Maternal-amniotic-fetal distribution of macrolide antibiotics following intravenous, intramuscular,...
8
BASIC SCIENCE: OBSTETRICS Maternal-amniotic-fetal distribution of macrolide antibiotics following intravenous, intramuscular, and intraamniotic administration in late pregnant sheep Jeffrey A. Keelan, PhD; Ilias Nitsos, PhD; Masatoshi Saito, MD, PhD; Gabrielle C. Musk, BVMS; Matthew W. Kemp, PhD; Matthew Timmins, PhD; Shaofu Li, BSc; Nobuo Yaegashi, MD, PhD; John P. Newnham, MD OBJECTIVE: The objective of the study was to explore the maternal-fe- tal pharmacokinetics of intraamniotic (IA), intravenous (IV), or intramus- cular (IM) administration of erythromycin or azithromycin in a pregnant sheep model. STUDY DESIGN: Pregnant ewes of 115-121 days’ gestation received a single maternal IV infusion (5 mg/kg over 60 min), a single IM injection, or a single IA injection (3.2 mg/kg fetal weight) of either erythromycin lactobionate or azithromycin. Maternal/fetal blood and amniotic fluid (AF) samples were collected across 48 h for macrolide assay by liquid chromatography and tandem mass spectrometry. RESULTS: Maternal administration achieved therapeutic maternal plasma macrolide concentrations (0.5 g/mL) with low concentra- tions in AF equivalent to less than 7% transfer; fetal plasma levels were even lower (1.5% transfer). The IA administration achieved therapeu- tic concentrations in AF and sustained for 48 h, with poor maternal-fetal transfer (1% maternal, 0.3% fetal). Modest pharmacokinetic dif- ferences were evident between erythromycin and azithromycin. CONCLUSION: Maternal macrolide administration achieves subthera- peutic concentrations in AF or fetal plasma, whereas a single IA injec- tion achieves therapeutic concentrations in AF but not in maternal-fetal circulations. Combined maternal and single IA administration of macro- lides may be a more effective regimen for treatment of intrauterine, but not fetal, infection. Key words: antibiotics, intrauterine infection, pharmacokinetics, sheep, ureaplasma Cite this article as: Keelan JA, Nitsos I, Saito M, et al. Maternal-amniotic-fetal distribution of macrolide antibiotics following intravenous, intramuscular, and intraamniotic administration in late pregnant sheep. Am J Obstet Gynecol 2011;204:546.e10-17. M acrolide antibiotics such as eryth- romycin and azithromycin are widely prescribed during pregnancy for the treatment of a variety of microbial infections; these drugs are perceived to be effective, well tolerated, and free of se- rious maternal and fetal side effects. 1-3 Erythromycin is a first-line antibiotic prescribed for the treatment of Chlamydia trochomatis and Group B streptococci in- fections and is the most frequently ad- ministered antibiotic for treatment of pre- mature prelabor rupture of membranes (PPROM) based on the findings of the ORACLE I trial. 4 Azithromycin, a second-generation macrolide, is less widely used in pregnancy, although it has a longer duration of action and half-life, greater tissue penetration, re- duced adverse effects, and a wider micro- bial coverage. Azithromycin is effective against many organisms of significance in pregnancy such as Staphylococci, Strepto- cocci, Chlamydia, Haemophilus, Legionella, Listeria, Nisseriae, Toxoplasma, Myco- plasma, and Plasmodium spp. Because of its preferential accumulation in tissues, it has improved efficacy against intracellular pathogens such as Mycoplasma and Urea- plasma spp. In light of the widely accepted role of intrauterine infection and inflammation in the aetiology of preterm labor and PPROM, antimicrobial therapy in preg- nancy has been evaluated with the goal of reducing rates of preterm birth and neo- natal morbidity and mortality. 2,5-7 A re- cent metaanalysis of maternal macrol- ide administration following PPROM found statistically significant reductions in chorioamnionitis, preterm birth, and neonatal morbidity. 8 However, antibi- otic treatment has been shown to have, at best, only modest benefits on preterm delivery rates and neonatal outcomes when administered to women at risk of preterm birth 2 or women presenting with preterm birth. 6-7,9 This relative lack of success is consist- ent with strong evidence that systemic From the School of Women’s and Infants’ Health (Drs Keelan, Nitsos, Kemp, and Newnham, Ms Musk, and Mr Li) and Metabolomics Australia, School of Biomedical, Biomolecular and Chemical Sciences (Dr Timmins), The University of Western Australia, Perth, Western Australia, Australia, and the Department of Obstetrics and Gynecology, Tohoku University, Sendai, Miyagi, Japan (Drs Saito and Yaegashi). Presented, in part, at the Annual Scientific Conference of the Society for Gynecologic Investigation, Miami Beach, FL, March 15-19th, 2011. Received Dec. 16, 2010; accepted Feb. 9, 2011. Reprints not available from the authors. This study was supported in part by the Women and Infants Research Foundation, Western Australia, and the National Health and Medical Research Council of Australia (project Grant APP1010315). 0002-9378/$36.00 • © 2011 Mosby, Inc. All rights reserved. • doi: 10.1016/j.ajog.2011.02.035 Research www. AJOG.org 546.e10 American Journal of Obstetrics & Gynecology JUNE 2011
-
Upload
jeffrey-a-keelan -
Category
Documents
-
view
225 -
download
0
Transcript of Maternal-amniotic-fetal distribution of macrolide antibiotics following intravenous, intramuscular,...

Research www.AJOG.org
BASIC SCIENCE: OBSTETRICS
Maternal-amniotic-fetal distribution of macrolide antibioticsfollowing intravenous, intramuscular, and intraamnioticadministration in late pregnant sheepJeffrey A. Keelan, PhD; Ilias Nitsos, PhD; Masatoshi Saito, MD, PhD; Gabrielle C. Musk, BVMS; Matthew W. Kemp, PhD;Matthew Timmins, PhD; Shaofu Li, BSc; Nobuo Yaegashi, MD, PhD; John P. Newnham, MD
OBJECTIVE: The objective of the study was to explore the maternal-fe-tal pharmacokinetics of intraamniotic (IA), intravenous (IV), or intramus-cular (IM) administration of erythromycin or azithromycin in a pregnantsheep model.
STUDY DESIGN: Pregnant ewes of 115-121 days’ gestation received asingle maternal IV infusion (5 mg/kg over 60 min), a single IM injection,or a single IA injection (3.2 mg/kg fetal weight) of either erythromycinlactobionate or azithromycin. Maternal/fetal blood and amniotic fluid(AF) samples were collected across 48 h for macrolide assay by liquidchromatography and tandem mass spectrometry.
RESULTS: Maternal administration achieved therapeutic maternalplasma macrolide concentrations (�0.5 �g/mL) with low concentra-
intraamniotic administration in late pregnant sheep. Am J Obstet Gynecol 2011;204:
0002-9378/$36.00 • © 2011 Mosby, Inc. All rights reserved. • doi: 10.1016
546.e10 American Journal of Obstetrics & Gynecology JUNE 2011
even lower (�1.5% transfer). The IA administration achieved therapeu-tic concentrations in AF and sustained for 48 h, with poor maternal-fetaltransfer (�1% maternal, �0.3% fetal). Modest pharmacokinetic dif-ferences were evident between erythromycin and azithromycin.
CONCLUSION: Maternal macrolide administration achieves subthera-peutic concentrations in AF or fetal plasma, whereas a single IA injec-tion achieves therapeutic concentrations in AF but not in maternal-fetalcirculations. Combined maternal and single IA administration of macro-lides may be a more effective regimen for treatment of intrauterine, butnot fetal, infection.
Key words: antibiotics, intrauterine infection, pharmacokinetics,
sheep, ureaplasma tions in AF equivalent to less than 7% transfer; fetal plasma levels wereCite this article as: Keelan JA, Nitsos I, Saito M, et al. Maternal-amniotic-fetal distribution of macrolide antibiotics following intravenous, intramuscular, and
546.e10-17.w
Macrolide antibiotics such as eryth-romycin and azithromycin are
widely prescribed during pregnancy forthe treatment of a variety of microbialinfections; these drugs are perceived tobe effective, well tolerated, and free of se-rious maternal and fetal side effects.1-3
Erythromycin is a first-line antibioticprescribed for the treatment of Chlamydiatrochomatis and Group B streptococci in-fections and is the most frequently ad-ministered antibiotic for treatment of pre-
From the School of Women’s and Infants’ HeMs Musk, and Mr Li) and Metabolomics AustChemical Sciences (Dr Timmins), The UniveAustralia, Australia, and the Department of OSendai, Miyagi, Japan (Drs Saito and Yaegashi).
Presented, in part, at the Annual Scientific ConfeInvestigation, Miami Beach, FL, March 15-19th,
Received Dec. 16, 2010; accepted Feb. 9, 2011
Reprints not available from the authors.
This study was supported in part by the WomenAustralia, and the National Health and Medical RAPP1010315).
mature prelabor rupture of membranes(PPROM) based on the findings of theORACLE I trial.4
Azithromycin, a second-generationmacrolide, is less widely used in pregnancy,although it has a longer duration of actionand half-life, greater tissue penetration, re-duced adverse effects, and a wider micro-bial coverage. Azithromycin is effectiveagainst many organisms of significance inpregnancy such as Staphylococci, Strepto-cocci, Chlamydia, Haemophilus, Legionella,
(Drs Keelan, Nitsos, Kemp, and Newnham,ia, School of Biomedical, Biomolecular and
of Western Australia, Perth, Westerntrics and Gynecology, Tohoku University,
ce of the Society for Gynecologic1.
Infants Research Foundation, Westernarch Council of Australia (project Grant
/j.ajog.2011.02.035
Listeria, Nisseriae, Toxoplasma, Myco-plasma, and Plasmodium spp. Because of itspreferential accumulation in tissues, it hasimproved efficacy against intracellularpathogens such as Mycoplasma and Urea-plasma spp.
In light of the widely accepted role ofintrauterine infection and inflammationin the aetiology of preterm labor andPPROM, antimicrobial therapy in preg-nancy has been evaluated with the goal ofreducing rates of preterm birth and neo-natal morbidity and mortality.2,5-7 A re-cent metaanalysis of maternal macrol-ide administration following PPROMfound statistically significant reductionsin chorioamnionitis, preterm birth, andneonatal morbidity.8 However, antibi-otic treatment has been shown to have, atbest, only modest benefits on pretermdelivery rates and neonatal outcomeswhen administered to women at risk ofpreterm birth2 or women presenting
ith preterm birth.6-7,9
This relative lack of success is consist-
althral
rsitybste
ren201
.
andese
ent with strong evidence that systemic

pi
cr
bahompa
m2
a
www.AJOG.org Basic Science: Obstetrics Research
JUNE 2011 American
maternal erythromycin administration islargely ineffective in eradicating intrauter-ine Ureaplasma infection,10 although re-
orts of more successful outcomes do ex-st.11,12 Ureaplasmas and Mycoplasmas are
the microorganisms most frequently iso-lated from human amniotic fluid (AF)13
and the placenta14-16 and are strongly asso-iated with an intrauterine inflammatoryesponse17,18 and preterm birth.19 Accord-
ingly, their eradication from the amnioticcavity is likely an essential prerequisite fordevelopment of an effective antimicrobialregimen. The efficacy of an intraamniotic(IA) route of antibiotic administration hasnot yet been evaluated and reported.
In our experimental sheep model ofintrauterine Ureaplasma colonization dur-ing pregnancy, we have recently shownthat maternal intramuscular (IM) eryth-romycin administration does not eradi-cate Ureaplasma infection from the am-niotic fluid, chorioamnion, umbilicalcord, or the fetal lung.20 However, the
iodistribution of macrolide antibioticsdministered maternally in this modelas not yet been described. The inabilityf maternal systemic erythromycin ad-inistration to combat intrauterine Urea-
lasma colonization is likely to be attribut-ble to poor transplacental passage.
In the perfused human placentaodel, the transfer rate of macrolides is
-4%.21 Sampling and analysis of mater-nal and fetal plasma at the time of thera-peutic abortion22 or elective cesareansection at term23 suggests that the degreeof erythromycin passage to the fetus isboth low and inconsistent. Transplacen-tal passage of erythromycin may be lim-ited by the presence of drug efflux pumpsin the placenta and fetal membranes.24,25
However, a small study performed inpregnant women at term reported thatthe transfer of macrolides from maternalcirculation to amniotic fluid was consid-erable (reaching 30-50% of maternalplasma concentrations) and that the pla-centa accumulated antibiotics and main-tained high concentrations for severaldays after administration.26
The aim of the present study, there-fore, was to compare the pharmacoki-netics of maternal vs IA administrationof erythromycin and azithromycin in
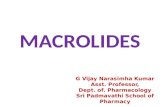
FIGURE 1Erythromycin concentrations in maternal plasma, AF, andfetal plasma after maternal IV, IM, or IA administration
Concentrations of erythromycin in maternal plasma, AF, and fetal plasma following maternal A, IVadministration, B, IM administration, or C, IA administration. Data shown are the mean � SD (n � 5nimals).
AF, amniotic fluid; IA, intraamniotic; IM, intramuscular; IV, intravenous.
Keelan. Macrolide pharmacokinetics in pregnancy. Am J Obstet Gynecol 2011.
the pregnant ovine model to deter-
Journal of Obstetrics & Gynecology 546.e11

tnwfl
wl
ckonoosm(
t
Research Basic Science: Obstetrics www.AJOG.org
mine the best antibiotic and route ofadministration for pharmacologicaltreatment of intrauterine Ureaplasmainfection.
MATERIALS AND METHODSSurgical procedures andantibiotic administrationAll experimental procedures describedin this study were approved by the Ani-mal Ethics Committee of the Universityof Western Australia. Pregnant ewesbearing single fetuses underwent asepticsurgery at 110 days’ gestation (term �150 days) for maternal and fetal cathe-terization. Ewes were premedicated withIM acetylpromazine (0.02 mg/kg) andbuprenorphine (0.01 mg/kg, IM) ap-proximately 30 minutes prior to induc-tion of anesthesia with intravenous (IV)midazolam (0.25 mg/kg) and ketamine(5 mg/kg).
After induction of anesthesia, the tra-chea was intubated, and anesthesia wasmaintained with 1.5-2% isoflurane in100% O2 delivered with intermittent pos-itive pressure ventilation. Using aseptictechniques, a paramedian abdominal inci-sion was made, the pregnant uterus wasidentified, and the fetal head palpated andthen delivered through a uterine incision.Polyvinyl catheters containing heparinizedsaline (50 IU/mL) were inserted into a fetalcarotid artery and amniotic fluid cavity.The fetus was administered antibiotics(100 mg engemycin [oxytetracyclin], IM)and returned to the uterus. After closure ofthe uterine incision, catheters were exteri-orised through a small incision in the ewe’sflank and the abdominal incision wasclosed in 2 layers.
Polyvinyl catheters containing hepa-rinized saline (50 IU/mL) were then in-serted into the maternal carotid arteryand jugular vein. The catheters were se-cured to the maternal skin in 3 places andpositioned behind the ewe’s neck. Theewe was administered antibiotics (400mg engemycin, IM) and a fentanyl patch(Duragesic 75 �g/h; Alza Corp., Moun-ain View, CA) was applied to the mater-al skin for postsurgery analgesia. Ewesere allowed to recover in individual
oor pens with free access to food and e546.e12 American Journal of Obstetrics & Gyneco
ater and were monitored daily for ateast 5 days before experimentation.
At 115 days’ gestation, chronicallyatheterized pregnant ewes (53.5-64.4g) were randomly selected to receivene of the following: (1) a single mater-al IV infusion of erythromycin lactobi-nate (5 mg/kg maternal weight; n � 5)ver 60 minutes in 100 mL of saline; (2)ingle maternal IV infusion of azithro-
ycin (5 mg/kg maternal weight, n � 5);3) a single maternal IM injection of
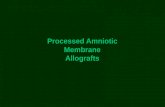
FIGURE 2Azithromycin concentrations in mafetal plasma after maternal IV or IA
Concentrations of azithromycin in maternal plasadministration or B, IA administration. Data showAF, amniotic fluid; IA, intraamniotic; IV, intravenous.
Keelan. Macrolide pharmacokinetics in pregnancy. Am J Obs
rythromycin lactobionate (5 mg/kg ma-
logy JUNE 2011
ernal weight, n � 5) (note: an IM azi-thromycin administration arm was notincorporated because clinically this anti-biotic is not given IM); or a single IA in-jection of (4) erythromycin lactobionateor (5) azithromycin (3.2 mg/kg esti-mated fetal weight, n � 5).
At this gestational age, fetal weight wasestimated to be 2.4 kg and amniotic fluidvolume 250 mL. Maternal (5 mL) and fetal(2 mL) arterial blood and amniotic fluid (2mL) samples were collected into heparin-
nal plasma, AF, anddministration
, AF, and fetal plasma following maternal A, IVre the mean � SD (n � 5 animals).
ynecol 2011.
tera
man a
tet G
ized tubes 15 minutes before and immedi-

P
pa
wa
iuatAjSpl1twr
mac(5maTs
trscctcraddtb
www.AJOG.org Basic Science: Obstetrics Research
ately prior to the administration of themacrolide antibiotics as described in thepreceding text; after the infusion/injec-tions, samples were taken at 1, 2, 4, 8, 12,24, and 48 hours. Arterial PO2 (PaO2),
CO2 (PaCO2), O2 saturation (SaO2), pH(pHa), and electrolytes were measuredwith a RapidLab 1265 blood gas analyzer(Siemens, Munich, Germany). Fetal andmaternal plasma and amniotic fluid sam-
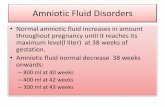
FIGURE 3Macrolide pharmacokinetic profilesor AF following maternal or IA adm
Comparison of macrolide pharmacokinetic profileor IA administration. Concentrations in other comshown. Data shown are the mean � SD (n � 5AF, amniotic fluid; IA, intraamniotic.
Keelan. Macrolide pharmacokinetics in pregnancy. Am J Obs
ples were collected and stored at �80°C
rior to quantification of the macrolidentibiotic concentrations.
Sample extraction and analysisCalibration standards, consisting of a se-ries of 5 10-fold serial dilutions of eryth-romycin and azithromycin antibiotics(4000 to 0.04 ng/mL), ovine plasma/am-niotic fluid samples, and quality controls(all 0.1 mL) were extracted with 300 �L
maternal plasmastration
A, maternal plasma or B, AF following maternalrtments are not visible in these plots so are notmals).
ynecol 2011.
methanol by vortexing for 30 seconds
JUNE 2011 American
and mixing on an orbital shaker for 10minutes after addition of internal stan-dard (0.5 ng roxithromycin). Qualitycontrol samples (200 ng/mL in plasma oramniotic fluid) were run with each assaybatch.
After centrifugation (3200 � g, 20minutes), extracts were transferred toglass tubes and dried with gentle heating(30oC) under nitrogen. Dried extracts
ere resuspended in 100 �L methanolnd filtered through 0.22 �m cellulose
acetate centrifuge tube filters (CorningInc, Corning, NY); 0.5 �L was injectednto an Agilent 1200-series capillary liq-id chromatography system coupled ton Agilent 6340 Ion Trap mass spec-rometer (Agilent Technologies, Palolto, CA). Methanol blanks were in-
ected after every 11 sample injections.eparation was achieved using reverse-hase chromatography on a 3.5 �m Agi-
ent Eclipse XDB-C18 column (2.1 �50 mm); a gradient of 0-75% acetoni-rile in 0.1% formic acid over 7 minutesas employed, followed by a 1 minute
ecovery wash at 100 % acetonitrile.Macrolide MRM transitions wereonitored in positive mode as follows:
zithromycin (748.9-591.0), erythromy-in (733.9-576.6), and roxithromycin837.0-679.0); elution times were 2.9,.1, and 5.9 minutes, respectively. Allass to charge ratio peaks were manu-
lly integrated using 6300 Series Ionrap liquid chromatography and mass
pectrometry software 6.1.Integrated signals from samples, con-
rols, and standards were blank cor-ected, expressed as a ratio of the internaltandard, and log transformed. A linearurve fit was applied to the calibrationurve and this used to derive the concen-ration of the samples. Extraction effi-iency for each sample was calculated byeference to the signal from a givenmount of roxithromycin internal stan-ard extracted and processed as per stan-ards and samples. The limit of quanti-ation was defined as 5 SD above theackground signal.
Statistical and pharmacokineticanalysisMacrolide concentration data from 5 an-
inini
s inpa
ani
tet G
imals per time point were grouped and
Journal of Obstetrics & Gynecology 546.e13

cpIaa4t(
ttmtg2h
tti
Ancel
cl
lto
bst
Research Basic Science: Obstetrics www.AJOG.org
the mean and SDs calculated. These datawere subject to pharmacokinetic analysisusing the Microsoft Excel add-in pro-gramme PKSolver.27 Maternal pharma-okinetic data were fitted using a 2 com-artment model, whereas the data fromA administration were best described by
noncompartmental model. Plasmand amniotic fluid control values from-6 assays were determined to derivehe interassay coefficient of variationCV).
RESULTSThe azithromycin and erythromycin as-says had a limit of quantitation of lessthan 0.1 and less than 0.3 �g/L, respec-tively. Mean extraction efficiency was70.75%. Interassay CVs for erythromy-cin in maternal plasma and AF controlsamples were 14.7% and 19.4%, respec-tively (n � 6). Azithromycin interassayCVs for plasma and AF samples (n � 4)were 6.2% and 5.7%, respectively.
The biodistribution profiles of themacrolide antibiotics in the 3 compart-ments (maternal plasma, AF, and fetalplasma) following IV, IM, and IA ad-ministration are shown in Figures 1and 2 using a log concentration axis toallow data from all compartments to bedisplayed on the same graph. Figure 3compares the profiles achieved of the 2antibiotics on a linear axis. The phar-macokinetic parameters for IM and IVmaternal macrolide administration arelisted in Table 1, whereas the parame-ters for IA administration are shown inTable 2.
Erythromycin pharmacokineticsMaternal administration of erythromy-cin achieved peak maternal plasma anti-biotic concentrations within an hour, ac-companied by markedly attenuated risein AF and fetal plasma concentrations(Figure 1, A and B). Delivery by IV in-fusion resulted in a greater maternalplasma maximum concentration (Cmax)han IM administration, but concentra-ions declined less rapidly with IM ad-
inistration, such that the area underhe curve (AUC) was considerablyreater with IM administration (3.97 vs.227 �g/mL per hour) and the initial
alf-life (t½�) was approximately 5 e546.e14 American Journal of Obstetrics & Gyneco
times longer (2.7 hours vs. 0.35 hours)(Table 1 and Figure 3, A). Maternalplasma concentrations following IV ad-ministration exceeded the estimated min-imal inhibitory concentration (MIC) forUreaplasma (0.5 �g/mL) only at the 1 hourime point, whereas with IM administra-ion MIC levels were sustained for approx-mately 4 hours (Figure 3, A).
Transfer from maternal circulation toF was negligible (�1% at peak mater-al levels), failing to achieve therapeuticoncentrations at any time point. Thextent of transfer to AF was greatest fol-owing IV administration, reaching lev-
TABLE 1Maternal plasma macrolide pharm
Parameter UnitErythrIM
A �g/mL 1.15...................................................................................................................
Alpha 1/hour 0.25...................................................................................................................
B �g/mL 0.04...................................................................................................................
Beta 1/hour 0.25...................................................................................................................
Dose mg 284.9...................................................................................................................
k10 1/hour 0.25...................................................................................................................
k12 1/hour 0.00...................................................................................................................
k21 1/hour 0.25...................................................................................................................
t� Hour 2.67...................................................................................................................
t� Hour 2.67...................................................................................................................
V/F (mg)/(�g/mL) 276.8...................................................................................................................
CL/F (mg)/(�g/mL)per hour
71.8
...................................................................................................................
V2/F (mg)/(�g/mL) 0.0...................................................................................................................
CL2/F (mg)/(�g/mL)per hour
0.0
...................................................................................................................
Tmax Hour 1.21...................................................................................................................
Cmax �g/mL 0.75...................................................................................................................
AUC0-t �g/mL per hour 3.97...................................................................................................................
AUC0-inf �g/mL per hour 3.97...................................................................................................................
AUMC �g/mL perhour2
17.41
...................................................................................................................
MRT Hour 4.39...................................................................................................................
Vss �g/(ng/mL)...................................................................................................................
Two compartment analysis of maternal plasma macrolide phmg/kg maternal weight).AUC, area under the curve; AUMC, area under the first mometration reached; F, bioavailability (fraction of dose absorbed)apparent volume of distribution; V2/F, apparent peripheral vol
Keelan. Macrolide pharmacokinetics in pregnancy. Am J O
ls of 0.025 �g/mL at 2 hours, although m
logy JUNE 2011
with IM administration the rise in AFlevels was more gradual and sustained(0.011 �g/mL at 24 hours). Fetal plasmaoncentrations were even lower than AFevels (less than 0.004 �g/mL), repre-
senting less than 1% of maternal concen-trations during the first 8 hours of theexperiment.
Intraamniotic erythromycin adminis-tration (Figure 1, C) achieved muchhigher concentrations than maternal ad-ministration (Cmax 8.7 �g/mL) with a faronger half-life (t½� 27.6 h). As a result,he AUC was 100-fold greater than thatbserved in maternal plasma following
kinetic parameters
ycin Erythromycin AzithromycinIV IV
3.075 1.218..................................................................................................................
1.964 2.284..................................................................................................................
0.247 0.154..................................................................................................................
0.374 0.0269..................................................................................................................
282.9 273.5..................................................................................................................
1.4916 0.2187..................................................................................................................
0.3540 1.8112..................................................................................................................
0.4921 0.2806..................................................................................................................
0.3529 0.3035..................................................................................................................
1.8546 25.797..................................................................................................................
85.2 199.3..................................................................................................................
127.0 43.6
..................................................................................................................
61.2 1286.2..................................................................................................................
30.1 360.9
..................................................................................................................
1.0..................................................................................................................
1.552 0.631..................................................................................................................
2.227 4.674..................................................................................................................
2.227 6.277..................................................................................................................
2.567 213,990
..................................................................................................................
1.15 34.1..................................................................................................................
146.4 1485.5..................................................................................................................
cokinetic parameters following IV or IM administration (5
rve; CL/F, apparent clearance; Cmax, maximum concen-T, mean residence time; Tmax, timepoint at Cmax; V/F,of distribution; Vss, volume of distribution at steady state.
et Gynecol 2011.
aco
om
1.........
9.........
2.........
9.........
.........
93.........
00.........
92.........
36.........
42.........
.........
.........
.........
.........
8.........
1.........
0.........
0.........
3
.........
.........
.........
arma
nt cu; MRume
aternal IV administration (Table 2),

itmr
atMt(
s
hmt
tFges1
nU
nomps
bst
www.AJOG.org Basic Science: Obstetrics Research
and therapeutic concentrations weremaintained in AF for at least 48 hoursafter injection (Figure 3, B). The extentof transfer from AF to fetal plasma wasvery poor, however, with peak levels (ap-proximately 0.017 �g/mL) at 8 h afternjection well below therapeutic concen-rations (Figure 1, C). Concentrations in
aternal plasma were even lower, barelyeaching 0.001 �g/mL.
Azithromycin pharmacokineticsAzithromycin pharmacokinetic profiles(Figure 2) were broadly similar to thoseof erythromycin, although there weresome differences (Figure 3). MaternalIV administration achieved transient (1hour) therapeutic concentrations (�0.5�g/mL) in maternal plasma. Apprecia-ble levels were subsequently measureablein AF and increased with time, reaching0.036 �g/mL at 24 hours, equivalent topproximately 50% of maternal concen-rations at that time point (Figure 2, A).
uch lower azithromycin concentra-ions were measured in fetal plasma
TABLE 2Amniotic fluid macrolide pharmaco
Parameter Unit
Dose mg...................................................................................................................
Lambda_z 1/hour...................................................................................................................
t hour...................................................................................................................
Clast obs/Cmax...................................................................................................................
Vzobs (mg)/(�g/mL)...................................................................................................................
Clobs (mg)/(�g/mL) per hour...................................................................................................................
Tmax hour...................................................................................................................
Cmax �g/mL...................................................................................................................
C0 �g/mL...................................................................................................................
AUC0-t �g/mL per hour...................................................................................................................
AUC0-inf_obs �g/mL per hour...................................................................................................................
AUMC0-inf_obs �g/mL per hour2
...................................................................................................................
MRT0-inf_obs hour...................................................................................................................
Vssobs (�g)/(ng/mL)...................................................................................................................
Noncompartmental analysis of AF macrolide pharmacokineticAUC, area under the curve; AUMC, area under the first momconcentration; C0, concentration at time zero; MRT, mean rvolume of distribution at steady state; Vz, volume of distributio
Keelan. Macrolide pharmacokinetics in pregnancy. Am J O
�0.002 �g/mL).
The IA azithromycin injection re-ulted in extremely high AF levels (�18
�g/mL), which declined steadily withtime (t½� 17.5 hours); surprisingly, therate of clearance of azithromycin fromAF was faster than that of erythromycin(Table 2 and Figure 3, B), although theAUCs were fairly similar because of thehigher starting concentrations of azi-thromycin (Table 2). AF-administeredazithromycin appeared to show a muchgreater degree of transfer to maternalplasma than fetal plasma (approximately100-fold) in contrast to the IA erythro-mycin pharmacokinetic profile (Figure2). Concentrations of azithromycin inmaternal blood equilibrated at around0.03-0.04 �g/mL for much of the first 12
ours after IA administration (approxi-ately 30% of AF levels), whereas in fe-
al blood, levels did not exceed 0.004�g/mL.
The half-life of azithromycin in AFwas less than that of erythromycin, 17.5vs 27.6 hours (Table 2), such that by 48hours after injection, the levels of the 2
etic parameters
Erythromycin AzithromycinIA IA
7.68 7.68..................................................................................................................
0.0251 0.0397..................................................................................................................
27.57 17.46..................................................................................................................
0.2595 0.1247..................................................................................................................
1.00 0.53..................................................................................................................
0.03 0.02..................................................................................................................
1 1..................................................................................................................
8.690 18.930..................................................................................................................
0.0001 0.0553..................................................................................................................
216.6 309.8..................................................................................................................
306.3 369.3..................................................................................................................
11799.3 9245.5..................................................................................................................
38.5 25.03..................................................................................................................
1.0 0.52..................................................................................................................
r IA bolus injection (3.2 mg/kg fetal weight).curve; C, concentration; Cl, clearance; Cmax, maximumnce time; Tmax, timepoint at Cmax; Vss[obs], observedring terminal phase.
et Gynecol 2011.
antibiotics were similar despite the larger
JUNE 2011 American
Cmax values at 1 hour achieved with azi-hromycin administration (Table 2 andigure 3, B). Azithromycin had a farreater accumulation in tissues thanrythromycin as reflected by their re-pective volumes of distribution (Vss):485 vs 147 �g/(ng/mL).
COMMENTTo effectively eradicate an intrauterineinfection, administration of antibioticsmust achieve therapeutic concentrationswithin the amniotic, maternal, and fetalcompartments. The MIC for erythromy-cin/azithromycin ranges from 0.01 togreater than 100 �g/mL according to or-ganism and method of determination; aconcentration of about 0.5-1 �g/mL is
eeded to achieve a MIC for nonresistantreaplasma spp.28
In the present study, although thera-peutic macrolide concentrations werereached briefly in maternal plasma fol-lowing maternal IM or IV administra-tion, neither route achieved effectiveconcentrations in AF or fetal plasma.This supports findings from severalstudies in humans that suggest that theextent of transfer of macrolides frommaternal to fetal plasma is low.21,26
Passive diffusion of molecules greaterthan 500 Daltons across the placenta isknown to be minimal (macrolides havea molecular weight of �700 Daltons);moreover, the placenta expresses a num-ber of active efflux pumps, at least oneof which recognizes erythromycin andwould likely act to minimize uptake andtransfer across the placenta.25 Although
o studies have been carried out to daten transfer of macrolides across the fetalembranes, we have shown that efflux
roteins are also expressed in these tis-ues24 and would predict that rates of
transfer from maternal blood to AF andvice versa would also be low.
The low levels of macrolides in the fe-tal circulation after IA treatment sug-gests that these antibiotics are poorly ab-sorbed by the immature fetal gut29
because the fetus swallows AF in largeamounts and macrolide concentrationswere relatively high for an extended pe-riod of time after IA delivery. This repre-
kin
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
s afteent
esiden du
sents a significant hurdle to achieving
Journal of Obstetrics & Gynecology 546.e15

sei
o0
ascprtAt
ddliobsmcc
vafHvspi
Research Basic Science: Obstetrics www.AJOG.org
therapeutic fetal antibiotic levels. It re-mains to be explored whether fetal gutabsorption may be improved in utero(eg, by hormone treatment).
Previous data exist on macrolidepharmacokinetics from studies in bothpregnant women30 and nonpregnantheep.31 Goudah et al,31 studying IVrythromycin administration to lactat-ng, nonpregnant ewes, reported a t½� of
0.4 hour, t½� of 4.5 hours, and an AUCf 7.91 �g/mL per hour. Our data (t½� of.35 hours, t½� of 1.85 hours, AUC 2.23
�g/mL per hour), suggest that maternalerythromycin clearance is increased inpregnancy, as might be predicted.
Salman et al30 recently presented dataon azithromycin pharmacokinetics afteroral administration in pregnant women(t½� of 0.88 hours, t½� of 20.7 hours,AUC 28.7 �g/mL per hour). Our com-parable data (t½� of 0.30 hours, t½� of25.8 hours, AUC 6.28 �g/mL per hour)re suggestive of reduced maternal expo-ure in the pregnant sheep due to in-reased clearance. Although there are norior reports of erythromycin clearanceates from AF, Ramsey et al26 reportedhat concentrations of azithromycin inF following maternal oral administra-
ion reached approximately 150 �g/mLand steadily declined, with a similar con-centration profile to that shown in Fig-ure 3, B. Hence, although there is notcomplete agreement between the phar-macokinetic data from all 3 studies, thedata are reasonably consistent with re-spect to overall picture.
Erythromycin and azithromycin havebeen reported to cross the placenta withsimilarly low levels of efficiency.21 Our
ata agree and would suggest that anyifferences between the 2 are minor and
acking biological significance. However,t is possible that the increased transferf azithromycin across the fetal mem-ranes into maternal plasma might haveome clinical advantages. We confirmed
any previous findings that azithromy-in has a longer half-life than erythromy-in in maternal plasma (25.7 vs 1.9 h)32
and also that azithromycin had a 10-foldgreater degree of tissue accumulationthan erythromycin. However, we unex-pectedly found that erythromycin has
the longer residence time in amniotic546.e16 American Journal of Obstetrics & Gyneco
fluid (27.6 vs 17.5 h), which could reflectenhanced uptake of azithromycin intointrauterine tissues and/or increasedtransmembrane transfer to maternalplasma.
In light of the minor pharmacokineticdifferences between the 2 macrolides, wewould propose that azithromycin ad-ministration should have therapeuticadvantages over erythromycin in thepresent context because of its wider mi-crobial coverage, more extensive tissueuptake characteristics and improved sideeffect profile.
Although the ovine placenta differsstructurally from the human placenta ina number of important ways,33 the preg-nant ewe remains a useful model to studyplacental function/transport and fetalgrowth and development.34 Our datasuggest that maternal administration ofmacrolides is unlikely to be effective indelivering antibiotics at therapeutic con-centrations to the fetus or AF (the site ofprimary infection). This is a likely expla-nation for the limited efficacy of mater-nal macrolide therapy in treating intra-uterine and fetal infection.
Importantly, our data also show thatthe IA route of administration exhibits avery different pharmacokinetic profilefrom maternal IV or IM administration,with amniotic concentrations stayingabove the MIC for at least 2 days after abolus injection. Clinically these findingsare important and encouraging becausethey suggest that a single IA injection of amacrolide antibiotic could be effective ineradicating an IA infection of a suscepti-ble organism such as Ureaplasma par-um. Ideally, IA injection would alsochieve effective concentrations in theetal circulation and maternal blood.
owever, our findings suggest that this isery unlikely, at least for a relatively re-istant organism such as Ureaplasmaarvum (the MIC for other microorgan-sms can be as low as 10-30 ng/mL26).
The transfer of macrolides out of AF ap-pears to be very inefficient, particularly inthe maternal direction, although this doeshave the benefit of extending the residencetime. As a consequence, we postulate thatto achieve therapeutic concentrations inmaternal and amniotic compartments, a
combination of maternal and IA adminis-logy JUNE 2011
tration will be necessary. Such a regimenshould eradicate the organisms from ma-ternal blood and AF and also deliver theantibiotic to both faces of the fetal mem-branes to prevent reinfection from reser-voirs within the membranes. However, al-though some antibiotic will reach fetalplasma via a combined maternal-amnioticdelivery approach, such a regimen wouldbe unlikely to achieve concentrations suf-ficient to effectively treat fetal infection.
Further research is required to deter-mine whether attainment of therapeuticmacrolide levels in the mother and AF(but not the fetus) is effective in treatingintrauterine infection at early gestationalages when secondary prevention of pre-term labor is feasible. Alternative treat-ment strategies need to be devised to im-prove fetal macrolide delivery; the sheepmodel is ideal for this purpose. Success-fully addressing these issues should leadto the development of protocols for theeffective treatment of intrauterine infec-tion and prevention of preterm birth. f
ACKNOWLEDGMENTSThe assistance of the staff of the Large AnimalFacility (The University of Western Australia) andour commercial sheep suppliers, Sara and An-drew Ritchie (Darkan, Western Australia) aregratefully acknowledged.
REFERENCES1. Sarkar M, Woodland C, Koren G, EinarsonAR. Pregnancy outcome following gestationalexposure to azithromycin. BMC PregnancyChildbirth 2006;6:18.2. Morency AM, Bujold E. The effect of second-trimester antibiotic therapy on the rate of pre-term birth. J Obstet Gynaecol Can 2007;29:35-44.3. Mylonas I. Antibiotic chemotherapy duringpregnancy and lactation period: aspects forconsideration. Arch Gynecol Obstet 2011;283:7-18.4. Kenyon SL, Taylor DJ, Tarnow-Mordi W.Broad-spectrum antibiotics for preterm, prela-bour rupture of fetal membranes: the ORACLE Irandomised trial. ORACLE Collaborative Group.Lancet 2001;357:979-88.5. Iams JD, Papatsonis DN, van Geijn HP, et al.The epidemiology of preterm birth. Clin Perina-tol 2003;30:651-64.6. McDonald HM, Brocklehurst P, Gordon A.Antibiotics for treating bacterial vaginosis inpregnancy. Cochrane Database Syst Rev 2007:CD000262.7. Romero R, Espinoza J, Chaiworapongsa T, et
al. Infection and prematurity and the role of pre-
www.AJOG.org Basic Science: Obstetrics Research
ventive strategies. Semin Neonatol 2002;7:259-74.8. Kenyon S, Boulvain M, Neilson JP. Antibiot-ics for preterm rupture of membranes. Co-chrane Database Syst Rev 2010;8:CD001058.9. Lamont RF, Jaggat AN. Emerging drug ther-apies for preventing spontaneous preterm laborand preterm birth. Expert Opin Investig Drugs2007;16:337-45.10. McDonald H, Brocklehurst P, Parsons J.Antibiotics for treating bacterial vaginosis inpregnancy. Cochrane Database Syst Rev 2005:CD000262.11. Mazor M, Chaim W, Horowitz S, LeibermanJR, Glezerman M. Successful treatment of pre-term labour by eradication of Ureaplasma urea-lyticum with erythromycin. Arch Gynecol Obstet1993;253:215-8.12. Smorgick N, Frenkel E, Zaidenstein R, Laz-arovitch T, Sherman DJ. Antibiotic treatment ofintra-amniotic infection with Ureaplasma urea-lyticum. A case report and literature review. Fe-tal Diagn Ther 2007;22:90-3.13. Maxwell NC, Davies LP, Kotecha S. Ante-natal infection and inflammation: what’s new?Curr Opin Infect Dis 2006;19:253-8.14. Kundsin RB, Driscoll SG, Monson RR, YehC, Biano SA, Cochran WD. Association of Urea-plasma urealyticum in the placenta with perina-tal morbidity and mortality. N Engl J Med1984;310:941-5.15. Kundsin RB, Leviton A, Allred EN, PoulinSA. Ureaplasma urealyticum infection of theplacenta in pregnancies that ended prema-turely. Obstet Gynecol 1996;87:122-7.16. Knox CL, Cave DG, Farrell DJ, EastmentHT, Timms P. The role of Ureaplasma urealyti-cum in adverse pregnancy outcome. Aust N Z J
Obstet Gynaecol 1997;37:45-51.17. Jacobsson B, Aaltonen R, Rantakokko-Jalava K, Morken NH, Alanen A. Quantifica-tion of Ureaplasma urealyticum DNA in theamniotic fluid from patients in PTL andpPROM and its relation to inflammatory cyto-kine levels. Acta Obstet Gynecol Scand2009;88:63-70.18. Aaltonen R, Heikkinen J, Vahlberg T, Jen-sen JS, Alanen A. Local inflammatory responsein choriodecidua induced by Ureaplasma urea-lyticum. BJOG 2007;114:1432-5.19. Goldenberg RL, Hauth JC, Andrews WW.Intrauterine infection and preterm delivery.N Engl J Med 2000;342:1500-7.20. Dando SJ, Nitsos I, Newnham JP, Jobe AH,Moss TJ, Knox CL. Maternal administration oferythromycin fails to eradicate intrauterine urea-plasma infection in an ovine model. Biol Reprod2010;83:616-22.21. Heikkinen T, Laine K, Neuvonen PJ, EkbladU. The transplacental transfer of the macrolideantibiotics erythromycin, roxithromycin and azi-thromycin. BJOG 2000;107:770-5.22. Kiefer L, Rubin A, McCoy JB, Foltz EL. Theplacental transfer of erythomycin. Am J ObstetGynecol 1955;69:174-7.23. Philipson A, Sabath LD, Charles D. Trans-placental passage of erythromycin and clinda-mycin. N Engl J Med 1973;288:1219-21.24. Aye IL, Paxton JW, Evseenko DA, KeelanJA. Expression, localisation and activity of ATPbinding cassette (ABC) family of drug transport-ers in human amnion membranes. Placenta2007;28:868-77.25. Evseenko D, Paxton JW, Keelan JA. Activetransport across the human placenta: impacton drug efficacy and toxicity. Expert Opin Drug
Metab Toxicol 2006;2:51-69.JUNE 2011 American
26. Ramsey PS, Vaules MB, Vasdev GM, An-drews WW, Ramin KD. Maternal and transpla-cental pharmacokinetics of azithromycin. Am JObstet Gynecol 2003;188:714-8.27. Zhang Y, Huo M, Zhou J, Xie S. PKSolver:an add-in program for pharmacokinetic andpharmacodynamic data analysis in MicrosoftExcel. Comput Methods Programs Biomed2010;99:306-14.28. Renaudin H, Bebear C. Comparative in vitroactivity of azithromycin, clarithromycin, erythro-mycin and lomefloxacin against Mycoplasmapneumoniae, Mycoplasma hominis and Urea-plasma urealyticum. Eur J Clin Microbiol InfectDis 1990;9:838-41.29. Lebenthal A, Lebenthal E. The ontogeny ofthe small intestinal epithelium. JPEN J ParenterEnteral Nutr 1999;23:S3-6.30. Salman S, Rogerson SJ, Kose K, et al.Pharmacokinetic properties of azithromycin inpregnancy. Antimicrob Agents Chemother2010;54:360-6.31. Goudah A, Sher Shah S, Shin HC, Shim JH,Abd El-Aty AM. Pharmacokinetics and mam-mary residual depletion of erythromycin inhealthy lactating ewes. J Vet Med A PhysiolPathol Clin Med 2007;54:607-11.32. Nicolau DP. Predicting antibacterial re-sponse from pharmacodynamic and pharma-cokinetic profiles. Infection 2001;29(Suppl 2):11-5.33. Carter AM. Animal models of humanplacentation—a review. Placenta 2007;28(SupplA):S41-7.34. Newnham JP, Kallapur SG, Kramer BW, etal. Betamethasone effects on chorioamnionitisinduced by intra-amniotic endotoxin in sheep.
Am J Obstet Gynecol 2003;189:1458-66.Journal of Obstetrics & Gynecology 546.e17