Medical Benefit Highlights - Haverford College...Tagalog, magagamit mo ang mga serbisyo na tulong sa...
7
Independence @1 Medical Benefit Highlights Personal Choice HDHP HDl-HCI Haverford College Covered Services Benefits per Calendar Year Deductible (Aggregate)1 Individual/Family Out-of-Pocket Maximum (Embedded)2 Individual/Family Coinsurance Your Costs (You pay) Out-of-Network In-Network $1 ,500/$3,000 $5,000/$10.000 $6 ,350/$ 12,700 0% $10,000/$20,000 50% Preventive Services Preventive Care Preventive Colonoscopy Preventive Plus Providers Hospital Based In-Network No charge no deductible Out-of-Work 50% no deductible No charge no deductible Nochargeno deductible Not covered 50%no deductible Physician Services Primary Care Physician (PCP) Office Visit Specialist Office Visit Retail Health Clinic Visit Urgent Care Visit In-Network No chargeafterdeductible No chargeafterdeductible No charge after deductible No charge after deductible Out-of-Network 50% after deductible 50% after deductible 50% after deductible 50% after deductible Virtual Care3 Telemedicine Teledermatology Telebehavioral Health In-Network No chargeafter deductible No chargeafterdeductible No chargeafterdeductible Out-of-Network Not covered Not covered Not covered Therapy Services Physical Therapy (60 visits/year)4 Freestanding Hospital Based Occupational Therapy (60 visits/year)4 Freestanding Hospital Based Speech Therapy (60 visits/year)5 In-Network Out-of-Network No charge after deductible No charge after deductible 50% after deductible 50% after deductible No chargeafterdeductible No chargeafterdeductible No chargeafterdeductible 50% after deductible 50% after deductible 50% after deductible Emergency Services Emergency Room Emergency Ambulance Non-Emergency Ambulance In-Network No charge after deductible No charge after deductible No charge after deductible Out-of-Network Covered at In-Network level Covered at In-Network level 50% after deductible Reference ID: 1004082301012021
Transcript of Medical Benefit Highlights - Haverford College...Tagalog, magagamit mo ang mga serbisyo na tulong sa...

Independence @1
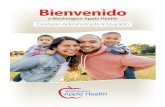
Medical Benefit HighlightsPersonal Choice HDHP HDl-HCI Haverford College
Covered Services
Benefits per Calendar YearDeductible (Aggregate)1
Individual/Family
Out-of-Pocket Maximum (Embedded)2Individual/Family
Coinsurance
Your Costs (You pay)Out-of-NetworkIn-Network
$1 ,500/$3,000 $5,000/$10.000
$6 ,350/$ 12,700
0%
$10,000/$20,00050%
Preventive ServicesPreventive Care
Preventive ColonoscopyPreventive Plus Providers
Hospital Based
In-Network
No charge no deductibleOut-of-Work50% no deductible
No charge no deductibleNo charge no deductible
Not covered50% no deductible
Physician ServicesPrimary Care Physician (PCP) Office Visit
Specialist Office VisitRetail Health Clinic Visit
Urgent Care Visit
In-Network
No charge after deductibleNo charge after deductibleNo charge after deductibleNo charge after deductible
Out-of-Network50% after deductible
50% after deductible
50% after deductible50% after deductible
Virtual Care3Telemedicine
TeledermatologyTelebehavioral Health
In-Network
No charge after deductibleNo charge after deductibleNo charge after deductible
Out-of-NetworkNot coveredNot coveredNot covered
Therapy ServicesPhysical Therapy (60 visits/year)4
Freestanding
Hospital BasedOccupational Therapy (60 visits/year)4
Freestanding
Hospital BasedSpeech Therapy (60 visits/year)5
In-Network Out-of-Network
No charge after deductible
No charge after deductible
50% after deductible
50% after deductible
No charge after deductibleNo charge after deductibleNo charge after deductible
50% after deductible
50% after deductible50% after deductible
Emergency ServicesEmergency Room
Emergency Ambulance
Non-Emergency Ambulance
In-Network
No charge after deductibleNo charge after deductibleNo charge after deductible
Out-of-NetworkCovered at In-Network level
Covered at In-Network level50% after deductible
Reference ID: 1004082301012021

Independence @I
Hospital ServicesInpatient Hospital Services (In-Network:365 days/year; Out-of-Network: 70 days/year)6Observation Services
Maternity Hospital Services6Inpatient ProfessIonal Services (includesMaternity)
In-Network
No charge after deductible
Out-of-Network50% after deductible
No charge after deductibleNo charge after deductibleNo charge after deductible
50% after deductible
50% after deductible
50% after deductible
Outpatient SurgeryFreestanding
Hospital BasedOutpatient Professional Services
In-Network
No charge after deductibleNo charge after deductibleNo charge after deductible
Out-of-Network50% after deductible
50% after deductible
50% after deductible
Outpatient DiagnosticsDiagnostic Medical (EKG)Routine Radiotogy (X-Ray)
Freestanding
Hospital Based
Advanced Imaging (MRI/MRA,CT/CTAScan, PET Scan)
Freestanding
Hospital Based
In-Network
No charge after deductible
Out-of-Network50% after deductible
No charge after deductibleNo charge after deductible
50% after deductible
50% after deductible
No charge after deductibleNo charge after deductible
50% after deductible
50% after deductible
Outpatient Lab and PathologyFreestanding
Hospital Based
In-Network
No charge after deductibleNo charge after deductible
Out-of-Network50% after deductible
50% after deductible
Other Medical Services
Spinal Manipulations (20 visits/year)5Acupuncture (18 visits/year)5
Standard InjectablesAllergy InjectionsBiotech/Specialty Injectables
Home/Office
OutpatientChemotherapy
Dialysis
Skilled Nursing Facility (120 days/year)5Home Health
Hospice
Durable Medical Equipment (DME)
In-Network
No charge after deductibleNo charge after deductible
No charge after deductible
No charge after deductible
Out-of-Network50% after deductible50% after deductible50% after deductible50% after deductible
No charge after deductibleNo charge after deductibleNo charge after deductibleNo charge after deductibleNo charge after deductibleNo charge after deductibleNo charge after deductibleNo charge after deductible
50% after deductible
50% after deductible
50% after deductible
50% after deductible
50% after deductible
50% after deductible
50% after deductible
50% after deductible
Reference ID: 1004082301012021

Independence @I
Mental Health – Outpatient (includesserious mental illness and substanceabuse)
Mental Health - Inpatient (includesserious mental illness and substanceabuse)6
No charge after deductible 50% after deductible
No charge after deductible 50% after deductible
1
2
3
4
5
6
Aggregate deductible: For family coverage, the entire family deductible must be met before copayments or coinsurance are applied for anindividual member.
Embedded out-of-pocket maximum: Each covered family member only needs to satisfy his or her individual out-of-pocket maximum, not the entirefamily out-of-pocket maximum
Telemedicine is provided by a designated telemedicine provider, please visit www.ibx.com/findcarenow.
Physical Therapy, Occupational Therapy, and Cognitive Therapy combined visit limit in and out-of-network
Combined in and out-of-network.
Inpatient hospital out-of-network day limit combined for all inpatient medical, maternity, mental health, serious mental illness, and substance abuseservices
The Personal Choice(B) Preferred Provider Organization (PPO) gives you freedom of choice by allowing you to select your own doctors and hospitalsYou maximize your coverage by accessing care through Personal Choice's network of hospitals, doctors, and specialists, or by accessing care throughpreferred providers who participate in the Blue(_,ard® PPO program. If you access care from a provider who does not participate in our network, you willhave higher out-of-pocket costs and may have to submit your claim for reimbursement
This summary represents only a partial listing of benefits and exclusions of the Medical Program described in this summary. If your employerpurchases another program, the benefits and exclusions may differ. Also, benefits and exclusions may be further defined by medical policy. As a resultthis managed care plan may not cover all of your health care expenses. Read your contract/member benefit booklet carefully for a complete listing ofterms, limitations, and exclusions of the program. For more information about your coverage, or to get a copy of the complete terms of coverage, visitwww.ibx.com/LGBooklet or call 1-800-ASK-BLUE (TTY: 71 1 )
Benefits may be changed by Independence Blue Cross to comply with applicable federal/state laws and regulations
Certain services require preapproval/precertification by the health plan prior to being performed. To obtain a list of services that require authorizationplease log on to http://www.ibx.com/preapproval or call the phone number that is listed on the back of your identification card
Benefits underwritten or administered by QCC Insurance Company, a subsidiary of Independence Blue Cross - Independent licensees of the BlueCross and Blue Shield Association. www.ibx.com
Reference ID: 1004082301012021

Independence @I
Drug Benefit HighlightsPersonal Choice HDHP HDl-HCI Haverford College Rx
Covered Services
Benefits per Calendar YearDeductible
Individual/FamilyOut-of-Pocket Maximum
Individual/Family
Formulary
Your Costs (You pay)In-Network Out-of-Network
Medical deductible applies. Medical deductible applies.
Combined with Medical Combined with Medical
Select
Retail PharmacyTier 1 Generic Drugs
In-Network$5 after deductible
Out-of-Network50% Reimbursement afterdeductible
50% Reimbursement afterdeductible
50% Reimbursement afterdeductible
30 day supply max
Tier 2 Preferred Brand $20 after deductible
Tier 3 Non-Preferred Drugs $45 after deductible
Dispensing Limits 30 day supply max
Mail Order PharmacyAvailable for maintenance drugsTier 1 Generic DrugsTier 2 Preferred Brand Drugs
Tier 3 Non-Preferred Drugs
Dispensing Limits1
In-Network Out-of-Network
$10 after deductible
$40 after deductible
$90 after deductible
90 day supply max
Not coveredNot coveredNot coveredNot covered
Drug CoverageACA Preventive Drugs2Compound Medications
Contraceptives
Diabetic Supplies (i.e., test strips)
Glucometers (no copaymenUcoinsurance requiredat participating pharmacies after deductible)Insulin
Insulin Needles and Syringes
Lancets (no copayment/coinsurance required atparticipating pharmacies after deductible)
Prescribed Tobacco Cessation Drugs (RX and OTC)
Retin-A (up to Age 35)
Allergy SerumI
Blood, Blood Plasma
r
In-NetworkCovered
Covered
Covered
Covered
Covered
Out-of-NetworkCovered
Covered
Covered
Covered
Covered
Covered
Covered
Covered
Covered
Covered
Covered
CoveredCovered
Not coveredNot coveredNot coveredNot covered
Covered
Covered
Not covered
Not covered
Not covered
Not covered
Reference ID: 1004082801012021

Independence @Immunization Agents Not covered Not covered
Injectable Fertility Drugs Not covered Not covered
Non-Federal Legend DrugsOver-The-Counter Drugs (Non-Prescription)
Not covered Not coveredNot covered
Not covered
Not coveredNot coveredWeight Control Drugs
1
2
Up to a 90-day supply of drugs to treat chronic conditions available at any participating retail pharmacy or mail for same cost share
Certain designated preventative medications will not be subject to any cost-sharing or deductibles, but will be subject to the terms and conditionsof your benefits contract. Refer to your summary of benefits, member handbook, and/or benefit booklet to determine if your plan includes 100percent coverage for in-network preventive services.
This summary represents only a partial listing of benefits and exclusions of the Prescription Drug Program described in this summary. If your employerpurchases another program, the benefits and exclusions may differ. Also, benefits and exclusions may be further defined by pharmacy policy. As aresult, this program may not cover all of your health care expenses. Read your contract/member benefit booklet carefully for a complete listing ofterms, limitations, and exclusions of the program. For more information about your coverage, or to get a copy of the complete terms of coverage, visitwww.ibx.com/LGBooklet or call 1-800-ASK-BLUE (TTY: 71 1),
Any prescription refilled in excess of the number of refills specified by the physician, or any refill dispensed after one year from the physician's originalorder are not covered. Devices or supplies except those specifically listed under covered drugs are not covered. Drugs used to treat hemophilia arenot covered
All covered self-administered specialty medications except insulin will be provided through the convenient Specialty Pharmacy Program for theappropriate cost sharing indicated above. If your doctor wants you to start the drug immediately, an initial 30-day supply may be obtained at a retailpharmacy. However, all subsequent fills must be purchased through the Specialty Pharmacy Program
FutureScripts® network includes more than 65,000 retail pharmacies. You can locate a participating pharmacy near you on www.ibx.com byselecting the Find a Participating Pharmacy featureFutureScripts® is an independent company providing pharmacy benefit management service.
Benefits underwritten or administered by QCC Insurance Company, a subsidiary of Independence Blue Cross - Independent licensees of the BlueCross and Blue Shield Association. www.ibx.com
Reference ID: 1004082801012021

Language Assistance Services Tagalog: PAUNAWA: Kung nagsasalita ka ngTagalog, magagamit mo ang mga serbisyo na tulongsa wika nang walang bayad. Tumawag sa1 -800-275-2583.
Spanish: ATENCION: Si habla espa6ol, cuenta consewicios de asistencia en idiomas disponiblesde forma gratuita para usted. Llarne al1-800-275-2583 (TTY: 711). French: ATTENTION: Si vous parlez frangais, des
services d'aide linguistique-vous sont propos6sgratuitement. Appelez Ie 1-800-275-2583.Chinese: H&: luRe:if OII Jg:aLl+B$1j%©Aqiti=
tD.ELBE%. it IB 1-800-275-2583.Pennsylvania Dutch: BASS UFF: Wann duPennsylvania Deitsch schwetzscht, kannscht du Hilfgriege in dei eegni Schprooch unni as es dich ennicheppes koschte zellt. Ruf die Nummer 1-800-275-2583
Korean: gF LH Alg : Be CHS /\F gap /\lb gg , a CH
RIg Al EIIAS PSB OIg aPg + £££ LI EP .1-800-275-2583 W ge 8 aF abd Al 9 .
Portuguese: ATEN(,,Ao: se voc6 fala portugu6s,encontram-se disponiveis servigos gratuitos deassist6ncia ao idioma. Ligue para 1-800-275-2583.
Hindi: Hra &: dk Hn fMI gjad i at 3rn# fBuqqal+HrvraFma+3Tt wwt! fIgfm q:+1 -800-275-2583 1
G„ja„ti, q&Fu, a dR DJ%el,fl daaru R, a tit:qc'8
eUNL tl,}ta &cut;a ,ItU el qL: eVaa& B.German: ACHTUNG: Wenn Sie Deutsch sprechen,k6nnen Sie kostenlos sprachliche UnterstOtzunganfordern . wahlen Sie 1-800-275-2583.
1-800-275-2583 aa 88.
Vietnamese: LL/U Y: N6u bgn n6i ti6ng viet, chClng t6isd cung cap djch vy ha trq ng6n ngO mi6n phi chobgn. Hay gQi 1-800-275-2583.
Japanese: fH4 : Hmi#ii rl4i#m + Ii, gi97 S/ 79 yx't–E'x (M++) &:#IIMb~/If:'}} it.1-800-275-2583 Ab’En < tI $ b ~.
Russian: BHmMAHHE: Ecnu Bbl roBopuTe no-pyccKU,TO Mo>KeTe 6ecnnaTHO BOcnonb30BaTbcn ycnyraMU
nepeBona. Ten .: 1-800-275-2583.
Persian (Farsi):dJ)'n c: CA+JI dl,A , a un I'\ Jl ,A a_nJli JI :+J
1-800-275-2583 .JU Ll .-JU u- ?-1) U ,gl j JKql J.+JiLl LWLd
Polish UWAGA: Je2eli m6wisz po polsku, mo2eszskorzysta6 z bezp+atnej pomocy jQzykowej . Zadzwohpod numer 1-800-275-2583. Navajo: Dif baa ak6 ninfzin: Dif saad bee y£nihi’go
Din6 Bizaad, saad bee £ka’anfda’iwo’dee’, t’ai jiik’eh.H6dfflnih koji’ 1-800-275-2583.Italian: ATTENZIONE: Se lei parla italiano, sono
disponibili sewizi di assistenza linguistica gratuitiChiamare il numero 1-800-275-2583. Urdu:
cd cS VT i ',A gla JLri J.Jl vi it :£!JKJ. +JdJS JLS _oH +LILA: dLA:i JJLAn JLjJ cen a,
. 1 -800-275-2583
Arabic:4JJ!\ iI&l,J\ atAri JP ,4+?JJ\ adI\ &E:i &K Ii] ::LEA
.1-800-275-2583 PJ b1 . C,a, 'a1 i,Ll-
French Creole: ATANSYON: Si w pale Krey61
Ayisyen, gen sdvis dd pou lang ki disponib gratis pouou. Rele 1-800-275-2583.
Mon-Khmer, Cambodian: hJHrHDl tn€iHliqrfn:al
Luhis IDeas Lin tom anus-igf yin Fm igf tFI :fist£iiGnm hn gains Gf$USd diFnnnHnFfn Etiama a n & a
8ni6 1 BlaiR tfltm8 1-800-275-25831CV U a
YO041 HM_17_47643 Accepted 10/14/2016 Taglines as of 1 0/14/2016

Discrimination is Against the Law
This Plan complies with applicable Federal civil rightslaws and does not discriminate on the basis of race,color, national origin, age, disability, or sex. This Plandoes not exclude people or treat them differentlybecause of race, color, national origin, age, disability,or sex.
If you need these services, contact our Civil RightsCoordinator. If you believe that This Plan has failedto provide these services or discriminated in anotherway on the basis of race, color, national origin, age,disability, or sex, you can file a grievance with our CivilRights Coordinator. You can file a grievance in thefollowing ways: in person or by mail: ATTN: CivilRights Coordinator, 1 901 Market Street,Philadelphia, PA 19103, By phone: 1-888-377-3933 (TTY: 711) By fax: 215-761-0245, By email:civilrightscoordinator@ 1901 market.com. If you needhelp filing a grievance, our Civil Rights Coordinator isavailable to help you
This Plan provides:• Free aids and services to people with disabilities
to communicate effectively with us, such as:qualified sign language interpreters, and writteninformation in other formats (large print, audio,accessible electronic formats, other formats).
• Free language services to people whoseprimary language is not English, such as:qualified interpreters and information written inother languages.
You can also file a civil rights complaint with the U.SDepartment of Health and Human Services, Office forCivil Rights electronically through the Office for CivilRights Complaint Portal, available athttps://ocrportal.hhs.qov/ocr/portal/lobbv,jsf or by mailor phone at: U.S. Department of Health and HumanServices, 200 Independence Avenue SW., Room509F, HHH Building, Washington, DC 20201, 1-800-368-1019, 800-537-7697 (TDD). Complaint forms areavailable athttp://www . h hs, gov/ocr/office/file/index, html .
YO041 HM 17 47643 Accepted 10/14/2016 Taglines as of 1 0/14/2016