measured by Doppler echocardiography: normal values and relation ...
6
BrHeart j 1995;73:334-339 Left ventricular diastolic function in children measured by Doppler echocardiography: normal values and relation with growth Frances A Bu'Lock, Martin G Mott, Robin P Martin Abstract Objectives-To determine normal values for variables of left ventricular diastolic function in children measured by Doppler echocardiography and their relations to body surface area (BSA). Background-There is increasing inter- est in echocardiographic assessment of left ventricular diastolic function in chil- dren but normal data for children are limited. Methods-Assessment of left ventricular diastolic function was performed in 130 normal participants (aged from 2-4 months to 19-6 years) from their trans- mitral flow patterns obtained by pulsed wave Doppler echocardiography. Results-Centile charts for commonly used left ventricular diastolic functional variables plotted against BSA are pre- sented. Peak early diastolic filling veloc- ity and atrial phase filling velocity integral were independent of BSA. Although most other filling indices showed strong relations with BSA, some had more curvilinear relations with BSA due to additional interactions with heart rate. The increase in left ventricular fill- ing with growth is largely achieved by an increase in the early "passive" contribu- tion to filling. The slower heart rates of older children are associated with lower atrial phase filling velocities but increased filling time, so the atrial con- tribution to filling remains relatively con- stant. Conclusions-Normal values of many left ventricular diastolic function variables change with growth in children and cannot be extrapolated from adult data. The data presented are suitable for use in size matched matched comparative studies of left ventricular function in children. Careful standardisation of echocardiographic protocols is necessary to ensure the validity of any comparisons. (Br Heart J 1995;73:334-339) Keywords: left ventricular diastolic function in children; Doppler echocardiography; body surface area. The accurate assessment of ventricular func- tion is becoming increasingly important in the management of children with heart disease, particularly with improvements in long-term survival for congenital and acquired heart disease. High quality echocardiography equipment is now in general use. Echocardiography is readily performed and multiple examinations are rarely contraindicated. Measures of left ventricular systolic function obtained by M mode echocardiography are widely accepted and used. Their utility, however, is limited in the presence of regional wall motion abnor- malities or dyskinesia.' It is also well recog- nised that symptomatic congestive cardiac failure may occur despite apparently normal cardiac function according to these indices in individuals with predominantly diastolic func- tional abnormalities.2 3 There is increasing interest in the use of Doppler echocardio- graphy to measure transmitral flow velocity patterns as an index of left ventricular filling and hence diastolic function. This may pro- vide a more global index of myocardial integrity.4 7 Normal values for diastolic filling para- meters measured by Doppler echocardio- graphy have been reported for preterm infants,8 neonates,9 and adults,6"1'" 11 There are, however, few data for older infants, children, and adolescents,12 although these measure- ments are known to vary markedly with age and heart rate in adults.3 14 There are no data on the relations of transmitral diastolic filling patterns to body surface area (BSA) in healthy children. Normal values for diastolic left ventricular function in 130 children and adolescents under 20 years of age measured by Doppler echocardiography are presented here. Patients and methods Echocardiographic examination of 130 healthy children and adolescents from whom full clinical histories had been obtained and cardiovascular examinations performed was recorded. Height (m), weight (kg), BSA (m2) and systolic and diastolic blood pressures (mm Hg) were noted in each case (table 1). There were 62 girls and 68 boys. Their ages ranged between 2-4 months and 19-6 (mean 7 52) years, with BSAs between 0-22 and 1 85 (mean 0-94) M2. No child had heart disease, as judged by history, clinical examination, and echocardiography, and all had normal systolic left ventricular function. Four had grade 1 or 2 ejection systolic mur- murs diagnosed clinically as "innocent" and confirmed echocardiographically as having no pathological significance. Departments of Paediatric Cardiology and Oncology, Bristol Royal Hospital for Sick Children, St Michael's Hill, Bristol BS2 8BJ F A Bu'Lock M G Mott R P Martin Correspondence to: Dr F A Bu'Lock, Department of Paediatric Cardiology, Alder Hey Children's Hospital, Eaton Road, Liverpool L12 2AP. Accepted for publication 20 September 1994 334
-
Upload
dangnguyet -
Category
Documents
-
view
223 -
download
1
Transcript of measured by Doppler echocardiography: normal values and relation ...

BrHeart j 1995;73:334-339
Left ventricular diastolic function in childrenmeasured by Doppler echocardiography: normalvalues and relation with growth
Frances A Bu'Lock, Martin G Mott, Robin P Martin
AbstractObjectives-To determine normal valuesfor variables of left ventricular diastolicfunction in children measured byDoppler echocardiography and theirrelations to body surface area (BSA).Background-There is increasing inter-est in echocardiographic assessment ofleft ventricular diastolic function in chil-dren but normal data for children arelimited.Methods-Assessment of left ventriculardiastolic function was performed in 130normal participants (aged from 2-4months to 19-6 years) from their trans-mitral flow patterns obtained by pulsedwave Doppler echocardiography.Results-Centile charts for commonlyused left ventricular diastolic functionalvariables plotted against BSA are pre-sented. Peak early diastolic filling veloc-ity and atrial phase filling velocityintegral were independent of BSA.Although most other filling indicesshowed strong relations with BSA, somehad more curvilinear relations with BSAdue to additional interactions with heartrate. The increase in left ventricular fill-ing with growth is largely achieved by anincrease in the early "passive" contribu-tion to filling. The slower heart rates ofolder children are associated with loweratrial phase filling velocities butincreased filling time, so the atrial con-tribution to filling remains relatively con-stant.Conclusions-Normal values ofmany leftventricular diastolic function variableschange with growth in children andcannot be extrapolated from adult data.The data presented are suitable for usein size matched matched comparativestudies of left ventricular function inchildren. Careful standardisation ofechocardiographic protocols is necessaryto ensure the validity ofany comparisons.
(Br Heart J 1995;73:334-339)
Keywords: left ventricular diastolic function inchildren; Doppler echocardiography; body surfacearea.
The accurate assessment of ventricular func-tion is becoming increasingly important in themanagement of children with heart disease,particularly with improvements in long-term
survival for congenital and acquired heartdisease.
High quality echocardiography equipmentis now in general use. Echocardiography isreadily performed and multiple examinationsare rarely contraindicated. Measures of leftventricular systolic function obtained by Mmode echocardiography are widely acceptedand used. Their utility, however, is limited inthe presence of regional wall motion abnor-malities or dyskinesia.' It is also well recog-nised that symptomatic congestive cardiacfailure may occur despite apparently normalcardiac function according to these indices inindividuals with predominantly diastolic func-tional abnormalities.2 3 There is increasinginterest in the use of Doppler echocardio-graphy to measure transmitral flow velocitypatterns as an index of left ventricular fillingand hence diastolic function. This may pro-vide a more global index of myocardialintegrity.4 7Normal values for diastolic filling para-
meters measured by Doppler echocardio-graphy have been reported for preterminfants,8 neonates,9 and adults,6"1'"11 There are,however, few data for older infants, children,and adolescents,12 although these measure-ments are known to vary markedly with ageand heart rate in adults.3 14 There are no dataon the relations of transmitral diastolic fillingpatterns to body surface area (BSA) in healthychildren.Normal values for diastolic left ventricular
function in 130 children and adolescentsunder 20 years of age measured by Dopplerechocardiography are presented here.
Patients and methodsEchocardiographic examination of 130healthy children and adolescents from whomfull clinical histories had been obtainedand cardiovascular examinations performedwas recorded. Height (m), weight (kg), BSA(m2) and systolic and diastolic blood pressures(mm Hg) were noted in each case (table 1).There were 62 girls and 68 boys. Theirages ranged between 2-4 months and 19-6(mean 7 52) years, with BSAs between 0-22and 1 85 (mean 0-94) M2. No child hadheart disease, as judged by history, clinicalexamination, and echocardiography, and allhad normal systolic left ventricular function.Four had grade 1 or 2 ejection systolic mur-murs diagnosed clinically as "innocent" andconfirmed echocardiographically as having nopathological significance.
Departments ofPaediatric Cardiologyand Oncology, BristolRoyal Hospital forSick Children,St Michael's Hill,Bristol BS2 8BJF A Bu'LockM G MottR P MartinCorrespondence to:Dr F A Bu'Lock,Department of PaediatricCardiology, Alder HeyChildren's Hospital, EatonRoad, Liverpool L12 2AP.Accepted for publication20 September 1994
334
Left ventricular diastolic function in children measured by Doppler echocardiography: normal values and relation with growth
Table 1 Cross correlation matrix of transmitralflow variables*
EAcc EAccT EDec EDecT A EVI AVI EAVI IVRT BSA HR
E 0*68 0 0-31 0-31 0-22 075 0-24 072 -0 16 0 -0-25EAcc - -0-7 054 -0-13 0-48 0-2 0-32 0-2 -0-24 -0-47 0-29EAccT - - -0-42 0-47 -0-41 0-46 -0-15 0-4 0-17 063 - 063EDec - - - -0-74 0-41 -027 0 -025 -0 5 -0 57 0-48EDecT - - - - -0-2 0-8 0-16 0-76 0 43 0-62 -0-63A - - - - - 0 086 0-16 -033 -0-38 068EVI - - - - - 02 094 015 0 45 -0-63AVI - - - - - - - 0-44 -0-14 0 0-38EAVI - - - - - - - - 0-13 0-4 -0-5IVRT - - - - - - - - - 056 -0-47BSA - - - - - - - - - - -064
*A, Peak atrial phase filling velocity (ms- '); AVI, velocity integral of A wave (cm); BSA, body surface area (m2); E, peak earlyphase filling velocity (ms-'); EA, EA ratio (E/A); EAcc, acceleration to peak E (ms-2); EAccT, time to peak E (ms); EAVI,velocity integral of entire transmitral flow complex (cm); EDec, deceleration from peak E (ms-2); EDecT, time from peak E tobaseline (ms); EVI, velocity integral of E wave (cm); HR, heart rate (beats min- '); IVRT, isovolumic relaxation time (ms); VIR,velocity integral ratio (EVI/EAVI). Table shows values of Pearson's correlation coefficient (r) for relations between transmitralflow variables. r Values in bold text denote those with P < 0 001.
Full ethical approval was given for thestudy by the Bristol and Weston DistrictEthical Committee. Informed consent foreach study was obtained from all parents andfrom the participants where appropriate.
ECHOCARDIOGRAPHIC EXAMINATIONEchocardiographic examination was per-formed in the left lateral semirecumbent posi-tion whenever possible. Sedation was not usedand some small children were examined onlyin a semirecumbent position on their mother'slap. Examinations were performed by a singleoperator (FAB) using a Hewlett Packard77020AC ultrasound scanner and recordedonto videotape. An electrocardiographic trace(ECG) and phonocardiogram were recordedsimultaneously with the echocardiogram.Transducer frequency was 3-5 MHz or5 MHz, either or both being used for eachpatient, to provide optimal imaging and
S2
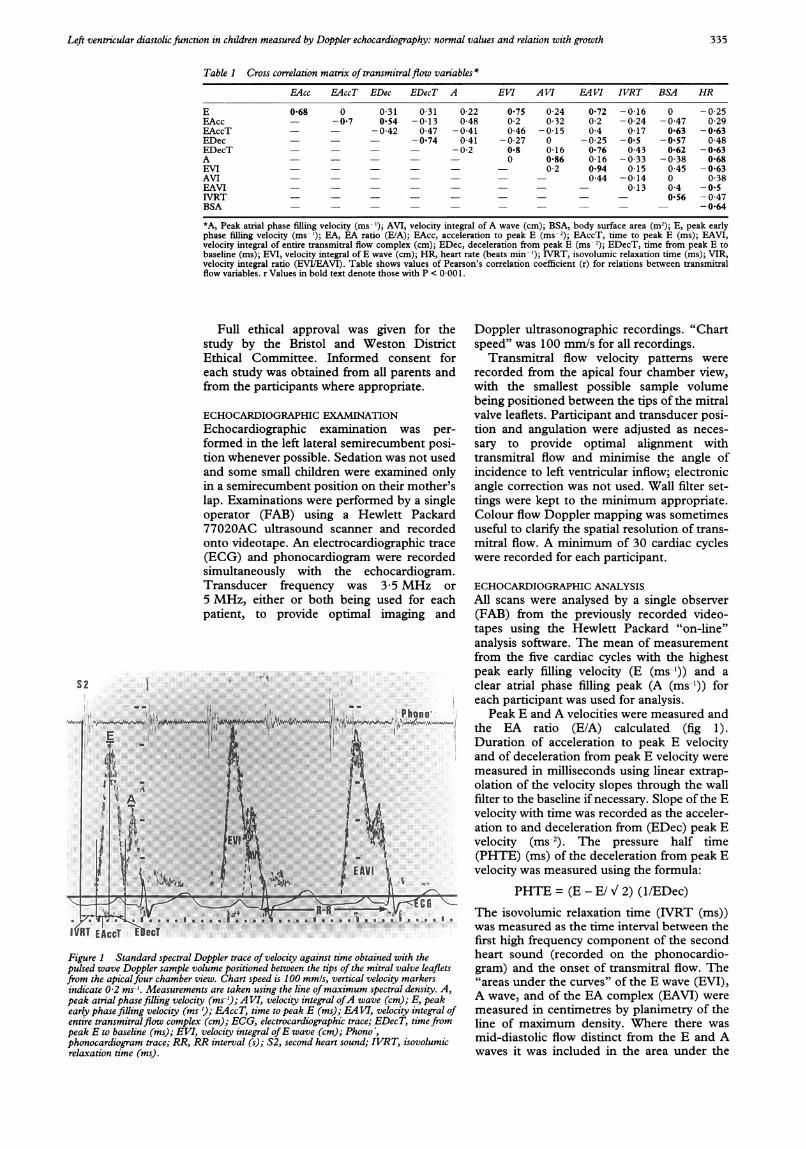
Figure 1 Standard spectral Doppler trace of velocity against time obtained with thepulsed wave Doppler sample volume positioned between the tips of the mitral valve leafletsfrom the apicalfour chamber view. Chart speed is 100 mmls, vertical velocity markersindicate 0-2 ms-'. Measurements are taken using the line ofmaximum spectral density. A,peak atrial phase filling velocity (ms-'); A VI, velocity integral ofA wave (cm); E, peakearly phase filling velocity (ms-'); EAccT, time to peak E (ms); EA VI, velocity integral ofentire transmitralflow complex (cm); ECG, electrocardiographic trace; EDecT, timefrompeak E to baseline (ms); EVI, velocity integral ofE wave (cm); Phono,phonocardiogram trace; RR, RR interval (s); S2, second heart sound; IVRT, isovolumicrelaxation time (ms).
Doppler ultrasonographic recordings. "Chartspeed" was 100 mm/s for all recordings.
Transmitral flow velocity patterns wererecorded from the apical four chamber view,with the smallest possible sample volumebeing positioned between the tips of the mitralvalve leaflets. Participant and transducer posi-tion and angulation were adjusted as neces-sary to provide optimal alignment withtransmitral flow and minimise the angle ofincidence to left ventricular inflow; electronicangle correction was not used. Wall filter set-tings were kept to the minimum appropriate.Colour flow Doppler mapping was sometimesuseful to clarify the spatial resolution of trans-mitral flow. A minimum of 30 cardiac cycleswere recorded for each participant.
ECHOCARDIOGRAPHIC ANALYSISAll scans were analysed by a single observer(FAB) from the previously recorded video-tapes using the Hewlett Packard "on-line"analysis software. The mean of measurementfrom the five cardiac cycles with the highestpeak early filling velocity (E (ms-')) and aclear atrial phase filling peak (A (ms-')) foreach participant was used for analysis.
Peak E and A velocities were measured andthe EA ratio (E/A) calculated (fig 1).Duration of acceleration to peak E velocityand of deceleration from peak E velocity weremeasured in milliseconds using linear extrap-olation of the velocity slopes through the wallfilter to the baseline if necessary. Slope of the Evelocity with time was recorded as the acceler-ation to and deceleration from (EDec) peak Evelocity (ms-2). The pressure half time(PHTE) (ms) of the deceleration from peak Evelocity was measured using the formula:
PHTE = (E - E/ V 2) (l/EDec)The isovolumic relaxation time (IVRT (ms))was measured as the time interval between thefirst high frequency component of the secondheart sound (recorded on the phonocardio-gram) and the onset of transmitral flow. The"areas under the curves" of the E wave (EVI),A wave, and of the EA complex (EAVI) weremeasured in centimetres by planimetry of theline of maximum density. Where there wasmid-diastolic flow distinct from the E and Awaves it was included in the area under the
335
It
Bu'Lock, Mott, Martin
Table 2 Normal percentile values for BSA independent variables
Centiles
10 25 50 75 90
Peak early phase filling velocity (ms -) 0 7 0 76 0 84 0.91 0 97Velocity integral ofA wave (cm) 2 34 2 82 3-35 3 81 4 36
total flow curve, but not within either the E orA velocity integrals. The velocity integral ratiowas calculated as EVI/EAVI. The RR interval(s) during the mitral recordings was alsonoted and heart rate (beats min-') calculatedas 60/RR.
ResultsSTATISTICAL ANALYSISUnivariate analyses confirmed that values ofthe study variables principally correlated withheight, weight, BSA, age, heart rate, and sys-tolic blood pressure. These variables highlycorrelated with each other and multivariateanalysis was performed to establish the smallest
possible set of predictor variables whichdescribed the variations in the study variables.Forward selection analysis showed that BSA(or a transformation of BSA) provided such amodel for most study variables and that fur-ther refinement (and added complexity)through adjustment for heart rate was of littleadditional predictive value. For some vari-ables, however, inherent curvilinearity in thedata was noted. This finding was related toheart rate in a univariate model and was prob-ably the result of the range of normal heartrates at any given BSA.
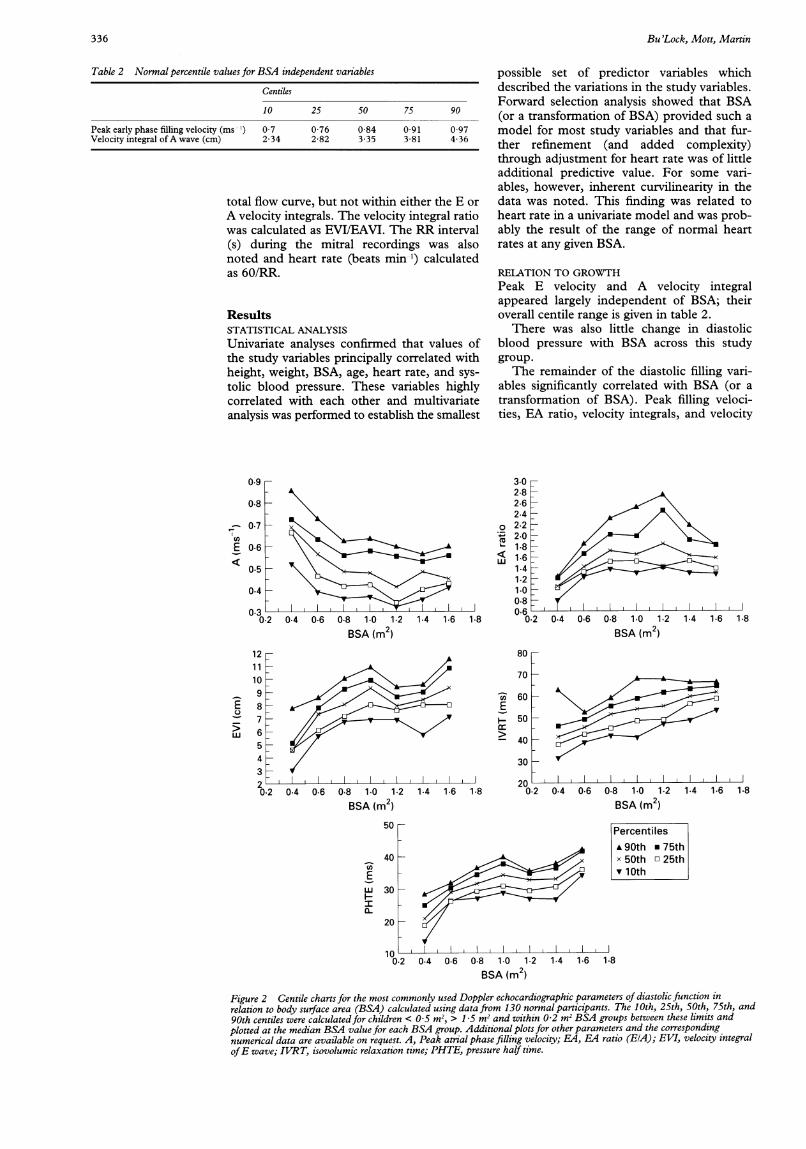
RELATION TO GROWTHPeak E velocity and A velocity integralappeared largely independent of BSA; theiroverall centile range is given in table 2.
There was also little change in diastolicblood pressure with BSA across this studygroup.The remainder of the diastolic filling vari-
ables significantly correlated with BSA (or atransformation of BSA). Peak filling veloci-ties, EA ratio, velocity integrals, and velocity
0
LL
Iv J
0.2 0.4 0.6 0.8 1.0 1.2BSA (m2)
121110987654320.2
1.4 1.6 1.8
E
Hr
0.4 0.6 0.8 1.0 1.2
BSA (m2)1.4 1.6 1.8
3.02.82.62.42.22.01.81.61.41.21.00.8 C I I,I0.66
0.2 0.4 06 0.8 1.0 1.2 1.4 1.6 1.8BSA (m2)
80
70
60
50
40
30
200.2 04 06 0.8 10 1.2 1.4 1.6 1.8
BSA (m2)50 Percentiles
A, 90th * 75th40 x 50th o 25th
10 v10thE
wu 30 - A
20
0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8
BSA(m )
Figure 2 Centile charts for the most commonly used Doppler echocardiographic parameters of diastolic function inrelation to body surface area (BSA) calculated using data from 130 normal participants. The 10th, 25th, 50th, 75th, and90th centiles were calculatedfor children < 0 5 m2, > 1 5 m2 and within 0-2 m2 BSA groups between these limits andplotted at the median BSA value for each BSA group. Additional plots for other parameters and the correspondingnumerical data are available on request. A, Peak atrial phase filling velocity; EA, EA4 ratio (EIA); EVI, velocity integralofE wave; IVRT, isovolumic relaxation time; PHTE, pressure half time.
0.9
0.8
0.7
06
0.50.4
(nE
-a>.wU
336
Left ventricular diastolic function in children measured by Doppler echocardiography: normal values and relation with growth
integral ratio all had a more linear relationshipwith heart rate than with BSA, but the rela-tion remained weak for peak E velocity and Avelocity integral. Although overall restingheart rate is inversely proportional to BSA inhealthy children, there is significant variabilityand thus, range of normal, for a given BSA.Therefore the 10th, 25th, 50th, 75th, and90th centile values for each variable werecalculated for children with BSAs < 0 5 m2n,> 1'5 m2, and within 0 2 m2 BSA groupsfrom 0 5 to 1-49 M2. Centile plots of the rela-tion of the most frequently used diastolic vari-ables with BSA are shown in fig 2. Plots forthe other study variables, and the correspond-ing numeric data are available from theauthors on request.
Cross correlations between transmitral flowvariables were examined (table 1). The PHTEfrom peak E velocity mainly correlated withBSA (r = 0 67), in keeping with its relationwith mitral valve area. IVRT also correlatedwith BSA (r = 0 56) and to a lesser degree toheart rate (r = - 047) and E deceleration(r = - 0-5), but showed no noteworthy rela-tion with any other variable.
There were no sex related differencesdetectable by comparative regression analysisin the relations between diastolic filling vari-ables and BSA.
DiscussionNormal values for left ventricular diastolic fill-ing variables change with age and this pro-vides some interesting insights into leftventricular diastolic function in childhood.Although in healthy children, BSA and ageare closely correlated, this is frequently notthe case in sick children, including those withcardiac dysfunction. Normal data are there-fore presented in relation to body size (BSA)rather than age.The change in profile of the transmitral
Doppler flow velocity envelope with growth isa result of the interdependence of filling vari-ables (shown in table 1) and their relationswith BSA and heart rate:- Peak early filling velocity is most stronglyrelated to the rate of acceleration to peak E,which depends principally on the atrioventric-ular pressure gradient.'5 This is inverselyrelated (among other factors) to mitral valvearea and therefore also to BSA, but is largelyunrelated to heart rate. Acceleration time isinversely proportional to heart rate and accel-eration to peak E. Thus peak E velocity islargely independent of BSA and only weaklyinversely related to heart rate.- The velocity integral of the E wave isstrongly correlated with deceleration timefrom peak E, which, like acceleration time,has similar but opposite relations with heartrate and BSA. As the heart rate decreases(with increased BSA), total early filling timelengthens. Therefore, despite little changein peak E velocity, E velocity integral andEA velocity integral increase with BSA asheart rate decreases. These findings are inagreement with observations'6 and pacing
studies'7 18 in adults, although absolute rela-tions differ. This might simply be the result ofthe much wider range of heart rates seen inthe present participants. It might also reflecttrue physiological differences, however,between changes in diastolic function andalteration of heart rate in the same individualas opposed to cross sectional relations in thenormal resting state.- Peak atrial phase filling velocity is notrelated to the velocity integral of the E wavebut is principally related to heart rate in thisstudy. Heart rate is known from studies innormal adults'718 to have a major effect onpeak A velocity and therefore on EA ratio.This is probably the result of the shorter timeavailable for early diastolic filling at fasterheart rates,'5 with a greater atrioventricularpressure gradient during atrial systole. Thevelocity integral of the A wave is related topeak A velocity but shows little overall changewith growth.
Thus, the lengthening of diastole at slowerheart rates affects early and atrial phases ofdiastolic filling; the prolongation of early fill-ing time is associated with a lower peak Avelocity, but the constancy of the A velocityintegral suggests that late filling also continuesfor longer. The increased total filling at higherBSAs (and lower heart rates) is thereforelargely the consequence of an increase in theproportion of left ventricular filling occurring"passively" during early diastole.The relation of IVRT to BSA, age, and
deceleration from peak E, with a weaker rela-tion to heart rate, is largely as expected. With alarger ventricle and slower heart rate, the timetaken during early diastolic relaxation for leftventricular pressure to decrease below leftatrial pressure is increased and transmitralflow begins later. The negative correlationbetween IVRT and acceleration to peak E (r >- 0 7) demonstrated in adults by Brecker etal 19 was not found in these children. Theadult group, however, had significant myocar-dial pathology with inco-ordinate relaxation,in addition to lower heart rates (the groupmean heart rate was only 75 beats min-').Such relations are clearly different in healthychildren.Normal values for PHTE in children have
not previously been reported. This variable isclearly related to BSA in children, and, as inadults, may provide a guide to functionalmitral valve area which might be of additionalbenefit in the evaluation of mitral stenosis.
These data provide new and potentiallyuseful information on normal diastolic func-tion in children. Concerns relating to theinfluence of loading conditions on resultsobtained as well as to technical factors in dataacquisition, however, must also be addressed.
LOADING CONDITIONSThere is no doubt that transmitral diastolicflow patterns are affected by loading condi-tions.5 1520 By selecting 130 healthy, restingbut unsedated children, the values obtained inthis study incorporate normal variations inphysiological loading conditions without
337

Bu'Lock, Mott, Martin
pharmacological or physical manipulations, asreflected in the recorded measurements ofblood pressure and heart rate. When makingcomparisons with these normal data, it isimportant to be aware that abnormalloading conditions are often associatedwith pathological processes and that either orboth factors may influence the variablesmeasured.
RESPIRATORY PHASEIt is well recognised that the respiratory phasemay have an effect on transmitral flow pat-terns."-" There are considerable practicaldifficulties involved in obtaining detailedechocardiographic records from small chil-dren with ECG leads and a phonocardiogramattached. The use of a respiratory phasedetector was considered to impose additionalcomplications which could not be justifiedin healthy children. Thus there is nodirect compensation for the respiratory phasein this study. It was felt, however, thatselection of multiple similar Doppler com-plexes fulfilling certain predefined criteria-that is, those with the highest E wave and aclear A wave, was likely to minimise thevariability due to the respiratory cycle.These are likely to be expiratory cycles as peakE velocity decreases during inspiration."'3
SAMPLE VOLUME POSITIONStudies in adults24 and infants25 havedemonstrated differences in transmitralflow velocities obtained in the same individualat different locations within the left ventricu-lar inflow tract. In common with manyother groups,5-7 sample volume location wasstandardised at the tips of the mitral valveleaflets. This was because personal experiencesuggested greater reproducibility of samplevolume siting at this location and also becauseit is suggested that the higher velocitiesobtained at this point best reflect the drivingforce across the mitral valve.5
REPRODUCIBII=TYMeasurement error may arise at the time ofscanning and analysis. The magnitude ofinteroperator and interanalyser variability hasbeen demonstrated to be mainly between 5and 10% in healthy adults.'6'7 Our own studiesof reproducibility in 22 children with anthra-cycline cardiomyopathy yielded similarresults, with only random variation for inter-operator differences. These studies alsodemonstrated the potential for small but sig-nificant systematic variability in data analysis(for peak E velocity, A velocity integral, anddeceleration time), although there was goodcorrelation between analysers for all variables.Careful audit of data analysis results isrequired to ensure uniformity of measurementcriteria if scans are to be analysed by morethan one individual. The adult studies26 27 alsoaddressed within subject variability on differ-ent days (without controlling for operator)and noted similar findings; generally 5-10%variation, with more error for flow time mea-surements than for absolute velocities.
Although different sources of measurementerror are not mutually exclusive, the magni-tude of errors introduced by multiple opera-tors, analysers, and examinations are likely tobe cumulative. Thus, particularly for serialstudies of individual patients, it is importantto minimise other sources of error by reducingthe number of operators and analysers, prefer-ably to unity. Moreover, fewer effects of vari-ability will occur with larger numbers ofparticipants in such a series.
ConclusionsStandard normal data for healthy childrenmay be used for comparative purposes inother studies. Such data are presented graphi-cally here as centiles for particular BSA inter-vals. They portray actual observed datawithout statistical assumptions and provide aready gauge of the degree of departure fromthe observed normal range for a given individ-ual's function. These may be of particularvalue with serial studies of individual patients.
Transmitral diastolic flow patterns arestrongly related to BSA. Some variables, how-ever, show a degree of additional variabilitywith resting heart rate. Differential effects ofheart rate variation within the same individualwere not examined here. Comparative studiesof left ventricular function in children requireBSA matching; the effects of heart rate inpathological situations also need careful con-sideration.
Doppler echocardiographic assessment oftransmitral flow is relatively simple to per-form, but the relations of the variablesobtained to diastolic performance are lessclear cut. The normal ranges for children(who are not small adults) are reported here,to permit further examination of these vari-ables in pathological states. When applyingthese normal data to clinical or experimentalresults, the precise study protocols used andparticipants examined will have an importantbearing on their accuracy and relevance. Therelevance of these data in the structurallyabnormal heart is not defined. The variabilityof transmitral flow velocity variables meansthat in clinical use, standardisation ofechocardiographic examination and analysistechniques is vitally important. Perhapsguidelines similar to those of the AmericanHeart Association for M mode echocardio-graphy28 are now indicated?
The authors thank Mrs M Shapland (Bristol UniversityComputer Service) for database design and help with datahandling, Mr J Halsey (Medical Research Council ClinicalTrials Service Unit, Radcliffe Infirmary, Oxford) for statisticalcomputing, and Mrs V Smith for data entry. FAB was sup-ported by a grant from the Cancer Research Campaign andMGM is supported by the Cancer and Leukaemia inChildhood Trust.
1 Gutgesell HP. Echocardiographic assessment of cardiacfunction in infants and children. JAm Coil Cardiol 1985;5:95-103s.
2 Cohn JN, Johnson G. Heart failure with normal ejectionfraction: the V-HeFT study. Circulation 1990;81(suppllII):48-53.
3 Grossman W. Diastolic dysfunction and congestive heartfailure. Circulation 1990;81 (suppl III): 1-7.
338
Left ventricular diastolic function in children measured by Doppler echocardiography: normal values and relation with growth
4 Nishamura RA, Housmans PR. Assessment of diastolicfunction of the heart: background and current applica-tions of Doppler echocardiography: Part 1. Physiologicand pathophysiologic features. Mayo Clin Proc 1989;64:71-81.
5 Nishamura RA, Abel MD, Hatle LK, Tajik J. Assessment ofdiastolic function of the heart: background and currentapplications of Doppler echocardiography: Part II.Clinical studies. Mayo Clin Proc 1989;64:181-204.
6 Appleton CP, Hatle LK, Popp RL. Relation of transmitralflow velocity patterns to left ventricular diastolic func-tion: new insights from a combined hemodynamic andDoppler echocardiographic study. Y Am Coll Cardiol1988;12:426-40.
7 Spirito P, Maron BJ. Doppler echocardiography for assess-ing left ventricular diastolic function. Ann Intern Med1988;109: 122-6.
8 Johnson GL, Moffett CB, Noonan JA. Doppler echocar-diographic studies of diastolic ventricular filling patternsin premature infants. Am Hearty 1988;116:1568-74.
9 Riggs TW, Rodriguez R, Snider AR, Batton DL. Dopplerechocardiographic evaluation of right and left ventriculardiastolic function in normal neonates. YAm Coll Cardiol1989;13:700-5.
10 Loeber CP, Goldberg SJ, Allen HD. Doppler echocardio-graphic comparison of flows distal to the 4 cardiacvalves. JAm Coll Cardiol 1984;4:268-72.
11 Labovitz AJ, Pearson AC. Evaluation of left ventriculardiastolic function: clinical relevance and recent echocar-diographic insights. Am HeartJ 1987;4:836-51.
12 Grenadier E, Oliveira C, Allen HD, et al. Normal intracar-diac and great vessel Doppler flow velocities in infantsand children. Am Coll Cardiol 1984;4:343-50.
13 Kuo LC, Quinones MA, Rokey R, Sartori M, AbinaderEG, Zoghbi WA. Quantification of atrial contribution toleft ventricular filling by pulsed Doppler echocardiogra-phy and the effects of age in normal and diseased hearts.Am Cardiol 1987;59:1174-8.
14 Smith SA, Stoner JE, Russell AE, Sheppard JM, AylwardPE. Transmitral velocities measured by pulsed Dopplerin healthy volunteers: effects of acute changes in bloodpressure and heart rate. BrHeartJ' 1989;61:344-7.
15 Thomas JD, Weyman AE. Echocardiographic Dopplerevaluation of left ventricular diastolic function: physicsand physiology. Circulation 199 1;84:977-90.
16 Stewart RAH, Joshi J, Alexander N, Nihoyannopoulos P,Oakley C. Adjustment for the influence of age and heartrate on Doppler measurements of left ventricular filling.Br HeartJ 1992;68:608-12.
17 Oniki T, Hashimoto Y, Shimizu S, Kakuta T, Yajima M,Numano F. Effect of increasing heart rate on Dopplerindices of left ventricular performance in healthy men.Br HeartJ 1992;68:425-9.
18 Harrison MR, Clifton GD, Pennell AT, DeMaria AN.Effect of heart rate on left ventricular diastolic trans-mitral flow velocity patterns assessed by Doppler echo-cardiography in normal subjects. Am _J Cardiol 1991;67:622-7.
19 Brecker SJD, Lee CH, Gibson DG. Relation of left ven-tricular isovolumic relaxation time and incoordination totransmitral Doppler filling patterns. Br Heart Jf 1992;68:567-73.
20 Stoddard MF, Pearson AC, Kern MJ, Ratcliff J, MrosekDG, Labovitz AJ. Influence of alteration in preload onthe pattern of left ventricular diastolic filling as assessedby Doppler echocardiography in humans. Circulation1989;79: 1226-36.
21 Dabestani A, Takenaka K, Allen B, et al. Effects of sponta-neous respiration on diastolic left ventricular fillingassessed by pulsed Doppler echocardiography. Am JCardiol 1988;61:1356-8.
22 Riggs TW, Snider AR. Respiratory influence on right andleft ventricular diastolic function in normal children. AmJf Cardiol 1989;63:858-6 1.
23 Uiterwaal C, Van Dam I, De Boo T, et al. The effect ofrespiration on diastolic blood flow velocities in thehuman heart. Eur HeartJ 1989;10: 108-12.
24 Gardin JM, Dabestani A, Takenaka K, et al. Effects ofimaging view and sample volume location in evaluationof mitral flow velocity by pulsed wave Doppler echocar-diography. Am Jf Cardiol 1986;57: 1335-7.
25 Johnson GL, Moffett CB, Jurnalov CD, Noonan JA. Effectof sample volume location on pulsed Doppler diastolicflow parameters in newborn infants. Pediatr Cardiol1988;9:221-4.
26 Fast J, van Dam I, Heringa A, et al. Limits of reproduci-bility of mitral pulsed Doppler spectra. Am Jf Cardiol1988;61:891-4.
27 Spirito P, Maron BJ, Verter J, Merrill JS. Reproducibilityof Doppler echocardiographic measurements of leftventricular diastolic function. Eur Heart Jf 1988;9:879-86.
28 Sahn DJ, De Maria A, Kisslo J, Weyman A.Recommendations regarding quantitation in M-modeechocardiography: results of a survey of echocardio-graphic measurements-the committee on M-modestandardisation of the American Society of Echocardio-graphy. Circulation 1978;58:1072-83.
339