MDPH Office of HIV/AIDS & BPHC HIV/AIDS Services Division October 16, 2014 1 HIV SERVICES ACUITY...
35
MDPH Office of HIV/AIDS & BPHC HIV/AIDS Services Division October 16, 2014 1 HIV SERVICES ACUITY TOOL PILOT IMPLEMENTATION MEETING
-
Upload
lester-rodgers -
Category
Documents
-
view
215 -
download
0
Transcript of MDPH Office of HIV/AIDS & BPHC HIV/AIDS Services Division October 16, 2014 1 HIV SERVICES ACUITY...
MDPH Office of HIV/AIDS&BPHC HIV/AIDS Services DivisionOctober 16, 2014
1
HIV SERVICES ACUITY TOOL PILOT
IMPLEMENTATION MEETING

Background: How did we get here?
Introducing the tool
Components of the pilot project
Q & A with contract managers and program coordinators
Evaluation components and feedback process
Practice session
Wrap-up and next steps
AGENDA
2
FY05 Case Management & Residential Support Services contract cycle Comprehensive CM assessment & acuity Self sufficiency outcomes and tools
FY12 Medical Case Management RFR Responsive and flexible service provision
Massachusetts State HIV/AIDS Plan Strengthen programmatic response
3
BACKGROUND OF ACUITY BASED SYSTEM
Tool is currently being used by three SPECTRuM sites (SPNS project focused on linkage and retention for high acuity and newly diagnosed people living with HIV/AIDS) Boston Medical Center Greater New Bedford Community Health Center UMass Memorial Medical Center
Tool will be used by Boston Health Care for the Homeless Program and East Boston Neighborhood Health Center linkage and retention program
CURRENT USE
4

Provide context for acuity systemReview draft acuity tool
Service areas Acuity levels
Review how the tool is used Data sources for completing the tool Assignment of acuity scores
Review evaluation components Client chart review Acuity summary forms Post pilot survey
MEETING OBJECTIVES
5
Pilot Specifics
•Six months
•20 participants per agency
•Mix of high and low acuity
Supports efficient and targeted use of resources at the funder and agency levels
Supports provision of services tailored to individual need
Allows for placement of clients in appropriate service intensity level
Offers multiple levels of engagement as clients’ level of need shifts
6
BENEFITS OF ACUITY BASED SYSTEM

Using acuity to highlight fluid nature of a client’s experiences with HIV/AIDS◦Acknowledging challenges with orienting and adapting to
the service system (especially for the newly diagnosed)◦Complexity of care and challenges experienced by clients
will change over time
Creating a responsive service system◦Primary focus on attaining HIV medical self-management◦Creating ancillary/adjunct services that evolve over time
to meet the needs of clients outside of the medical settings
7
DEFINING SUCCESS AND ACHIEVEMENTS

MCM Assessment and Reassessment
Acuity Tool (in review process)
Individual Service Plan
8
COMPONENTS OF ACUITY SYSTEM
Determines client’s level of need Objective when possibleConsistent
Helps triage clients to the appropriate level of medical case management
Documents provider’s knowledge of and experience with the client
Provides funders with information about client need at the agency level, across the EMA, and throughout the Commonwealth
9
PURPOSE OF ACUITY TOOL
10
APPLYING ACUITY TO MCM SERVICES
MCM Levels
Intensive needModerate needBasic needSelf management
Areas of Functioning Care adherence Current health status Medication adherence Health literacy Sexual/reproductive health
promotion Mental health Drug and alcohol use Housing Living situation/support
systems Legal Income/personal finance Transportation Nutrition 11
TOOL SPECIFICS
Care Adherence: Missing medical appointments, MCM appointments, or other
appointments with care teamCurrent Health Status:
Viral Load/CD4 labs Refusal of ARVs Opportunistic infections Hospitalizations New diagnosis
Medication Adherence Missed doses Significant adverse side effects
DEFINING THE SERVICE AREAS
12

Health Literacy HIV/HCV/STI knowledge Demonstrated understanding of transmission, treatments, and/or
risk reduction Demonstrated understanding of how to take medication as
prescribed and the importance of adherenceSexual/Reproductive Health
Condom access and use Disclosure of status Engagement in transactional sex or commercial sex work Serodiscorant relationships HIV+ and pregnancy
DEFINING THE SERVICE AREAS
13
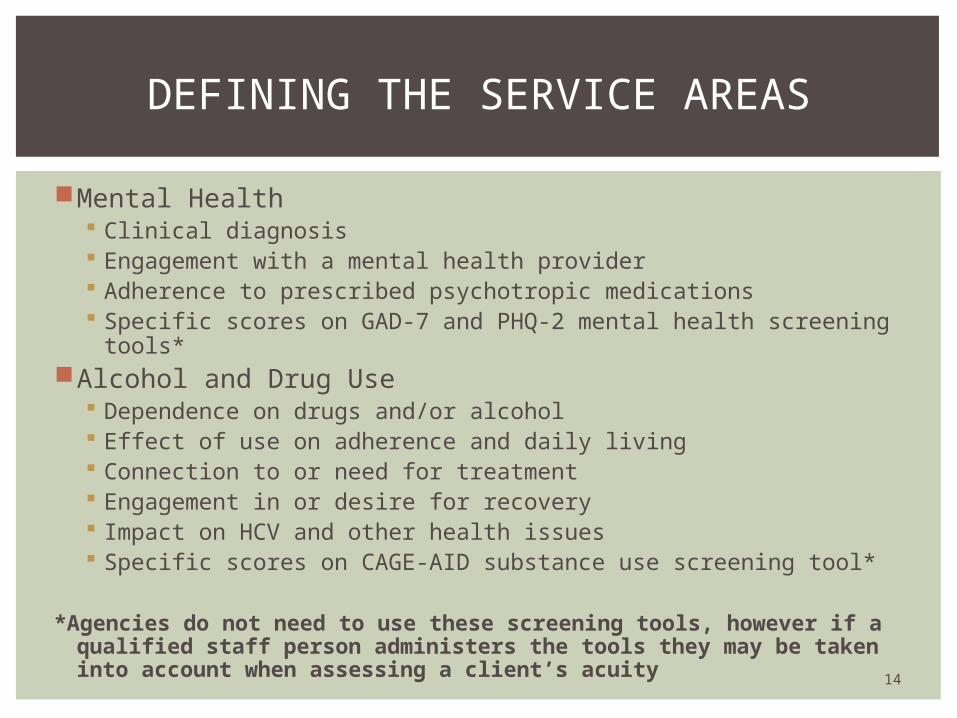
Mental Health Clinical diagnosis Engagement with a mental health provider Adherence to prescribed psychotropic medications Specific scores on GAD-7 and PHQ-2 mental health screening
tools*Alcohol and Drug Use
Dependence on drugs and/or alcohol Effect of use on adherence and daily living Connection to or need for treatment Engagement in or desire for recovery Impact on HCV and other health issues Specific scores on CAGE-AID substance use screening tool*
*Agencies do not need to use these screening tools, however if a qualified staff person administers the tools they may be taken into account when assessing a client’s acuity
DEFINING THE SERVICE AREAS
14

Housing Living in place not meant for habitation (street, car, etc) Living in shelter or doubled up Facing eviction Safety issues Difficulty managing activities of daily living Consistent challenges with maintaining housing (including financial) Currently or recently incarcerated
Legal Facing eviction Issues related to discrimination (employment, housing, etc) Standard legal documents (wills, guardianship, immigration
paperwork, etc.)
DEFINING THE SERVICE AREAS
15

Living Situation/Support Systems Current or past interpersonal relationship violence Inadequate support systems Disclosure of HIV status
Income/Personal Finance Management Financial stability Ability to complete applications Has or needs a representative payee
Transportation Lacks access to transportation for medical and other necessary
appointments Ability to coordinate/access transportation
Nutrition Access to food Medical necessity
DEFINING THE SERVICE AREAS
16
17
GATHERING INFORMATION
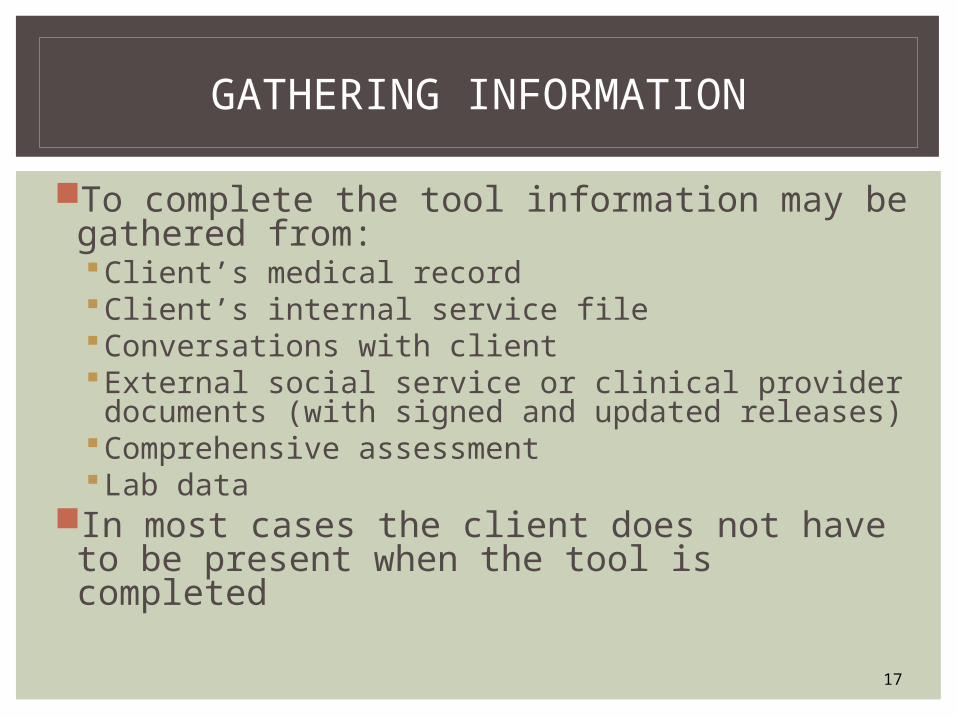
To complete the tool information may be gathered from:Client’s medical recordClient’s internal service fileConversations with client External social service or clinical provider documents (with signed and updated releases)
Comprehensive assessmentLab data
In most cases the client does not have to be present when the tool is completed

Based on information gathered from the previously listed sources check the boxes for all applicable criteria in each area of functioning and enter the number that corresponds to the level of need in the left column
USING THE TOOL
18
Current Health Status Acuity level:
Has detectable VL and CD4 below 200 and refuses ARVsHas current OI and is not being treated or refuses treatment Has been hospitalized in last 30 days Newly diagnosed within last six months and concurrently diagnosed with AIDS
Has detectable VL and low CD4 below 350 and refuses ARVs Has history of OI in last six months which are treated and client using prophylaxis (if indicated)Has been hospitalized in last six months Newly diagnosed within last six months; high CD4 (over 350)
Has detectable VL but is on ARVs Has no history of OIs in last six months or is on treatment for an OIHas had no hospitalizations in last six months
Is virally suppressedHas no history of OIs in last 12 monthsHas no history of hospitalizations in last 12 months
Area of Functioning
Intensive Need(3)
Moderate Need (2)
Basic Need (1)
Self Management (0)

Clients who meet criteria in two or more levels of need for any area of functioning are automatically assigned the number corresponding to the highest level of need.
USING THE TOOL
19
Current Health Status
Acuity level: 3
Has detectable VL and CD4 below 200 and refuses ARVsHas current OI and is not being treated or refuses treatmentHas been hospitalized in last 30 days Newly diagnosed within last six months and concurrently diagnosed with AIDS
Has detectable VL and low CD4 below 350 and refuses ARVs Has history of OI in last six months which are treated and client using prophylaxis (if indicated)Has been hospitalized in last six months Newly diagnosed within last six months; high CD4 (over 350)
Has detectable VL but is on ARVs Has no history of OIs in last six months or is on treatment for an OIHas had no hospitalizations in last six months
Is virally suppressedHas no history of OIs in last 12 monthsHas no history of hospitalizations in last 12 months
Area of Functioning
Intensive Need(3)
Moderate Need (2)
Basic Need (1)
Self Management (0)
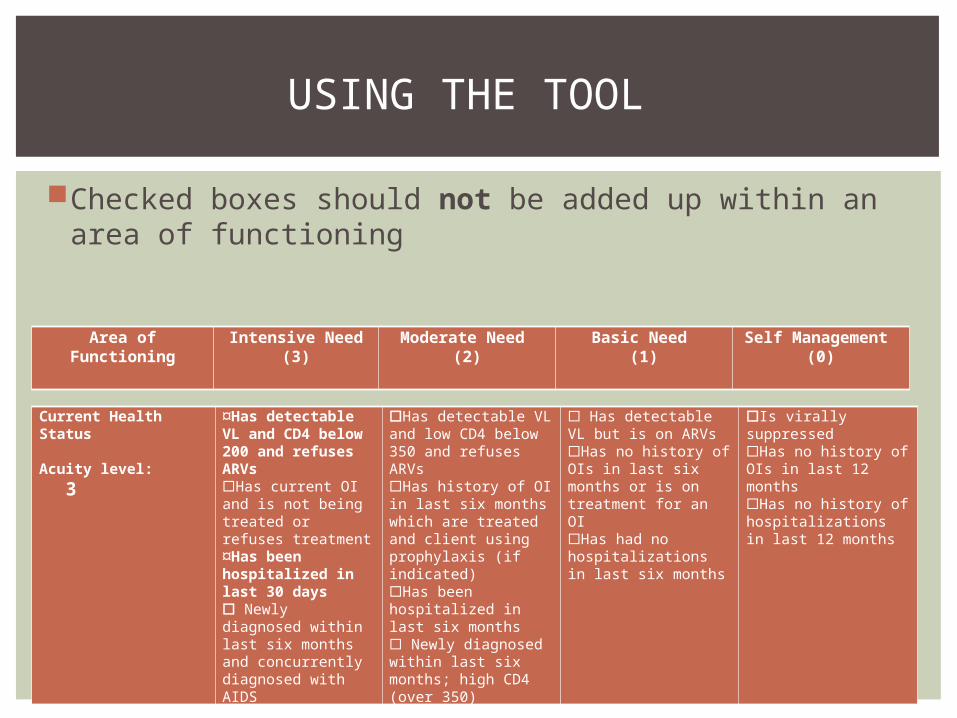
Checked boxes should not be added up within an area of functioning
USING THE TOOL
20
Current Health Status
Acuity level: 3
Has detectable VL and CD4 below 200 and refuses ARVsHas current OI and is not being treated or refuses treatmentHas been hospitalized in last 30 days Newly diagnosed within last six months and concurrently diagnosed with AIDS
Has detectable VL and low CD4 below 350 and refuses ARVs Has history of OI in last six months which are treated and client using prophylaxis (if indicated)Has been hospitalized in last six months Newly diagnosed within last six months; high CD4 (over 350)
Has detectable VL but is on ARVs Has no history of OIs in last six months or is on treatment for an OIHas had no hospitalizations in last six months
Is virally suppressedHas no history of OIs in last 12 monthsHas no history of hospitalizations in last 12 months
Area of Functioning
Intensive Need(3)
Moderate Need (2)
Basic Need (1)
Self Management (0)
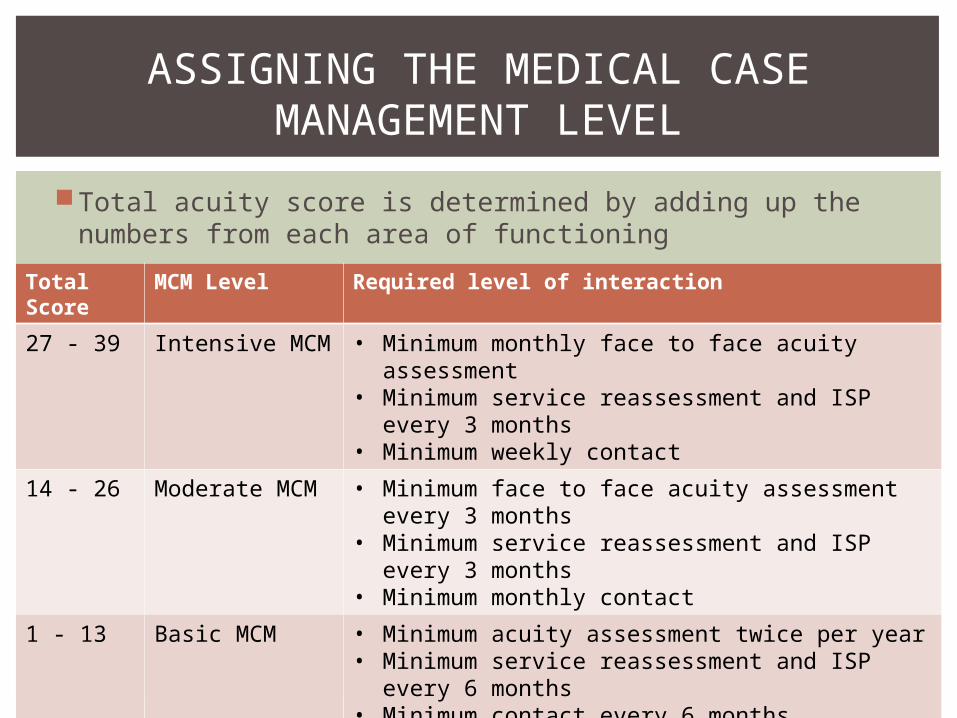
Total acuity score is determined by adding up the numbers from each area of functioning
ASSIGNING THE MEDICAL CASE MANAGEMENT LEVEL
21
Total Score
MCM Level Required level of interaction
27 - 39 Intensive MCM • Minimum monthly face to face acuity assessment
• Minimum service reassessment and ISP every 3 months
• Minimum weekly contact
14 - 26 Moderate MCM • Minimum face to face acuity assessment every 3 months
• Minimum service reassessment and ISP every 3 months
• Minimum monthly contact
1 - 13 Basic MCM • Minimum acuity assessment twice per year• Minimum service reassessment and ISP every 6
months• Minimum contact every 6 months
0 Self Management
• No required level of interaction
22
THE PILOT
Pilot will run from November 1, 2014 to April 30, 2015
Agency participation is not mandatory, however the pilot process is the mechanism to give feedback and input to the funders
At the end of the pilot BPHC and OHA will implement an acuity index which agencies will be expected to use
You’re the experts! We want a tool that works for you
Agencies must enroll a minimum of 20 clients
No more than ten clients who appear to be high need
At least five clients who appear to be low need
If possible agencies should enroll between one and five clients who are either newly diagnosed or new to the agency
Care team members should discuss the pilot and identify appropriate participants as soon as possible
PILOT PARTICIPANTS
23
Agencies with a client population less than 50 will negotiate an appropriate number of pilot participants with their program coordinator/contract manager
Agencies that enroll more than 20 must enroll 20 meeting the previously listed criteria, and may use any criteria they choose for selecting the additional clients
Agencies will explain selection process in a post-pilot survey
PILOT PARTICIPANTS
24
Pilot participants who are newly diagnosed or new to the clinic should have their acuity assessed as soon as possible to determine the MCM level
Pilot participants who are existing agency clients should have an initial acuity assessment the next time they meet with MCM staff (by November 20, 2014 at the latest)
Acuity tool should be administered at least twice during the course of the six month pilot
TIMELINE FOR USING THE TOOL
25

TABLE TALK
26

LUNCH!
27
For each pilot client, agencies must complete the Acuity Summary Sheet to be maintained in a paper file
During the six months from November 2014 to May 2015 BPHC and OHA staff will add a pilot check-in agenda item to the monthly call
From April – June 2015 BPHC and OHA staff (or their designees) will review all pilot participant charts using the Acuity Tool Client File Review form
At the end of the pilot a survey will be sent to all participating agencies
EVALUATION COMPONENTS
28

During the six month pilot all participants must have paper charts available for funder review with all appropriate documents maintained (including ISP and assessment tools)
Paper charts do not need to include non-service specific documents (e.g. grievance form, client responsibilities, etc)
Your contract manager or program coordinator will give you specifics
The chart review will include a review and comparison of the acuity tool, the ISP, the reassessment, and case notes
FUNDER CHART REVIEW
29
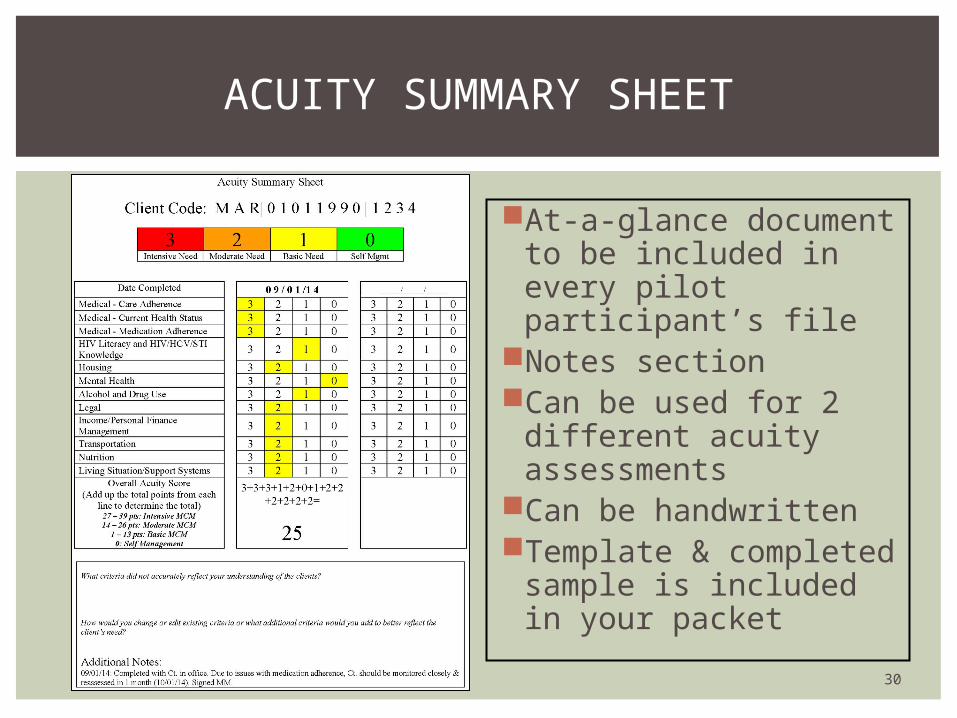
At-a-glance document to be included in every pilot participant’s file
Notes sectionCan be used for 2
different acuity assessments
Can be handwrittenTemplate & completed
sample is included in your packet
ACUITY SUMMARY SHEET
30
In addition to the acuity level for each area of functioning, each Acuity Summary sheet has the following questions:
What criteria did not accurately reflect your understanding of the client’s need?
How would you change or edit existing criteria or what additional criteria would you add to better reflect the client’s need?
GIVING INPUT AND FEEDBACK:ACCURACY OF THE TOOL
31
The post-pilot survey will include questions about the ease of use of the tool, suggestions for change, areas for improvement, etc.
Agencies are encouraged to contact their program coordinator or contract manager with any questions or concerns that come up during the six months
At the end of the six months agencies will be asked to submit copies of each pilot participant’s acuity tool and acuity summary sheets
GIVING INPUT AND FEEDBACK:IMPLEMENTATION
32

Read the case studies
Complete the acuity tool using the information given
Discuss with others at your table
ACUITY TOOL PRACTICE
33
Contact your program coordinator or contract manager by Friday October 24th to confirm your participation in the pilot
Contact your program coordinator or contract manager with any questions
CONTACT INFORMATION
34
Meet with your care team to review the tool, explain the pilot, and identify pilot participants
BPHC and MDPH will develop and distribute an FAQ
Start using the tool!
NEXT STEPS
35