Mechanisms and management of TAVR-related complications
12
NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 685 Department of Cardiology, Bichat Hospital, University Paris VII, 46 Rue Henri- Huchard, 75018 Paris, France (A.‑A. Fassa, D. Himbert, A. Vahanian). Correspondence to: A. Vahanian alec.vahanian@ bch.aphp.fr Mechanisms and management of TAVR‑related complications Amir-Ali Fassa, Dominique Himbert and Alec Vahanian Abstract | Patients with severe aortic stenosis who are at high surgical risk or not considered to be suitable candidates for surgical aortic valve replacement are increasingly being treated with transcatheter aortic valve replacement (TAVR). Although this novel treatment modality has been proven to be effective in this patient population, serious complications oc cur in approximately one-third of patients during the month after the procedure. Such events include myocardial infarction, cerebrovascular events, vascular complications, bleeding, acute kidney injury, valve regurgitation, valve malpositioning, coronary obstruction, and conduction disturbances and arrhythmias, which can all lead to death. Prevention of these complications should be based on patient screening and selection by a dedicated ‘heart team’ and the use of multimodality imaging. Anticipation and early recognition of these complications, followed by prompt management using a wide range of percutaneous or surgical rescue interventions, is vital to patient outcome. Continuous patient assessment and reporting of complications according to standardized definitions, in addition to growing operator experience and upcoming technological refinements, will hopefully reduce the future rate of complications related to this procedure. Fassa, A.-A. et al. Nat. Rev. Cardiol. 10, 685–695 (2013); published online 8 October 2013; corrected online 6 November 2013; doi:10.1038/nrcardio.2013.156 Introduction Since the first transcatheter implantation of an aortic valve in 2002, transcatheter aortic valve replacement (TAVR) has emerged as an alternative to surgical aortic valve replace- ment for patients deemed at high or prohibitive risk for surgery. 1–4 Outcomes have improved over the years, mainly as a result of appropriate patient selection, growing opera- tor experience, and major technical refinements. However, the rate of complications related to TAVR remains substan- tial. 5 Anticipating complications, as well as their prompt detection and management, is important to limiting the potential consequences of these adverse events. The evaluation of TAVR-related complications has greatly benefited from the standardized definitions of outcomes developed and published by the Valve Academic Research Consortium (VARC). 6,7 In a meta- analysis by Généreux and colleagues, pooling results from studies in which the VARC criteria were used, the 30-day safety end point (composite of all-cause mortal- ity, major stroke, life-threatening bleeding, stage 3 acute kidney injury [AKI], periprocedural myocardial infarc- tion [MI], major vascular complications, and repeat procedure for valve-related dysfunction) occurred in 33% of 1,286 patients undergoing TAVR. 5 This result should probably be interpreted with caution, however, as a degree of overlap between the various complica- tions might have been present (for example, a patient with a major vascular complication might also have experienced life-threatening bleeding and AKI). In this Review, we describe TAVR-related complica- tions (Box 1), the mechanisms that cause these events, and methods of preventing them. Of note, new cardiac conduction abnormalities that occur after TAVR have previously been described in the journal, 8 and will not be covered in this Review. Complications Comprehensive screening of patients by the ‘heart team’ before TAVR is important for the prevention and management of all TAVR-related complications. 9 Such a team should include cardiologists, cardiac surgeons, imaging specialists, anaesthesiologists with experience in valve disease, and other specialists such as geriatri- cians. Furthermore, appropriate training of members of this team in the techniques and materials required for bail-out procedures is also crucial. Moreover, immediate availability of surgical backup is essential. Indeed, many TAVR-related complications require cardiopulmonary bypass while salvage management measures are put in place, including surgical interventions such as urgent aortic valve replacement, repair of myocardial or vascular injury, or pericardial drainage. 10 Death In their report, the VARC representatives recommend the use of all-cause mortality as a primary end point Competing interests D. Himbert declares associations with the following companies: Edwards Lifesciences and Medtronic. A. Vahanian declares associations with the following companies: Abbott, Edwards Lifesciences, Medtronic, and Valtech Cardio. See the article online for full details of the relationships. A.-A. Fassa declares no competing interests. REVIEWS © 2013 Macmillan Publishers Limited. All rights reserved
Transcript of Mechanisms and management of TAVR-related complications

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 685
Department of Cardiology, Bichat Hospital, University Paris VII, 46 Rue Henri-Huchard, 75018 Paris, France (A.‑A. Fassa, D. Himbert, A. Vahanian).
Correspondence to: A. Vahanian alec.vahanian@ bch.aphp.fr
Mechanisms and management of TAVR‑related complicationsAmir-Ali Fassa, Dominique Himbert and Alec Vahanian
Abstract | Patients with severe aortic stenosis who are at high surgical risk or not considered to be suitable candidates for surgical aortic valve replacement are increasingly being treated with transcatheter aortic valve replacement (TAVR). Although this novel treatment modality has been proven to be effective in this patient population, serious complications oc cur in approximately one-third of patients during the month after the procedure. Such events include myocardial infarction, cerebrovascular events, vascular complications, bleeding, acute kidney injury, valve regurgitation, valve malpositioning, coronary obstruction, and conduction disturbances and arrhythmias, which can all lead to death. Prevention of these complications should be based on patient screening and selection by a dedicated ‘heart team’ and the use of multimodality imaging. Anticipation and early recognition of these complications, followed by prompt management using a wide range of percutaneous or surgical rescue interventions, is vital to patient outcome. Continuous patient assessment and reporting of complications according to standardized definitions, in addition to growing operator experience and upcoming technological refinements, will hopefully reduce the future rate of complications related to this procedure.
Fassa, A.-A. et al. Nat. Rev. Cardiol. 10, 685–695 (2013); published online 8 October 2013; corrected online 6 November 2013; doi:10.1038/nrcardio.2013.156
IntroductionSince the first transcatheter implantation of an aortic valve in 2002, transcatheter aortic valve replacement (TAVR) has emerged as an alternative to surgical aortic valve replace-ment for patients deemed at high or prohibitive risk for surgery.1–4 Outcomes have improved over the years, mainly as a result of appropriate patient selection, growing opera-tor experience, and major technical refinements. However, the rate of complications related to TAVR remains substan-tial.5 Anticipating complications, as well as their prompt detection and management, is important to limiting the potential consequences of these adverse events.
The evaluation of TAVR-related complications has greatly benefited from the standardized definitions of outcomes developed and published by the Valve Academic Research Consortium (VARC).6,7 In a meta-analysis by Généreux and colleagues, pooling results from studies in which the VARC criteria were used, the 30-day safety end point (composite of all-cause mortal-ity, major stroke, life-threatening bleeding, stage 3 acute kidney injury [AKI], periprocedural myocardial infarc-tion [MI], major vascular complications, and repeat procedure for valve-related dysfunction) occurred in 33% of 1,286 patients undergoing TAVR.5 This result should probably be interpreted with caution, however,
as a degree of overlap between the various complica-tions might have been present (for example, a patient with a major vascular complication might also have e xperienced life-threatening bleeding and AKI).
In this Review, we describe TAVR-related complica-tions (Box 1), the mechanisms that cause these events, and methods of preventing them. Of note, new cardiac conduction abnormalities that occur after TAVR have previously been described in the journal,8 and will not be covered in this Review.
ComplicationsComprehensive screening of patients by the ‘heart team’ before TAVR is important for the prevention and management of all TAVR-related complications.9 Such a team should include cardiologists, cardiac surgeons, imaging specialists, anaesthesiologists with experience in valve disease, and other specialists such as geriatri-cians. Furthermore, appropriate training of members of this team in the techniques and materials required for bail-out procedures is also crucial. Moreover, immediate availability of surgical backup is essential. Indeed, many TAVR-related complications require cardio pulmonary bypass while salvage management measures are put in place, including surgical interventions such as urgent aortic valve replacement, repair of myocardial or v ascular injury, or pericardial drainage.10
DeathIn their report, the VARC representatives recommend the use of all-cause mortality as a primary end point
Competing interestsD. Himbert declares associations with the following companies: Edwards Lifesciences and Medtronic. A. Vahanian declares associations with the following companies: Abbott, Edwards Lifesciences, Medtronic, and Valtech Cardio. See the article online for full details of the relationships. A.-A. Fassa declares no competing interests.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

686 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrcardio
after TAVR, whereas cardiovascular mortality (death due to proximate cardiac causes or noncoronary vas-cular conditions, procedure-related death, and death of unknown cause) is considered to be an important sec-ondary end point.6 In the VARC-2 update, immediate procedural mortality is defined as death ≤72 h after the procedure, and procedural mortality as all-cause mor-tality within 30 days of the procedure or during index procedure hospitalization.7
Overall, 30-day all-cause mortality after TAVR ranges from 5% to 10%.2,3,5,11,12 Although no differences have been reported between patients undergoing implantation of the Edwards SAPIEN® valve (Edwards Lifesciences, Irvine, CA, USA) and the CoreValve® (Medtronic CV, Luxembourg), the use of the trans apical route is associated with significantly higher mortality than the trans arterial route for patients treated with the Edwards SAPIEN® (10.0% [95% CI 8.4–11.6%] versus 6.3% [95% CI 5.1–7.6%], P = 0.001), which is likely to be related, to some extent, to the increased risk profile of patients treated with the transapical approach.11 A study by Van Mieghem et al. showed that, although most deaths (75%) were of cardiac origin and occurred during the first 48 h after TAVR, a noncardiac cause was involved in 69% of deaths that occurred between 48 h and 30 days after the proce-dure.13 The most-frequent causes of non cardiac death were infection or sepsis and stroke, whereas causes of cardiac death included heart failure, cardiac t amponade, and arrhythmias.
Periprocedural myocardial infarctionIn the VARC consensus documents, periprocedural MI is defined as the presence of new ischaemic signs
Key points
■ Major complications occur in one-third of patients during the month after transcatheter aortic valve replacement (TAVR)
■ Adequate patient screening and selection, using a ‘heart team’ approach and multimodality imaging, is important for the prevention of TAVR-related complications
■ Complications should be anticipated during a multidisciplinary evaluation before TAVR, to enable prompt recognition and management should such events occur during the procedure
■ The TAVR team should always be ready to perform immediate percutaneous or surgical rescue interventions in the event of serious TAVR-related complications
■ Growing operator experience and upcoming technological refinements will reduce the incidence of TAVR-related complications in the future
(imaging evidence of new loss of viable myocardium or new wall motion abnormality, new ST-segment changes, new patho logical Q-waves in at least two con-tiguous leads, haemodynamic instability, ventricular arrhythmias, or new or worsening heart failure) or symp-toms (such as chest pain or shortness of breath), associ-ated with an elevation in cardiac biomarkers (preferably creatine kinase MB) within 72 h of the procedure.6,7 In the initial report, biomarker elevation was defined as >10-times the upper reference limit (URL), or more than five-times the URL with new Q-waves in two contiguous leads.6 These values were adjusted to 15-times the URL for troponin levels and five-times the URL for the crea-tine kinase MB level in the VARC-2 update, with the p resence of new Q-waves not being mandatory.7
Nearly all patients undergoing TAVR experience some degree of myocardial injury, as defined by any increase in troponin levels. The higher the degree of injury, the less improvement in left ventricular ejection fraction is seen during follow-up.14 When the VARC definition of periprocedural MI is used, the incidence of this compli-cation has been reported to be 1.1%.5,11 The transapical approach is associated with a higher rate of peri procedural MI than the transarterial route (1.9% versus 0.8%; P <0.05).11 Periprocedural MI is an independent pr edictor of midterm mortality (9 months to 1 year).14,15
The causes of periprocedural MI include ischae-mia related to hypotension or rapid ventricular pacing, myocardial tissue compression by prosthesis expansion, coronary microembolism, and direct trauma of the ven-tricular apex during the transapical approach.14 Reported independent predictors of myocardial injury during TAVR include baseline renal dysfunction, the presence of peripheral artery disease, the absence of preprocedural β-blocker use, the use of the transapical approach, pro-cedural duration, and prosthesis implantation depth (for the CoreValve®).14–16 Concerns have been raised about the risk of performing TAVR in patients with untreated, severe coronary artery stenoses.17 However, no evidence currently exists that such a strategy might result in a higher incidence of periprocedural MI when compared with patients who have undergone previous revasculariza-tion.18–20 Periprocedural MI due to coronary obstruction is specifically addressed in a later section of this Review.
The broad use of preprocedural β-blocker therapy in patients at high risk of periprocedural MI could result in a reduced rate of myocardial injury and subsequent adverse outcomes.15 However, such a strategy needs to be prospectively assessed. The issue of whether to perform percutaneous coronary intervention (PCI) before TAVR in patients with severe coronary artery disease, either as a staged or combined procedure, should be based on an individualized assessment, taking into account the patient’s clinical condition, their coronary anatomy, and the extent of the myocardium at risk.4
Cerebrovascular eventsCerebrovascular events, which include stroke and tran-sient ischaemic attack, are among the most-devastating complications of TAVR. Stroke in the setting of TAVR is
Box 1 | Summary of TAVR-related complications
■ Death ■ Myocardial infarction ■ Cerebrovascular events ■ Vascular events ■ Bleeding ■ Acute kidney injury ■ Transcatheter valve regurgitation ■ Valve malpositioning ■ Coronary obstruction ■ Cardiac conduction abnormalities*
*Previously described in the journal,8 and not covered in this Review. Abbreviation: TAVR, transcatheter aortic valve replacement.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 687
defined as a focal or global neurological deficit lasting >24 h resulting from a cerebral, spinal, or retinal dysfunc-tion caused by ischaemia or haemorrhage, with neuro-imaging proof of a new lesion.6 Stroke is classified as minor or major on the basis of neurological assessment using the modified Rankin score21 at 30 and 90 days. If the neurological episode lasts <24 h and neuroimag-ing does not demonstrate new haemorrhage or infarct, the event is defined as a transient ischaemic attack.
The incidence of cerebrovascular events during the 30-day period after TAVR ranges from 3% to 7%, with the majority of patients experiencing ‘major’ strokes.2,5,11,22–25 Approximately 50–70% of these events occur during, or within 24 h of, the procedure.22–24 No significant differences are apparent in the rate of stroke according to valve type or access route.11 The occurrence of stroke is associated with a 3.5-fold to 10-fold increase in 30-day mortality.23–25 Cerebrovascular events that occur during the subacute phase (from 24 h to 30 days after the procedure) have been suggested to relate to new-onset atrial fibrillation, which occurs in approximately one-third of patients undergoing TAVR with no history of atrial fibrillation.23,26
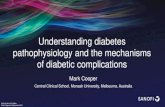
Among patients undergoing retrograde crossing of a stenotic aortic valve, 22% have been shown to develop new cerebral ischaemic lesions, as assessed by diffusion-weighted MRI (Figure 1a).27 New, but clinically silent, lesions were found in 68–91% of patients after TAVR using the same technique.28–33 However, these clinically silent lesions were not related to survival, self-sufficiency, cognitive function, or health-related quality of life during follow-up.28–30 In another study, in which transcranial Doppler ultrasonography was used during 83 TAVR procedures, high intensity transient signals indicating microembolization were detected during all interven-tions, with only two patients experiencing a procedural stroke, and no sequelae among other patients during follow-up (Figure 1b).34 These signals most commonly occurred during positioning and implantation of the valve.34 In a study on the histopathology of embolic debris captured with a filter-based embolic protection device during TAVR, most of the material originated from the native aortic valve leaflets or aortic wall.35 Thrombotic material was found in 70% of the captured debris, which included features of acute thrombi in more than half of the patients.35 Postimplantation balloon dilatation of the valve, and valve dislodgement or embolization have been reported to be independent predictors of acute stroke.23 In addition, Stortecky et al. showed that the attempt to implant more than one valve was also an independent predictor of acute cerebrovascular events, suggesting that additional catheter manipulation might result in increased embolism.24 Furthermore, in the PARTNER trial,22 small aortic area index was associated with an increased risk of early cerebrovascular events, probably owing to the high degree of calcification in tight valves.
Performing TAVR without prior aortic balloon dilata-tion has been suggested as a strategy to reduce the rate of embolic stroke.36 Although this approach has been shown to be feasible with the CoreValve®, the potential reduction
in cerebrovascular events remains to be proven.36 Limiting manipulations of large catheters in the aortic arch might also contribute to reducing the occurrence of cerebro-vascular events.37 More specifically, dedicated mechanical cerebral protection devices have been developed for pre-vention of cerebrovascular events during TAVR, and are currently under evaluation in clinical trials (Figure 2).38–40 The Claret Montage™ Dual Filter System (Claret Medical, Inc., Santa Rosa, CA, USA; Figure 2a) consists of a catheter with proximal and distal filters that are placed from a right radial or brachial approach in the brachiocephalic and left common carotid arteries, respectively. Conversely, the Shimon embolic filter™ (SMT Research and Development, Herzliya, Israel; Figure 2b) and the Embrella® embolic deflector system (Embrella Cardiovascular, Inc., Wayne, PA, USA; Figure 2c) both operate as debris deflectors. These systems are deployed in the aortic arch, protecting supra-aortic vessels from embolic debris. The improved profile of upcoming generations of delivery catheters and prostheses is likely to enable atraumatic manipula-tion and implantation of valves, possibly resulting in a reduced rate of embolic events.41 Strategies involving the use of antiplatelet and anticoagulant agents during and after TAVR also need to be assessed in order to prevent the occurrence of cerebrovascular events. Likewise, pharma-cological prevention of new-onset atrial fibrillation after TAVR with antiarrhythmic drugs should be evaluated.
Vascular eventsMajor vascular complications include thoracic aortic dis-section; distal embolization (noncerebral) from a vascular source, requiring surgery or resulting in amputation or irreversible end-organ damage; access-site or access-related injury leading to death, the need for blood trans-fusion (>4 units), unplanned percutaneous or surgical intervention, or irreversible end-organ damage. Minor vascular complications include access-site or access-related injury not requiring unplanned percutaneous or surgical intervention and not resulting in end-organ damage.6 In the VARC-2 update, rupture of the device landing zone (which includes the aortic annulus and
0.210 0.421 0.631 0.042 0.05?
a b
Figure 1 | Stroke during transcatheter aortic valve replacement. a | Diffusion-weighted magnetic resonance image showing multiple hyperintense defects (arrows) corresponding to small cerebral infarctions that were clinically silent. b | Transcranial Doppler ultrasonogram showing a high intensity transient signal (arrow) indicating microembolization.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

688 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrcardio
root, and the left ventricular outflow tract) was included among vascular complications, whereas percutane-ous closure device failure (leading to treatment other than manual compression or adjunctive endo vascular ballooning) was defined as a distinct component of vascular c omplications, separate from the minor and major categories.7
The reported rates of vascular complications vary con-siderably, mainly owing to differences in definitions.42 In the meta-analysis by Généreux and colleagues, the pooled estimated rate of all vascular complications after TAVR was 19% (major complications 12%; minor complications 10%).5 In another meta-analysis, in which studies with less-uniform definitions (published before the VARC definitions were available) were included, the overall rate of vascular complications associated with the CoreValve® was lower than with the Edwards SAPIEN® valve for transarterial implantations (11% versus 22%, respec-tively; P = 0.002).11 However, most of the studies with the Edwards SAPIEN® valve involved the use of large deliv-ery sheaths (22–24 French), whereas those in which the smaller, third-generation CoreValve® was used required an 18 French delivery system.11 The use of the newer-generation Edwards SAPIEN XT® valve, which requires 18–19 French delivery sheaths, has been associated with a significant decrease in vascular complications.43 The occurrence of vascular complications has a substantial effect on midterm survival. In the PARTNER trial,44 these complications were independent predictors of 1-year mortality (HR 2.31, 95% CI 1.20–4.43, P = 0.012).
Predictors of major vascular complications include female sex, the ratio of the sheath outer diam eter to the minimal femoral artery diameter, and the deg ree of femoral artery calcification.44,45 More importantly, TAVR has a learning curve effect, as operator and centre experience are clearly related to the rate of vascular complications.45,46
Vascular access-site complications are mainly related to the large calibre sheaths used to deliver the valve. The first generation of sheaths (22–25 French, correspond-ing to an outer diameter of 9–10 mm), was associated with high rates of vascular complications.47 However, with growing operator experience, improved patient screen-ing and selection, and the smaller diameter of newer-generation sheaths (18–19 French, corresponding to an outer diam eter of 7.2–7.5 mm), the incidence of vascular c omplication has significantly decreased over time.48
Device landing-zone rupture is a rare, but serious, complication of TAVR reported in approximately 1% of patients, and is associated with high mortality (48–50%).5,49,50 Rupture of the valve landing zone occurs after implantation of balloon-expandable valves, although this complication has also been reported following post-implantation balloon dilatation of a self-expandable valve.49,51 Independent predictors of this complication include valve oversizing (by ≥20%) and the presence of moderate or severe calcification in the left ventricular outflow tract or subannular region.50,52 Landing-zone rupture generally requires immediate haemodynamic support with inotropes and possible circulatory assis-tance. Cardiac tamponade is a common occurrence after landing-zone rupture, and is best managed with peri-cardiocentesis. Although surgical repair, with or without aortic valve replacement, is usually the only treatment for uncontained ruptures, successful conservative (medical) management of contained ruptures and haematomas has been reported (Figure 3).50
The use of percutaneous closure devices for transfem-oral procedures has increased over time, such as with the Perclose ProGlide® (Abbott Vascular Inc., Santa Clara, CA, USA) and the Prostar® XL (Abbott Vascular Inc., Redwood City, CA, USA). Success rates of up to 91% using a percutaneous approach have been reported with the Prostar® device, and even higher success rates (up to 96%) have been achieved with the decreased diameter of newer-generation delivery sheaths.48 More importantly, percutaneous device failure was not associated with major vascular complications.48 Failure of percutaneous closure devices is also related to operator experience and sheath outer diameter to minimal femoral artery diam-eter.48 In addition, percutaneous closure is particularly challenging in patients with morbid obesity. In cases of closure device failure or vessel rupture, the use of a self-expanding covered stent can often lead to an optimal result (Figure 4). As a last resort, if other approaches fail, surgical revision and closure might be required.
Preprocedural evaluation by the heart team is impor-tant to preventing vascular complications, and should involve screening by angiography and CT. Evaluation should be based on an integrative approach taking into account vessel size, calcification, and tortuosity. Femoral
a c
d e
b
Figure 2 | Embolic protection devices used during transcatheter aortic valve replacement. a | Claret Montage™ Dual Filter System. Permission obtained from Claret Medical Inc. (Santa Rosa, CA, USA). b | The Shimon embolic filter™ (SMT Research and Development Ltd, Herzliya, Israel). Reprinted from EuroIntervention Vol. 8, number 5, Bourantas, C. V. et al., Transcatheter aortic valve implantation: new developments and upcoming clinical trials. Pages 617–627 Copyright (2012), with permission from Europa Digital & Publishing.91 c | The Embrella® embolic deflector system (Embrella Cardiovascular, Inc., Wayne, PA, USA). d | Fluroscopy image showing the Embrella® device (arrow) being placed in the aorta using the right radial approach. e | Aortic angiogram showing the Embrella® device appropriately covering all the supra-aortic vessels (arrows).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 689
access should not be used in patients whose vessels exhibit severe tortuosity, are small (diameter <6 mm), or are substantially calcified. During TAVR using an arterial approach, the large delivery sheath should be advanced gently and, if resistance occurs, another approach should be considered as forceful insertion of the sheath can lead to vessel rupture or intimal strip-ping and dissection. During the closure phase, a cross-over wire should be inserted into the main vessel from the contralateral side, to allow rapid treatment with balloon inflation or covered stent p lacement in case of u ncontrolled haemorrhage.
BleedingBleeding is defined as ‘life-threatening’ or ‘disabling’ if it leads to death; occurs in a critical area, such as the central nervous system, the pericardium (requiring drainage), or in the muscle with compartment syndrome; causes shock or severe hypotension; leads to a drop of ≥5 g/dl in haemoglobin; or requires transfusion of ≥4 units of red blood cells.7 When the haemorrhage does not meet these criteria, but is associated with a drop in haemo-globin ≥3 g/dl or requires transfusion of 2–3 units of red blood cells, the bleeding is classified as ‘major’. Any other bleeding that does not fulfil these criteria, but is worth mentioning is considered to be ‘minor’.
In the meta-analysis by Généreux and colleagues, the overall incidence of bleeding was 41% (life-threatening haemorrhage 16%).5 Life-threatening bleeding is associ-ated with a sixfold to ninefold increase in 30-day mor-tality after TAVR, and was an independent predictor of 1-year mortality (HR 2.5).53,54 The transapical route has consistently been reported as an independent predictor of life-threatening bleeding.53–55
Bleeding during TAVR is caused by the combination of procedure-induced haemorrhage and patient fragil-ity in this high-risk population. Bleeding is related to access-site complications in up to 69% of patients (life-threatenin g bleeding in 23–31% of patients), including those whose procedure involved transapical access.53,54,56 Other sources of haemorrhage include the digestive tract, the retroperitoneum, and the pleura. Bleeding in the peri cardium leading to cardiac tamponade occurs in 3–4% of TAVR procedures, and is associated with high mortality (24%).5,57 Tamponade is most frequently caused by right ventricular perforation by temporary pacemaker wires; other causes include aortic annulus rupture, aortic dissection, and left ventricular perforation owing to stiff wires placed in the left ventricular cavity.57
Patient selection, mainly with regard to vascular access, is critical in reducing the incidence of life-threatenin g bleeding. Strategies such as inserting a balloon into the iliac artery via contralateral access to prevent bleeding during access closure might be beneficial. Performing TAVR without administration of clopidogrel, or replac-ing heparin with bivalirudin, have also been suggested as methods of preventing haemorrhage.53 Treatment should be focused on obtaining haemostasis at the source of the bleed (either percutaneously or surgically). In most patients with low-rate bleeding after percutaneous vessel
closure, prolonged manual compression, in addition to partial or total reversal of anticoagulation is often suffi-cient to achieve haemostasis. Crossover balloon inflation can be useful to treat persistent or uncontrolled bleeding and pseudoaneurysms. Transfusion of red blood cells can also be performed; however, a policy of restricted trans-fusion is advocated to limit deleterious consequences such as AKI.
Acute kidney injuryThe VARC definition of AKI is based on a modified version of the RIFLE (Risk, Injury, Failure, Loss, and End-stage kidney disease) classification, with incremen-tal staging from 1 to 3 on the basis of relative or absolute elevation of serum creatinine at 72 h after TAVR. Patients who require renal replacement therapy (haemodialysis, peritoneal dialysis, or haemofiltration) are considered to meet stage 3 criteria irrespective of creatinine level.6
a b
Figure 4 | Vascular events after transfemoral transcatheter aortic valve replacement. a | Angiogram showing incomplete arteriotomy closure (arrow) owing to closure device failure. b | Complete haemostasis was achieved after implantation of a covered stent (arrows).
Figure 3 | Device landing-zone rupture. 3D CT reconstruction showing a contained rupture of the aortic root after transcatheter aortic valve replacement in an asymptomatic patient who was managed conservatively (medical therapy).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

690 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrcardio
The VARC-2 update recommends the use of the AKIN (Acute Kidney Injury Network) system, and extends the timing for diagnosis of AKI to 7 days.7
The overall rate of AKI after TAVR has been reported to be 22%, whereas the incidence of stage 2 or 3 AKI was 8.4%.58 In the meta-analysis by Khatri and colleagues, 5% of all patients required renal replacement therapy, although the rate was higher in patients treated with the transapical approach to TAVR (8%) than in those whose procedure involved transarterial routes (3%).11 Several studies have shown that AKI is associated with a twofold to fivefold increase in mortality at 30 days and 1 year, when compared with patients without AKI.58
The origin of AKI is likely to be multifactorial; involv-ing predisposing conditions such as diabetes mellitus, chronic kidney disease, or peripheral vascular disease; and procedure-related events such as aortic plaque embolism in the renal arteries and hypoperfusion during rapid ventricular pacing.59 The use of the trans-apical approach has been reported to be an independent predictor of AKI in several studies, probably reflecting underlying comorbidities that predispose these patients to such a complication.58 In addition, AKI seems to be strongly related to the number of perioperative blood transfusions, which are thought to have a direct harmful effect on the kidneys.60,61
General preventive measures against AKI, such as optimal hydration, minimal contrast use, and cessation of nephrotoxic drugs should be part of the usual care for patients undergoing TAVR.59 Careful planning is essen-tial, particularly in patients at risk of AKI, to allow suf-ficient time between preprocedural investigations that require a contrast medium and the TAVR procedure. Imaging modalities that are not harmful to kidney func-tion because they do not involve a contrast agent, such as MRI, can also be used for preprocedural work-up.62 Furthermore, restricting use of blood transfusion might decrease the occurrence of AKI, but such a strategy remains to be tested in prospective studies.60
Aortic valve regurgitationAortic regurgitation (AR) is frequently encountered after TAVR, and can be either central or para valvular. Central leaks are usually related to structural dys-function of the valve, whereas paravalvular leaks are not. Assessment of AR is challenging and imprecise, and should be based on an integrative multimodality approach. Echo cardiography is limited by the shield-ing and reverb erations of the valvular frame, as well as the eccentricity of the regurgitant jets, and echo-cardiographic parameters have not been validated in the s pecific setting of TAVR.7,63–65 Aortic root angio-graphy is an established technique for the quantifica-tion of AR, and is usually performed immediately after TAVR. However, this imaging strategy relies on sub-jective assessment of unidimensional images, and can be affected by interobserver and intra observer vari-ability.5,66 Other signs that can indicate the presence of clinically relevant AR include haemodynamic param-eters, such as decreased aortic diastolic blood pressure
(DBP) associated with increased left-ventricula r end-diastolic pressure (LVEDP). Sinning et al. reported that the aortic regurgitation index—defined as [(DBP – LVEDP)/systolic blood pressure] × 100—can be useful for defining the severity of AR, with a value <25 being p redictive of increased mortality risk.67
The overall incidence of moderate or severe AR after TAVR ranges from 4.5% to 11.7%.5,11,68 In a meta-analysis by Athappan and colleagues, the CoreValve® was associ-ated with a higher rate of moderate or severe AR than the Edwards SAPIEN® valve (16.0% vs 9.1%, respectively; P = 0.005).68
Paravalvular AR after TAVR and before hospital dis-charge (including small or trace leaks) is quite common (incidence 50–85%), with the majority of cases graded as mild (grade 1).65,69 The incidence of moderate or severe (grades 3 and 4) para valvular AR before hospi-tal discharge ranges from 0% to 24%.65,69 However, the reported rate of paravalvular AR after TAVR has marked hetero geneity between studies, mainly owing to impor-tant differences in assessment of presence and severity of AR, both in terms of methodology used and independ-ent adjud ication of imaging.69 The presence of para-valvular AR grade 2 or higher after TAVR is associated with a twofold to fourfold increase in 1-year mortal-ity, compared with patients who do not have clinically relevant paravalvular AR.68–70 By contrast, more than trace (grade 1) central AR after TAVR is rare (9–29% of patients, with only 1% moderate or higher),2,12 and could be related to post implantation dilatation with an oversized balloon. In rare instances, severe trans valvular regurgitation owing to structural dysfunction of the valve resulting in a ‘frozen’ leaflet has been reported.71,72
Paravalvular AR after TAVR has three main mecha-nisms.67,68 First, suboptimal placement of the prosthe-sis, with incomplete sealing of the annulus by the skirt owing to ‘too high’ or ‘too low’ positioning of the pros-thesis. Second, incomplete apposition of the stent frame owing to calcification of the annulus, the native leaflets, or the left ventricular outflow tract (device landing zone). Third, mismatch between the size of the annulus and the size of the prosthesis owing to under-sizing of the replacement aortic valve. Correct sizing of the annulus with mild oversizing should ensure that the prosthesis is large enough to minimize paravalvu-lar AR, without excessive oversizing, which could lead to annular injury.50,52,73,74 Although echocardiography was used to determine aortic annulus size during the initial experience of TAVR, studies conducted since 2010 suggest that multidetector CT could improve the accu-racy of assessment and extent to which the results can be reproduced, potentially leading to a decrease in the incidence of paravalvular AR.73–76 Accurate prosthesis positioning requires definition of the delivery angle and guidance during implantation, using angiography, trans-oesophageal echocardiography, or dedicated real-time navigation tools.77 Technical improvements, such as the addition of sealing cuffs, in devices under development have also shown encouraging reductions in the rate of paravalvular AR.78
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 691
When clinically relevant (≥grade 2) AR is observed after valve implantation, once the regurgitation is deter-mined to be central or paravalvular (ideally using trans-oesophageal echocardiography), several interventional strategies are possible.69,70 In case of a central leak, the guidewire should be withdrawn. If moderate or severe regurgitation persists, valve-in-valve implant ation should be performed. In the presence of paravalvu-lar AR with incomplete apposition of the stent frame owing to severe calcification of the native valve, post-implantation balloon dilatation of the valve prosthe-sis can allow greater valve expansion and reduction of paravalvular AR. However, the potential beneficial effect on AR should be balanced against the increased risk of annulus rupture, and caution is required in the presence of extensive calcification of the device landing zone or shallow sinuses of Valsalva. If paravalvular AR results from suboptimal placement of the prosthesis, valve-in-valve implantation can be performed (Figure 5). In addition, in the specific case of a ‘too low’ implant-ation of a CoreValve®, a manoeuvre for snaring the frame and pulling back the valve has been described.79 Percutaneous paravalvular leak closure after TAVR has also been reported.80
Valve malpositioningValve malpositioning includes migration after initial correct positioning, in which the valve prosthesis moves up or down within the aortic annulus from its initial position with or without consequences; embolization, in which the valve prosthesis moves during or after deploy-ment such that it loses contact with the aortic annulus; and ectopic deployment, in which the valve prosthesis is permanently deployed in a location other than the aortic root.7 Although malpositioning generally occurs immediately during or after valve implantation (with diagnosis during the procedure or on the angiographic control study performed immediately after implant-ation), delayed valve migration has been reported in rare instances and has been associated with acute heart failure and cardiogenic shock.81,82
The overall incidence of valve malpositioning during TAVR is 1.3%.11 The rate has been reported to be higher with the CoreValve® (2.3%) than with the Edwards SAPIEN® valve (1.0%), although the difference was not significant.11 In the PARTNER trial,83 valve embolization occurred in 1% of TAVR procedures, with high 30-day all-cause mortality (27%). In a series of seven patients with ectopic deployment of a balloon-expandable valve at the time of implantation, six patients remained alive in NYHA class I or II heart failure at the end of the follow-up period (mean 3 years; one patient died from an un related cause).84 Similar outcomes were observed in another study after malpositioning of self-expandable valves.79
There are several possible reasons for valve mal-positioning. Spontaneous migration or embolization can occur with erroneous assessment of the annulus size and implantation of an undersized valve prosthe-sis, or incorrect positioning (too high or too low, often owing to inadequate visualization of the valve plane).83,84
For balloon-expandable valves, valve malpositioning can occur if rapid ventricular pacing is insufficient or is term inated before complete deflation of the balloon during valve implantation. Other conditions that can predispose the patient to valve malpositioning are the presence of a bulging hypertrophied interventricular septum, a mitral valve prosthesis, or severe calcification of the mitral annulus extending towards the anterior mitral leaflet and the left ventricular outflow tract.
Adequate visualization of the native aortic valve plane before prosthetic valve implantation is important in avoiding valve malpositioning, with all three sinuses of the aorta lying on a line with the long axis of the valve positioned perpendicular to this line.84 Preprocedural CT or dedicated real-time navigation tools can, there-fore, be useful to determine the correct plane.77 For balloon-expandable valves, the operator should always verify the efficiency of rapid ventricular pacing before valve implantation, and ensure that the balloon is com-pletely deflated before pacing is terminated. In addition, slow balloon inflation during implantation might also reduce malpositioning.
Treatment of a malpositioned valve depends on the type of implanted prosthesis, the site of final deploy-ment, and the potential haemodynamic consequences of malpositioning (such as paravalvular regurgita-tion or coronary occlusion). Malpositioning of self-expandabl e valves is usually treated either by pulling the valve back towards the aorta with a snare,80 or implant ation of a second valve-in-valve, which can also be performed when a balloon-expandable valve has migrated. Treatment of aortic embolization of a balloon-expandabl e valve should involve retrieval of the valve within the descending aorta using an inflated balloon placed within the prosthesis. In addition, avoiding with-drawal of the guidewire is imperative to prevent inver-sion of the valve prosthesis. Conversely, management of ventricular migration might require emergency surgical removal of the valve, although transapical extraction or balloon recapture and repositioning within the aortic valve or the aorta are also p ossible (Figure 6).31,83,85
a b
Figure 5 | Paravalvular regurgitation after transcatheter aortic valve replacement. a | Severe paravalvular aortic regurgitation with complete and dense opacification of the left ventricle during aortic angiograph owing to a ‘too low’ implantation of a 31 mm CoreValve® (Medtronic CV, Luxembourg). b | Implantation of a second valve-in-valve (CoreValve®) resulted in reduction of the regurgitation (graded as mild).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

692 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrcardio
Coronary obstructionCoronary obstruction is defined as angiographic or echo-cardiographic evidence of a new, partial, or complete obstruction of a coronary ostium during or after TAVR.7 Confirmation of coronary obstruction is usually obtained using aortography after valve implantation or, if the
diagnosis remains in doubt, by selective angiograph y of the obstructed coronary artery.
Coronary obstruction is a rare complication, with a reported incidence of 0.8%.11 The risk of this compli-cation seems to be higher (incidence 3.5%) for patients undergoing valve-in-valve procedures for the treat-ment of a degenerative bioprosthetic aortic valve.86 In a review of published cases, coronary obstruction was more common in the left main than in the right coro-nary artery (83.3% vs 12.5%).87 Mean in-hospital mortal-ity after coronary obstruction was 8.3%, which is similar to overall hospital mortality after TAVR.87 However, this rate might be an underestimate as publication bias towards cases in which patients survived is likely.
Coronary obstruction is usually caused by displace-ment of the calcified native leaflet over the coronary ostium (Figure 7).87 Although concerns about coro-nary obstruction by the structures of the valve prosthe-sis itself (such as the frame or the cuff) have been raised since the inception of TAVR, no such cases have been reported to date. A distance ≤10 mm between the coro-nary ostia and the aortic annulus has been suggested as an identifier of patients at risk of coronary occlusion.88 However, in 60% of the cases reported in a systematic review by Ribeiro and colleagues, the coronary ostia height was >10 mm.87 Therefore, other factors might be involved, such as the presence of bulky calcium nodules on the coronary leaflets or a narrow aortic root with shallow sinuses of Valsalva, which leave little room to accommodate the displaced native leaflets.87
As coronary obstruction is likely to be the result of anatomical factors, selection of patients on the basis of assessment using multidetector CT might prevent this complication. Indeed, TAVR should probably be discouraged in patients with a coronary ostia height <10–12 mm, especially if associated with the presence of bulky calcium nodules on the coronary leaflets and a narrow aortic root (<27–28 mm) with shallow sinuses of Valsalva. In borderline patients, aortic root angiography during balloon aortic valvuloplasty can predict the risk of coronary obstruction by visualization of the displace-ment of the native aortic leaflet and the flow in the coro-nary artery.89 If the risk of coronary artery obstruction is substantial and surgical valve replacement is absolutely contraindicated, one option is to establish an additional arterial access route and to place one or more protection 0.014 inch guidewires in the coronary artery through a guiding catheter, which will be pulled back into the ascending aorta before valve implantation.90 This s trategy allows rapid intervention if PCI is required.
Confirmation of coronary obstruction requires prompt treatment owing to the high risk of haemo-dynamic collapse. Emergency PCI should be attempted immediately, with the implantation of a stent to restore coronary patency. As warranted for all TAVR procedures, circulatory assistance should be immediately available to address any refractory haemodynamic instability. Emergency CABG surgery has also been described in this setting, although this option should be used only as a last resort in these high-risk patients.10,87
a
c d
b
Figure 6 | Valve embolization after transcatheter aortic valve replacement. a | Ventricular embolization of a 23 mm Edwards SAPIEN XT® (Edwards Lifesciences Corporation, Irvine, CA, USA) valve after implantation from the transapical approach. b | The embolized valve was recaptured with the inflation balloon and pushed into the aorta. c | Final position of the embolized valve with ectopic deployment in the proximal descending aorta. d | A second Edwards SAPIEN XT® valve was successfully implanted in the aortic valve (arrow).
a b
Figure 7 | Coronary obstruction after transcatheter aortic valve replacement. a | Angiogram showing complete occlusion of the left main coronary artery. The patient died despite cardiopulmonary resuscitation, extracorporeal membrane oxygenation, and emergency cardiac surgery. b | Postmortem examination showing the left main coronary artery ostium (black arrow) covered by the displaced native aortic valve leaflet (white arrow).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 693
ConclusionsMajor progress has been achieved during the past decade in the prevention and management of compli-cations related to TAVR. Advances have been primar-ily as a result of a multidisciplinary approach by the ‘heart team’ enabling improved patient selection and optimal management of complications. Continuous patient assessment after TAVR, and reporting of adverse events according to standardized definitions, should be encouraged, particularly as new devices are developed, to further improve the outcome of patients under going this procedure. Improved outcomes among patient populations currently indicated to undergo TAVR will also be mandatory before this t echnique can be used in lower-risk patient populations.
In the future, the main areas of research will include miniaturization of delivery systems to decrease vascular access-site complications, and embolic protection devices and improved antithrombotic regimens for prevention of
stroke. In addition, upcoming transcatheter heart valves with enhanced paravalvular sealing, and new imaging techniques allowing improved valve prosthesis sizing and positioning, should also result in a decreased incidence of paravalvular AR.
Review criteria
We identified relevant original articles and reviews from the PubMed database. The search terms “transcatheter aortic valve implantation” or “transcatheter aortic valve replacement” were used in combination with the following key words: “complication”, “outcome”, “myocardial infarction”, “stroke”, “cerebrovascular event”, “vascular access”, “access site”, “bleeding”, “acute kidney injury”, “regurgitation”, “malposition”, “migration”, “embolization”, and “coronary obstruction”. We selected full-text articles written in English. No date restrictions were applied to the search. The reference lists of identified papers were also searched for additional relevant articles.
1. Cribier, A. et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 106, 3006–3008 (2002).
2. Leon, M. B. et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 363, 1597–1607 (2010).
3. Smith, C. R. et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 364, 2187–2198 (2011).
4. Vahanian, A. et al. Guidelines on the management of valvular heart disease (version 2012). Eur. Heart J. 33, 2451–2496 (2012).
5. Généreux, P. et al. Clinical outcomes after transcatheter aortic valve replacement using valve academic research consortium definitions: a weighted meta-analysis of 3,519 patients from 16 studies. J. Am. Coll. Cardiol. 59, 2317–2326 (2012).
6. Leon, M. B. et al. Standardized endpoint definitions for transcatheter aortic valve implantation clinical trials: a consensus report from the Valve Academic Research Consortium. Eur. Heart J. 32, 205–217 (2011).
7. Kappetein, A. P. et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. Eur. Heart J. 33, 2403–2418 (2012).
8. van der Boon, R. M. et al. New conduction abnormalities after TAVI—frequency and causes. Nat. Rev. Cardiol. 9, 454–463 (2012).
9. Himbert, D. et al. Tools & techniques: transcatheter aortic valve implantation: transfemoral approach. EuroIntervention 6, 784–785 (2011).
10. Eggebrecht, H. et al. Emergent cardiac surgery during transcatheter aortic valve implantation (TAVI): a weighted meta-analysis of 9,251 patients from 46 studies. EuroIntervention 8, 1072–1080 (2013).
11. Khatri, P. J. et al. Adverse effects associated with transcatheter aortic valve implantation: a meta-analysis of contemporary studies. Ann. Intern. Med. 158, 35–46 (2013).
12. Gilard, M. et al. Registry of transcatheter aortic-valve implantation in high-risk patients. N. Engl. J. Med. 366, 1705–1715 (2012).
13. Van Mieghem, N. M. et al. Cause of death after transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. http://dx.doi.org/ 10.1002/ccd.24597.
14. Rodés-Cabau, J. et al. Incidence, predictive factors, and prognostic value of myocardial injury following uncomplicated transcatheter aortic valve implantation. J. Am. Coll. Cardiol. 57, 1988–1999 (2011).
15. Yong, Z. Y. et al. Predictors and prognostic value of myocardial injury during transcatheter aortic valve implantation. Circ. Cardiovasc. Interv. 5, 415–423 (2012).
16. Barbash, I. M. et al. Prevalence and effect of myocardial injury after transcatheter aortic valve replacement. Am. J. Cardiol. 111, 1337–1343 (2013).
17. Dewey, T. M. et al. Effect of concomitant coronary artery disease on procedural and late outcomes of transcatheter aortic valve implantation. Ann. Thorac. Surg. 89, 758–767 (2010).
18. Gasparetto, V. et al. Safety and effectiveness of a selective strategy for coronary artery revascularization before transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 81, 376–383 (2013).
19. Gautier, M. et al. Impact of coronary artery disease on indications for transcatheter aortic valve implantation and on procedural outcomes. EuroIntervention 7, 549–555 (2011).
20. Wenaweser, P. et al. Impact of coronary artery disease and percutaneous coronary intervention on outcomes in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation. EuroIntervention 7, 541–548 (2011).
21. van Swieten, J. C., Koudstaal, P. J., Visser, M. C., Schouten, H. J. & van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 19, 604–607 (1988).
22. Miller, D. C. et al. Transcatheter (TAVR) versus surgical (AVR) aortic valve replacement: occurrence, hazard, risk factors, and consequences of neurologic events in the PARTNER trial. J. Thorac. Cardiovasc. Surg. 143, 832–843.e13 (2012).
23. Nombela-Franco, L. et al. Timing, predictive factors, and prognostic value of cerebrovascular events in a large cohort of patients undergoing
transcatheter aortic valve implantation. Circulation 126, 3041–3053 (2012).
24. Stortecky, S. et al. Cerebrovascular accidents complicating transcatheter aortic valve implantation: frequency, timing and impact on outcomes. EuroIntervention 8, 62–70 (2012).
25. Eggebrecht, H. et al. Risk of stroke after transcatheter aortic valve implantation (TAVI): a meta-analysis of 10,037 published patients. EuroIntervention 8, 129–138 (2012).
26. Amat-Santos, I. J. et al. Incidence, predictive factors, and prognostic value of new-onset atrial fibrillation following transcatheter aortic valve implantation. J. Am. Coll. Cardiol. 59, 178–188 (2012).
27. Omran, H. et al. Silent and apparent cerebral embolism after retrograde catheterisation of the aortic valve in valvular stenosis: a prospective, randomised study. Lancet 361, 1241–1246 (2003).
28. Ghanem, A. et al. Prognostic value of cerebral injury following transfemoral aortic valve implantation. EuroIntervention 8, 1296–1306 (2013).
29. Fairbairn, T. A. et al. Diffusion-weighted MRI determined cerebral embolic infarction following transcatheter aortic valve implantation: assessment of predictive risk factors and the relationship to subsequent health status. Heart 98, 18–23 (2012).
30. Kahlert, P. et al. Silent and apparent cerebral ischemia after percutaneous transfemoral aortic valve implantation: a diffusion-weighted magnetic resonance imaging study. Circulation 121, 870–878 (2010).
31. Astarci, P. et al. Cerebral embolization during percutaneous valve implantation does not occur during balloon inflation valvuloplasty: prospective diffusion-weighted brain MRI study. J. Heart Valve Dis. 22, 79–84 (2013).
32. Ghanem, A. et al. Risk and fate of cerebral embolism after transfemoral aortic valve implantation: a prospective pilot study with diffusion-weighted magnetic resonance imaging. J. Am. Coll. Cardiol. 55, 1427–1432 (2010).
33. Rodés-Cabau, J. et al. Cerebral embolism following transcatheter aortic valve implantation: comparison of transfemoral and transapical approaches. J. Am. Coll. Cardiol. 57, 18–28 (2011).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

694 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrcardio
34. Kahlert, P. et al. Cerebral embolization during transcatheter aortic valve implantation: a transcranial Doppler study. Circulation 126, 1245–1255 (2012).
35. Van Mieghem, N. M. et al. Histopathology of embolic debris captured during transcatheter aortic valve replacement. Circulation 127, 2194–2201 (2013).
36. Grube, E. et al. Feasibility of transcatheter aortic valve implantation without balloon pre-dilation: a pilot study. JACC Cardiovasc. Interv. 4, 751–757 (2011).
37. Bagur, R. et al. Transcatheter aortic valve implantation with “no touch” of the aortic arch for the treatment of severe aortic stenosis associated with complex aortic atherosclerosis. J. Card. Surg. 25, 501–503 (2010).
38. Nietlispach, F. et al. An embolic deflection device for aortic valve interventions. JACC Cardiovasc. Interv. 3, 1133–1138 (2010).
39. Bourantas, C. V. et al. Transcatheter aortic valve implantation: new developments and upcoming clinical trials. EuroIntervention 8, 617–627 (2012).
40. Naber, C. K. et al. First-in-man use of a novel embolic protection device for patients undergoing transcatheter aortic valve implantation. EuroIntervention 8, 43–50 (2012).
41. Webb, J. G. & Barbanti, M. Cerebral embolization during transcatheter aortic valve implantation. Circulation 126, 1567–1569 (2012).
42. Van Mieghem, N. M. et al. Transcatheter aortic valve replacement and vascular complications definitions. EuroIntervention [online], http://www.pcronline.com/eurointervention/ ahead_of_print/201209-05.
43. Mussardo, M. et al. Periprocedural and short-term outcomes of transfemoral transcatheter aortic valve implantation with the Sapien XT as compared with the Edwards Sapien valve. JACC Cardiovasc. Interv. 4, 743–750 (2011).
44. Généreux, P. et al. Vascular complications after transcatheter aortic valve replacement: insights from the PARTNER (Placement of AoRTic TraNscathetER Valve) trial. J. Am. Coll. Cardiol. 60, 1043–1052 (2012).
45. Hayashida, K. et al. Transfemoral aortic valve implantation new criteria to predict vascular complications. JACC Cardiovasc. Interv. 4, 851–858 (2011).
46. Van Mieghem, N. M. et al. Trends in outcome after transfemoral transcatheter aortic valve implantation. Am. Heart J. 165, 183–192 (2013).
47. Ducrocq, G. et al. Vascular complications of transfemoral aortic valve implantation with the Edwards SAPIEN prosthesis: incidence and impact on outcome. EuroIntervention 6, 666–672 (2010).
48. Hayashida, K. et al. True percutaneous approach for transfemoral aortic valve implantation using the Prostar XL device: impact of learning curve on vascular complications. JACC Cardiovasc. Interv. 5, 207–214 (2012).
49. Pasic, M. et al. Rupture of the device landing zone during transcatheter aortic valve implantation: a life-threatening but treatable complication. Circ. Cardiovasc. Interv. 5, 424–432 (2012).
50. Barbanti, M. et al. Anatomical and procedural features associated with aortic root rupture during balloon-expandable transcatheter aortic valve replacement. Circulation 128, 244–253 (2013).
51. Martinez, M. I., Garcia, H. G. & Calvar, J. A. Interventricular septum rupture after transcatheter aortic valve implantation. Eur. Heart J. 33, 190 (2012).
52. Blanke, P. et al. Prosthesis oversizing in balloon-expandable transcatheter aortic valve implantation is associated with contained rupture of the aortic root. Circ. Cardiovasc. Interv. 5, 540–548 (2012).
53. Borz, B. et al. Incidence, predictors and impact of bleeding after transcatheter aortic valve implantation using the balloon-expandable Edwards prosthesis. Heart 99, 860–865 (2013).
54. Pilgrim, T., Stortecky, S., Luterbacher, F., Windecker, S. & Wenaweser, P. Transcatheter aortic valve implantation and bleeding: incidence, predictors and prognosis. J. Thromb. Thrombolysis 35, 456–462 (2013).
55. Amabile, N. et al. Incidence, predictors and prognostic value of serious hemorrhagic complications following transcatheter aortic valve implantation. Int. J. Cardiol. 168, 151–156 (2013). .
56. Tchetche, D. et al. Adverse impact of bleeding and transfusion on the outcome post-transcatheter aortic valve implantation: insights from the Pooled-RotterdAm-Milano-Toulouse In Collaboration Plus (PRAGMATIC Plus) initiative. Am. Heart J. 164, 402–409 (2012).
57. Rezq, A. et al. Incidence, management, and outcomes of cardiac tamponade during transcatheter aortic valve implantation: a single-center study. JACC Cardiovasc. Interv. 5, 1264–1272 (2012).
58. Takagi, H., Niwa, M., Mizuno, Y., Goto, S. N. & Umemoto, T. Incidence, predictors, and prognosis of acute kidney injury after transcatheter aortic valve implantation: a summary of contemporary studies using Valve Academic Research Consortium definitions. Int. J. Cardiol. http://dx.doi.org/10.1016/ j.ijcard.2013.01.273.
59. Khawaja, M. Z. et al. The effects of VARC-defined acute kidney injury after transcatheter aortic valve implantation (TAVI) using the Edwards bioprosthesis. EuroIntervention 8, 563–570 (2012).
60. Nuis, R. J. et al. Blood transfusion and the risk of acute kidney injury after transcatheter aortic valve implantation. Circ. Cardiovasc. Interv. 5, 680–688 (2012).
61. Bagur, R. et al. Acute kidney injury following transcatheter aortic valve implantation: predictive factors, prognostic value, and comparison with surgical aortic valve replacement. Eur. Heart J. 31, 865–874 (2010).
62. Jabbour, A. et al. Multimodality imaging in transcatheter aortic valve implantation and post-procedural aortic regurgitation: comparison among cardiovascular magnetic resonance, cardiac computed tomography, and echocardiography. J. Am. Coll. Cardiol. 58, 2165–2173 (2011).
63. Zamorano, J. L. et al. EAE/ASE recommendations for the use of echocardiography in new transcatheter interventions for valvular heart disease. Eur. J. Echocardiogr. 12, 557–584 (2011).
64. Zoghbi, W. A. et al. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound: a report From the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and
the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 22, 975–1014 (2009).
65. Lerakis, S., Hayek, S. S. & Douglas, P. S. Paravalvular aortic leak after transcatheter aortic valve replacement: current knowledge. Circulation 127, 397–407 (2013).
66. Michel, P. L., Vahanian, A., Besnainou, F. & Acar, J. Value of qualitative angiographic grading in aortic regurgitation. Eur. Heart J. 8 (Suppl. C), 11–14 (1987).
67. Sinning, J. M. et al. Aortic regurgitation index defines severity of peri-prosthetic regurgitation and predicts outcome in patients after transcatheter aortic valve implantation. J. Am. Coll. Cardiol. 59, 1134–1141 (2012).
68. Athappan, G. et al. Incidence, predictors, and outcomes of aortic regurgitation after transcatheter aortic valve replacement: meta-analysis and systematic review of literature. J. Am. Coll. Cardiol. 61, 1585–1595 (2013).
69. Généreux, P. et al. Paravalvular leak after transcatheter aortic valve replacement: the new Achilles’ heel? A comprehensive review of the literature. J. Am. Coll. Cardiol. 61, 1125–1136 (2013).
70. Sinning, J. M. et al. Evaluation and management of paravalvular aortic regurgitation after transcatheter aortic valve replacement. J. Am. Coll. Cardiol. 62, 11–20 (2013).
71. Al-Attar, N., Himbert, D., Vahanian, A. & Nataf, P. Severe intraprosthetic regurgitation by immobile leaflet after trans-catheter aortic valve implantation. Eur. J. Cardiothorac. Surg. 39, 591–592 (2011).
72. Agostoni, P., Buijsrogge, M. P. & Stella, P. R. “Frozen” leaflet: a dreadful complication of transcatheter aortic valve implantation. Circ. Cardiovasc. Interv. 5, 321–323 (2012).
73. Willson, A. B. et al. Computed tomography-based sizing recommendations for transcatheter aortic valve replacement with balloon-expandable valves: comparison with transesophageal echocardiography and rationale for implementation in a prospective trial. J. Cardiovasc. Comput. Tomogr. 6, 406–414 (2012).
74. Binder, R. K. et al. The impact of integration of a multidetector computed tomography annulus area sizing algorithm on outcomes of transcatheter aortic valve replacement: a prospective, multicenter, controlled trial. J. Am. Coll. Cardiol. 62, 431–438 (2013).
75. Schultz, C. J. et al. Three dimensional evaluation of the aortic annulus using multislice computer tomography: are manufacturer’s guidelines for sizing for percutaneous aortic valve replacement helpful? Eur. Heart J. 31, 849–856 (2010).
76. Hayashida, K. et al. Impact of CT-guided valve sizing on post-procedural aortic regurgitation in transcatheter aortic valve implantation. EuroIntervention 8, 546–555 (2012).
77. Dvir, D. et al. Multicenter evaluation of Edwards SAPIEN positioning during transcatheter aortic valve implantation with correlates for device movement during final deployment. JACC Cardiovasc. Interv. 5, 563–570 (2012).
78. Binder, R. K. et al. Transcatheter aortic valve replacement with the SAPIEN 3: a new balloon-expandable transcatheter heart valve. JACC Cardiovasc. Interv. 6, 293–300 (2013).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | 695
79. Ussia, G. P. et al. Transcatheter aortic bioprosthesis dislocation: technical aspects and midterm follow-up. EuroIntervention 7, 1285–1292 (2012).
80. Sinning, J. M., Vasa-Nicotera, M., Werner, N., Nickenig, G. & Hammerstingl, C. Interventional closure of paravalvular leakage after transcatheter aortic valve implantation. Eur. Heart J. 33, 2498 (2012).
81. Clavel, M. A. et al. Severe valvular regurgitation and late prosthesis embolization after percutaneous aortic valve implantation. Ann. Thorac. Surg. 87, 618–621 (2009).
82. Pang, P. Y., Chiam, P. T., Chua, Y. L. & Sin, Y. K. A survivor of late prosthesis migration and rotation following percutaneous transcatheter aortic valve implantation. Eur. J. Cardiothorac. Surg. 41, 1195–1196 (2012).
83. Makkar, R. R. et al. Determinants and outcomes of acute transcatheter valve-in-valve therapy or embolization: a study of multiple valve implants
in the US PARTNER trial (Placement of AoRTic TraNscathetER Valve Trial Edwards SAPIEN Transcatheter Heart Valve). J. Am. Coll. Cardiol. 62, 418–430 (2013).
84. Tay, E. L. et al. Outcome of patients after transcatheter aortic valve embolization. JACC Cardiovasc. Interv. 4, 228–234 (2011).
85. Dumonteil, N. et al. Left ventricular embolization of an aortic balloon-expandable bioprosthesis: balloon capture and reimpaction as an alternative to emergent conversion to open-heart surgery. JACC Cardiovasc. Interv. 6, 308–310 (2013).
86. Dvir, D. et al. Transcatheter aortic valve replacement for degenerative bioprosthetic surgical valves: results from the global valve-in-valve registry. Circulation 126, 2335–2344 (2012).
87. Ribeiro, H. B. et al. Coronary obstruction following transcatheter aortic valve implantation: a systematic review. JACC Cardiovasc. Interv. 6, 452–461 (2013).
88. Holmes, D. R. Jr et al. 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valve replacement. J. Am. Coll. Cardiol. 59, 1200–1254 (2012).
89. Himbert, D. et al. Results of transfemoral or transapical aortic valve implantation following a uniform assessment in high-risk patients with aortic stenosis. J. Am. Coll. Cardiol. 54, 303–311 (2009).
90. Stabile, E. et al. Acute left main obstructions following TAVI. EuroIntervention 6, 100–105 (2010).
91. Bourantas, C. V. et al. Transcatheter aortic valve implantation: new developments and upcoming clinical trials. EuroIntervention 8, 617–627 (2012).
Author contributionsA.-A. Fassa, researched data for the article. All the authors contributed to the discussion of content, wrote the article, and reviewed/edited the manuscript before submission.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 10 | DECEMBER 2013 | i
CORRECTION
Mechanisms and management of TAVR‑related complicationsAmir-Ali Fassa, Dominique Himbert & Alec Vahanian
Nat. Rev. Cardiol advance online publication 8 October 2013; doi:10.1038/nrcardio.2013.156
In the version of this article originally published online, the sentence “The Claret CE Pro™ system (Claret Medical, Inc., Santa Rosa, CA, USA; Figure 2a) consists of...” should have read “The Claret Montage™ Dual Filter System (Claret Medical, Inc., Santa Rosa, CA, USA; Figure 2a) consists of...”. The error has been corrected in the HTML and PDF versions of the article.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved