Medial Capsule Knee - Update - AHN · Medial Capsule Knee - Update 04.07.17 David Crane MD ......
19
04/27/2017 1 Medial Capsule Knee - Update 04.07.17 David Crane MD Declarations Consultant for Arthrex Discussing off-label use of technology Balloon, Boing-Boing, Bioreactor I. Static and Dynamic Stabilization of the Joint Capsule and Supporting Ligament, Tendon, and Myofascial structures. II. Mechanotransduction of the Articular cartilage and Meniscus III. Nutrition, Lubrication, and Regeneration Function of the Synovium and Peri-articular vasculature and Surrounding Marrow.
Transcript of Medial Capsule Knee - Update - AHN · Medial Capsule Knee - Update 04.07.17 David Crane MD ......

04/27/2017
1
Medial Capsule Knee -
Update04.07.17
David Crane MD
Declarations Consultant for Arthrex
Discussing off-label use of technology
Balloon, Boing-Boing, Bioreactor I. Static and Dynamic Stabilization of the Joint Capsule and
Supporting Ligament, Tendon, and Myofascial structures.
II. Mechanotransduction of the Articular cartilage and
Meniscus
III. Nutrition, Lubrication, and Regeneration Function of the
Synovium and Peri-articular vasculature and Surrounding
Marrow.

04/27/2017
2
Scope of the problem
Meniscal injuries may be the most common knee
injury. The prevalence of acute meniscal tears is 61
cases per 100,000 persons.
The overall male-to-female incidence is
approximately 2.5:1.
Peak incidence of meniscal injury for males is in
those aged 31-40 years. For females, the peak
incidence is in those aged 11-20 years.
Bin SI, Kim JM, Shin SJ. Radial tears of the posterior horn of the medial meniscus. Arthroscopy. 2004
Apr. 20(4):373-8.
Arendt EA, ed. Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, Ill: American Academy of
Orthopaedic Surgeons; 1999.
Scope of the problem
In patients older than 65 years, the rate of
degenerative meniscal tears is 60%.
Root tears are observed in 28% of medial meniscal
tears.
Surgical procedures of the meniscus are performed
on an estimated 850,000 patients each year.
Bin SI, Kim JM, Shin SJ. Radial tears of the posterior horn of the medial meniscus. Arthroscopy. 2004
Apr. 20(4):373-8.
Arendt EA, ed. Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, Ill: American Academy of
Orthopaedic Surgeons; 1999.
Meniscus Anatomy
The microanatomy of the meniscus is dense
fibrocartilage composed of cells and an extracellular
matrix of collagen fibers in network. The cells are
termed fibrochondrocytes because they appear to be
a mixture of fibroblasts and chondrocytes. These
cells are responsible for the synthesis and
maintenance of the extracellular fibrocartilaginous
matrix.
Rodkey WG. Basic biology of the meniscus and response to injury. Instr Course Lect.
2000. 49:189-93.
Fu FH, Harner CD, Vince KG, eds. Knee Surgery. Philadelphia, Pa: Lippincott Williams &
Wilkins; 1994.

04/27/2017
3
Meniscus Anatomy The most abundant component of the menisci is
collagen (75%)—mainly type I collagen (>90%) but it
also contains types II, III, V, and VI. Collagen fibers
are arranged mostly along a longitudinal or
circumferential direction, with some interwoven radial
and oblique fibers. The circumferential fibers are
related directly to the menisci's functional ability to
dissipate compressive loads. The other fibers act
primarily as ties to enhance structural rigidity and to
help prevent longitudinal splitting. The extracellular
matrix also includes proteoglycans, glycoproteins,
and elastin.
Rodkey WG. Basic biology of the meniscus and response to injury. Instr Course Lect.
2000. 49:189-93.
Fu FH, Harner CD, Vince KG, eds. Knee Surgery. Philadelphia, Pa: Lippincott Williams &
Wilkins; 1994.
Meniscus Anatomy
Arnoczky and Warren demonstrated the important
vascular anatomy of the menisci. The limited
peripheral blood supply originates from the medial
and lateral inferior and superior geniculate arteries.
Branches from these vessels give rise to a
perimeniscal capillary plexus within the synovium
and joint capsule, which, in turn, supplies the
meniscus periphery.
Arnoczky SP, Warren RF. The microvasculature of the meniscus and its response to injury. An
experimental study in the dog. Am J Sports Med. 1983 May-Jun. 11(3):131-41.
Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med. 1982
Mar-Apr. 10(2):90-5.
Meniscus Anatomy
Studies have shown that 10-30% of the periphery of
the medial meniscus and 10-25% of the lateral
meniscus receives a vascular supply
the remainder receives its nutrition from the synovial
fluid from passive diffusion and mechanical pumping.
A few terminal branches of these vessels, along with
the middle geniculate artery through the synovial
covering of the anterior and posterior horn
attachments, supply increased vascularity to the
meniscal horns
Arnoczky SP, Warren RF. The microvasculature of the meniscus and its response to injury. An
experimental study in the dog. Am J Sports Med. 1983 May-Jun. 11(3):131-41.
Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med. 1982
Mar-Apr. 10(2):90-5.

04/27/2017
4
Meniscus Anatomy important functions, which include load bearing, load
and force distribution, joint stability, joint lubrication,
and proprioception.
One of the primary functions is to provide load
bearing across the knee joint.
Fifty percent of the compressive load in the knee is
transferred by the menisci in extension, whereas up
to 85% of the load is transferred at 90° of flexion. The
collagen orientation makes this load bearing possible
by converting the compressive forces to tensile
forces.
Insall JN, Scott WN, eds. Surgery of the Knee. 3rd ed. Philadelphia, Pa: WB Saunders Co; 2001.
Rodkey WG. Basic biology of the meniscus and response to injury. Instr Course Lect. 2000. 49:189-93.
Vaziri A, Nayeb-Hashemi H, Singh A, Tafti BA. Influence of meniscectomy and meniscus replacement on the
stress distribution in human knee joint. Ann Biomed Eng. 2008 May 22. epub ahead of print.
Meniscus Anatomy
Load and forces are distributed across a much larger
surface area because of the menisci, which:
(1) decrease focal contact pressure by increasing the
contact area
(2) protect the underlying articular cartilage.
Resection of 15-34% of a meniscus may increase
contact pressure by more than 350%. Normal knees
have 20% better shock-absorbing capacity than
meniscectomized knees.
Insall JN, Scott WN, eds. Surgery of the Knee. 3rd ed. Philadelphia, Pa: WB Saunders Co; 2001.
Rodkey WG. Basic biology of the meniscus and response to injury. Instr Course Lect. 2000. 49:189-93.
Vaziri A, Nayeb-Hashemi H, Singh A, Tafti BA. Influence of meniscectomy and meniscus replacement on the
stress distribution in human knee joint. Ann Biomed Eng. 2008 May 22. epub ahead of print.
Scope of the problem
Osteoartritis
Most common form of arthritis.
Classified as: Idiopathic (localized or generalized) or
Secondary (traumatic, congenital,
metabolic/endocrine/neuropathic and other medical
causes).
Characterized by focal and progressive loss of the
hyaline cartilage of joints, underlying bony changes.
04/27/2017
5
Scope of the problem
Osteoartritis
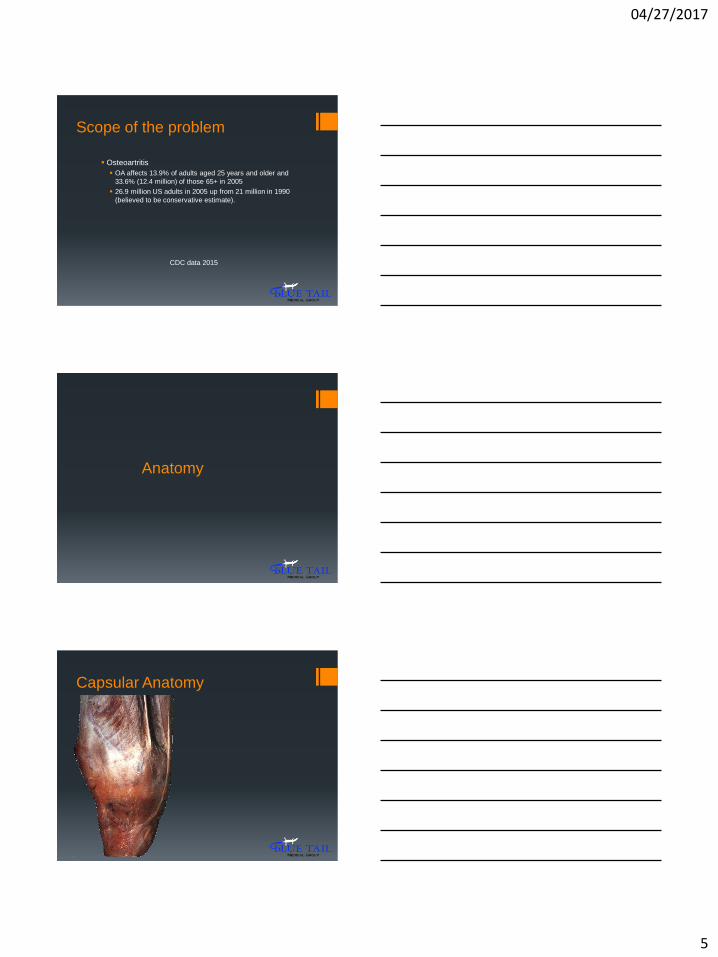
OA affects 13.9% of adults aged 25 years and older and
33.6% (12.4 million) of those 65+ in 2005
26.9 million US adults in 2005 up from 21 million in 1990
(believed to be conservative estimate).
CDC data 2015
Anatomy
Capsular Anatomy

04/27/2017
6
Capsular Anatomy
Capsular Anatomy
Three layers of the
medial capsule:
I. Crural fascia
II. Superficial portion
of the MCL
III. Deep portion of
the MCL including
the
meniscofemoral
and meniscotibial
extensions of the
deep MCL.

04/27/2017
7
Capsular Anatomy
Coronal proton-density-weighted
MR image (3,000/15) obtained
along the middle third of the
medial knee joint shows the fascia
(layer 1 [I], arrowheads) and the
sartorius (straight arrow), gracilis
(gr), and semitendinosus (st)
tendons. Note the superficial
portion of the MCL (layer 2 [II],
curved arrows).
Note the area where a split (S)
occurs in layer 2. Both the vertical
(V) and oblique (O) portions of the
MCL are shown.
Transverse section of the
medial joint capsule above
the level of the joint line:
Layers I and II are fused
anteriorly
Layers II and III are fused
posteriorly

04/27/2017
8
Cadaver Study

04/27/2017
9

04/27/2017
10
Instron Data 19% increase in meniscal extrusion can be expected from
baseline to lesion conditions
13% decrease is expected between lesion and repair
There was a 6% difference between baseline and repaired
values
Clinical Cases 8 Patients to date
2 had failed to improve w prior arthroscopic partial medial
meniscectomy > 9 mos prior
All had pain > 1 year
Case 1

04/27/2017
11

04/27/2017
12

04/27/2017
13

04/27/2017
14
Case 2

04/27/2017
15

04/27/2017
16

04/27/2017
17
04/27/2017
18
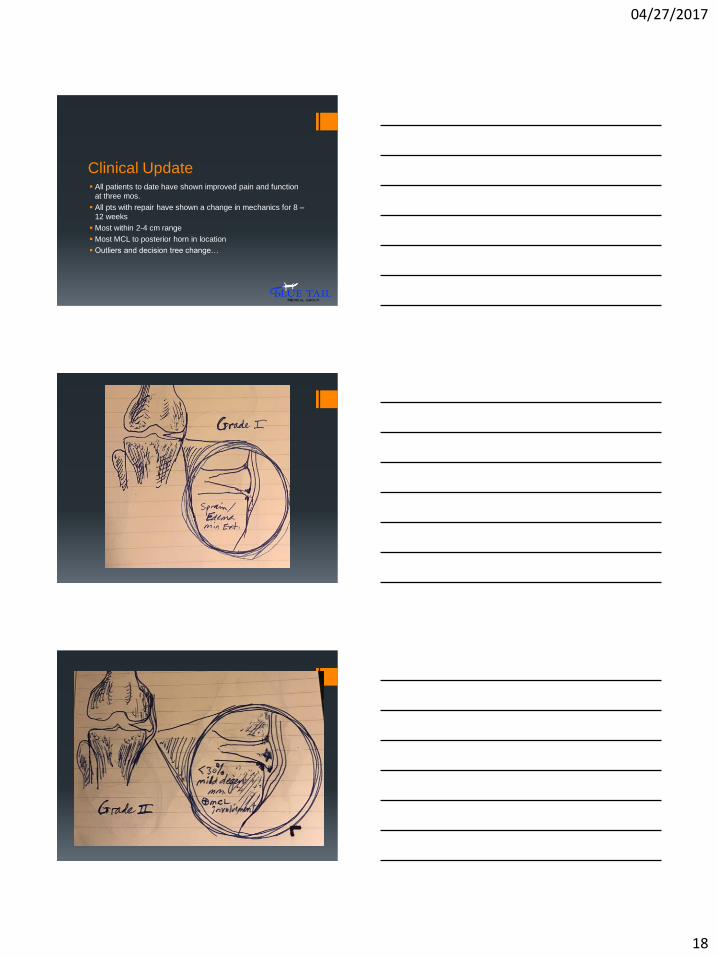
Clinical Update All patients to date have shown improved pain and function
at three mos.
All pts with repair have shown a change in mechanics for 8 –
12 weeks
Most within 2-4 cm range
Most MCL to posterior horn in location
Outliers and decision tree change…

04/27/2017
19