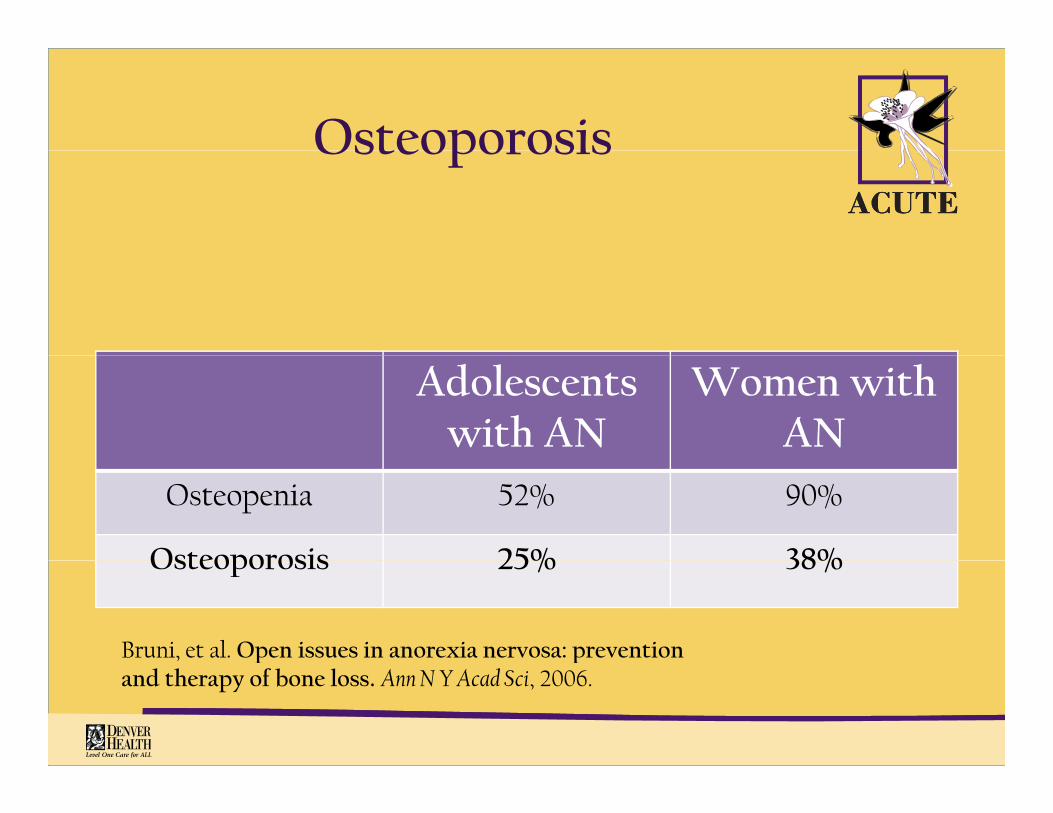
OsteoporosisOsteoporosis
Adolescentswith AN
Women withAN
Osteopenia 52% 90%
Osteoporosis 25% 38%Osteoporosis 25% 38%
Bruni, et al. Open issues in anorexia nervosa: prevention p pand therapy of bone loss. Ann N Y Acad Sci, 2006.
OsteoporosisOsteoporosis
• Treatment:
• Estrogen replacement and exercise are neither g pprotective nor therapeutic
• Bisphosphonates have questionable benefit and can h (f h hcause harm to neonates (for patients that weight
restore)
• All patients should be placed on Calcium and have • All patients should be placed on Calcium and have adequate vitamin D levels (25-OH vit D above 30)
Anorexia Nervosa PearlsAnorexia Nervosa Pearls
• Patients at < 70% IBW should undergo refeeding in a hospitalized setting with professionals familiar with such
ti tpatients
• Refeeding syndrome can be deadly and patients should be closely monitoredy
• “Start low and go slow” with kcalories
• Most medical complications, except osteoporosis, do resolve with weight restoration
Medical Complications of lBulimia Nervosa
• Metabolic • Dental erosion– Electrolyte imbalance
– Dehydration
• Renal
• Cardiac– Arrhythmias
– Diet pill toxicity: palpitations,
– Acute kidney injury
– Edema: total body, pulmonary, cerebral
hypertension
– Emetine cardiotoxicity
– Mitral valve prolapse
• Endocrine• Gastrointestinal
– Constipation
– Esophageal rupture
• Endocrine– Irregular menses
– Mineralocorticoid excess
• Pulmonary Mediastinal– GERD
– Cathartic colon
• Sialadenitis
• Pulmonary-Mediastinal– Aspiration pneumonitis
– Pneumomediastinum
PseudoBartter’s SyndromePseudoBartter s Syndrome
• Case:
– 18 yr female with AN-binge purge subtype who vomits 3-4 times daily presented to ACUTE complaining of abdominal pain and bloating
– Height 5’3” with a weight of 72 6 lbs ( 63% IBW)Height 5 3 with a weight of 72.6 lbs ( 63% IBW)
– Labs
• Na: 124 mmol/L
• K: 1.6 mmol/L
• Bicarbonate: 52 mmol/L
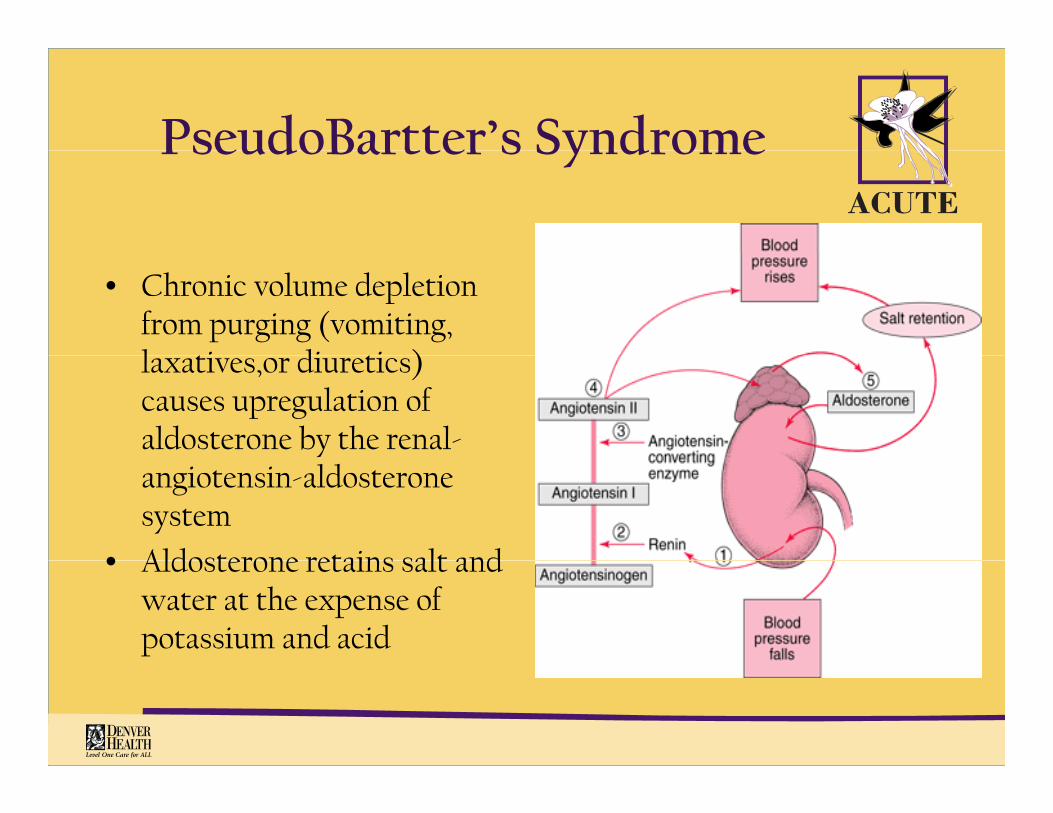
PseudoBartter’s SyndromePseudoBartter s Syndrome
• Chronic volume depletion from purging (vomiting, l ti di ti ) laxatives,or diuretics) causes upregulation of aldosterone by the renal-angiotensin-aldosterone system
• Aldosterone retains salt and • Aldosterone retains salt and water at the expense of potassium and acid
PseudoBartter’s SyndromePseudoBartter s Syndrome
• Renal retention of salt and water (due to high circulating aldosterone) leads to low serum potassium and high bi b t ( t b li lk l i / t ti lk l i )bicarbonate (metabolic alkalosis/contraction alkalosis)
• In order to downregulate, or “shut off” aldosterone, volume restoration is keyy
• Aggressive volume resuscitation may lead to acute congestive heart failure or severe edema so with most other things in h i fl id b d i i d l l D5NS these patients, fluids are to be administered slowly, D5NS at
50cc/hr for 1-2 days
PseudoBartter’s SyndromePseudoBartter s Syndrome
• Potassium repletion is futile unless concomitant volume prestoration is in progress
– May place KCl in D5NS
• Because aldosterone is a hormone, its downregulation may take up to 2-3 weeks
– Spironolactone maybe given in these patients for the first 2 Spironolactone maybe given in these patients for the first 2 weeks of cessation of purging behaviors in order to block the action of aldosterone while waiting for the axis to shut i lf ffitself off
– Spironolactone is an aldosterone inhibitor, provides mild diuresis, and as a potassium-sparing diuretic aids in the diuresis, and as a potassium sparing diuretic aids in the correction of hypokalemia

PseudoBartter’s SyndromePseudoBartter s Syndrome
• Dose of spironolactone is 25-50mg daily for 1 to 2 weeks
• In addition to volume restoration +/- use of spironolactone, patients should
– Be on a low salt diet (< 3gm of salt per day)
Elevate legs– Elevate legs
– Be patient as the edema will resolve within two to three weeks of cessation of purgingp g g
GERDGERD
• Commonly seen in BN given vomiting
• Symptom severity does not predict the occurrence of Barrett’s esophagus but chronicity does
• No need for endoscopy unless “red flags” occur such as dysphagia anemia or persistent dyspepsia despite treatment dysphagia, anemia, or persistent dyspepsia despite treatment
• Proton pump inhibitors are more effective for healing esophagitis than are histamine-2 receptor blockers
• Metoclopromide may also be used 30 minutes prior to meals to decrease the frequency of vomiting
ConstipationConstipation
• Weight loss may lead to slow colonic transit and low caloric intake may lead to reflex hypofunctioning of the colon
• Worsened by electrolyte abnormalities such as hypokalemia and volume depletion
• Cathartic colon syndromeCathartic colon syndrome• consequence of laxative abuse
• permanent damage to colonic nerves leading to further constipation d l t it tiand slower transit time
ConstipationConstipation
• Counsel patients about the ineffectiveness of laxatives for weight lloss
• Reassure patients that bowel function will normalize again after laxatives have been discontinued but may take up to several y pweeks
• Remind patients that per Rome criteria, “normal bowel function” is anything more than 2 bowel movements per WEEK!is anything more than 2 bowel movements per WEEK!
• Polyethylene glycol (Miralax), an osmotic laxative, has been the most successful in such patients. Avoid any stimulant laxative (senna)
• If constipation persists and becomes bothersome, glycerin suppositories are very helpfulsuppositories are very helpful
SialoadenosisSialoadenosis
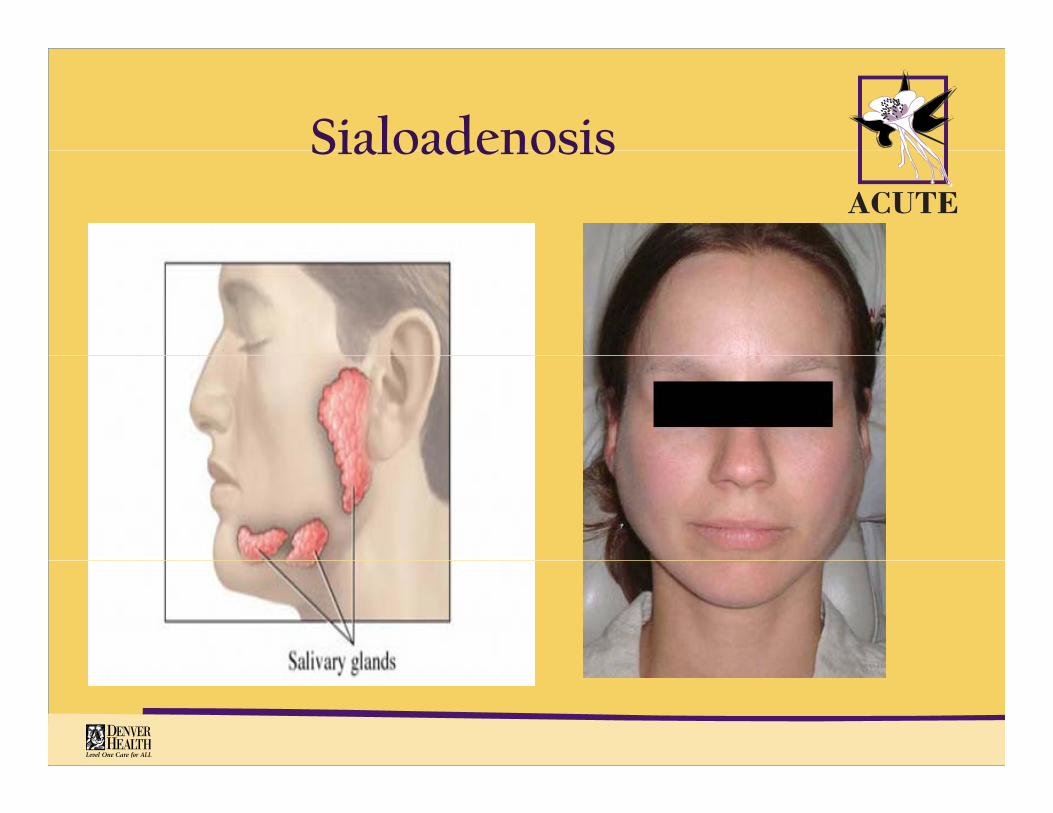
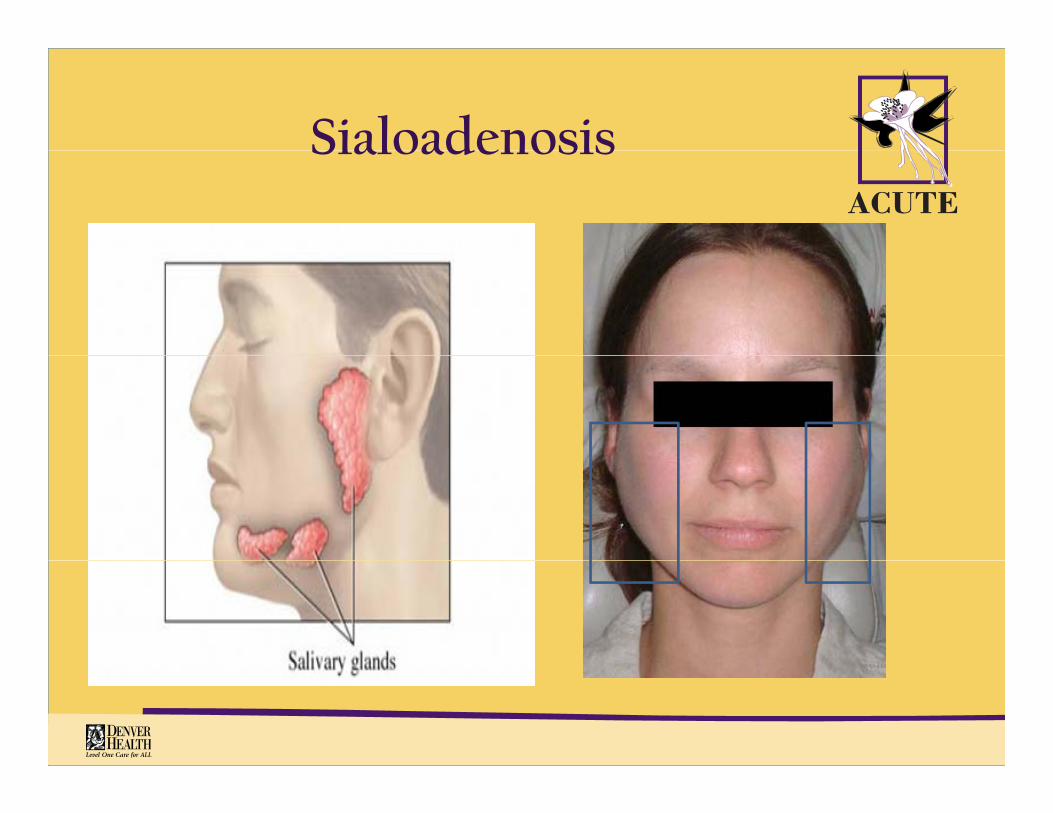
• Hypertrophy of the salivary glands in response to chronic purging
• Seen about three days after cessation of vomiting
• Can be very distressing for patients given their body image issuesissues
• Painful at times
• Recedes within a few weeks of purging cessationp g g
SialoadenosisSialoadenosis
SialoadenosisSialoadenosis
SialoadenosisSialoadenosis
• Treatment:
– Cessation of vomiting
– Application of warm compresses to the glands
– Sucking sour/tart candies in order to stimulate saliva production, clear the ducts, and decompress the glands
NSAIDs– NSAIDs
– In extreme cases, pilocarpine (parasympathetic muscarinic receptor agonist that increases saliva production) maybe p g p ) yused
• 5 mg TID
Bulimia Nervosa PearlsBulimia Nervosa Pearls
• Stop purging behaviorsp p g g
• Slowly restore volume in order to shut off hormonal mechanisms responsible for edema and electrolyte
b litiabnormalities
• Judiciously use spironolactone in select cases
• Do not treat constipation with stimulant laxatives but with Do not treat constipation with stimulant laxatives but with osmotic laxaties such as polyethylene glycol or suppositories
• Treat GERD with PPIs
• Treat sialadenosis with warm compresses and sour candy
• Complications will resolve with weight restoration
Questions?????Questions?????