
media.mlive.commedia.mlive.com/saginawnews_impact/other/Discussion of AG... · Web viewThe revision...
33
http://www.michigancannabispatients.com/Forum/viewtopic.php? f=12&t=3438 Sec 1 Obviously no change, this is just the title of the Act. Sec 2 a/ Clearly this is an attempt to rewrite the ballot language to fit something that is more acceptable to the AG’s political views. Rather than say marihuana has been shown to have medical benefits, it is 1
Transcript of media.mlive.commedia.mlive.com/saginawnews_impact/other/Discussion of AG... · Web viewThe revision...

http://www.michigancannabispatients.com/Forum/viewtopic.php?f=12&t=3438
Sec 1
Obviously no change, this is just the title of the Act.
Sec 2
a/ Clearly this is an attempt to rewrite the ballot language to fit something that is more acceptable to the AG’s political views. Rather than say marihuana has been shown to have medical benefits, it is ‘qualified’ to say ‘some components’ of marihuana have been shown to have ‘some beneficial use’. The purpose of this distinction is to raise ‘doubt’ about the actual medical support and uses of marihuana to
1

treat medical conditions, especially ‘unprocessed’ marihuana as opposed to some pharmaceutical preparation.
It changes the intent of the Act from an endorsement of the medical value of marihuana as endorsed by the voters to a qualified maybe. This is to set it up to be questioned by the courts later and to justify prosecutions with very little resistance. It changes the choice to use marihuana as therapy from a reasonable alternative to more traditional therapy to a ‘last resort’ when all other therapy has failed.
b/ This is simply legal trickery. The initial section in the MMMA made it clear that most prosecutions for marihuana were under state law, and the Act was intended to address those prosecutions. It is changed by the AG to indicate the intent was to prevent arrest under ‘state’ law for the ‘vast majority’ of medical users. The reason it is worded this way is to specifically allow state authorities to arrest you under federal law. They are just shifting the justification from state to federal law. The ‘vast majority’ of medical patients mean everyone but YOU. Rather than have the protection from arrest in the original MMMA, all they are saying here is that they won’t arrest a majority of medical users but they will arrest some. Again, by some, that means YOU.
c/ The original Act acknowledges that marihuana is illegal under federal law, but also states many other states have allowed the medical use of marihuana, and that Michigan, like those states, is not required to enforce federal law. The clear implication behind that language is that local law enforcement should honor the MMMA and leave the enforcement of federal law to the federal authorities. The key provision of the MMMA is that local law enforcement is expected to honor the medical use of marihuana. If the intent of the Act was to have the local police enforce federal law, the Act becomes more of a statement of the will of the people as opposed to a binding legal protection. The voters passed the initiative because they wanted sick people to have access to marihuana, period.
The change suggested by the AG does several things. First it again questions the protection of the law and the medical benefits of marihuana with a long discussion about how the only appropriate use under federal law is research by approved labs. Any other use puts people at legal ‘risk’.
It further changes the intent of the MMMA- which originally emphasized that Michigan was joining the other MMJ state to allow the compassionate use of marihuana, clearly a patient centric tone, to one that stresses the continued illegality of marihuana. Again, it demonizes marihuana and allows some select criminals to escape prosecution rather than acknowledges medical use for patients as a viable alternative to traditional care. It also all but states federal law is still there to prosecute those criminals that escape justice under state law because of the revised Act.
Sec 3
1/ Is poorly phrased and confusing in the AG revision, but clearly designed to create an additional burden of proof on the patient to ‘prove’ he or she is ‘sick enough’. The original Act made it clear that if you had one of these conditions, you were by definition ‘sick enough’. The AG is attempting to add a further burden of proof to the patient to essentially show they are at death’s door. The purpose of making this distinction is to aid in prosecution (patient must prove they are suffering enough to a hostile
2

lawyer/prosecutor that they are ‘worthy’), it undermines the decision of the physician, and it reinforces the idea marihuana should only be used in the terminal stages as a treatment of ‘last resort’.
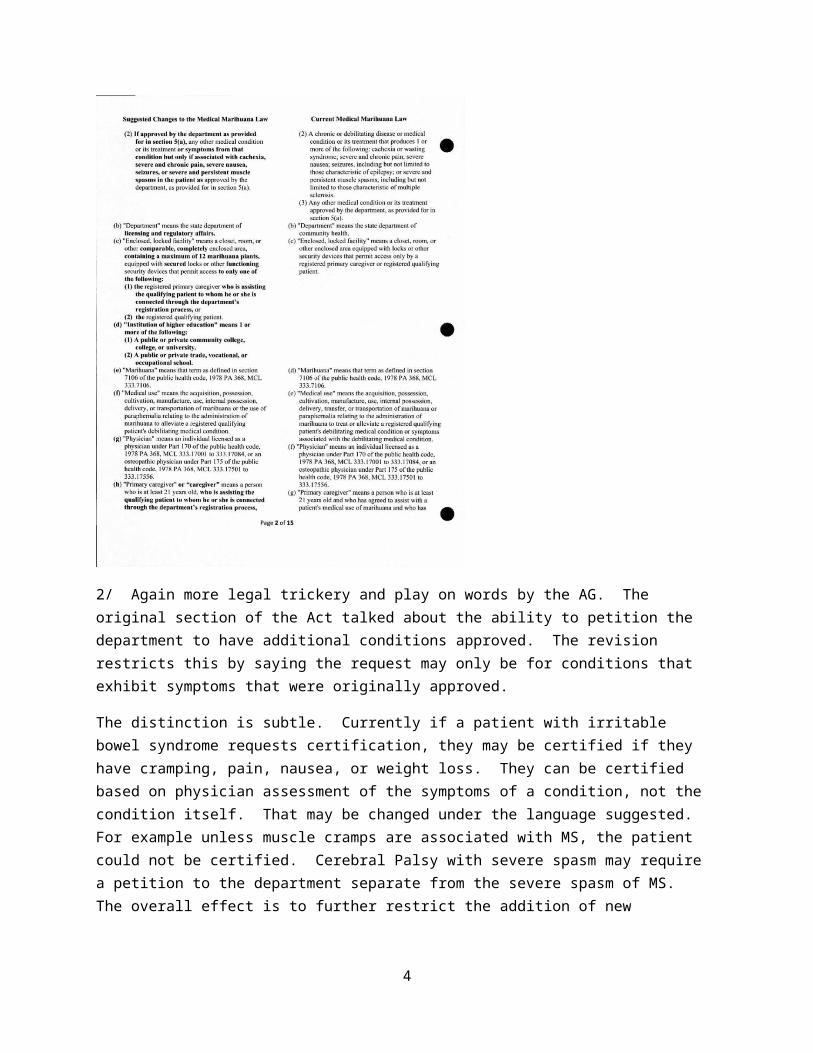
2/ Again more legal trickery and play on words by the AG. The original section of the Act talked about the ability to petition the department to have additional conditions approved. The revision restricts this by saying the request may only be for conditions that exhibit symptoms that were originally approved.
The distinction is subtle. Currently if a patient with irritable bowel syndrome requests certification, they may be certified if they have cramping, pain, nausea, or weight loss. They can be certified based on physician assessment of the symptoms of a condition, not the condition itself. That may be changed under the language suggested. For example unless muscle cramps are associated with MS, the patient could not be certified. Cerebral Palsy with severe spasm may require a petition to the department separate from the severe spasm of MS. The overall effect is to further restrict the addition of new conditions and the application of current conditions to different disease states.
The remainder of the section deals with significant restrictions to the original Act. Highlights of these changes include the following…
3
- The original concept of a ‘enclosed, locked facility’ is strictly defined to include coverage on all sides, top and bottom like a closet. This is specified to disallow uncovered grow areas.
- The AG’s contention that each patient must have a fully separate grow area with not more than 12 plants is formalized in the law. Each caregiver would have to provide 6-12 rooms to keep his and 5 patient’s marihuana fully separated.
- Who could actually enter the room are very narrowly defined to just the caregiver and the registry associated patient. Even something completely innocent and legal under the current MMMA- Grandma with glaucoma growing for herself and her husband with cancer could asking grandson to carry a 50# bag of dirt into the grow room, would be illegal. It would also involve two trips for two separate grow rooms.
- Definitions of what constitutes an institute of higher education (going back the ‘approved research only’ concept) are given. This seems innocuous but is again designed to make a prosecution of a caregiver easier. ‘You aren’t an official research scientist, associated with a university, working on a federally approved protocol, are you Mr. Smith??”
4

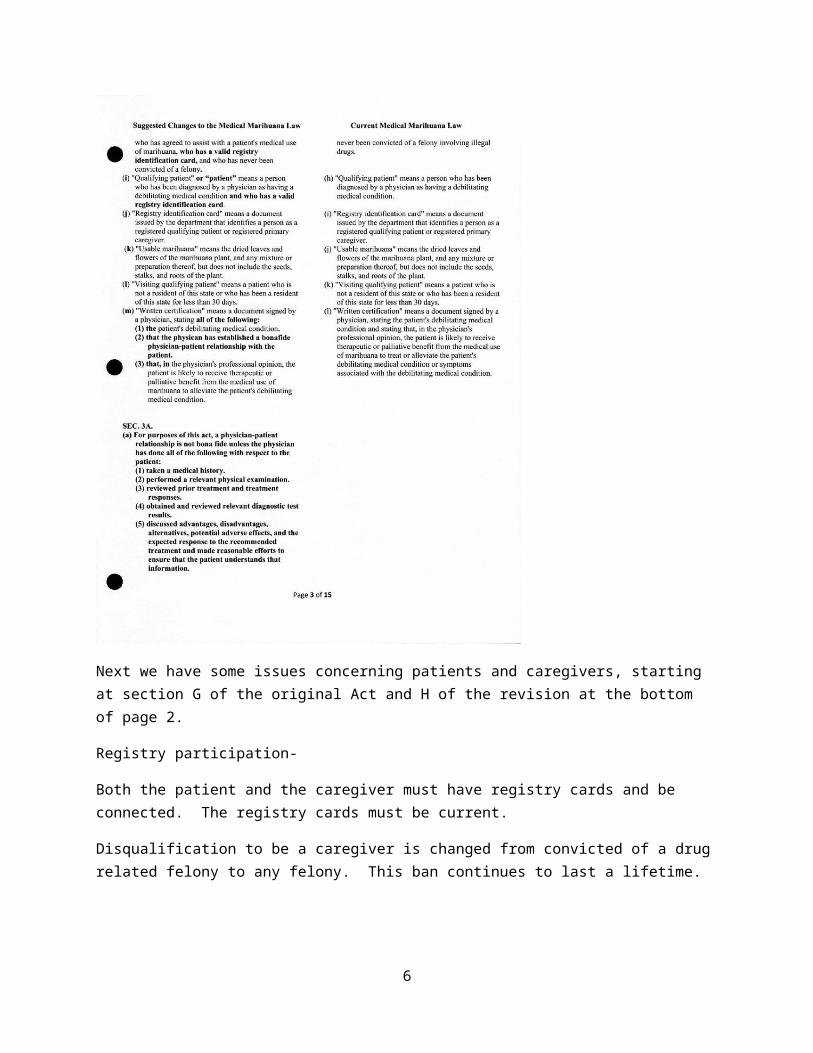
Next we have some issues concerning patients and caregivers, starting at section G of the original Act and H of the revision at the bottom of page 2.
Registry participation-
Both the patient and the caregiver must have registry cards and be connected. The registry cards must be current.
Disqualification to be a caregiver is changed from convicted of a drug related felony to any felony. This ban continues to last a lifetime.
As a separate note, this section appears to require a patient and a caregiver to have the actual card in their possession, rather than paperwork.
Bona fide dr/pt relationship-
There are some common sense and basic good medical practice types of parameters. History, relevant physical exam, discussion of advantages/disadvantages of therapy, follow up are just good medical practice. There is some question of requiring the physician to personally order diagnostic testing and personally review the results. Does this mean the certification physician must order the MRI? Do they have to see the actual MRI report/films, or can they rely on the mention of a disk bulge on the MRI noted in the primary care physician’s report?
Two things that are of significant concern are the requirement to report the certification to the primary care physician and the threat of revocation of the certificate and/or licensure action against the physician. Primary care physicians routinely cut patients off of pain medication or discharge patients for getting medical marijuana cards. Physicians are directly threatened with licensure action for participation in the MMJ program. Both factors will have a chilling effect on certifications, both from the patient’s and the physician’s standpoint. Currently only 1 in 15 physicians have written even one certification and this section will only serve to reduce that number.
As a side note, I am a major certification physician in Michigan and the following is my definition of a ‘bona fide’ doctor patient relationship.
1. Each initial certification and renewal MUST involve ‘real time’ interaction between the patient and the physician.
2. If the patient’s diagnosis has been established to a degree of reasonable medical certainty by a physician level (MD, DO, DC) provider, the certifying physician may ‘confirm’ the diagnosis and issue the cert.
3. If the patient’s diagnosis has not been established as in #2, then the certifying physician must establish the diagnosis themselves. This would involve history, exam, testing, consultation etc. to a level of reasonable medical certainty.
5
4. A treatment plan to include goals of treatment and follow up will be documented in the medical record.
5. Reasonable medical certainty implies using acceptable medical practices to reach a diagnosis which is supported by objective findings and able to withstand peer review.
This is the definition I use and I feel it is appropriate. I will continue to use it until the state comes up with a legally binding definition.
Here in Sec 4 they are again stressing a ‘valid’ card. Again, under the current system a patient can be seen by a certification doctor, get documented but decide not to participate in the registry yet still use a medical defense at trial. The card is supposed to make you immune to arrest and allow you to participate in the patient/caregiver system. If you just wanted to grow your own you could rely on the
6

defense of the certification, but not immune to arrest. They are attempting to put an end to that protection and force you into the registry.
On this page, again the possession of a valid registry card is again stress. It is also clarified that the ONLY legal means of transfer is from caregiver to THEIR registry connected patient. This will settle the question of P2P, Cg2Cg, and Cg2 Non registry associated patient. This will eliminate any pretense of legality for dispensaries, farmers markets, etc. It is a very narrow definition, which is common throughout the revision.
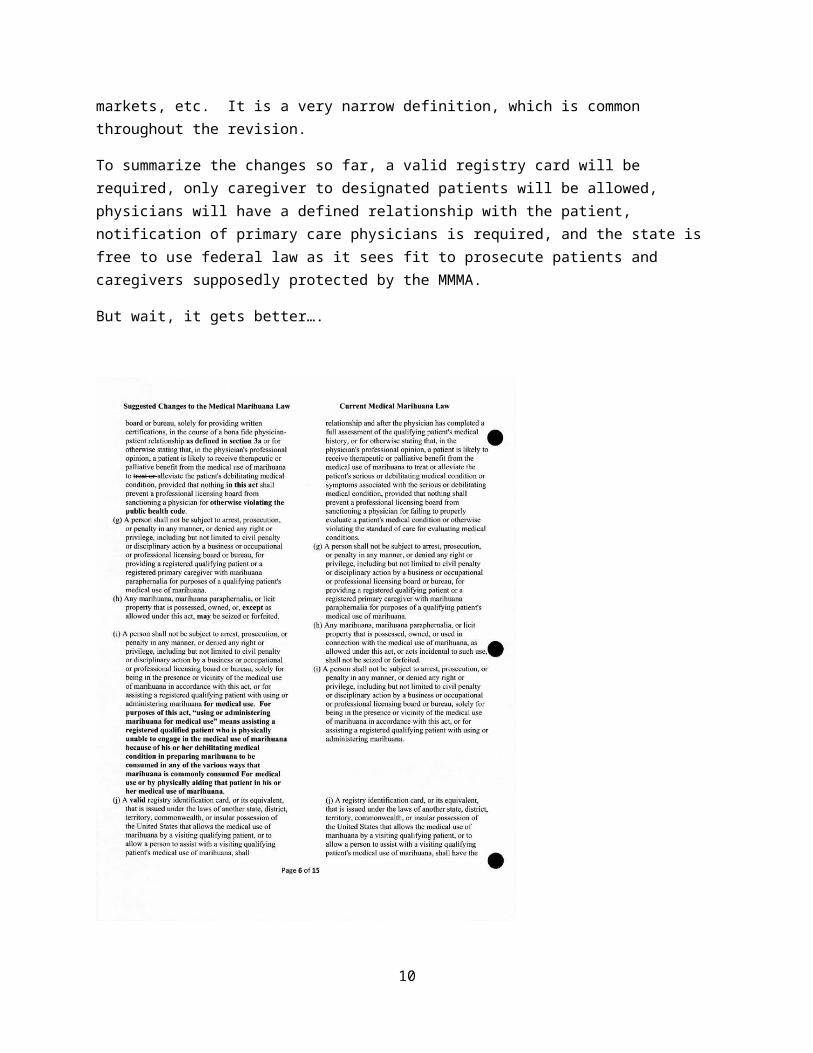
To summarize the changes so far, a valid registry card will be required, only caregiver to designated patients will be allowed, physicians will have a defined relationship with the patient, notification of primary care physicians is required, and the state is free to use federal law as it sees fit to prosecute patients and caregivers supposedly protected by the MMMA.
But wait, it gets better….
7

Highlights of page 6
- Again a rather thinly veiled threat against doctors if they are ruled as violating the ‘bona fide’ doctor/patient relationship, including notification of the primary care doctor.
- Violations of the public health code, unless specifically allowed by the Act, could result in discipline of physicians. Included with this is any ‘off label’ certification. An example would be muscle spasms associated with cerebral palsy or irritable bowel.
- 2.51 ounces of brownie will result in seizure of your assets. As will any violation of the very narrow definition of the Act offered by the AG.
- Assisting with medical use involves ONLY rolling the joint, packing the pipe or offering a lighter IF the patient is physically incapable of doing so. This clearly is an effort to eliminate the ‘assisting with medical use’ by dispensing, delivering, or otherwise transferring to a patient argument used to attempt to justify dispensaries.
- Again the ‘valid id card’ argument is used. This may be a set up to destroy the paperwork ‘temp license’ defense later.
8

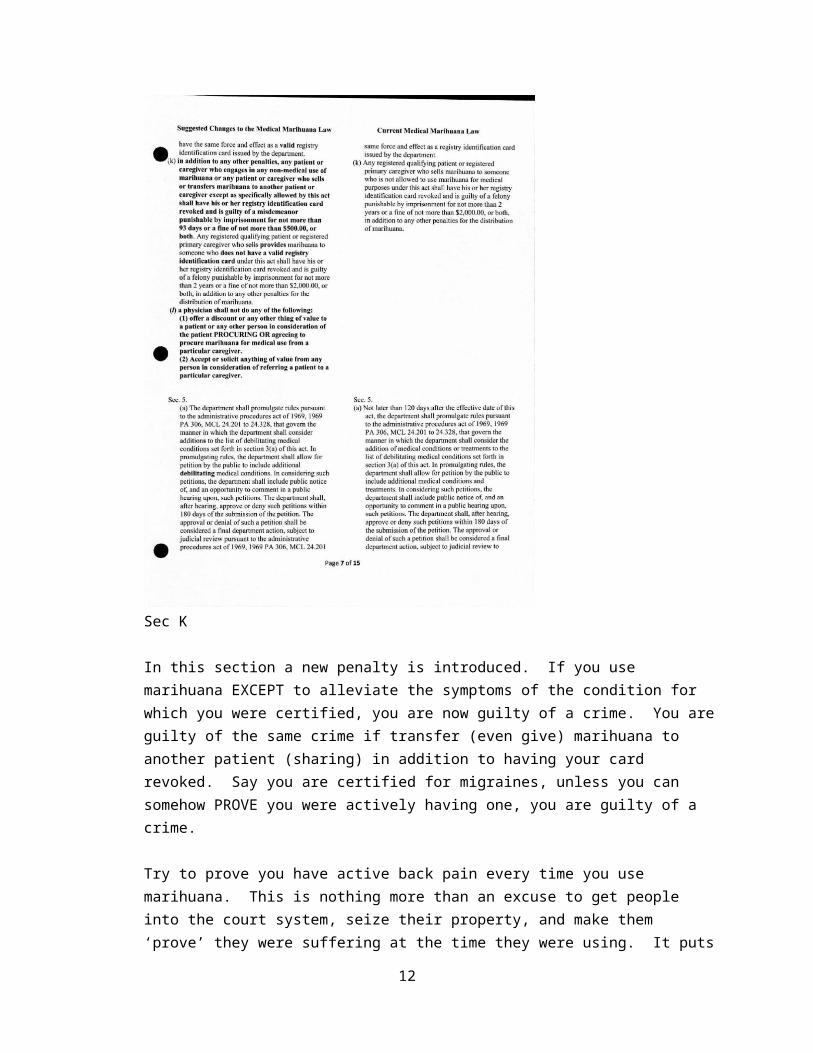
Sec K
In this section a new penalty is introduced. If you use marihuana EXCEPT to alleviate the symptoms of the condition for which you were certified, you are now guilty of a crime. You are guilty of the same crime if transfer (even give) marihuana to another patient (sharing) in addition to having your card revoked. Say you are certified for migraines, unless you can somehow PROVE you were actively having one, you are guilty of a crime.
Try to prove you have active back pain every time you use marihuana. This is nothing more than an excuse to get people into the court system, seize their property, and make them ‘prove’ they were suffering at the time they were using. It puts an excessive burden of proof on patients. Off the top of my head the only ones qualified to use marihuana would be hospice patients actively dying.
Sec L
9
This is a pretty standard prohibition used in the medical profession. Contrary to popular belief on the board, doctors are not paid or compensated for prescribing a particular medication and there are rules against it.
The sticky part may be with referrals. Can a certification clinic be held in conjunction with a compassion club that contains caregivers? Can a caregiver pay for a patient’s certification if they bring them to the clinic? Can a compassion club offer copy assistance, space to set up, or any other form of assistance?
I recall one hospital in SC when I practice down there. They got nailed by Medicare for buying physician practices at excessive prices in exchange for the doctors becoming hospital employees. Obviously this is questionable. That hospital bought the one where I was on staff. One day I was sending out preventative care reminders to about 500 patients and asked if I could use the letter folding machine. Under the terms of the settlement with Medicare they claimed they would have to figure out the depreciation and wear and tear on the machine and charge me for it, otherwise it would be viewed as compensating an admitting physician.
Though I thought it was laughable at the time and an extreme application of the ruling, it was really no big deal to me. I had my staff do it, with my help. I was NOT subject to arrest, loss of my license, my patients arrested, and their homes seized. Where is the line drawn? What is the value of a caregiver opening a door for me as I walk in a building carrying a copier? Doormen get a wage, was the caregiver offering me something of value? How about the heat/electricity/rent on the compassion club, do they need to prepare a prorated bill? If they don’t, did they compensate me? Get the idea?
Sec 5
Again, stressing debilitating conditions. Tonight I had a patient renew that no longer had the muscle spasms I certified him for last year. The MMJ had stopped them. Does that mean he no longer has the condition, or that it is under control as a direct result of the certification? By stressing debilitation, they are laying the groundwork to prosecute due to the fact the patient is not on death’s door. The tone of the entire Act is being changed to restrict access, tighten qualifications, and otherwise gut the intent of the initiative.
Recall that the standard is liberal interpretation of the common meaning of the initiative. By harshening the tone, making it criminal behavior that is being allowed to slide rather than compassionate use and patient centric, they are changing the meaning to the point it moves away from the will of the voters and toward the will of the AG.
10

Sec B
Expands the department’s authority to write rules related to medical the marihuana program. Why is this change made? What further rules and regulations require this change?
Sec 6
The three major changes in this section require participation in the registry as previously discussed, and homeless people must identify where they ‘live’ to a greater degree. The final change, which is new to the revision, is that the growing patient or caregiver must not only identify their address as before, but specifically must identify the location of the grow facility.
The concern here is that by requiring the location of the grow, it dovetails into earlier sections of the revision. Marihuana is illegal in Michigan, but the MMMA prevents the enforcement of the prohibition for the ‘vast majority’ of patients, but not all apparently. It remains illegal under
11
federal law, and federal law can be used by local authorities to prosecute caregivers and patients in possession of marihuana. That is easier if the grows are registered. Currently the Act gives some privacy on these locations, the AG wishes to end that to exercise tighter control.
As an extension of this the AG added language to require the registration of the location where the usable marihuana is kept. To comply with this section, a locked medication chest at the registered address must be used. To medicate, a patient will have to go to this specific location. Taking a supply of medication on vacation, or to a friend’s house and medicating there would violate the registration requirement- the medication is not at the registered address. This section is put in to aid prosecution- ‘your medication was not at the address you registered, therefore you violated the Act and are not entitled to the protections of the Act’.
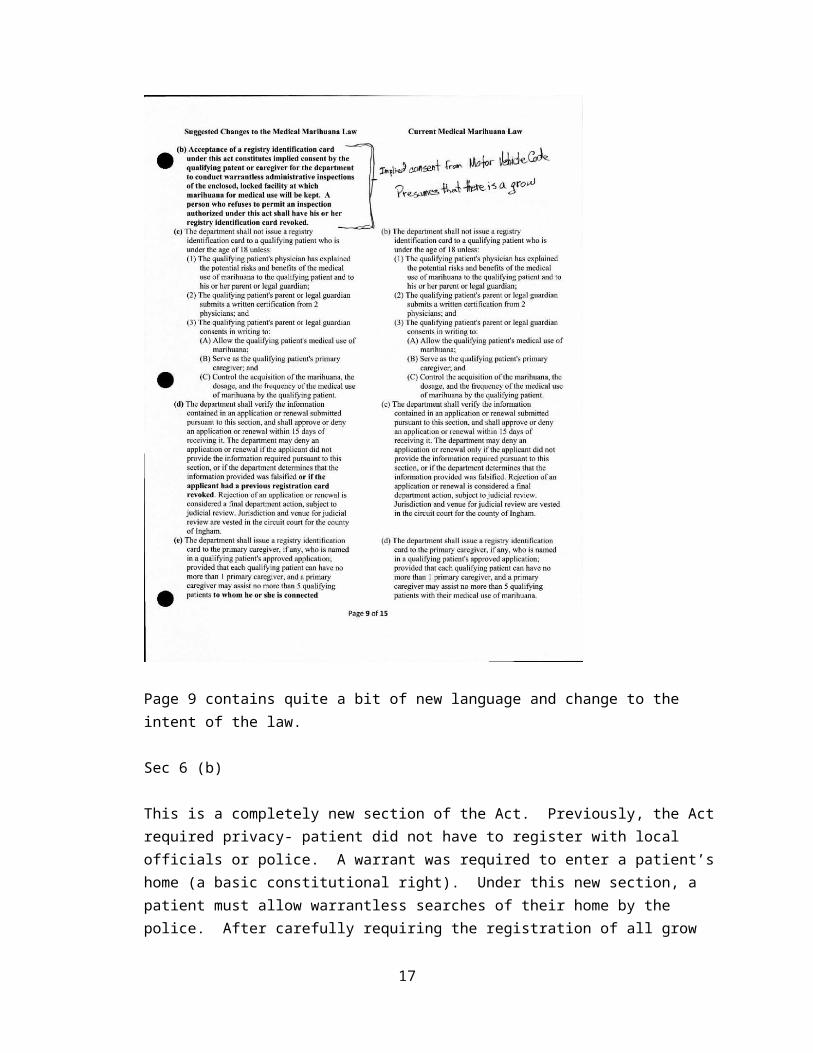
Page 9 contains quite a bit of new language and change to the intent of the law.
12

Sec 6 (b)
This is a completely new section of the Act. Previously, the Act required privacy- patient did not have to register with local officials or police. A warrant was required to enter a patient’s home (a basic constitutional right). Under this new section, a patient must allow warrantless searches of their home by the police. After carefully requiring the registration of all grow facilities, medication storage locations, and patients even to the point of park bench a homeless person sleeps on, now simply having a card gives the police the right by law to swoop in at any time for unannounced and warrantless ‘inspections’. This is very troubling. Failure to comply and allow police into the home results in revocation of the card, which leaves the patient defenseless to a criminal charge of possession and manufacturing. As the location of the grow and medication is registered, the police would have no problem getting a warrant to investigate the now ‘criminal’ activity and arrest the patient/caregiver.
Another troubling aspect of this section is that the entire revision of the Act was based on changing the premise of the voter initiative. It is taken from a compassionate act acknowledging the medical qualities of marihuana to ease the suffering of patients to a focus on the criminal activity of using marihuana and limited protection for the ‘majority’ of patients under state law. Federal law is still available for local authorities to bypass the limited protections offered by the Act, and patients are forced to aid their own prosecution by giving the location of their ‘criminal’ activity and allowing the police the ability to swoop in and arrest them with warrantless searches. This clearly violates the 5th amendment to the constitution and is just wrong and un-American.
Note that in the original Act, section 6 (g) specifically states that mere possession of a registry card is NOT probable cause for a search or inspection by law enforcement or local officials. A warrant is specifically required to protect the privacy and constitutional rights of patients. This entire protection is thrown out in the revision suggested by the AG, the man the people of Michigan elected to protect their rights. Patients are presumed criminals and must give up their basic constitutional rights. Their homes are no longer their castles and they are a subclass of citizen with limited rights.
Sec 6 (d)
Get your card revoked for any reason; including refusing a warrantless search by the police, you can’t get another one. In order to participate in the program, patients must toe the line and give up basic constitutional rights. If they refuse or protest, they cannot participate in the program. Recall that vague language about allowing the department to come up with ‘rules’ to regulate other aspects of the Act- more reasons to revoke cards?
13

America was built on the concept of protest against injustice. Unless you are a grandma with cancer that is.
Sec 6 (e)
Again caregivers and patients must be connected through the registry.
The attack on patient privacy continues with page 10
Sec 6 (f)
Within 48 hours of the card being issued to the patient (before it even arrives in the mail) the state police are notified of the location of a patient. As the department does not issue cards in a timely manner, the current Act ‘presumes approval’ if the department does not act on the application within 20 days, and patients can use their paperwork and cashed check as a temporary license.
14

Recall all the talk in the revised Act about ‘possession’ of a valid registry card. This section gives the state police the location of a marihuana patient and a marihuana grow before the patient has his/her card in hand. A warrantless search is conducted, patients are asked to produce their card or be subject to arrest. Plants are destroyed, medication seized. As the patient was not in possession of a valid card at the time of the ‘inspection’ they are not entitled to the protection of the Act.
The section goes on to state that the registry card must include the patient’s name, home address, location of their medicine, and location of their grow. How about adding their social security number, bank accounts and security system codes? Not only is this far too much information available to the police, what if the card is lost and falls into criminal hands? This will not improve public safety; it is an invitation to a home invasion robbery.
15

Page 11, the assault on rights continues….
(3) Under the current Act, the department is required to verify to law enforcement, upon request and accompanied by a registry identification number, the minimal amount of information needed to confirm a patient is a valid patient.
The revision expands this duty and those allowed access to the information exponentially. No longer is a registry number required, merely a name and date of birth or address. Anyone with access to the LIENs system (to include federal authorities who are free to prosecute anyone for marihuana) can now access the registry. Note the emphasis on the addition of ‘pursuant to state or FEDERAL law’.
So not only can state officials do unwarranted searches of homes, the federal authorities can, with the push of a button, get the name of any medical marihuana patient, caregiver, and grow facility in the state. If only other classes of criminals would make their own apprehension and prosecution so easy. Add access to the public by county and you have the sex offender registry.
16
Page 12
Sec J (6) is added to the department’s reporting guidelines. In addition to the expected statistics on the program, the department must now research the world scientific literature on the medical use of marihuana. Their annual report just went for a single sheet of paper to literally THOUSANDS of pages of medical research that will take hundreds of hours of state employee time to collect.
This is outright absurd. It is NOT the duty of the state licensure board to analyze medical research. As a certification physician, I can testify personally that I have had discussions with the department over application forms. If a condition box is not checked, the application is rejected even though the qualifying condition is CLEARLY listed in the remarks section on the physician certification. Can these same employees be charged with the analysis of the endocannabinoid system? Or is this just an excuse to present the latest DEA position on why marihuana deserves to be a schedule 1 narcotic?
Sec K and L
Any violation of the rules, direct or indirect, will result in the revocation of a patient’s registry card and that of their caregiver. There is some due process allowed. The police will immediately be notified of the revocation and location of the patient, their medication, their caregiver and their grow for immediate law enforcement action up to and including seizure of their assets under the forfeiture laws.
17
Starting at the top of page 13
- Medical use of marihuana is no longer allowed on college or university property.
Sec 4 concerning the operation of motor vehicles (and boats, airplanes, etc)- Under the original Act, operation of motor vehicles while impaired due to marihuana was not
allowed. - Under the revision, any use of marihuana, including the presence of any measurable amount of
marihuana in the body, prohibits the operation of a motor vehicle of any kind. This is very concerning as marihuana and byproducts remain in a patient’s body for up to 60 days. This will essentially preclude any medical marihuana patient from driving a car. It will pave the way for prosecutions for ‘impaired driving’ based on possession of a marihuana registry card.
- Currently if a police officer even sees a card while you are getting your license out of your wallet, you are going to have a blood sample taken. That is under the current system that says mere possession of a card cannot be used as probable cause to issue a warrant. The revised section further expands the ability of the police to prosecute marihuana patients for impaired driving.
- As there is no data suggesting a ‘safe’ or ‘impaired’ level of thc in the blood, as there is for alcohol. As a result, the AG is suggesting a zero tolerance protocol, without the need to demonstrate physical impairment.
18

Sec 6
Local communities can simply zone out all use of marihuana if they wish. A patient’s ability to use marihuana is not restricted, but their access to it is gone. No dispensaries, farmers markets, caregivers, or self grows if the local zoning board so decides.
Originally marihuana was controlled and essentially outlawed because in order to produce it you needed a tax stamp. You were not allowed to cross state lines with marihuana and in order to get the stamp, you had to bring the actual marihuana to Washington DC. In order to get it there, you had to cross state lines from anywhere in the country, thus violating the law. Zoning out the cultivation of marihuana accomplishes the same thing, which is why this provision is added by the AG.
Sec (c)
No insurance compensation for the medical use of marihuana at any level or from any source of healthcare money.
Again, the original Act called for no accommodation of employees UNDER THE INFLUENCE of marihuana. The revision calls for no accommodation for the USE of marihuana. Essentially, if you are a medical marihuana patient, you not only are not allowed to drive, you are not allowed to work. Additional changes expand the provision from ‘employees’ to ‘persons’. Now even private contractors working out of their own homes can be discharged or refuse employment.
19

Page 14 deals mostly with Sec 8. This is the medical affirmative defense. There are no suggested changes from the AG. It appears they are leaving it as written in the original Act. There are no changes because the courts have ruled that ANY failure to strictly comply with ANY provision of the Act results in the inability of the patient to use the defense in front of the jury. As Michael Komorn, attorney and director of the MMMA has noted, in our court system anyone is allowed to present a defense, even if it flies in the facts of the case. It is a basic right of our legal system, unless you are a MMJ patient.
20

Sec 9
The current Act has a ‘fish or cut bait’ provision. The department MUST reject a registry application within 15 days of receipt. They MUST issue a registry card to a patient within 20 days if they are not rejected. If the department fails to issue the card, the registry application is presumed approved and a copy of the application accompanied by proof the department has had the application for the required 20 days is considered a temporary license.
Currently the department is at least 6 months behind issuing cards. They are doing nothing to suggest this will change at any time in the future, until they are forced to do so by the courts.
21

Under the suggested revision of the Act, this situation changes dramatically.
- The provision that the application and proof of department possession for 20 days remains and the paperwork/copy of cashed check is considered a temporary license.
- The copy of the application/cancelled check temporary license is temporary. It expires in 120 days.
- If the department fails to issue the card within 140 days (quite common, current wait is 180-200 days+), the patient NO LONGER is legal, even though they have been for 120 days.
- The department may reject a patient at any time during the 140 days, and the patient is automatically revoked at 140 days until the department gets around to issuing the actual card.
This is a very significant change and will severely affect patients for many reasons….
- A patient becomes legal at 21 days after the department receives the application and plants a crop of marihuana as a legal patient. At 140 days, they are no longer legal, and must destroy all their plants and medical supplies.
- If the department decides to reject the application while the patient is growing at any time during the first 120 days the patient is legal (day 21 to day 140), the patient must destroy all plants and medication.
- The state police are notified of the name, medication location, grow location and caregiver of the patient when the department rejects them, while the patient unknowingly continues to grow assuming under the law they are legal. Remember the warrantless ‘inspections’?
- Caregivers, who are smart enough to figure out the last point, will not grow for a patient until they have a card in hand to avoid the chance of being ‘inspected’ and arrested for growing for a rejected patient.
- The department not only is not getting the cards out in 20 days, they are not getting them out in 140 days. It is now the end of November and they are working on cards from early June.
Conclusion:
1. The entire Act is changed from one calling for the compassionate use of marihuana by medical patients as enacted by the people of Michigan to limited tolerance of criminal activity.
2. Patients are criminalized3. Local law enforcement is given the ability to completely bypass the Act by citing federal law.4. Local communities can eliminate the use of marihuana by patients simply by zoning out the
cultivation at a community level.5. The registry is converted to an investigative tool with:
a. Mandatory participation in the registryb. Registration of patients, medication, and grow operationsc. Local enforcement of federal lawd. Warrantless searches of homes and grow facilities
6. The medical basis of the Act as enacted by the voters is watered down, going from a firm statement by the voters that marihuana has medical use to a ‘suggestion’ that ‘some
22

components’ MIGHT have some medical benefits. This is designed to attack the very premise the Act is based on for later challenge.
7. The entire medical tone of the revision is designed to put a chilling effect on certificationsa. New conditions may only be added based on previously approved conditions.b. Physicians are directly threatened with licensure and possibly criminal prosecution. As a
result, few if any will participate in the program, resulting in decreased access to certification at increased cost to the patients.
c. Notification of primary care physicians is required; otherwise the certification is permanently revoked. There is NO protection for the patient against inappropriate discontinuation of pain medication or discharge from the primary care practice once they obtain a MMJ card. Both these practices are common.
d. There is no protection for primary care doctors from being prevented from participation in the program in the first place. It is common for hospital systems to bar their staff physicians from writing certifications. This can result in licensure action against the physician if they write certifications- suspensions or other actions by hospitals have to be reported to the National Practitioner Database. What physician would be willing to risk that?
8. The entire tone of the revision is to control and prosecute medical marihuana patients under both state and federal law. The Act was designed and approved by the People of Michigan to shield patients from prosecution for their medical use of marihuana. This revision is designed specifically to trip patients up, after they have been identified and located, to ease their prosecution.
9. Basic functions and rights are denied to patients:a. They are not allowed to driveb. They are not allowed to workc. They are denied insurance coverage for their treatmentd. They must open their homes and businesses to warrantless searchese. They have no medical privacy and risk loss of their healthcare and medication
10. The ability to use medical marijuana is no longer offered as an alternative to more traditional therapy, it is reduced to a treatment of last resort, after all others have failed, in the terminal stages of the condition.
a. Patients must ‘prove’ they are actively suffering at the time of their useb. Patients must ‘prove’ they are suffering ‘enough’ to deserve to have a card.
i. This proof must stand up to non-medical reviewii. Physicians may not exercise judgment in their therapy decisions
c. The proposed revision in no way promotes access to medication, certification, or supports patients in any way. It is designed from start to finish to restrict, prosecute and deny access in direct violation of the language and intent of the initiative approved by over 63% of Michigan voters and reaffirmed repeatedly both on the state and national level. Most recently in Kalamazoo, where 65% of the voters passed a charter amendment to make the prosecution of small amount marihuana the lowest law enforcement priority.
23


















