
Matary Surgitoons General 2013 AllTebFamily.com
155
GE]IERAL SURGEHT
-
Upload
raouf-rafat-soliman -
Category
Documents
-
view
294 -
download
19
Transcript of Matary Surgitoons General 2013 AllTebFamily.com

GE]IERALSURGEHT

O Copgrglt 2013 bg llv/,o,,a,d El-/lrlanE
AA ugffi ,utetted, Nu pnt r{td bnlo uug bo ud, n w!,udttpl, n
ailU aarusl ulafrouw uilnt u,rffpn poutttillior;, exapt infu cap, o{
bd quffif,inu enldid, i* c,,trinol ,l,firh 0,0 ,rttfridt.
Tl,o pubkl% fiam, ,,Mlo uu7 e/{o,,tAfiac0fu *pgrylt lrldat {r,t
bo,vwd uutuiat. l{frr{ loru trnlr,/atafl{ wurlrokil W, to uit[l
bo plutedta ,r,algtp uttttwrg anwguilefi utflo fi^t rppnrfrilrfu.
frutpltru,n 2013Foo fi,lilrul u{oqnation, plnop nff owo ueb tfr,:
I/I/WLI/, III ATA PYO N LI N E, N ET

l'd &kotofioilh atg Ten*:
/Uichae/ Safrrat Eedikrl/.A,A,Cl- An Sluns // rtrrers rty
llt ua fro 6rdrtf,rs0 ,{til Bmh uilo /,it tuus ,l ililr,,r,v
aild tpetnl afl[fiu b dml uilrtit tus,firto tubiwtr uffi, trcfi, A^*gu,rfu pltra md uiln an annztug diffiilufion ,{t0 dafn ,,{^g fu pog^,
Peo[h , l'* lrpW b lfflbdilru twlo a dinoud, {* g*Cp*lfiailldb.,.
$fiertf lots, ilofianndB,6t/-Ath 9fians // nyars rty
Fn l,u ltutanl, tittnttp, trttrttinrl ,{fro uufrla ,rrofuilnl {r,ltil bmh
fatna Badr El Kont$fians /lrtryersrty
Fn l,n C"m,rf,* intu bnt(,
Karrn ilolarund.4tirl/.a,a,cn -An 9frans // nryrs ty
Foo ila ,nl,nbh@ *d M
Dr tl/ofianrued tl r/atary

HOTTTOIISETTIISBOOK ?Tk B*h ai tagrudO CqW 'C*gnry" *d wat@ tr*r,t*g a fftl,oald bs.
Eail, b,wdr it t,ond ,rppd inflB {tar rfhl{u, ulgr,uf,rw aild rtngwtt? u,,o*g
tr ag {* g*b ,utnsta ulo{B b'uruh in a Motrsl ,{ firuu!
Tfipo't a burult, ,{ {peml All,ou {rMn*g ut/, b,nru/a nfrit bnolo, ufiicl,
uill a,o*o gouro tr,fu ilwenbfiofangil,., ;
TWEET hl AEBIIATuafi o{ lil/oitilotbtufrotgru, aog trtilt drrrtrg tW,rgfub,nwla, AlnE uil, toto twpo'tnt poafi fr*rfro lllcQt
AA Trgefuo rn a wph ,l popeu!!
KEYC TO CASES
ed fu dm ol iwpo,tfofi C$r,k"t utet, ul,atgou t*d{Mdb kilN oloutendo us in o {w uudt
QUECTION BAIIKQ,rut u l,o*.p',ur,nu exarl amqel onl, cafigo'il4d,
aundtilg toflo Mfiufb gilru !ru an attunnb lhfritob
fuiw gom afa[ionbtto tnpo'tant uil, ,upeafrl, qtattu,
TAKE YOUP NOTEC
l{g0,, rt^d u,ro efio, hIo,urrafio,+ us{ul,
6, *! AAtartr,,a!!llaa
lloru o blottryq,nq "CURGI-T00NC" :)

BREASI:a
a
a
I}IYROID:I
a
a
I
a
E]IIDOCRINE SUR,GERY:t
t
a
SWEttIiIGS AND $AIIVARY GLANDS:
:*g'Go. Sturg 8lom. Sf,Eg fieftL Gil
btrnol,is
SURGICAL INFECIIONS. SchcmhsudbdhHnrc.loulcdcoaes. oallfiq. EFfoob, h1 crhnnb. lrrli{l 4in Lgnirgloe rd- Ielnrs, hCrgltr*' $rtFJ rib i*otur. llrrd frfrofus. fr1]3' f.UsloorE* Anrmr Brrt T&
gurldoc
2g67t516
24
44454G
rcT'712
T?75T'78&|
IMUMAIOLOGY AIUD
BAs!C GENERAT SUROERYI
a
I
a
I
a
a
a
m
AR,IERIAL gYgIEM
I
T
a
T
I
:*'
VENOUS gYgIEM
I
. Urim
TYMPHATIC SYSTEMrlt.lumphe&r.lgnpJm
gut
vx2

rMkhael.{..4,i"
'':;: .lir'-: :. !tt'r:t:::.!

ilRq-Twr5 1^w*Nv'J'R4W t?.
I
I
I
T
!
Nipple abrasions, bad hggiene, bad general cond.
&tACrffioNDEFINITION: Acule baclerial inflammalion lhal occurs during laclalionORGANI$M: 8IAPH.
PRECIPITATING factor )CLINICAL PICTURE:
Pain Dull achinr 4 Throbbing Attacks ofremissions&
exacerbalionsPgrexia Mild Conlinous 4 Heclic fever
8'rgns l) Enlargemenl,lenderness
2)NO sions ofinflammalion
l) Sions ofinflammalion
2) D(TLARY LN8:. Enlarged. Tender. Firrn. Mobile
Ederna of skinr)
2lfender swelling
with gieldingcenler
lnvesl. r zfr TLC,
^EgR, ^CRP, C/8 for the choice of antibiolics
. U/g ) sile & tgpe of abscess
. lf no response wilhin 2 weeks ) BIOP8Y
{-Lo-ts{-oo3.F
Prophglaclic irealrnenl :. lasl 2 monlhs of pregnanou ) Massage of Nipple & Panlhinol. Al lime of deliveru: lf Fissures are presenl) Painl {issures wilh anli-septics
Stop Laclalion:- lf infanl>9 monlhs) bg giving PARIODEI
- lf lnfanl<gmonlhs) Slop lactation fiorn affecled side , FeedinA from the olher side
Evacuale breasl * Augmenlin(lgm/8hrs)
& analgesics+
Hol fomenlalions
l) Oeneral aneslhesia
2) Radial incision nol reaching nipple, areola3) Deslrog loculi bg {inger
4) COUNTER lNClSlON if in an UN-
dependenl area
5l Antibiotics & dressino
Signs of inflammalion

P hlAts'Flm-
A FIBROSIS
EPITHILIOSIS
"J./Pq4wr5 nupCR[..lE lJg{q%l
Fibrous tissue replaces lhe elastic & fattg lissue )Obslruclion of ducl:
. Unilaleral
. Bilaleral
. Affecting sector of breast )"Seclor Maslilis"This leads lo cgsl forrnalion:. Srnall ( Micro-cgst). Large (macro-cgst). lf Cgsts coalesce)Blue-dorned cast of BTOODGOOD
Atgpical epithelialhgperplasia
?h l1
. Large cgsl conlain Altered blood 1rej pr
. DD: bluish. greenish discharge from Nipple
Aberralion ofNorrnal
developrneni &lnvolution of
Breast
Sorne consideril as a norrnal
varianl

ChJNrcAtPIC,TURE,
. AAPMT
. Dull aching pain;./ 4 Pre-menestruallg or bg Breast rnovernenl/ V Posl-rneneslruallg or bg breasl supporl
I. For lhe lurnD) friple assessment. For Discharee) Cgtological \.
exarninalion & Benzidine tesl, For Cgst ) Aspiration
. Cornrnonlg Bilateral
. $olid or cgslic
. Freelg mobile
. Diffuse
SUR+-TCr/.r5 6.\W(*NY IJRqW
. Recurrent cgslsr Sclerosing Adenosisr Cancer
a
#ltrlrilti
. Clear
' Yellow. lf retenlion Cgsts
) greenish
''FE S;rrrLE
ffi| ' # lea, coffee
I
l. VitaminE I
?Aqv t +
. Enlarged
. Elastic
. fender
. Mobile
MorcAr' Analgesics. Prim Rose Oil. Parlodel. Danazol. Psgchotherapg
SI,FGBY. Biopsg. Aspiration of cgsls. lf cgsts are
recurrenl ,or Cgslof Blood-good)Excision
DocrltupAprur.oiA
oF
eAhlAucr,l.{B
Tl,lEilP,q=Tw.J6 hloocxr,qr 5,R(#l ? Aqe I 5
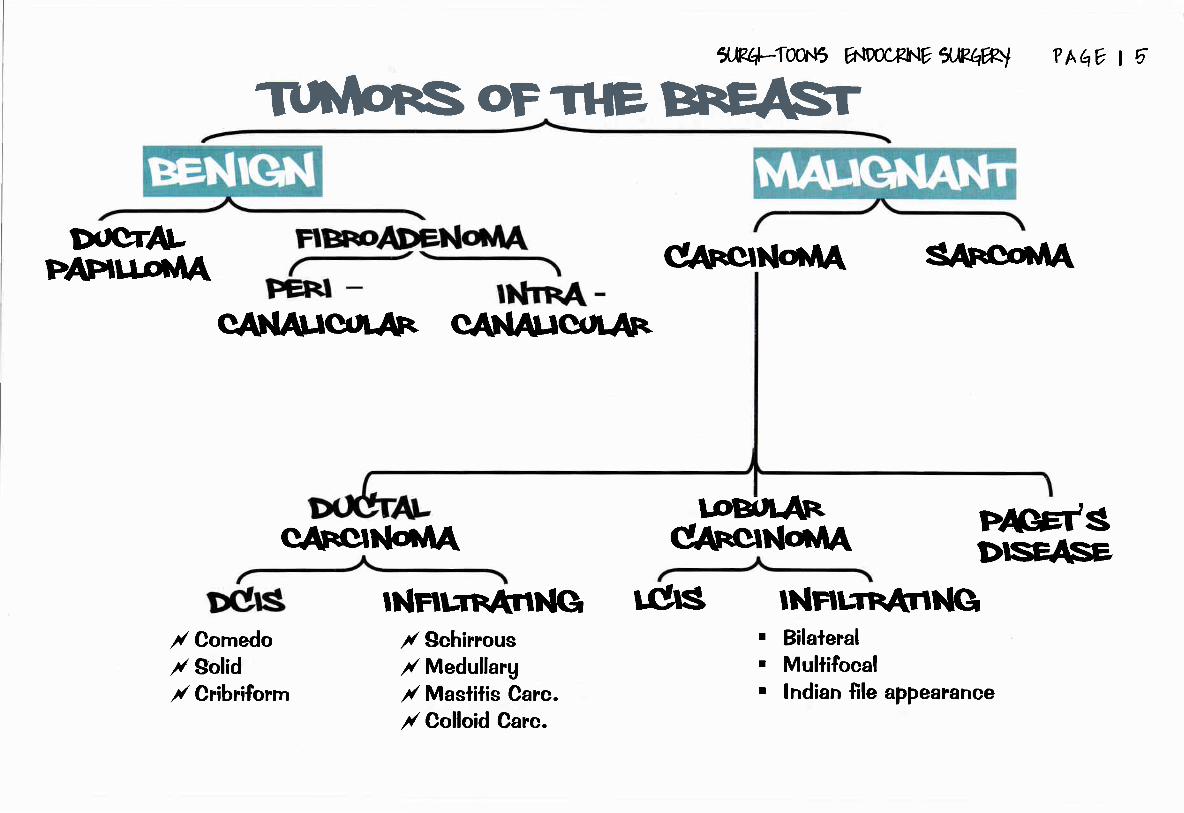
/ Comedo/ Solid/ Cfibriforrn
qltrclN6tA
CARC'N6TA
INrtT.rnATINGr( $chinousr( Medullarg/ Maslilis Carc./ Colloid Carc.
W
CAtrCJN6TAtoBu[.An
tcls INHTTnANNGBilaleralMultifocalIndian file appearance
rrI
PAGEt'SDISEASE,

. Benrgn
. ll's lhe
. Macro)single pedunculaled mass, mag ulcerale
. Micro) Vascular CT core + hgperplastic epithelium
DOCTPAPITI.or.IAEEhllGt{ oFTl-lEffi
Female, 3,O-4Onipple +
. Bleeding, ) Zonal pressure wil! reveal discharge
. Swdling) RETENTION CYSf.. Single, Srnall, Near nipple ..
.2 NO > NO pain, NO LNs enlargemenl
Uears with bleeding perSwelling +2 NO
@ pr -) For the discharge : Benzidine lesl@ iira,tl,t)For lhe Papilloma: Glaclographg ..({illing defect)
@;r.ro)For lhe resl of the breasl: Mammographg
Micro-dochectomg & histopathologg
PT.
ilR{dl-Twr5 E{9ocRlNE IJRAW
Micro
2EnITII
Macro
lumor of the breasl aff
I
. ducls
Fernale. 2O-3;O Uears
NUMBER: SingleSIZE: SrnallGFrRcEt E!@E*ur[ace dsirrn o+rrd
ilirfiEIiIat
CONSISTENCY: Firrn
CUT SECTION:
c/oo/E
(Capsule )True + False cap. )
Mal'rg.
TTT
I
I
?h I b
rnobile:Painless Breasl lump,
Painless lump
f
wilh No LNs enlargernenl
Fernale, 3O-5O Uears
NUMBER: Single
Never lurn malignanl
SIZE: Largr
SURFACE:
Eneculalion(Circum-areolar incision)
SriuD
CONSISTENCY: Soft
ze l2O-9;O cm).. probe passes
CUI SECTION:
[La
EWUtrEducls
CAPSUTE:
tIl
Painful rapidlg growing lump
Painfu! rapidlg growing lurnp,mobile, wilh no LNs enlargemeni
urfiace o*rs,
lf srnall :
r' Excision with safetg rnargin, Biopsglf Larqe (cqstosarcoma Phqlloidesl :
{ Vld,lde local excision or Sirnple masleclomg
Mag Turn ) SARCOMA

DOCTALclrrcll.httA
Biopsg bg self-retainingneedle under mamographg
row G+RADE
lE"r-'* I
lJR+Iw.l5 A{mCFhlE flJts@l
. Discovered accidenlallg aflerrnarnrnographg) Bg Core-cut Biopsg
. No rnicro-calcificalions
. ll's a risk faclor for Cancer breasl..
r Managernenl :l) Follow up2) Prophglaciic Tamoxifen3) lf lhere's *ve Farnilg Historg)
MRM * reconslruclive surgerg
?h l7
Bilateral
Multifocal lndian {ileaPPearunce
. Exarninalion everu 6 rnonlhs
. Mammographg everu 2 gears bgobligue laleral view
(l gear in HRG)

lncidence
Pathologg
INFIffiNG@CAFCINoD.,IAti
. Extensive Fibrous TissueMacroscopicallg:. Hard rnass, in{iltrating er
. cut surface)@areas if Hge, Necrosis
Microscopicallg:. Malignant rounded cells
Fibrous tissues
Most common tupe
:t!{tlrts
Clinicalpiclure
..75yofit
3i[":',' Dimpling..(Cooper's ligarnenr) \
Prognosis
HIHHI
. Relracled nipple..(Milk duct)
. Exlensive Malignant cellsMacroscopicallg:. SOFT like Brain. Cul surface)
6%
lJRq-ro}r5 696ffihlE 5,)?4W
I it
Microscopicallg:. Mahgnanl cells, li{tle
fibrous tissue,
Bad
ffiMacroscopicallg:. SOFT rnass
Miuoscopicallg:
' Spheroidal cellsproducing mucoidmaterial
Good
?A vt6
rl,
,l
During Lactalion
TNVoLVES 4ESI[E]
llrvrlrl If La
Good.. BAD prognosis in
slornach ..
.@
. C/Oz Anorexia, Slowlgprogressive pain
. O/E: Enlarged LNs,
No siqns of inflarnrnalion
Bad

lJFq-T1un5 nD0cFll.lv ilPhw) ?hqY t 1
rlh: p@oFcANcERffiINCIDENCE / Most comrnon maligna
/ Mosl common siie is.JYfrOFPffiFAtli
neurostt{GrFACIORS
5$asag
S;rrcilNG'
FRoGftlGlS
F Axillarg LN-ve
/ 99% in females
/ Age > 20 Uears
Sjg+c ,girilil.c g .,iiili. 9 .r,rrig+c , asil e*E
d'Srsii+. at*ii 9 pirrfll 9 d{r.r.i , elc &c 9. Fernale , Nulliparous, peak of age 60 gears. Earlg menarche,lale rnenopause. Posilive familg historg. Alcoholios, OCPs, lnactive, Obese. HIGH RtgK FACTORS:
l) Pre-cancerous lesions ..Papilloma, LCIS..
2) Previous affection with Cancer breast
Lgmphatic, blood spread, direct spread
TNM * Manchester
Good + bad indicalors ...
* BRCA I (chromosome 17)
n BRCA 2 (chromosome 13)
, Lu-Frurnini sgndrome (mutalion in gene P53)n Goddwen sgndrome
(Assoc. with PAPILLARY CARCINOMA OF IHYROIDI
. Size, LNs affeclion. Invasion. Melaslaiic polenlial
according lohistopalhological tgpe

ilK+-TooN5 Y 1JPqW ll0
SPREADLYMPHATIC .. BY EMBOLISAIION & PERMEATION..
. Axillaru LNs) Supraclavicular LNs , Rarelg lo lnternal mamrnarg LNs
. lgmphalic from Lower inner quadranl pierce reclus sheath ) liver nodules) Mag melaslasize as "SISTER JOSEPH NODULE"
. Obstruction ) Pcau d'oranle, Melastatic nodule, Cancer en Cuirasse
DIRECT
. Skin, pecloral Fascia, Pecloralis major, Serralus anierior, Chesi wall
BLOOD
. Bone secondaries)OSTEOLYTIC LESIONS in
. Through valveless cornrnunicalion belween Posleriorlntercostalis Veins & Paravertebral venous plexus ..
N.B. ln Proslalic cancer ) Bone secondaries are Osleogenic lesions
TRANSCEOLOMIC ..Relrograde lgrnphatic perrneation..
. OVARIES) Krukenberg's iumor
. NODULES lN DOUGLAS POUOH) Plurnmer's shelf nodules
. PERIQIQNEUM) Malignant ascitis
CANCER BREAST SPREADS BY BLOODgPREAg) DI$TANT MICROMETA$TASI g
srAgnlq II(rlcgII
'T *l\-;\ q
EARLY
CANCER
BREAST
LOCALTY ADVANCED
BREAST CANCERTa, oDg N, Mo
MEIASTATIC

CLn.I'CAt PIGK,FE oF EREAST CArCn
PAINLESS BR,EAST LUMP(Discovered bg routine screening)
DISCHARGE:Waterg, Blood slained, pastg discharge
OCCULT PR,ESENTATION:o BONE) Bone ache, pathological fraclureo Lung) Drg cough, hemoplgsis, dgspneao Liver) Malignant jaundiceo Axillarg lurnp
SyiimE,
FEMALE, 50-60 YEARSIN UPPER LATERAL
ooo
WIIH PAINLESS SWELLINGQUADRANT OF BREASI
IATE SIAGEMASIITIS CARCI NOMAIOSISPAGET'S DISEASE OF NIPPLE
a&q-Toar5 E{pocxx.lE a.Eqw
GENERAL:CACHEXIA + SIGNS OF METASIASIS
(LNs: Troiser sign, BONE: fender spine, LIVER: Jaundice, Hepatomegalg)
LOCAL:EXAMINE BOTH BREASTS + AXILLA + SUPRACLAVICULAR LNs
INSPECTION.. PALPATION:.,ASYMETRICAL BREAST" I
. Nipple & Areola:t) Nipple retraclion2) Areola)Pagel's disease of Nipple
. Skin proper:l) Skin Nodules2l Skin Ulceralion3) Cancer en cuirasse
lnfillralion o{ Cooper's ligamenll) Skin teethering2) Skin dimpling3l Skin puckering
Lgmphedema:
U Peau d'orange2l Brawng ederna
Metaslasis:) Sisler joseph's Nodules
?[,q ! [
SlCr}.lS
BREAST MASS..Starl wilh lhe norrnat sile
l) Site) Upper laleral quadranl2) surface) irregular3) Edge) lll-de{ined4) Consislencg) Hard in schirrous
carcinorna. sofl in Medullargcarcinorna
5) Mobilitg) Earlg mobilitg, fixedIatelg.
LYMPH NODES:l) Free axilla2) Enlarged, Mobite3) Enlarged, Fixed4) Supraclavicular LNs enlargernent

I (,FffiCANCERDUGD{oSIS
TRIPI.EaSSESMertr
Hisiorg * Sono-Clinical MarnrnographgExarninalionJ
-
Mammographg U/S
INDICATIONS:
" Screening in high riskgroirP
. Delecl impalpablebreasl cancer
" Evaluale sound breastgICNS SUGGESTIVE
OF MATIGNANCY:
' Cluslered Micro-calcificalion
(DUCTAL: 2O%). Slar shaped mass
SrAglNG'I
I
I
cxRu/sTCrn
5R{4=Tw.t5 ElPPffhtE fl'.Ph#rl
. CT scan
. MR.I
cYsTrc sollDIIASPIRAIION FNABC
Can'l differentialebetween CtS,
invasive carcinoma
PREOP
. TruOcut needleunder Localaneslhesia
. Frozen Sectioninlraoperativelg
. Excision Biopsg
. Mammographgguided usingSelf-retaining needle
TrrtvloR.ffi
PtLoti, OP
?hqv t w
. CEA
. cA l5-3
HORNIONAtffiT
I
I
tffi-u{SruD/I r+ cr-rrurcAllYI rueonrnrs
-
EstrogenProgesleroneSlain wiihHer-Z antigen(Dcls)
Not affectedI
FOLLOWUP
I
IOTALDISSECTION
Affecied

(,FffiAANCER
. Cancer breasl is a sgslernic disease
. Aim is to CURE mg palient
. Once il is evident) lt melaslasizesin lhe forrn of MICROMEIASTASIS
. TTT> TOCAL + SYSIEMIC TTT.
STAGE I, !I
I
I
t
I
Rernoval of breasl lurnpR.emoval of Breasl lissueBlock dissection of axillaReconslruclion of breaslwith Mgo-culaneous flapor proslhesis " silicon"
Maslectomg
t timii -,f HIGH Grade lumor.... Give ISOO RAD ll -Quadranleneclomg
l
{ -HALL LNs are POSITIVE li -Axilla Clearance i
i -ln MEDIAL IUMORS .... lnlernal rnammarg LNs affeclion : -Radiotherapg.-... -..-....*....^,, .
STAGE
5uA{4-:lw.t5 a{DocxhlE f,.M{4rf}l
Neo-adjuvanl Chernoiherapg is given) ForDOWNSTAGING of Turnor (From Stage lll>ll)Surgerg is decided according lo response toChernolherapg) MRM OR LUMPECTOMY
.- Removal of breast lumpPosl-operalive Radiolherapg5OOO RADLocal conlrol of Axilla:- Clinicallg *ve) Block disseclion- Clinicallg -ve Senlinel LN Biopsg
"Pl.d*k I 17
@ . Fernale >Togears
HORMONAL THEMPY- Horrnonal receplors *ve- Bone MelasiasisCHEMOTHERAPYTTT. OF COMPLICAIIONS
CgclophosphamideMelholrexale5-Fluorouracil
STAGE IV
I
I
rI
Free axillaHorrnonal
*ve
g-t rtplarJtr
0tle+ur!! rS\i

lJp.q-{1q.t5 1^w,Pli^r7 xwwl
PATIENT,/ Pregnanl
/ Preference
{ Ptevious imadialion,/ Conlraindicated
?hqv tw
f aI! 51lri n,/ Complications of operations./ Local recurrence./ Disiant melaslasis,/ Carcinorna of olher breasl
TUMORg./ Bilaleral ... Multi-focal/ Pagel's dis. ...Central lumors/ Tumor > 4cmr' High grade (lll) ... Fxed to Ms... Dislanl melaslasis
,/ clg > 20 vo
Breast'/ Small
I o;l -Li #/ ln firsl 2 gears ) Everg 3 monlhs
/ Nexl2 gears ) everg 4 monlhsr'Yearlu for !ife) rnarnmographg of
the olher breasl,D. lnlra-duclalcarcinoma. Reirograde lgmphatic spread from schirrous carcinorna
AT{UAFEOTAETIOLOGY:
/ Middle aged femalez glderlu female
ttitsiri+,o iilur6 i', rl
Resislant to usual TII of eczerna
Modified radical
rnasteclomu. ln nipple )Erosion. NO itching. NO oozing. NO vesicles. Well delined lesion. Breasl lump
lffiBiopsg & Histopathologg
. Epilhelial hgperplasia, Lgmphocgtic infiltralion

9.W-TWr5 A{9tr4?[.lE XMW ?hqv t w
A Risk faclors :
l) Prosialic cancer
2) BRCA 2 mulalion
frealrnenl )CA$IRACIION, MRM
MRM + CHEMOTHEMPY
AFTER ISI TRTMESTERt f, Radiotherapgt f, Chemotherapg in ldt $ Horrnonal therapg
( -ve homonal receplors)
ETIOLOGY:. DE-novo or on lop of sofl
fibroadenorna
CLINICAL PICTURE:I
Large breasl mass.. Spread mainlg bg Blood..( LNs
spread is rare & late )INVESIIGAIIONB:
IREATMENI:Simple rnaslectorng + Radiotherapg
' Triple assesrnent)
DEFINITION:
Painless Enlargernent of MALE breasl due
lo
Etiologg :
a) Comrnonesl cause is
b) 9metabolism of eslrogen,LCF
Trealrnenl :
l) SC masleclomg2) Suction lipeclomg3) Endoscopic surgerg
*.:.
***
DEFINIIION: Dilaled major milk duclshasM
CLINICAL PICIURE: Fernale, middle aged, srnoker presenled bg :l) NIPPIE DI$CHARGE ... uearng, serous, blood slained
2) SUBAREOLAR PAINIESS SWEILING
INVE8TIGATIONS:
l) lf Pt. presenied with sub-areolar rnass) Triple assessment
2) lI Pt. is presenled with Nipple dischaqe) Benzidine tesl, cglologg
l) Earlg) Combination qle!!lbig!!gq

lJPq:Tw\5 V XMW ?hqY I uo
l) Reason for referra! io breast clinic )2) )rnore cornrnon in srnokers
3) Cause of Blood slained discharge
4) Cause of Green discharge. Ducla! changes
. Relention cgsls of5) Cause of Serosangious discharge )6) Site of breast cancer )7) Histological tgpe of breasl cancer )8) Cause of bilaleral breasl cahcer
9) Secondarg deposil in carcinorna
lO)MOT of breast abscess )along
)of breast )
(Nipples)
MRI breasl imaging:. Dislinguishes scar from recurrence. lmaging of breasl implanls
Managernent of axilla in breasl cancer & recurrenl disease
CONGENITAT NIPPLE RETRACTION .. Simple nipple inversion:. Occurs at pubertg.. Unknown etiologg.. Bilateral in 25%.. Mag cause problerns during lactalion.
POLYMASTIA. Accessorg breasl.. Usuallg bilaleral.. Wlhout nipple.. MaU occur below pectoral region in groin or even in fhigh but with nipple.
MACROM AZIAMild cases can be lrealed bg anti-eslrogen.
TRAUMATIC FAT NECROSIS. Can occur via blunl lraurna or even indirecl violence i.e. vigorous conlraction o{ pecloral muscle.
. Granuloma formalion with rnarked fibrosis.
. No LN enlargernenl in axilla.
. Mamrnographg is nol conclusive as il gives feaiures similar lo lhose of cancer.

x,w-Twr5 E{DocFNe ilRqW ? hqv I EINFI.AMMATION OF BREAST
Acule breasl abscess.
Chronic breast abscess
T.B.
.. Obscure igpe of thrombophlebitis affecting veins of the breasl5) Mammarg ducl ectasia.
tr Sites of breasl abscess:. Pre-mammarg ) on top of infected sebaceous cgsl..@9I9)deeplopecioralfasciaonlopofinfecledhematoma.. lnlra-mammarv ) inside breasl during laclalion: can oecur al ang parl of lhe breasl.
-ln slage of milk engorgement: Dull aching pain referred lo shoulder wilh persislenl fever and atlacks of shivering.-!n slage of acule abscess lhere is pitting edema.
tr CHRONIC BREAST ABSCESB:. C/O) painless breasl lump and sornelimes dull aching pain wilh no sgslemic sgmploms. O/E) lhe swelling is irregular.. TREATMENT) Excision under general anesthesia.
tr TB OF BREAST ) usuallg occurs wilh pulmonarg TB.
FIBROADENOMA. Benign simple fibroadenorna is less lhan 3 cm.. Gianl fibroadenoma more than 5 cm.. PHYLLOIDES IUMOR) occurs usuallg in perimenopausal women in 30-50 age groups.
BREASI CANCER
tr FNABC ) can't differentiale belween ClS, ln{iltralive cancer (wrDE BoRE cANNULA )tr TUBUTAR CARCINOMA
It is a rare bul a well diff. cancer. lt is small in size being aboul I cm in diameler hard and oneseclion has radial appearance. .Histologicallg it forms lubular structures formed of single lager
o{ epithelium. ll spread bg lgmphocgles and it has verg good prognosis.
tr PAPILLARY CAR,CINOMA.. INTRACYSIIC PAPILLARY CARCINOMARare lgpe that is dif{icult io disfinguish from benign inlraduclal papillomafosis.
Well circumsoibed and hislolo$callg demonstrale papillarg formalion it presenls bg
bleeding per nipple and it is of good prognosis.. lnflarnmaiorg carcinorna can occul in all age groups.. lnvasive lobular cancer indislinguishable fiom invasive ducl carcinoma.. fhe second line Hormonal therapg used when famoxifen responders relapse ) Sgnthetic
progeslerone .. "Medroxg progeslerone acelale (provera)" .
. Chemotherapg is the lrealmenl of choice for melastasistr Side effecls of Radiotherapg :. Local burn. Pulrnonarg librosis. End arleriiis
tr Axillarg surgerg in breasl carcinoma. Axillaru LNs melaslasis is lhe besl marker for prognosis. Trealmenl of axillarg lgmph nodes positivelg influences survival. NO RADIOTHERAPY is applied if axillarg clearance is performed
tr Lgmph obslruclion of advanced breasl cancer :. Peau d'orange, 9kin noduler Cancer en cuirasse ) (skin nodule + lgmphedema of breast skin). Edema of arm. Lgmph-an$osarcoma
r)
2)s)4l

I
It-
l'.Rq-Twr5 hID00RINY gMR't
well
?h I tg
fernale in child bearing period presenledwilh a mass better felt bg tip of {ingers notlhe flat of the hand , pain and swelling arerelated io the cgcle ,Axillarg LNs are
enlarged, elastic, fender, mobile
fbruystrb dbase2- Young Female 20 gears, presenls withcircurnscribed painless rnass, Firrn in
consisfencg, freelg mobile, Axilla is Free
fbro ademma3-female 4O gears old presenled with bleeding per nipple on zonal pressure
lrrtra- fuctal lafllbrt/d,4-old female presenled with painless mass in lhe upper lateral quadranl oflhe breasl
6atcer brast.S-Mostlg old female presents wilh unilateral eczema like around areola (ordiscoloration), not ilchg and nol respond lo rnedical TIT
PaM dbase.6-female 3O,4O gears old presented with large firm to soft palpable mass mighlreach Hulh size with NON- palpable axillarg tNS and skin ulceration might occur
6ystosarcoma /E/bd.8-Laclating female presented with painful breasl O/E inflarnmatorg reactionpresenled in a Seclor of the breasl. Axillarg LNs are enlarged, elasic,fender,mobile
,4cilte lactatru fi/astttb (nrk etelrgefi/etrt)9-Lactating female presenls with bad general condition, induration of the breasland Axillarg LNs are Hard and Fixed
)/as t itb carc irlor/atos rb,lo-Laclating fernale presents with breast rnass, hectic fever and lhrobbing pain
Aclte brast dbscess,ll-Female, middle aged, srnoker presented with creamg breast discharge andpainless swelling (rnostlg sub-areolar)
Dtct atasn

lJRr+-rwr5 1a.liw*Nv XMWI
r Earlg deteclion of cancer breast
r Managernenl of Acule breasl abscess
r Discuss Trealrnenl of Milk engorgernent
r Causes of chronic breasl rnass
r Breast abscess
r Nipple discharge
r Breast rnass: lnvesl'lgation
?hq? t q
( Ailar f,2@7)
( ,4ilar f' 2@7 )
( ,4y'rar F' 2@6 )
( ,4ilar f,2M )
( ,4ilar f,2CCL4' - r4y'rar ril' ZmO - An sfrafi/s,2@4 )
Cancer Breasl : diagnosis & ttt( Atu sl/aus/@5 )
Managernenl of earlg cancer breasl( ,4ilar ,1r1, 2o2,2d/ - Kasn 2@8 )
r Pathologu of cancer breasl
r Fibro-adenosis :etiologg , CIP & pathologg
( ,4/rar f' 2fu5 )
(r4drar F,2M )
( ,4/rar )A zma I
( Alil shafils,2m )

5,W-T0ur5 VSWW Thtqvlm

? hEV | ?.1.er{m@D: dpnen
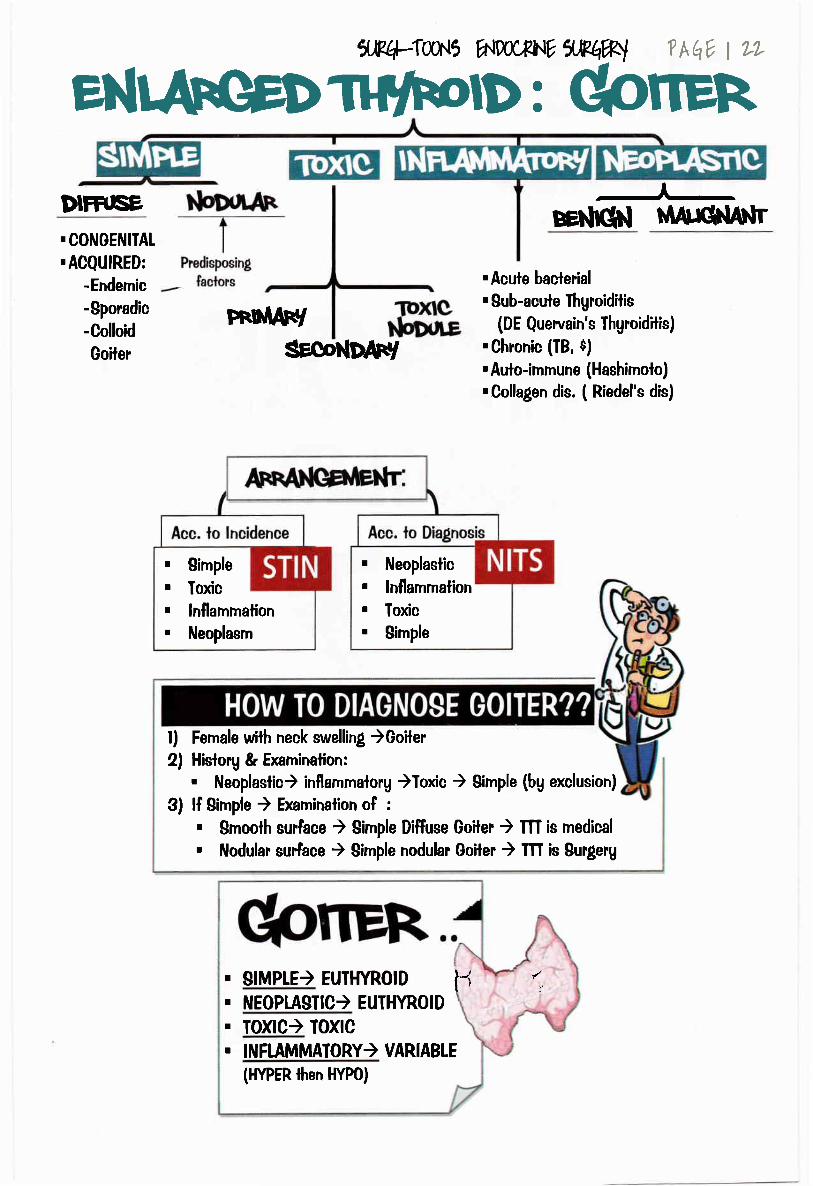
DIH'SE BEh[chl rilArqilA]tr. CONOENITAL
. ACQUIRED:
-Endemic
-Sporadic
-Colloid
Goiler
l) Female with neck swelling )Goiler2) History & Examination:
. Neoplaslic) inflammalorg )Toxic ) Sirnple (bg exclusion)
FRnTAN/
SECONDAF/
. Acuie baclerial
' Sub-acule lhgroiditis(DE Queruain's Thgroiditis)
. Chronic (TB, $)
. Aulo-immune (Hashimoto)
.Collagen dis. ( Riedel's dis)
xR4-Tw\5 1H'.{W*WXR@I
. Neoplaslic
. ln{lammation
. Toxic
. Simple
. Simple
. Toxic
. lnflammation
. ileoplasm
3) lf Bimple ) Examinalion of :
. Smoolh surface ) Simple Diffuse Goiler ) m is medical
. Nodular surlace ) $imple nodular Goiter ) III is Surgerg
. stMP[E) EUTHYROTD t{ ',. NEOPLASIIC) EUIHYR.OID
. Ioxtc) Ioxc
. INFLAMMAIORY) VARIABTE
(HYPER then HYP0)

lJ(q-Taar5 n9ocPltlt ilPI#) Thav I L1
SMru,qptrER
. Endemic) AbsoluteVlodine uocit
llrlgll
. PhgsioloAical) Relalive V lodine
At pubertg, pregnancg, lacialion(VENUS NECrq
Repeated episodes of Slress (Stress) Hge) Necrcsis) nodule)
Painless Mild enlargemenl of the
Gland
. Nodular swelling in the neck)cosrnelic disligurernent
. Pressure manifeslalions,
Gland
. Srnoolh, Sgrnrnetrical )
. Mobile, Nol lender
. No olher manifestalions
. Enlarged
. Firrn, Asgrnmelrical
' Moves with deglulilion. No loxic manifeslalions
EI Tracheo-malacia (Kocker's tesl
MCarclid arlerg pulse (Berrg
tesl)
Same lnvesligalions
as Nodular Goiter, but..
- U/S)Diffuse Goiler. NO FNABC
l) Function )2) Morphologg
3)
4)Exclusion of :
' Mal'rgnancg) FNABC
Treatmenl
0.2 ngld for several monlhs
lhen lapered lo 0.1 mXld for gearc
Total thgroideclomg wilh Posl-op replacemenl therapg
(l-thgroxin 0.1-0.2 ngd I *Histopathological sample
lf smal! sized in a Uoung Pf. )Medical thgroideclomg. m. of Complicalions
Partial lhgrcideclomg
Sublotal thgroideclomg
To{al thgrcideclomg(Io avoid recurrence)
Dunhill operalion
2rg thgrolo{gggElq{glg1gus inlernodular lissue ..257o )
Pressure on lrachea) Poslural dgspnea
Hge , lnfeclion, Cgslic degeneralion, Calci{icalion
Relro-sternal exlension.
trtrtrtrtr

- HYPERTIIYROIDIEM.. +Thgroxin due lo thgroid gland hgperactivitg- TIIYROTOXCOSIS.. +Thgrofn due to Thgroid gfand, drqg induced, eclopic hormone produclion.. elc
ffiffi
1#.14-{ooN,5 A\W*NY qu?q%l
NEoNATAt
RAITEffi
Il) qAS+trroxtlGrS2) w eoEFVAtN -rrnc/RolDrrts
tffi
YAQK I ?4
l)rHffiFACrrmA2)ffirHffi
DRrrc-rNp(rcm
l) FnlciloNtNG sEcoNDAF$/CAFCINortTA
2) SrxrfaoVAFll3) TSH srlenEflNg IDENortA
oF Ptfl,rrA{/ GI.AND

1JK4-T1U\5 hleoCFN? il?4w T h{4V | 15
0 I I ilil
EIIOLOGY:
Aulo-immune..flEII)Iupe V Hupersensitivitu
Osec. from 4 sec. from
0n iop of Normal Gland 0n top of long standing SNG
0,c,D . Sudden Onsel, Rernission & Exacerbation
. Gradual onsel
. Slowlg progressive
CLINICAL PI )TURE:
Tgpe o{
palieni
Fernale at ffi age
subjected lo Traurna,
Dre{nahcu, lacialion
clo:,,gEE
LATER''
,foxic sgmploms, Auloirnrnune manifeslalions
. foxic sgmptoms
. M Artoirnrnune manifestalions
Dominanl
manifes{alionsSp rnanifeslalions @8 rnanifestations . Youngl Pl.) CNg
. old Pt.) cvs
olEl,,GLAND"
. Firrn, well defined edge
. Non lender , Freelg mobile
. Ihrill
INVESTIOAIIONS:
Laboralorg AT3,T4 + VISH
r - ve Antibodies r - ve Aniibodies
U/S : Mild diffuse enlar[emenl Mulliple Nodules Solitaru Nodule
Thgroid scan :
(Diffuse A Uprake) (OVER-active inlernodular lissue) (Low uplake ofsurrounding lissues )
TREATMENT:
l) Neornercazole (10 mg x 3 /d)
2)lnderal (80-l60mg/d)
3)Valium (s-15 mg/d)
N.B. IF MEDICAL ITI FAILED:. (45 Years & Large) Surgerg
' >45 g.rr.)ll3l
Main Line is
Sublolal Thgroideclomg
afler Preparalion
lf High risk Pt. (Hearl failure)) ll3l
:: Medica! ITT is used ONLY
for PREPARAIION(Lugol's iodine 2 weeks before surgerg)
lf Pl. < 45 Years:
lpsilateral Tolal
Lobeclorng afler
preparation
(Hemi-lhgroideclomg)
No role for FNABC)As incidence of malignancg in a loxic goiter is exlremelg rare

Uo
ChJN
ff 6d 6dlb JiIe o) *,ri,Diplopia t rl,Jt*te J-trt t #J6xll oi$6f
6Jly't u'lN!)t 9 u'JJlaq$Ihgroid paradoxl-J
!. -nrlir o "i
r ls il lrue or false?. Nafzrger lesl , Ruler tesl
tr Darlgmph's sign
(Rim of sclera)
tr Stellwa!'s sign
(lnfrequent blinking, lremors)
tr Joffrog's silnlack of wrinkling on
looking upwards
E Von Gravie's sign
Lid tag
Etr Rosenbach's sign
Fine lremors on 4fentle closure
tr Mobius Sign
Failure of convelgence
f ot6p j *otr J.rLSCT ederna .rtll.-irn
. PULSE: (Tachgcardia, Waler Hurnmer pulse,
mag be irregular). B[00D PRESSURE: Asgstolic,9Diaslolic. IEMPEMIURE: Oin Thgrotoxic Crises
. ABDOMEN ) HSM
. UPPER, UMB: )Aoopacg (Clubbirrgf
. LOWER UMB ) Pretibial mgxedema
. IA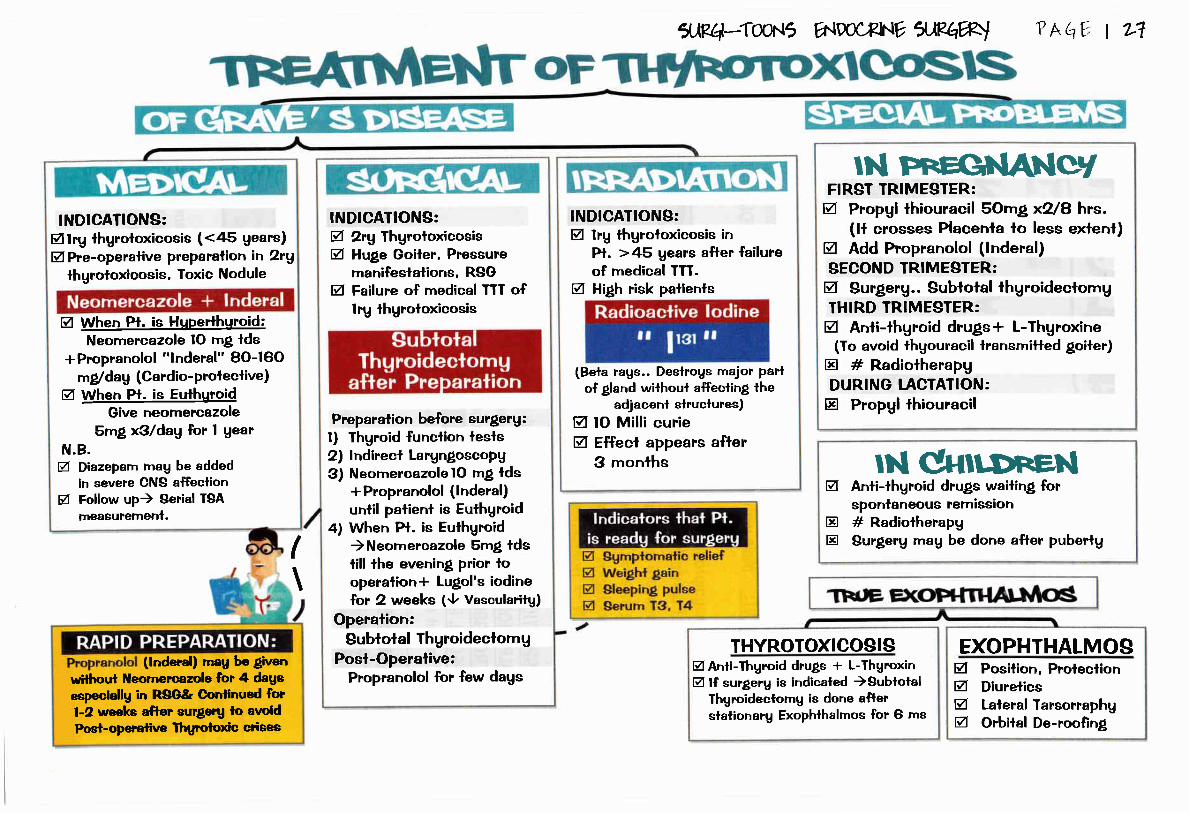
INDICATIONS:Mlrg lhgrotoxicosis (<45 gears)EI Pne-operalive preparalion in 2rg
lhgroioxicosis. Toxic Nodule
M When Pt. is HqPerthuroid:Neomercazole lO mg tds
* Propranolol "lnderal" 80-160mgl dag (Cardio- Proleclive)
M When Pt. is EuthuroidGive neomercazole
Smg x3ldag for I gearN.B.@ Diazeparn rnau be added
in severe CNS affeclionEI Follow up) Serial TBA
measurement.
INDICATIONS:V 2rg fhgroloxicosisM Huge Goiler. Pressure
rnanifeslalions, RSGEI Failure of medical TTT of
lrg thgrotoxicosis
1,^?4:lw=t5 A{DOCBhIE ilPq%l
Preparation before surgerg:l) Thgroid funclion lesls2) lndirecl LargntoscoPg3) NeomercazolelO rng lds
*Propranolol (lnderal)until palient is Euthgroid
4) When Pt. is Euthgroid)Neomercazole Smg tdstill the evening prior looperalion+ Lugo!'s iodinelor 2 weeks (9 Vasoularitg)
Operalion:Subtoial f hgroideclom g
Posi-Operalive:Propranolol for few dagswithoul Neomercazole for 4 dags
especiallg in R8G& Conlinued fiorl-2 weeks after surgerg lo anoidPoet-operalive Thgto,ioxio crisea
INDICATIONS:EI lrg lhgroloxicosis in
Pt. >45 Uears after failureof rnedical TTT.
EI High risk palients
(lnderal) mag be given
I\
(Bela rags.. Deslrogs major Parlof gland without affecling the
adjacenl slruclures)EI tO Milli curieM Effecl appears afler
3 monlhs
IN FII=GIIANCrIFIRST TRIMESTER:g Propgl lhiouracil SOmg x?8 hrs.
(lf crosses Placenla io less exlenl)g Add Propranolol (lnderal)SECOND TR.IMESTER:g Surgerg.. Subtotal thgroideclomgIHIRD TR.IMESTER,:A Anfi-lhgroid drugs+ L-Thgroxine
(To avoid thgouracil lransrnilted goiter)tr # RadiotherapgDUR.ING T.ACTATION:tr Propgl lhiouracil
? hq, t 7;?
ry'I EI ggmpiomalic relief I
I g weigl* gain I
I u eUeping pulee I
I el gerum rs. r+ |
,
g
trtr
lN Cutr.oneNAnti-thgroid drugs wailing forspontaneous remission# RadiotherapgSur"gerg mag be done after pubertg
THYROTOXCOSISM Anfi-fhgroid drugs * L-ThgroxinM lf surgerg is indicated )Subtotal
fhgroideclomg is done aflerslalionarg Exophthalmos for Ci ms
EXOPHTHALMOSg Posilion, Protecliong Diureticsg Laleral Tarsorraphgg Orbital De-roofing

i*.q I B
.:ti-:[:;.-..
PU'Nql}GRises wilhdeglutilion
Descends again
{hrough lhoracicgoiler
CIINTAUHCTURE,
TYPE OF PATIENT:
a
T
I
I
. Gland is presenl in chesl
. SeDaraled frorn rnain (land
. Arises from Eclopic thgroid lissue
. Takes blood supplg frorn
rnediastinal vessels
I
I
cluT
T
T
olE:I
T
T
T
ggg
Idea! lreatmenl ) Subtota! thgroideclomg from Neck "piece meal"
lf toxic ) Subtotal thgroideclorng after preparation with TNDERAL onlg
Avoid ) lnjurg of RLN , Fragrnenlation if malignancg is suspecled
1JK4-Tm\5 ww*NV,.lF(lW
*'' *"+"q. ;:{+jl-*flEfu'*i; "' B;'**.'
cprreR
"wlmnAsnrlAr,@rrRe"Nodule presenl in Chest
Connecled lo rnain gland bg
band of lissues
Takes blood supplg from
Thuroid vessels
, RSG. Reidle's thgroiditis. Malignancg. Mgopathg of slrialed rns. 0f esophegous
. RSG
. Ihgmoma
. lgmphoma
. Aorlic aneurgsrn
. INS ++
It Mag be sirnple, Toxic, or Malignanl Goilre
Male with shorl neck, slrong slrap rnuscles (MEDIASTINAL WPE)
Mag be asumplomaiic
Hislorg of cervical goiter which has disappeared
Severe pressure rnanifeslations :
l) Trachea )Dgspnea2) Esophagus ) Dgsphagia
3) RLN ) Hoarseness of voice
INSPECTION) Engorgernenl of neck veins, dilaled chesl veins
PALPATION) Lower border isn'l palpable
PERCUSSI0N) Dullness over rnanubrium-slerni
SPECIAL SIGNS)"Patient elevates arrn above level of head) Facia! nlelhora due to venous conoesfion "
is the invest'rgalion of choice
lsolope scan
PIain X-rag ) shadow in superior mediaslinum........
Flow Volume Ioop pulrnonarg funclion lesl

Autoirnmune disease: Abs against Thgroglobulin& Micrcsome )Destruclion of Follicles
Middle aged Female ClO ol manifeslaiions of loxiciig(HASHITOXICOSIS) then Goitrous Mgxederna+Other aulo-immunemanifesialions
O/E: Gland isAsgrnmetrical.
>ACIDOPHILIC
' Lgmphocgtic in{iltralion(Features of Chronic Thgroidilis)
Latge, Multi-nodular, Firm,and Moves with deglulition
9 61115 i,ri&li.rrr'
. 9Thgroid function (Mgxederna)
.AEgR
. Anti-Thurogllobulin Abs +ve
. Anli-rnicrosornal Abs +ve
THy'trolDrns4AFibrosis
o/sMultiplenodules
. L-Thgroxine + Corlisone
. Surgerg if Lar"ge, Mal'rgnant
T[tlrFotD sScAD.l
COID Nodule
Mag be associaled with:' Reiro-periloneal {ibrosis. Mediaslinal {ibrosis. $clerosing Cholangiiis
DEffiS(ffi)
?hq I L1
Viral or Cornplicalion of Mumps
Pain in Gland, Knee. LiverEnlargemenl of fhgroidMrcRoscoPrc
Isthmectomg
@ffi.
^ESR. Thgroid Anlibodies)- ve. Thgroid Scan) @[I
PREDNISOLONE

Well-formed acini * askanazg eells
' U/8 ) Solitarg Nodule. Thuroid Scan > COLD Nodule
(Can'l differenliate belween follicularadenorna, Follicular carcinorna)
ag
Hemi-ThgroidecfomgOpen biopsg & Paraffin seciion
1L\P.4:locrr5 E{D,CF^IE ilRqW
ADEhb- MeUrr.qFyCancnr.nne Ahnctl|ortlA
eAlalrrdt!/,ffi
PRIIJIAI{/
thlotffi
?AqY I rc
ChJN'CALg Rapidlg growing swelling in lower part of froni of Neckg Earlg painless, Painful latelg (referred lo ear)V ln{illrative manifeslalionsA Meiaslaiic rnanifestalions
SIGNS:Z GENERAL) Cachexia. rnelasiasisg TOCAL SIGNS:g Hard gland, Earlg mobile & fixed lalielgA Trachea fixed lo Gland, Posilive Berrg's signg LNg+ + (Delphian. Cervical LNs)

ilRt+-Twr5 flW*NY WW P *hV I ?i
Exlernal radialion of Neck in children, Genelic faclors (Goodwen's $, Onco$ens)
Delphg [Nspilrtu;1ri
:
Fernale 2O-4O gears wiih
Solitary lhgroid swelling in Neck
I ll-defined rnass in{iltraling surroundings
wilh vascular Cf core
. loss of polaritg, signs of Milosis
Microscopic :
e{(D-+IoEoJCLoJo(s
v
)Fo+oo+t
Uq-o{+
eE-o
UU
=o12.9e-o
(Coo-ct,
(DFL
-s.o
Old Age, rapid progressive swelling in Neck
PRESSURE MANIFESIATIONS
* RLN ) Hoarseness of voice
* Carolid )Absenl carolid
pulsation (BERRY SIGN)
. Ugg@qlq1)Greg Unicenleric mass
. Miuoscopic:l) Clusters of2) Separated bg Fibrcus lissue
. Loss of polaritg * silns of melastasis
ETI0LOGY: SNG, Follicular adenorna, Hislopatholo$cal surprise
Fernale, Hislorg of 8N0 eilher:. Left wilhoul surgerg) Follicular carcinoma. Hislopathological surprise during subtolal
thgroideclomg bl 8N0
Fernale 40 grs.)mpid progressive swelling in Neck
. Mggrylg. )Brown Unicenleric mass
' Ulgrgsss&,l) Follicles wifh rrilrble degre rentialion.
. Loss of polaritg + signs of rnelaslasis
Bolilarg
Painful
Pulsating
0steolgtic

ilR4-Tw\5 htw*ht,ww
TUMOR & GLAND
l'l,*V I 1L
Dlffi ONurrrxeNntrp
. Tolal Thgroideclorng +
Cenlral Nodal Disseclion. Post-Op L-Thgroxin
R.eplacemenl &radioaclive iodine
LYMPH NODES
. CHILD) No Disseclion
. ADULT$) Prophglactic
Disseclion of cenlral group
of LNs. lf One LN is Affecied)Block
Disseclion of LNs of neck
RADIOACTIVE IODINE
. Deslrog ang rernnanls of norrnal thgroid iissue,
Ablale ang rnelaslasis of lurnor. STEPS:
Wait for manifeslalions of MYXEDEMA lo appear..
l) Give srnall dose of Radioaclive iodine
) Total bodg scan
2) lf there's *ve rnelaslasis) Large ablalive
dose of Radioaclive iodine
3) Posl-therapu scan afler few weeks
FOLLOW UP .. 5 gears post-operative..
. Everg 3 months do the following :
l) Clinicalexarninalion
2) Thgroid scanning
3) Iumors rnarkers
lf palient wilh residual turnor afler tolalthgroidectomg) Serum lhgroglobulin > Zngl ml
IF INOPEMBIE:. Surgical debulking. Pallialive Iracheoslorng
IF OPEMBLE:Tolal lhgroideclorng * Posl-
operative Radiotherapg &Chemotherapg
DlreT{Cus:. Funclion)Thgroid funclion : N0RMAL. MorDholoAu) U/S
(Solitarg Nodule,
Cgsl with papillarg projection)
' Morpholoqg & funclion :
lsolope scanning )COLD Nodule. FNABC
(ln follicular) Hemilhgroideclorng & Paraflin)
s3rrerNg:. CT, MRl, U/S. CXR, abdominal U/S. Bone scan (done after lotal lhgroidectomg)
FNE{DEnA]TTE0rgan profile "CBC,KF[,LF[,ECG"
. Posilron emission tomographg (PET)
.. To delecl RECURRENCE ..
Follicular carcinorna
lrcaled bg thgroidectorng
+ Post-op Athgroglobulin Level

ilPq-Twr5 ww*NvwwltvleWcAFclNo,lA r;*
'"J c1., I ffi
ETIOLOGY:. Sporadic ) Falal. Farnilial ) MEN ll = SIPPLE's $
CLINICAI PICTURE:
)'a*C-Cells
\z\
TYPE 0F PAIIENT: OLD Aged patienl
SIGNS:
tr GENERAT) Cachexia, Melaslasis
tr IOCAL:. Earlg mobile thgroid swelling, latelg fixed. NECK lgrnph nodes ) Enlarged , Hard. lnfillralive) Trachea, Carolid sheath (+ve Berrg's sign)
SPREAD:. LYMPHAIIC SPREAD) Mediaslinal LNs
. B[0OD SPREAD) liver, Skull nodules, ascilis
INVESIIGATIONS:. SCREENING ) Calcilonin, Calcium. DlAGN0Slg ) Ug/FNABC/Calcilonin (>0.08 nglnl). $IAGING) CT, CXR, U/S, Bone scan, Pre-OPERATIVE) CBC, KF[, [FI, FBS. EXCIUDE PHEOCHROMOCYTOMA)
TREATMENT:. fofa! lhgroidectomg * Cenlral Neck Nodal disseclion. SPOMDIC CASES) All the Paralhgroid is Preserved. FAMILIAT CASES)
l) Ireal(Combined Alpha & Beta Blockers ) Adrenalectomg)
2) Preserue YzPmalhgroid gland.. (for fear of hgpo-parathgroidisrn)
. Trealrnent of Complicalions
' Posl-operative Follow up everu 3 monlhs
!! Jrll 9! brtull
. Rapidlg progressive swelling in
lhe lower parl of fronl of neck. PAIN: earlg painless, lalelg painful
..Secrelion of serolonin... Diarrhea
'Bronchospasm. Flushing
. Dgspnea
. Dgsphagia, Hoarceness of voice,. Horner sundrorne
*ve Farnilg Historu + ,lt Calcitonin
= IOIAL IHYROIDECTOMY
even if Normal Gland

crFq-Twfi a{Docw ww ?hEV t ++
-
PARATHYROID ADENOMA PITUITARY TUMOR
PARATHYROID ADENOMA
PHEOCHROMOCTTOMA
f./'
Ii:,
it'v\
PANCREATIC IUMOR
t.JlEN - llA
MEDULTARY CARCINOMA PHEOCHROMOC\TOMA
tilEhl - llB
)1
ffi{*llD! vldl,6'. thytld,qtah3 b d&lhr,lDrEd ffilmt
MEDUTTARY CARCINOMA NEUROFIBROMA +HIRSHSPRUNG+
MARFANOID FEATURES

ilEI4-Tw$ 1a"]lW*WWW
.TRAPPING of inorganic iodide fiorn Blood
.@[!9! of iodide bg peroxidase enzgme inlo lodine
.@ru!E!qAM! binding of iodine wilh lgrcsine
bg Tgrosinase lo forrn M0N0- iodo lgrosine, Dl-iodo lgrosine.COUPUNG of rnono-iodo lgrosine lo forrn lg, T4 \^J€) unile wilh lhgroglobulin) Stored in Follicles
l- THE TIIYR0GIOSBAL DUCT; is related to cenlral part ofbone (rnoving of thgroglossal cgst up wilh tongue protrusion)
2. IHE T}IYROGLOSSAI CYSI;- MrU be present al ang level of lhgroglossal lracl in lhe midline from forarnen caecum to lhe suprastemal
nolch excepl in lhe reglion of the lhgroid carlilage where fhe figro$ossal lract is pushed io one side
- Trealed sur$callg bg rernoval of the lracl with cenlral pad of hgoid bone (as infection is inevltable)
3- rlmoclossAr FtsTU[A:- Alwags acquired (following infeclion, inadequate remova! of thgroglossal cgst)- lt is lined bg columnar Epithelium.
- ln long standing lhgroglossal {istula, fistula is silualed lour dorrrn in lhe rreck.
4- PENDRED'S $: due lo de{iciencg of peroxidase enzumer in which lhe patienl is deaf, mule, but NOI blind.
S IINOUAL IHYROID- MrU represenl the onlg thgrcid lissue.- Forms a rounded swelling at the forarnen caecum, cause irnpairmenl of speech or respiralorg obslruction.
- lt is besl lrealed bg full replacement wilh L-thgroxin or excision.
& MEDIAN ECI0PIC IHfRO|D) usuallg rnislaken as lhgrcglossalcgst
l- ln simple goifer, lhe mosl imporlanl faclor is dietary deliciencg of iodine (Ihe dailg requiranarl100-t25 qg)
2- Vegelables of brassica familg, PAS, Ca, lhiocganate, Carbirnazole and lhiouracil are goilrogenics.
3- ln diffuse hgperplastic goiter)lhgroid hormones level are normal (euthgroid).
& A colloid goiter is late stage of diffuse hgperylasia.
5. MUIIITIODUTAR GOITER,
- Onlg rnacroscopic nodule is found.. (Micrcscopic changes will be presenl throughoul the gland and
mag be one forrn of a clinicallg solitarg nodule.
- Irlodule mag be colloid or cellular, and cgslic degeneralion and hemorfiage arc oommon
0- Regading thgroid funclion lesls, no single tesl is conclusive & lf TSH is normal)lg, T4 arcn't needed.
7- Regrding FNABC:
- Ihe invesligalion of choice in discrele lhgroid surelling, Simple & quick, with excellenl patient com$ance- Cannol differenliale Belween Follicular Adenorna and carcinoma
8- Regardin! isotope lhgroid scan,
- Most useful in loxic adenoma of thgroid
- Cold nodule )Under aclive nodules (usuallg Malignanl nodule)
- Warm nodule )Acllve nodules
- Hot nodule )(her aslive nodules (usuallg lhgrcioxi,c nodule)
9- lndicalion of surgerg in isolaled thgroid swelling are: foxic adenoma , Pressute sgrnPlorns, Neoplasia, for
Cosmoslic purposes
l0- Regdin! largngeal paralgsis :
-30 Yo of cases arc idiopalhic, 3-4 % of palients have congenilal paralgsis of one of the vocal cords
() Do lndhecl laryngoscope before ang opemlion per.forned on lhe thgrcid gland for medicoJegal putposes )
ll- Invesligalion of choice in Sltl0 ) U/g
lf a dominant Nodule > 1.5 cm) FNABC (exclude malignancg)

2-
g-
1,)?4-TW\5 A{DoCENV WW ttu
PRIMARY THYROTOXICOSIS (Grave's disease): is an auloimrnune disease thal develops in a previouslg
healthg thgroid gland where the gland is enlarged or shows mild enlargemenl.
Thgroloxicosis should be suspecled in :- Children with growth spurt, Behaviora! problerns
- Un-explained tachgcardia, arrhulhmia, diarrhea, loss of weighl
- Resislanl heart failure
Effecls of Thgroloxicosis on Bone:. THYR0IOXIC0SIS ) 0steoporosis
. After operation) B0NE HUNGER.... (Osteoporolic bone wilhdraw Calcium from blood, manifesled bg Tetang)
Pretibial rngxederna:
- ls a thickening of the skin bg a rnucin-like deposit.
- MaU be cganolic when cold, Associated with clubbing of lingers and loes.
TREAIMENT OF THYROTOXICOSIS:
Disadvanla(e of anli-thuroid dru[s Advanlales of surgenl
a- Trealrnenl is prolonged
b- Failure rale afler 2 gears is 50%
c- ll is impossible to predicl which
palienl willgo inlo rernission
d- Some goilers enlarge and becorne
vascular durin( lrealrnenl
a- the goiler is removed
b- the cure is rapid
o- lhe cure rale is high
if surgerg is adequale
6- Regarding ITT. schedule for diffuse loxic goiler
a- 0ver 45 gears) radioaclive iodine
b- Under 45 gears * large goiter )surgergc- Under 45 gears + smallgoiler ) anti- lhgroid drugs
7- Surgerg is the TTI of choice in loxic nodular goiler as il doesn'l respond lo drugs rapidlg or lo radiolherapg
8- Ihe lsl line of TTT of Grave's disease is mainlg rnedica! for hope of perrnanenl rernission.
9- Patients on anti-thgroid drugs rnusl do CBC periodicallg for fear of AGRANUTOCYTOSI$
l0- Post-thgroideclorng slridor mag be due lo:a. Bilateral RLN injurg.
b. largngeal ederna.
c. Iracheal collapse.
d. Deep neck hernalorna.
ll- lndications of surgeru in Grave's disease include:
a) Large goiter which is uncornrnon wilh Grave's.
b) Failure of conservalive rneasures.
o) Suspicion of malignancg.
12- PEDIAIRIC GRAVE'S DISEASE: surgerg is rnore preferred because radio-iodine is poientiallg carcinogenic
and causes lale mgxederna and antithgroid drugs aren'l wilhout side effects.
13. THYROTOXC CRISES:
- An ER. case manalled in lCU.. (lV {luids, lV hgdrocortisone, Digoxin for hearl failure, Lugol's iodine & propranolol)
- MaU follow an unrelaled operalion, lnadequale Pre-oPeralive preparalion
- SUPPR0TIVE TTT for dehgdralion, hgperpgrexia, restlessness is essenlial in Thgrotoxic crises
14- EXOPHTHALMOS is a comrnon fealure of Grave's disease (Radioactive iodine lherapg is better avoided in ttT)
15- SECONDARY IHYROTOXICOSIS (Plumme/s diseasel :
- Develope on lop of multinodular ;loiler- ln Plummer's disease lhere're aclive inlernodular lissue wilh inaclive nodules.
- Cardiac sgmplorns are rnore prominenl in Plurnmer's disease lhan in Grave's disease.

lJRq-Twt5 ilpocru7ww ?AhY t 11
Rarelg caused bg enlargemenl of eclopic thgroid lissue in lhe rnediastinurn.
Asgrnplomalic and rnag presenl as dgspha$a, Palienls attend lo chesl clinic and diagnosed as "aslhma"ln severe cases lhere rnag be obslruction of superior Vena cava.
Recurrenl largngeal paralgsis is nol cornrnon.
TTT: Have lo be rernoved rneal.
- Presenls as rnulti nodular goiler, fealures of chronic lgmphocgtic ihgroiditis are comrnon on hislologg- lrg mgxedema wilhoul deteclable thgroid enlargernenl represents the end slage of the pathological process.
- Complicaiions: Ihgroid failure is cornrnon, lnuease lhe risk of lhgroid lgmphoma.
- Invesligations.. Aulo antibodies against thgroid peroxidase, thgroglobulin.
- ldeal TTT. of hashirnolo's thgroiditis is THYROXIN .. (DOESN'T ALWAY$ require thgroidectomg)
2. RIEDLE'S T}TYROIDITIg
- Thgroid iissue is replaced bg {ibrous lissue.. (Mediaslinal fibrosis) ..
- MrU be misdiagnosed as lhgroid carcinoma- Ihgroid scan shows no uplake over lhe swelling.
3. DE QUER.VAIN'S THYROIDITIS
- Due lo viral infection- ln tgpical sub-acule presenlalion of De-Quervian thgroidilis lhere's pain in lhe knee, liver rnalaise, and firrn
irregular enlarlernent of thgroid.- lnvesl'rgalions: Thgroid aniibodies are absenl.
Ihgroid malignancg is rnore in females lhan in male.
LATERAL ABBERANI THYROID... A melaslasis in arrival lgmph from an occuli thgroid carcinoma.
SPREAD: Papillary carcinorna)lgmphatic roule, Follicular carcinorna)blood & Anaplaslic
carcinoma)Local in{ihration of surrounding tissue
Melaslasis lo ceruical [N occurs in 50-60%.PAPIIIARY CARCINOMA
- The rnosl cornmon lrg mal'rgnant lhgroid lurnor, Slowesl growing lurnor & mag lurn lo anaplaslic forrn
- Dependent on T$H slimulalion.- Has a lendencg io become rnore rnalignanl wilh age.
- Not associaled wilh hoarseness of voice.
6- FOTLICULAR ADENOMA presenls clinicallg as a solitarg nodule, Best TTT is LOBECI0MY
N.B. (Distinction bel. Follicular adenorna and carcinorna can onlg be made bg hislopathologieal
examinalion, ln adenoma lhere is no invasion of lhe capsule or pericapsular blood vessels)
7. FOLTICUTAR CARCINOMA
- Thgroid cancer with mulliple bone rnetaslasis
- lf suspected) Hemi thgroidectorng is needed io diagnose it.
8- FNABC {indings are diagnoslic regarding papillarg carcinoma, bul nol a conclusive evidence regadin!
follicular carcinorna.
9. ANAPI.ASIIC CARCINOMA
- Usuallg affects old males & cang worsl prognosis.
- Iotal thgroidectorng is often impossible for anaplaslic carcinoma.
IO. MEDULTARY CARCINOMA
- A lurnor of C- cells derived frorn neural cresl with characlerislic amgloid slrorna and A calcilonin.
- MrU presenl wilh (Earache, hoarseness, sfridor, Enlarged cervical LN, Diarrhea due lo serolonin)
- ln thgroid carcinoma, Mediaslinal node involvernenl is a feature of medullarg catcinorna of lhgroid.
- The level of calcitonin falls after lhe resection of the lurnor.
II. PHEOCHROMOC\TOMA
- MrU be found at aorlic bifurcation.
- Rule of len ) lO% bilateral -lOTo exlru adrenal - lOTo multible
l-2-g-
4-5-
I. HA$HIMOTO IHYROIDITIS:

Toxb Nolttar Wrter4. Female with one palpable nodule in her neck- thgroid scan shows hol nodule.
Toxb Thyrolit Ndtle5. Middle aged fernale wilh past hislorg lo thgroid disease with or without exposure lo a
stressful condilion presenled wilh hgpertherrnia, arrhgthrnia up to corna
Thyrotoxic 6rbes6. Obese rnale, complaining of dgspnea, wilh hislorg of neck swelling which disappeared
recenllg , and pressure sgmploms appeared.
Retrostertal Wtter7. Middle aged Fernale with enlargemenl of lhgroid gland, thgroid scan shows cold
nodule & inter-nodular lissue
//as fiinoto's tltyrordrt b8.01d female with hard thgroid nodule, pressure manifeslalions, Frozen neck,
relroperiloneal fibrosis.
&rd/e's Tltyrorditrb
9. goun! female with solitarg lhgroid nodule & no toxic or pressure manifestalions
Paf'tta7 carcthor/a
10. Old female with pas"t hislorg of SNG, Rapidlg progressive swelling in neck,
picture sirnilar lo a skull abscess.. Thgroid scan shows cold nodule
follrfular cdrutlottldll. Old male with rapidlg progressive swelling in neck, absenl carotid pulsalion &
hoarseness of voice.
lJPt4-Twr5l. Youn! prelnanl female presenls wilh mild diffuse
enlargemenl of the thgroid gland occurs for firsl limein pregnancg and gives hislorg for the sarne condilionwith previous prelnancg which fades with deliverg.
DrTtse srnVle prter2. Young! fernale with N0 Historg of lhgroid disease
subjected to Psgchic lraurna, presenled wilhdiffuse enlargemenl of lhe gland, Toxic C/0
hrDocRNYww
Difuse to\tc lotter3. Middle aged fernale with Past hislorg of thgroid disease presenled wilh toxic
sgmptorns, 0n Palpation: Ihgroid was Nodular
?hqv t%
,haVlastb cdrcrloftia
12. Old age patienl with rapidlg prollressive swelling in neck, *ve farnilg historgpresenled with Diarrhea, Bronchospasm, Flushing (Carcinoid sgndrome)
,ilAnrury carcfuottld

ilP.q-Twt5 ww.iEN0 l"Rhw ? Aqv I n
- Give an explanation for: Papillarg carcinorna of thgroid should be
lrealed bg lotal ThgroideclorngKasr,2W)
- Managernenl of Thgroloxicosis, Trealrnenl of Prirnarg
thgrotoxicosis( r4ilar rl/,2o/2,2o//,-zml Au s/uns,2m/)
- Managernenl of solilarg lhgroid noduleG4il slhns2@2,2@5, r4ilar f'2@5
- r4ilar rl,L 2w.Z@4, 2fu5 )- Manalfernenl of ihgroid Neoplasia
( ,4n sfians,2@5 - r4ilar il'ZO// )- Thgro-glossal cgst : eiiologu , tupes and ClP , Trealrnenl
(r4rh stldt/s,2M, r4ilar f,2@5 - Ay'tar ril,2m )
- Multinodular goiler: investigalions, Cornplicalions04/tar f,2M, rAur f'2M)
- Toxic goiter: Tgpes and Trealrnenl04/rar f
' 2ob, 2@5, 2@4, r4y'ur f' 2a/)
- Huper-paralhgroidisrn: Diagnosis & Investigations(Alur fiZM, r4y'ur f,20b )
- Relro-slernal goiter: CIP
- Ihgrotoxic crisis: lnvesligalions
- Cornplications of lhgroideclorng
aa

ctBq'41ar5 VWW ?AqVt+0
SUR(
rllrclraet SafrutlAB.BCh - /////uersify

ww*tv lJ?wl ? hEv t +7.
r Cushing sundrorne! Pheochrornocglornar Hgperparathgroidisrn
1fr14-Tw\5 ENDoCFIE ilRqWt ?hqe t ffi
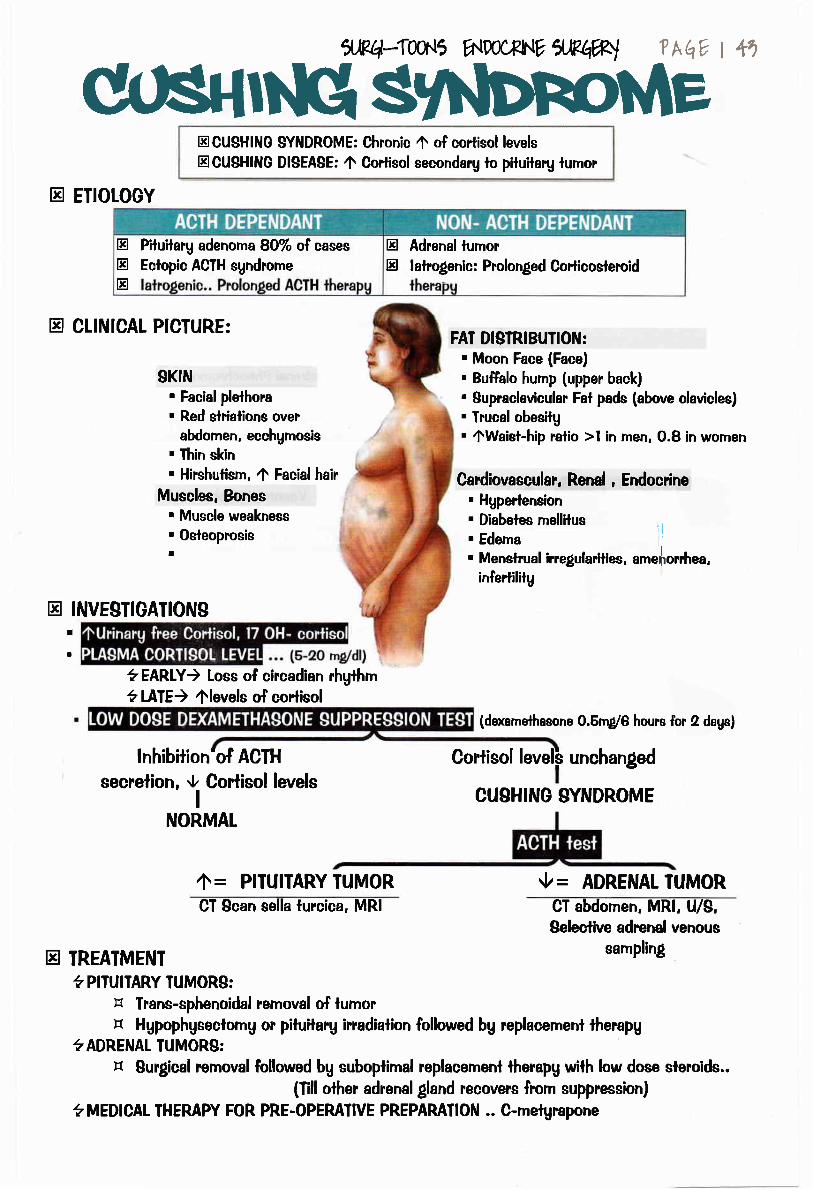
Wn{GlShbnoMetrCUSHlNG SYNDROME: Chronic t of cortisol levels
trCUSHING DI$EABE: 4 Cortisol secondarg lo pituilary lumor
tr ETIOTOGY
trtrtr
Plluilarg adenorna 80% of cases
Eclopic ACTH sgndrometr Adrenal tumortr lalrolenic: Prolonged Corticosleroid
tr CLINICAI PICTURE:
nl'$;,*,,,i,:::.",",
abdomen, ecchgrnosis. Thin skin. Hirshulism, 4 Facial hair
'il:iH#*i:"..
tr INVESTIGATIONSI
a
FAT DISIRIBUIION:. Moon Face (Face). Buffalo hump (upper back)
' Supraclavicular Fal pads (above clavicles). Trucal obesitg. 4Waiet-hip ratio >l in rnen, O.8 in wornen
Cardiovascular, Renal , Endocrine. Hgperlension. Diabetes mellilus. Edema 1l
. Menslrual irregulaillirs, amrJ,omh"r.infertilitg
(dexamelhasone O.5rn/6 hours for 2 dags)
Corliso! level$ unchanged
CUSHING SYNDROME
CT abdomen, MRl, U/S,Selestive adrenal venous
sampling
?EARLY) Loss of circadian rhg[hm?t-IiIE) flevels of cortisol
lnhibition'of ACTH
secrelion, O Corlisol levelsI
NORMAT
tr
ZIr = PITUITARY TUMOR {z = ADRENAT TUMORCT Scan sella lurcica, MRI
TREATMENT? PITUITARY TUMORS:
tr lrans-sphenoidal rernoval of lurnortr Hgpophgseclomg or piluilarg irradiation followed bg replacement therapg
?ADRENAL TUMORS:tr Sur$cal removal followed bg suboplimal rcplacement therapg wilh low dose slercids..
(Till olher adrenalgland recove!'s from suppression)
?MEDICAI THEMPY FOR PRE-OPEMIIVE PREPARAIIO!{ .. C-metgrapone

trtr
lLlPq-{wr5 A\lDpC4€hlV lJRhWl ?A v I ++
DEFINITION: Turnor of chromaffin tissues secretin! Catecholamines
ETIOLOGY:
E Forrned of Embrgonic Chrornaffin cells around abdorninal
aorla that Normallg atrophg during ChildhoodE Maior sites of Exlra-adrenal Pheochromoculoma
tr CTINICAL PICIURE
Recenl onsel of relinopathg wifh DM
Sgmplornatic HTN * Vasomolor phenomena or DM
HTN (e.0. Postural HTN
t - Iachgcardia, Palpitation- Swealing, pallor
- Anxielg , Trernors- Arrgthmia, precipilalion of angina
. HYPER,IROPH IC CARDIOMYOPATHY
. FEATURES OF "MEN II":
d
- Medullarg carcinoma
- Hgperpamlhgroidism\r t . ..U."..... \- - Neuroftbromalosis
tr INVESTIGATIONS. LABOMIORY ... 4 Urinarg VMA, Calecholarnines, Plasma Catecholarnines. MDIOLOGY ... Abdominal U/S, CT scan, MRl, Seleclive adrenal vein sampling
tr TREATMENT:. ADRENALECIOMY of diseased side afler Pre-operaiive preparalion bg Alpha
blockers 7-lO dags followed bg Beta blockers for 3-4 dags before operalionN.B. avoid using HALOIHANE in aneslhesia lo avoid arrgthmia
d
d6
tr Adulttr <lO7o Bilateral
tr lOTo malipnanl,lOTo
tr childtr 50% bilateral
tr Mau be oarl of "MEN ll"
. Sueening of Hgpertensive palients for Pheochromocglorna :

5"Rq*Twr5 rNDoCEtl' XRhWI ?Aqv t +6
H ,trOlDlSMEctopic secrelion of PIHbg small oell bronchial
carcinoma
ADENOMA:
- gz%ofcases
- Middle aged female
- Affecls I glandtr Olher causes:
e.g. Hgperplasia, Carcinoma,
Compensalorghgperplasia due toprolonged
hgpercalcemia(e.9. CRF,
Malabsorption)
tr After prolonged
secondarg
hgperparalhgroidism
tr CLINICAL PICTURE:
BONE
- Bone pain
- Pathological fraclures- Ostitis fibrosa cgslica
GIT
MOOD..( MORE !N PAilENTS >60 YEARS)
- Apathg, loss ofconcenlralion, Depression
- Anorexia, Nausea, Vomiting- PU, acute pancreatitis
STONE..( MORE rN PAT|ENTS <60 YEARB)
- Recurrent Renal slones- Nephrocalcinosis
tr INVESTIGATIONS:
TREATMENT
tr PRIMARY HYPERPARATHYROIDISM ) Surgical removal of enlarged gland- Adenoma) reseclion- Hgperplasia) removal of 43 ol gland & implanlalion of l/3 ln deltoid .
tr SEOONDARY HYPERPARAIHYROIDISM- t alpha hgdroxgl Vitamin D3
- Calcimimelics
tr TERTIARY HYPERPARATHYROIDISM- Total parathgr autotransplanlalion of parathgroid fragment
equa! lo normal size in arm Muscles
I
rl
FOR LOCALIZATION IN RECUR,RENT CASES
O Serum calcium except in 2rg
hgperparathgroidismV Serum Phosphorus
O Serum PTH
X-MY: multiple bone cgsls, reabsorplion
tr ffi...MOSTACCUMTEtr CT scan
tr TCnn

1JR{4-TW\5 ^IDOCRNV
ilPq%l
Regarding PARATHYROID HORMONE (PTH):- A peptide hormone- f Phosphorus excrelion in urine.- PTH serurn levels are Ain chronic renal failure.- Require vilarnin D as a Precursor.
ETIOLOGY OF HYPERPAMT}TYROIDISM:Hgperparalhgroidism resull from single adenorna (the most cornrnon cause) or mulliple adenorna,
Carcinorna is a rare cause.
CIINICAI PICTURE OF HYPERPAMT}TYROIDISM :
l- Hgperparathgroidism associaled wilh mulliple bone cgsls, can Presenl with renal slones.
2- As regard hgperparathgroidism, lhe commonest presentalion is asgmplomatic
hgpercalcemia.
3- Clinical fealures relaled lo hgperparalhgroidisma- Bone pain, multiple bone cgsls, palhological fraclureb- Renal slones.c- Abdominal Groan
d- Psgchic rnoan
4- Chvoslek's srgn is twitchin! of the facial rnuscles produced bg lapping over the
prorninence of facial bone in fionl of lragus of the ear in a person has lelang.
5- Pancrealitis is a recognized complicalion of hgperparathgroidism.
I NVESTIGATION$ OF }IYPERPAMT}IYROI DISM :
l- The biochemica! findings related to hgperpatalhgroidism:r J Serurn alkaline Phosphatase. 1 Ca in urine.
2- Radionuclide scan is the besf wag of preoperalive localizalion of paralhgroid adenorna.
TREATMENT OF HYPERPAMTHYROI DISM :
l- Hgperparaihgroidism can'l be cured bg using anli- parathgroid hormone drugs.
2- TfT. of hgperparathgroidisml'e: Surlery2ry : rnedical
3ry: surterg

ilR{+-{wr' ww,PNY XMW ? AqY | +6

tblichaetlr',B.Edh Arn s/uns unirersl;4

cJ,,Eq-Twr.t5 htpOCFNE f/-tp4B{ ? Aq I 60
Liporna
NeurofibrornaHernan$orna
Vascular rnalforrnalions
Derrnoid cgstFistulas
Sirnple ganllionMiscellaneous lopics

@@@ glTE : Back, shoulder,
Bullocks@ Attached to Skin
@ Well de{ined slippergedge
@ Mobile
@
@
@
@
@
SlfE: ForeheadFirm
Nol allached lo skinNO slipperg edgeLirnited mobilitg
swelling, of gradual onset
DDiagnosed bg MRI
DDD: Osleo-arthritis,Baker's Cgst
@ MICRO$COHCPICTURE:Aggregation of Fat o"lb)@,separaled bg fibrous liesue, contains Blood vessels
tNVESTIGAIIONS: ... Clinicallg diagnosed...BPECIFIC: Excisional biopsg, X-rag, Spira! CT spinal cord
Treaimenl of choice is Enuclealion of tumor frorn its
l./{Pq-Twn5 a.Doc*hlE 5JR4W
ODANOEROUS)COMPTICAT!ONS:- Respiralorg
obslruction- lnlussusceplion
@Related toLong!, flal bones
@Diagnosis: MRI
:IC MISCELLANEOUS 'F
@Site:Spina! cord
BUTIHHITN
6ifi@CP:
Pressurernanifeslalions
?AEV t d
@
@
@
Neuro-LipomaDercum disease
Complicated lipoma
@ Palient: Fernale, post-rnenopausa! patient
@ Site: lower limb@ Clinical oiclure:
Small, rnulliple,Painful swellings
@Sile: Ihighs,shoulders
@OE : becornesrnore {irrn onMuscularconlraclion
SUBMUCOUS> RespiralorgObstruclion & lnlesiinallnlussceplionR,ETRO-PERITONEAL>PremalignanlDCTRADURAL) Pressuremanifeslalions
@
@
Relro-periloneal lipomaSC lipoma in fhighs, Bul^locks(Slighrlg higher incidence)

Hernangiorna
SlrawberrgHernangiorna
CONGENITAL
Capillarg
Porl Winesfain
t-sgufuib.[r
Low Flow
SalrnonPatch
loJ +rbr rrr i.t
Vascularrnalforrnalions
VenousI
CavernousHernan$orna
prrS .g.url,=lifr: Loi
Venousmalformalion
il84-T0ur5 wwtxNr' a^Pqw ? hq, t 61-
LgrnphI
CgsticHggroma(Cavernous
Lgmphangioma)
High Flow
DEFINITION:Mal-arrangemenl of Normal tissues
Arterial
CersoidAneurgsrn
,=rrJ pf,1i
OTHERS
. Pigmenled skin Iesions
. Neuro-fibromas
. Lung!, brain hamarlomas
A-V Fistula
Congenital
Sgndrornes.Slurge weber.Klippel Trenaunag. Kasabuch Merrill
Acquired(traumalic)

MOST COMMON TYPE
rYPE(l):- AD, Chrornosorne 17
. CTINICAL PICTUR.E:
Tenderness+ Caf6 au lail palches+Pheochromocgloma(if a part of MEN llb $)
- Special characler in fgpe(l):Alnlra cranial iension
TYPE(ll) ACOUSilC NEUR,OMA:
- Chromosorne 22- Associaled with Acoustic Nerve
lumor- CtlNlCAt PICIURE: Painful ,
leading lo Deafness & vertigo
Caf6 au laitpatches PTEXIFORM NEUR.OMA
@ Cgstic swelling in lhe face@ Palpation: Sensalion of
bag of worrns
lRq-Twr5 A.DoCFNE 5tM4W ? AqV I m
C/O: painless swelling, of gradual onsel, progressive courseo/E:
@Site: Scalp, face, lrunk@Consistencu: Sofr
@DEFINITION: Tumor like rnassforrned frorn Nerue sheaih
COM Ptl CATI ONB :_Mag lurn Mal'rgnant) "Neuro-fibrosa rcoma"
@Congenilal disease@Site: Limbs@Clinical picture:
Hgpertrophg
TREATMENT:
- lf sin$e) Excision
@ Not atlached lo skin
@ Moves across Nerve aLoUiJJI iirrl,ii
- lf Multiple: "Let lhe patient die in peace nol in pieces" !!
Caf6 au lail palches
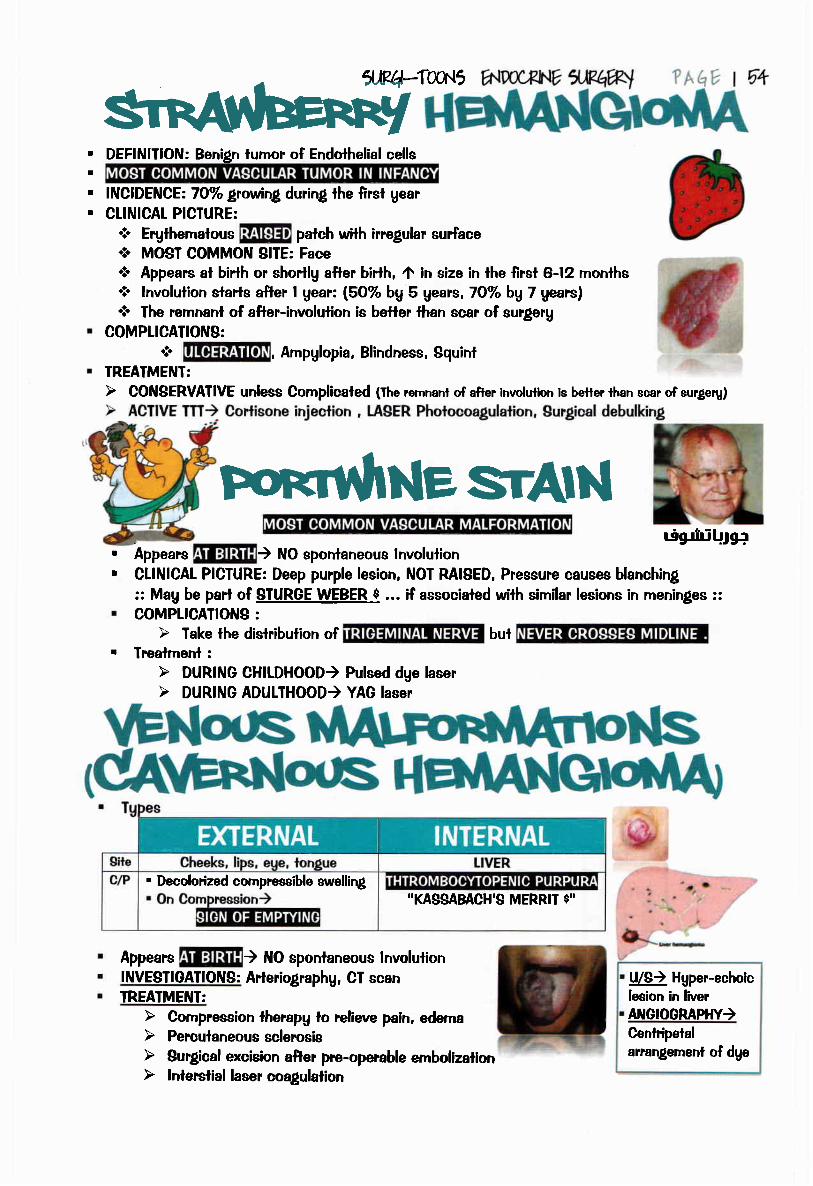
, DEFINITION: Benign furnor of Endolhelial cells
. INCIDENCE:7OTo growing during lhe first gear
. CLINICAT PICTURE:
* Erylhernatous palch with irregular surface* MOST COMMON SITE: Face* Appears at birth or shortlg a$er birlh, 4 in size in lhe first 6-12 rnonlhs* lnvolulion starts afler I gear: (5O% bg 5 gears, TOyo bg 7 gears)* The remnanl of after-involution is better lhan scar d surgerg
COMPLICATIONS:
* , Ampglopia, Blindness, SquinlTREATMENT:
t
I
MNesrAlNAppears ) NO sponlaneous lnvolulionCLINICAL PICTURE: Deep purple lesion, NOT RAISED, Pressure causes blanching:: Mag be parl of SIURGE WEBER, $ ... if associaled with similar lesions in meninges ::COMPLICATIONS :
. Trealmenl :
. Decolorized compressible swelling
Appears ) ttlO sponlaneous lnvolulionINVE$TIOATIONS: Arteriographg, CT scanTREAIMEIIIT:
r-iglriri Lr.lgc
"KASSABACH'g MERRI $"
U/S) Hgper-echoiclesion in liverAI'IGIOORAPIIY)Cenlripelalarrangement of dge

lJ?{44wr5 ww,PNY ilRq%l ?hqv t 55
. Mosl common sile€. gCAtP (lemporal , Occipiia! relion).w.
N. C/O: Headache + cosmelic disliguremenl* O/E: Waler harnrner pulse, lrregular swelling with norrnal
overlging skin, Pulsaiing with machinerg murmur on auscullalion
' !.Eyes!!Et!ons.!l) Doppler, Duplex2l ECA an$ographg3) Xrag) Rarifaclion of bones
. Trealmenl :
(Semisitting posilion, Hgpolensive GA . Pre-operalive Ernbolisalion , ligalion of ECA )
Nurnber SingleSite Rool of neck in Posterior trianfle,
suoerlicial lo slernornasloid ms.Size large
Shape RoundedSurface irregular
Edge il! de{inedConsislencg Lax, Custic
Specialcharaclers
I
T
I
. DD : Branchial Cgst
frealment:
Mr APPears in Neonales
Sequeslration
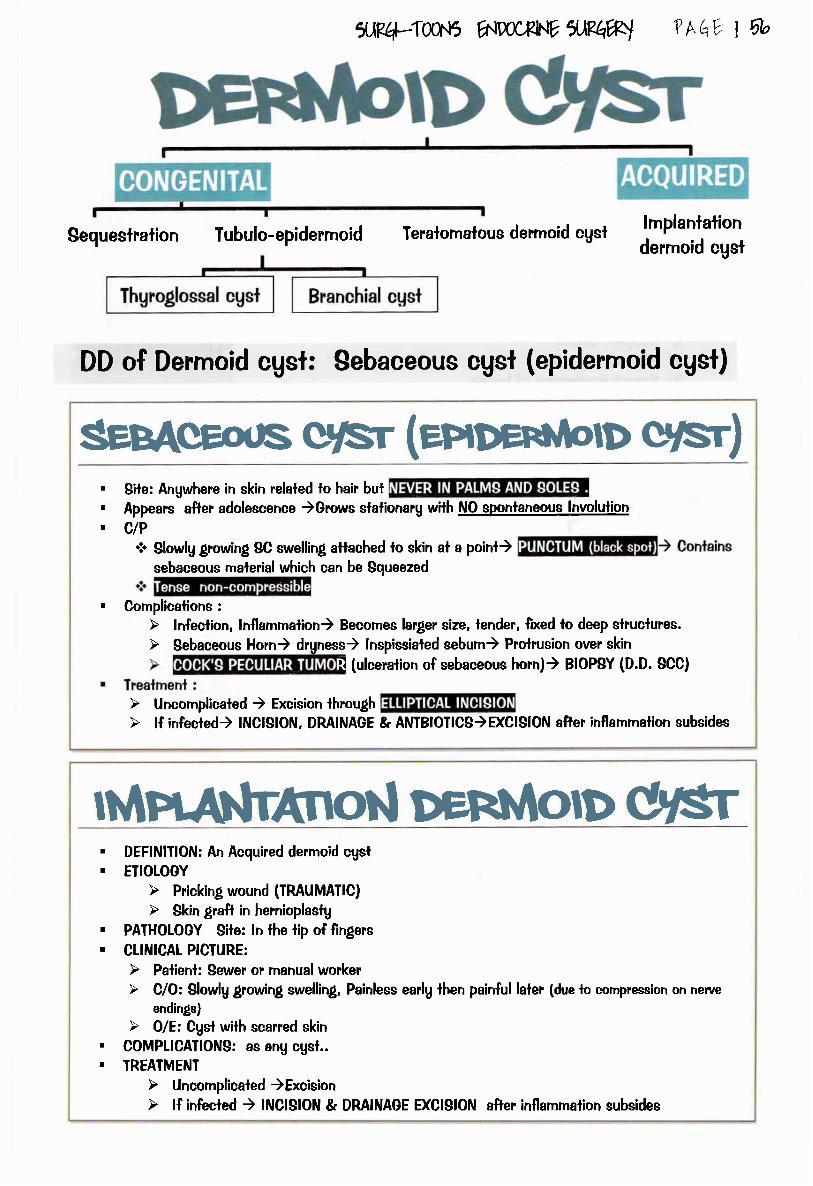
ilRq-Twr5 A{rcruV ffiqw
DD of Derrnoid cgsi: Sebaceous cusl (epiderrnoid cust)
Tubulo-epiderrnoid
crrsr (enOennmD q/sr). Bile: Angwhere in skin relaled lo hair bul. Appears after adolescence )Grows slalionarg with NO sDonlaneous lnvolulion. CIP
* Slowlg growing SC swelling attached lo skin al a point)sebaceous rnalerial which can be Squeezed
Teralomalous derrnoid cgst
Thq* t 5b
. Cornplicalions :
lmplanlationdermoid cusl
MffiAnol.l g/srI
t
DEFINIIION: An Acquired derrnoid cgslEIIOTOGY
PATHOTOGY Site: ln the tip of fingers
CLINICAL PICIURE:
endings)
COMPIICAIIONS: as anu cgsl..TREATMENT
! (ulceration of sebaceous horn)) BIOPBY (D.D. SCC)
I
I
I
!

ilPq-Twr5 ww*NV IJP^W
N.B. Branchial cgst, Thgroglossal cgst ... See Pedialrics surgerg
?hqv t 67
. Infeclion )rupture
. Inadequale excision ofcgst
Since birth . Rupture. lncornplele
excision orincision
, Opening is near midline or lothe Left side
. Viscous discharge or pus
. Parliallu deep to sternornasloidrnuscle giving Mucoid discharge
rich in Choleslerol
DEFINIIION: Chronic cgsl conlaining rnucoid malerial, relaled lo a lendon
EIIOLOGY: Mucoid degeneralion of {ibrous lissue of lendon sheath
C/O: Painless swelling al dorsurn of hand or around ankle
o/E:
coMPUCATTONS:
INVESTIGATIONS:
TREAIMENT :
Moves across lendonMobilitg V bg Pulling on lendon

M roPlcs@ Port wine@ 2rg varicose veins
due lo A-V fislula
e.B4-TooN5 hlDoCFlNtr ilRhwl
@ Weak poirrl in lhgroid membranep@ Cgstic swelling in the Neck
@ Becomes hominenl on Straining
Cornmon associalion wilh Port wine stain
@ Capillarg vascular rnalformalion@ Leplo-rneningeal AV rnalforrnalions
@ AV Malforrnalion in Exlremiiies
@ Sile: On one side of longue
@ ORIOIN: Sub-lingual gland
@ Cgstic, Translucenl
@ Blood vessels ovel il, Mucous rnembrane
@ Crossed bg Wharton's ducl@ lf ruplured) Pass belween lhe Muscles
io lhe neck (PLUNGING TYPE)
@ Trealmenl : Marsupilizalion (deroo{ing1)
@ Hernialion of Lung apex lhrough Sibson's
@ Cgstic swelling in Supra-clavicular region
@ Prorninenl on slraining
?^qv t 56
@ Hemangioma *Ihrombocgtopenia
@ Vascular lumor Ieading to9Platelet & other bleeding
disorders
@ Complicalions: DIC
@ Pre-patellar : Housemaid
@ Olecranon : Sludenls@ Over head of shoulder : Porlers
@ Over big toe : Bunion
iijglLuLtll iiy gaJJI , [l+JI ii 14rtr a
Exlends begond the edges of lhe wound
@ Site : Face, neck, fionl of Chest &
@ Locallg malignani lurnor in a Mutipara fernale
@ Cornrnon with OARDENER $
@ Site:- Al site of previous sur$cal incision
- From the reclus shealh, Rl >Li. NEVER IN MTDLINE
@ Best invesi'rtalions : MRI
abdornen
@ Comrnon in Negros
@ Have inherited lendencg
@ Acule: 1';o; ) Chronic: Uirf.li
@ Occurs in rnidline of the back of kna,rr
@ lf ruptures) Severe pain (DD : DW)
@ Treatmenl:- Surglical excision with safetg rnargin 2.5 cm *
Post-operative radiolherapu lo avoid recumence
I,Jat

ilRq*TwN5 'NDoCF[.lVflR{1W
?h Y I E
Acuie Bacterial SialoadenilisSalivarg sloneSalivarg fistulaSalivarg turnors
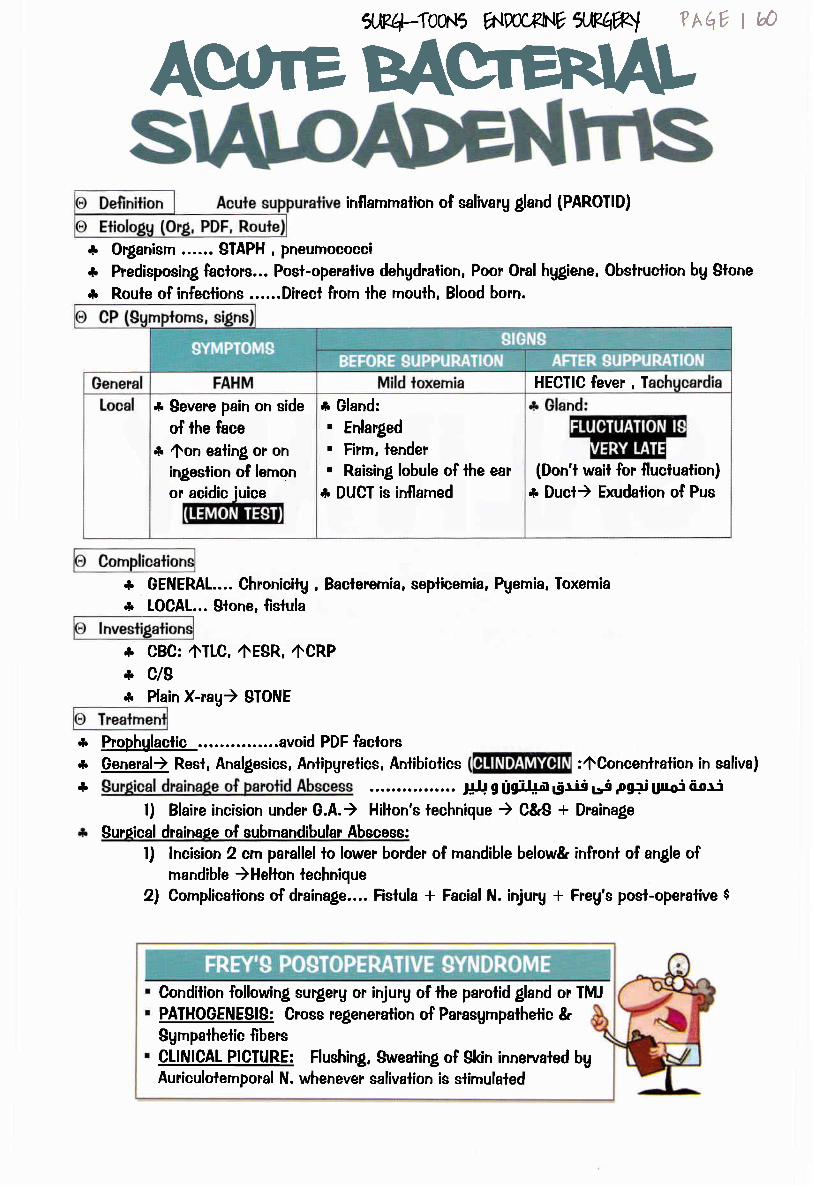
Sffi* Organism ...... STAPH , pneurnococci
.r Predisposing faclors... Posl-operalive dehgdralion, Poor Oral hggiene, Obslruction bg Slone
& Route of infections ......Direcl from lhe mouth, Blood born.
5er4-Twt5 hlpoC^RNE 5WW
inflammation of salivarg gland (PAROTID)
* Severe pain on side
of the face
* fon ealing or oningeslion of lernon
or acidic iuice
?Aqv | @
.r GENERAL.... Chronicilg , Baclerernia, seplicemia, Pgernia, Toxemia
* LOCAL... Slone, fistula
* Gland:. Enlarged. Firm, lender. Raising, lobule of lhe ear
* DUCT is inflamed
***
CBC: 4ILC, 4EgR, ACRPc/g
.r
**
Prophglaclic ..avoid PDF faclorsGeneral) Resl, Analgesics, Antipgretics, Anlibiotics
Plain X-rag) 9TONE
... ,;J,; g figif+a 6rii Lrs pgrp Ulroi 6-0r:
l) Blaire incision under G.A.) Hihon's lechnique ) C&S * Drainage
Suroical drainaoe of subrnandibular Abscess:
HECTIC fever , T
l) lncision 2 qn parallel io lower border of mandible below& infronl of angle ofmandible )Helton technique
2) Complicalions of draina!e.... Fislula * Facial N. injurg * Freg's post-operalive $
(Don't wail for fluctualion)* Duct) Erudalion of Pus
Condition following surgerg or injury of the parolid gland or fMJPAIHOGENEBIS: Cross regeneration of Parasgmpathetic &Sgmpathetic fibersCLINICAL PICTURE: Flushing, Sweating of Skin innervaled bgAurieulolernporal N. whenever salivaiion is slimulaled
:OConcenlration in saliva)

xRq,-Tw.J5 rNDocF[.], *R@l
lncidence. Submandibular > parotid (50:l)
- More viscid secrelion , 40oncenlralion ol Ca*z
- Ducl ascends upwards ... lnadequale drainage- Ori{ice lies in lhe floor of moulh ... Could be blocked
faclors. lnfeclions(ex: Chrcnicsialoadenitis)
ofren's $)
... MAINY ASYMPTOMATIC .... Episodes of pain afler eating followed bg relief in the side of Face
. Submandibular slone (radiopaque)) appear with x-rau (Closed mouth)
. Parolid slone (radiolucent)) appear with Sialographg
. U/g) Echogenic stone * acousiic shadowing
frealmentSubmandibular )submandibular sialo-adenectomgParotid Gland ) Superficial conservalive PAROTIDECTOMYglone in Duct) according to place:
l) Slone from ori{ice of Parolid Gland) Mealolomg2) Blone in ducl) Removal under loca! aneslhesia
3) lf Recurrerrl) Submandibular sialo-adeneclomg
- lnfernal) requires no TTf
Clinical
?AqY I bl
@ Ett"t"gs;l
- Trauma, inflammalion, Neoplasm
@-IUGI- Exlernal) requires TTT
T
I
. lF EXTERNAL) Waterg discharge from opening * Eczema of skin around opening
Trealmenl
Submandibular fislula) submandibular Sialo-adeneclomgPAROTID GI-AI{D
- CON8ERVATIVE: Parasgmpathetic drugs for I week- Avulsion of auriculolemporal N. or superficial conseryalive parotideclomg- lf fails) fotul conservalive parolidectomg
PAROTID DUCI:- MAS$EIERIC) Excision with end lo end anaslomosis- PRE-MA$8EIERIC) re-implanlalion of ducl in Buccinalor

lncidence
Macro.
2T
Micro.Malignancg
More comrnon in Males
I
ll tI lrttll 117t
c/o
Mullicenlric * lncomplele Capsule
Sile
Epithelial cells * rnucinous rnalerial. Benign .. Malignanl lransformalion
occurs after lO uears (rare in 2-3%l
ttrat
Size
(Wharton's lurnor). (Adenolgmphoma)(Papillarg cgsf-adenoma-lgrnphornalosurn)
Shape
SurfaceConsislencg
tvt [0
Mobililu
Specialcharacler
Parolid )Superficial parl
lnvesligalione
Painless, slowlg growing swelling in the side of lhe face
4ilP.14:loN5 A'DoCxhlE 1,,Mh#}l
Firrn or cuslic.. (NI:M:EIElIl-rl
Trealrnenl
Variable
rt [l) rvl tll iI 2 I
lrreqularLobulated
,llOTo ol Parotid lurnors,
. CTscan
. Tc99 ) COLD spol (Avascular)
. Free needle biopsu
freelq
Colurnnar eoilhelium * Lurnohoid lissueCgstic, encapsulaled lumor
Old aEe, smokers
mobile
SURGICAL ITI ....( see Ialerl
]
MUCO.EPIDER,MOID CARCINOMA. Mosl common lgpe. Sheers of Columnar + squamous epilhelium
ADENOID CYSTIC CARCINOMA. Most cornrnon rnalignancu arnong Minor
Parolid ) Superlicial parl,M
rI
I
a
4Gland size ...flumorVGland size ...4MalignancgMosl lumors are BENIGNMore common in parolid
m
salivarg glandsI
I
I
(Mgo-epithelial + epithelia! cells)ACINIC CEIT CAR,CINOMA
. Serous acini, ONIY lN PAROTID GLAND
ADENOCARCINOMA ... Bad prognosisCAR.CINOMA EX.PLEOMORPHIC ADENOMAUN DI FFER.ENIIATED CAR,CI NOMA
I
CfscanTc99 ) HOT spot
Conservalive supet"flicial parolideclomq
Sgrnploms. Pain: Awith maslicalion. Swelling on the side of face. Dislurbance Of funclion ....
Signs of rnalignanl turnor .... Firm lo hard. lrregular, Nodular surface. lll-defined edge, lnfillralive lo skin,. LNs **
lnvesl'rgalions:. For diagnosis) fc99 (COLD) + Biopsg. For staging) CT, FNABC
Facial N. palsg
SWELLING
vessels

PARTID GLAND:. Superficia! conserualive parotidectomg. Tolalconservaliveparolideclorng
(preserualion of facial N.)gU BMANDI BUI.AR GI.AND GLAND:
gubmandibular sialadeneclorng
3 nenes could be injured:l) Facial N. (Ceruical & mandibular Br.)2l Lingual N.
PARIID GLAND:. Buper"{icial conservativeparolideclomg
IF OPEMBLE:. Total radical parctideclomg. folal block disseclion of neck LNs. Posl-operafiveRadiolherapg
IF OPERABLE:
COMMANDO OPERATION. Tolal radical submandibular
sialadeneclomg. Hemi-mandibuleclomg. Block disseciion of LNS
?hqv I v)ilR+-TWr5 ,N90C8N' *fr@l

t.2.
3.
4.
5.
6.
Lipoma is a universal lurnor.Plexiform Neurofibrornalosis NEVER affeclsTR,IGEMINAT NERVE
Branchial cgst is best differenlialed from coldabscess bg conlaining cholesterol crgslals.CYSTIC HYGROMA can be the EARLIEST
$WELLING OF THE NECK lo appear in life.
Cervical LNs are "300" oul of the 80O lgmph
nodes in the bodg
T}MOGTOSSAL FISIULA:
5,R4-TW'V wu[r*N?ilRhry
- MaU follow infeclion, inadequaie remova! of lhgroglossal cgsl.- lt is lined bg columnar epitheliurn and never be congenilal
Thgroglossal cgsl Mag be presenl in ang part of the thgroglossal fracl.
t.2.3.4.5.
MNUTA is lhe MOST COMMON indicalion for rernoval of sublingual salivarg gland.
Mosl cornrnon salivarg lurnor is PLEOMORPHIC ADENOMA
Mosl comrnon sile for acule baclerial sialoadenilis is PAROTID OLAND
Sjogren's $ affecls 4 glands) 3 salivary (submandibular, sublingual, parolid)* Lacrimalgland
?hqv I b+
' ll's Stones are lheMOST OPAQUE
' lt's secrelions are
mosl MUCINOUS. ll has lhe TEAST
TUMOURg. ll's Tumors are mosl
MALIGNANI
. lf's Slones are lheMOSI MDIO-IUCENT
. lt's secrelions are lhemosl SEROUS
. ll has MOSI IUMOURS
. ll's lurnors are MostBENIGN
. EOTI of sativarg slones arise
from Submandibular Gland. Gland secrelions: Viscid
+ ACalcium concenlralion. Ducl ascends upwards:
Orifice lies in floor of rnoulh

l. Middle aged male or fernale complaining ofpainless swelling in shoulder accideniallgdiscovered. Clinical exarnination shows lhal itis lobulaled and attached lo skin bg mulliplepoinls but mobile over deep slrucfures.
Sttbcttanarc lrpna,2. Palienl complaining of lim painless swelling in the forehead 't have a slipperg edge.
Sfu filtU lryna,4. Palienl presenled with painless swellings lhal move onlg across lhe neFves of gradual
onsel slowlg progressive course associated with dark brown palches on lhe back. Ihepatient lives positive familg historg to lhe same condilion.
Qeteralful ilerofibronatosrb Ylil fuklrhg llatset s dbasd.ChiH presenls with dark puryle lesion not raised above lhe surfiace. Pressure causes
blanching of the color. Molher sags that if's presenl since bidh.
Pofi fftrle stamAdult male presenls with slowlg growin! painless subculaneous swelling wilh black
spof. On squeezingil discharges sebum.
Sebaails cystFemale patieni arcund 2O gears old presents with a slowlg growing painless swelling atlhe laleral side of lhe uppel part of lhe neck protruding benealh the anlerior border ofsternomastoid .
Bratcltra/ cyst8. An adull male presenls wilh painless swelling rnostlg al lhe dorsum of the hand, lense,
cgslic, rounded relaled lo a tendon and its mobilitg decrease bg pulling on lhe lendon.
ww/Pw1frqw ?hqv I 6
5.
.+xte Baterral shlo afuiitrb,2. Adull male presenied wilh painless slowlg growing swelling in the side of lhe face
elevaling lobule of lhe ear. On examinalion lhe swelling is irregular, Iobulated, freelg
mobile, no ceruical LN enlargemenl.
SrnVh ldrdtotl9. ltlewborn presents wilh large single cgslic swelling al poslerior lriangle of lhe neck.
Trans-illuminalion lesl is posifive.
6yshb lrygrona,lO. Patienl presents wilh cgslic, bluish ,translucenl swelling wilh prominenl blood vessels
on ils surfiace on lhe floor of the moulh.
foMa
t. Adult male C/O of painful swelling in the sile of lhe face, Awilh lernon ingeslion.
PlnuaVhrb d&tllfi/a

I Give an explanalion : Slones of lhe Parolid salivarggland ate rare and less cornrnon than lhose of thesubrnandibular salivarg lllands
(Kasn 2@nI Salivaru neoplasrns
( Kasn 2d/ )! Manalernent of salivaru slones
( r4ilarf'2W )r Managernent of paroiid abscess
(Kdsr'2M )r Liporna : fgpes, Diagnosis, TTT
Kasr, ZO@, Au shans,2@4, r4lur rl/, ZooZ)r sebaceous cgst : Cornplications, Pathologu,
ManalernenlKasn 2@Z Ail siaills,2005, ,4y'tar f, 2@Z 2@4)
?ifr+IwJ6 6lD0CFt'1tr lrRqBY ?hqv I b
r Derrnoid cgst
I Cgstic hggrorna
r Neurofibrornatosis
( ,4trar f,2@6, ,4y'tar;,29p( )
G4h siafils,2M)
O+i/ sfiafils,2M )




aa
Definition
iologg (Org, PDF, Roule
* Organisrn ..................r........
1Rq-TWr5 A{DoCFhltr XMW
* Prgdisposin! factors ....t........* Roulg of infgctions ... . ... . .. . . . ..
aaaaaaaaaaaaaaaaoaaaaaaaaaaa
* Sitg .................r....* Patho
agngSJS ......................
?hhv t 10
. Pain: Dull aching then
Throbbing. Swelling of lissues. Loss of function
Cornoli
* Genera! >Baclerernia, seplicemia, Pgemia, foxernia
. Definition
. Etiologg
* Loca!: Chronicilg, Pus loculus, Spread
a
lnvesti
. Palhologg
. Clinical piclure
. Complicalions
* CBC )Leucocglosis in mosl of infeclions
. lnveslitalions
HECTIC fever , Tachucardia
* c/s
. Swelling) Hot, red ,lender
. LNS) Enlarged, elastic,lender, Mobile
* Plain X-rag
D Trealrn
* lnvesligations according lo sile...
* General) R.A.A.A... Resl, Analgesics, Anfipgrelics, Antibiolics (AUGMENITN)
* LocalI
I
aaaaaaaaaaaaaaa
Hol FornenlalionAclivg lrgalrngnl: ...................

SJRq.-TW]'S rNDoCFX.ltr ilRhw
Definition ... Localized suppurative inflammation
iolo{u (OTI- PDF, Route
*SKIN, NECK ABSCE$S) Sraph (coagulase *ve), ABDOMINAL ABSCESS> EOoli.
* PDF) Bad general condition, Slasis, Bad hggiene
CP (Sgmptorns,
Special signs according to tgpe :
Breasl, brain(4l0T), Lung (pus on poslural drainale),Liver, peri-nephric, Sub-phrenic , cold abscess
icalions
General ) Bacferemia, septicemia, Pgemia, Toxemia
Local :
ANTIBIOMA
Chrcnicitg, Spread, Sinus, Fistula
CBC ) Leucocglosis
c&sPlain X-rag, CT scan, MRI
(According lo site of abscess)
?hqv I ?r
**
@
@
@
&
**
***
TTT. Of Predisposing factorsGeneral)Resl, AAI (flugmenlin)
Local. Resl, Hol Fomeniation. lncision & Drainage .................
:: INCISION & DRAINAGE ::O Under general aneslhesia
O lncision )(long, dependenl, never crosrs a skin
creaser parallel lo imporlanl Slructures)O lntroduce {inger lo break ALL septae
O Packing for 48 hours
O Dressing everg dag unlil co@OFor importanl strrtfur"* ) @
. tf Amoebic liver abscess, Brain, Cold abscess ) Aspiralion
. Chronic abscess: tf Thin walled) lncision & drainage , !Ilh!g@!!gd) Excision
* Roule ) Direcl, Blood, Lgrnphatics, lhrough nalural Passages.
Peripheral zone) rSlrlro!Hgperemia
lntermediale zone)69!5 ff '(J raGranulalion tissue Cenlral zone) 6+rh? iiJ{io
Mimo-organisrn# dead WBCs
. $wellinS) Hol, red ,lender. Pain : Dull aching) Throbbing,V bg elevalion of the part
. Surelling of lissues
. Loss of funclion tale fluctualion
O Breast
O Proslaleo ParolidO Perineurn
o Pulp space

Non suppuralive infeclion of loose
Conneclive lissue :qD dllrh s r+ppi
xfrq-Twr5 E{rccFhlE ilPAW ? Aqv I
OENERAL)FAHM .... LOCAL)Pain, swellinq, disturbance of funclion
oooo
Tender
Duskg red
Hot area wilh induraled edge
* Post-strept GN (after skin inf.)
* Scarlel fever
* slRs (coMMoN coMPIcATloNs)
I
* Lumphederna, R.heurnalic hearl
Non suppuralive infeclion ofSuperficial Lgmphatic vessels r)A>i
olal\ rEonn oiVeubtq o:qp q d\irJ\
( lf no response >48 hrs)euspecl abscess )
Infeclion of ) Perifolliculilis
Give Erulhromucin if Pl. is
ORGANI$M: Slaph. Aureus ..()Nemoloxin)
O Firg red swelling in face &exlrernilies
lt
A/M + Rest *Hol fomenlalion
TREATMENT) lmprove general condilion (Control DM,
nulrilion, Vitamins) + MA * Resl, fornenlalion- Antibiotics ) Flucloxacilin or(Augmenfin)
* Seplicemia
* Facia! ergsipelas) Cavernous
sinus lhrombosis
* Recurrence) Block lgmphatics
ciultrn iln: (Boil subsides leaving thick indurated arca)
Palient is isolaled(As disease is highlg contagious)
oooo
ORGANISM: Slaph aureus) Necroloxin )lnfeclion of SC lissue
ffi [ffi :HHl :,X,I'lii#li'mnPATHOIOGY: lnfeclion slarls in hair follicle) Spreads to SC fissue)Loculafed abscess
ooo
) Each bursl on Surface individuallg
CIINICAL PICIURE: Multiple puslules appea? on surfaceCOMPLICATIONS: Chronicilg, CAVERNOUS SINUS IHROMBO$I$IR.EATMENT: - Resf, AAA (Flucloxacilin), lrnprove leneral condilion
- lf Pus is formed:. Cruciale incision& Debridemenl of necrolic tissue. Glgcerine Mg sulfate lill sloughing occurs. Dressing until healthg lissue is fomed
' Skin Graft
I
Etirlt+f

cJ'JF.q-Twr5 ,NDocElNltr IJRqW\ ? hqY I 71
DEFINITION:O Bilaleral diffuse Cellulitis of floor of mo
ORGANISM:
O Mixed infection (e.g. SIREPT... moulh
ROUTE OF SPREAD:
O Due to Direcl spread frorn infecledof longue or submandibular sialoade
CLINICAL PICTURE:O C/O)Bevere dgsphagia & Dgspnea, surrtruarru,r
o o/E:-CERVICAL: Swelling in submandibular region
TREATMENT:O EARLY)massive doses of Antibiotics (Amoxicillin,
Melronidazole), Resl in semi-sitling posilion
O SUBMENTAL CURVED incision of skin & Deep fascia
O TRACHEOSTOMY if needed
ffiNq)EFINITION:
O Bilaleral diffuse Cellulitis of floor of mo
)RGANISM:O Mixed infection (e.g. SIREPT... moulh
TOUTE OF SPREAD:
O Due to Direcl spread frorn infecledof longue or submandibular sialoade
)LINICAL PICTURE:,?\ ,.t/ar \n^..^-^ J..^-L^r!^ O- h..^--^
DEFINITION:O Nemosis of a nail edge which is embedded in skin
& SC lissue of nail sulcus
ETIOTOGY & PATHOLOGY:
O Sile : BIG TOE
O Etiologg : Faultg nail lrimming, wearing lighl shoes
, Nail abnorrnalities as Hgpercurved nai!)
IREATMENT:CONSERVAIIVE
O Gauze soaked in anli-seplic lo separate Nail {rom Nai! bed
O Correct trimming (square trimming)O Avoid tighl shoes
O Keep fooi clean & drg
OPERATIVE
O DEFINIIIVE IREATEMNI) WEDGE EXCISION
O Excision of Nail with periosleurn
O lf Heavilg infecled ) Left lo hea! bg 2rg inlenlion
EI{TiERGEilCT
Betrore

Definilion
Organism
Acule speci{ic infeclion leading to 4nervous excilalion due lo release of
neuroloxin.
rtalmrF1fr4=Tw\5 hlD0cB[lpf/,M@ Th 17+
. Gram *ve
' An-aeorbic. Spore forming. DRUM STICK aDDearance
Clostridium fetani :
Roule
. Aorganism contenl ) Conlaminalion in {ield & slreels s>\io
. VO2 conlenl) Deep laceraled wounds, lschemic limb, shock, Compadmenlal $
. Lack of proper sierilizalion of cal gul & inslrumenls p\il\ qe aibAl
Secreles Neuro-loxin
Pafhologg:
Fr)I
Acule specific infeclion leading lo spreading ofgangrene wiih excess gas formalion
r)
2)3)
WOUNDS, endogenousPosl-operalive ielanusTelanus Neonalorum
Oroanisrn release EXOT0XIN:. ANTI-CHOLINE ESTR.ASE) fonic
rigidifg of muscles at NMJ. OExcilabilifg of motor neurons
al AHC) Clonic conlraclion. LOCAL) Minimal inflammalorg
reaction.
CI.WELCH ll (Sacgharolqticl,Ct. HI$TOLYTICUM (Proteolulic) :
. Gram *ve
. An-aeorbic
. 9pore forming
. Secreles Aloha-foxin
clP..IP
gYMPTOMSl-21 dags
. General) FAHM (low grade feverexcepl during convulsions)
. Local ) pain, swelling, dislurbanceOf funclion (Convulsions)
S!GNS
. SACHCAROLYTIC GP.)acls on CHO of dead muscles) Gases)Elevale sarcolernma) Cul blood supplg
. PROIEOLYTIC GP.)
GENEML:Slage of lonic conlraclion :
IEG, Risus sardonicus,
Opislhotonus, dgsphagia, dgspnea,
slridorSlage of Clonic conlraclions:
Clonic Spasm on lop of tonicspastic muscles
LOCAL) Red, hol , tender wound
acls on Proleins) Arnmonia) H2S) mix
wiih lron of Hb) IRON SULPHIDE "Blackcolor, Bad odour"
. GENERAL) RBC hemolusis, de(eneralion
Complications
!nvesl'rgalions
l-2 dags. General ) FAHM (slighl fever or even
subnormal femperalure). Local) Pain, BIack swelling wilh offensive
odour, loss of funclion
MORTALIW 45%. Hgperpgrexia , Exhauslion. Asphuxia, ResDiraloru failure & HF. Smears from Wounds) organism
' Organ profile, ABGs. CBC) Leukocglosis. CSF) Normal. SPATULA TESI .. bed-side test
GENERAL:
LOCAL:. Wound crepi+us, Black color, foul
odour (Burnt sweel or Spoiled eggs). Sulures appear afler lension. Loss of sensalion & Ms. conlraclion
Jaundice, MOF
MORTAUW >25%leciihenase is lhe mosl dangerous loxinSevere loxemia, MULTI-ORGAN FAILURE. cT, MRt (THE BEST)
' TLC ) Leucopenia, anernia
' 4Bilirubin. Smear from discharge. Plain x-rag) fissue gases

l) $kin incision2) Open Deep fascia3) Ms. Debridernenl4) Wash with H2O25) lf <8 hrs) Close skin looselg wilhout deep fascia
6) lf >8 hrs, excess necrolic tissue or heavilg
conlarninaled) wound is lefl opened
OFffi
Patienls who ispreviouslg immunized in
the last lO gearsv
Give Boosier dose oflelanus loxoid (o.5 ml lM)
r)2)
lnitial dose (O.5 ML)2 doses given with 4weeks inlerval
r)2)3)
R.esuscilation & Moniloringlsolalion in dark roorn, Nulrition bg NG tubeRESPMTORY PROBLEMS) 02, lracheostomg
? h{qV I 75
eutralizes circulaling loxin
2)
Tetanus toxoidIIG (25O units lM)Cornpleleirnrnunizalion courseanlibiolics
. Conlrol of convulsions bg Valium, barbiturales
. ln severe cases > VENTILATOR.
. Conlrol of Hgperpgrexia bg Cooling
.. lnjected in the proxirnal porlion
. Vaccinalion bg DPT
. 2,4,6 rnonths
. Booslet al 18 muscles
. HRG should be vaccinaledeverg 5 gears

r)2)3)4)5)6)
Skin incisionOpen Deep fasciaMs. DebridernentWash wilh H2O2lf <8 hrs) Close skin looselg without deep fascial+ >B hrs, excess necrolic lissue or heavilgcontarninaled) wound is lefl opened
T
I
T
T
Sterile instrurnenls, sutureslsolationPolgvalent Anti-gas gangrene serurnAntibiotics ... Penicillin G
5)P.q=Tw)5 A.DOCXhIE A,EaW)
r)234
IsolalionResuscilalion & Monitoring!V fluids . BIood lransfusion
))
It's lhe least imporfant step
2) ... lO million lU/dag
?Ahq t 7b
. Massive tgpe)H'Eh amputaiion above all a{fectedrnuscles
. Localized tgpe)excision of muscles, dusling wound withpenicillin powder, drainage of wound

Definition: Non-specific infeclion ihat follow surgerg or Hospital admission
Stah. aureus
MRSA
Sierpt.EnlerococciPseudornonas
xfrq-Tw.t5 ENDocFhlE l.M@l ? Aq I T1
trtr
trtrtrtr
trtrtrtr
trtrtrtrtr
Age
Obesiig
Malnulrilionlnrrnuno-
cornpromizalion
Foreign bodies
lschemiaHemalorna
Unlidg wounds
Poor lech.Long time
CBC) Leucocglosisc&s
trtr
. Wound : red, hol,tender, wilhoozing pus
. LNs : Enlarled,lender, elastic,
mobile
. Pain
. Ewellin8
. Dislurbance Offunction:
@ lnfection < 30 dags aflersurgeru
@ lnvolve skin & SC onlg
@ Purulenl DISCHARGE
@ lsolaled Organism
. Non-lraurnalic wound in Glf, uilnarg, Respiratorg tmci
. Risk o{ SSI <2%
. gurgerg inlo lracls with No significanl spillage, Riskof 8Bt 2-5%
Open aocidenlal wounds , Gross spillage from GIII
I
ffi Perfioraied viscus accompanied bg high
Risk of 38! up lo 4OTo
gV
gg
NO Prophglaciic anlibiolics in clean surgerg
lN CLEAN CONTAMINATED) Aniibioiics are $ven 3O min. before skin incision
& Repeated intra-operative with insertion of FB (e.g. Mesh)
lN DIRTY WOUND) Antibiotics are Curalive
CUMIIVE TREAIMENT OF WOUND INFECTION:
- Drain, anlibiotics, Dailg dreesing

ffi+Twr5 1a{iw*NY
Definilion
.r Organism:
* Predisposing factors )bad hggiene, bad general condition, manual
working, housewives
a a a a a a a a a o a a a a a a a aa a a aa a a a aa
PDF, Roule
Route of infeclions
. SWELLING: according to sile..- Ederna al dorsurn.of hand- Pulp space )distal phalgnx- Acule parongchia )Nail fold
. DI$TURBANCE OF FUNCTION:
Corn
* General )Bacterernia , septicemia , Pgemia , Toxemia* Local : Accordin{ to tupe of infection :
' SWELLINGS:
- Hol, red ,fender
**
/ Pulp space infeclion )Thrombos:s, Osteomgelilis
lftf
BEFORE SUPPURATION.F Oeneral ) Resl, analgesics,
anlipgedtcis, antibiotics , HotFornenlalion
* tocal )a) Posilion of reslb) Position of exercise if sliffness
I
/ Acule parongchia )Subungual abscess
. LNS:
Enlarged, elaslic, tender, Mobile
FB is suspecled )X-ragrecurrent )Blood sullar for DM
AFTER SUPPURATIONlncision and drainage
l) General aneslhesia
2l Bloodless fieldgl lncision al site of seleclion
(never cross skin crease,
avoid rnidline incision in
4)5)6)
digirs)
Rernove pus
NO DRAllllg) TullgrassDrg dressing changed afterlsl dag, lhen every 2 dags

xMq-Twr5 E lDocFhttr lJkhw ?^qv 1 fi
DEFINIIION:lnfeclion of lissues surrounding Nail bed
EIIOTOGY:. Organisrn
' PDFBaclerial
Bad lrimming of Nail
Thorn driven under nail
>rd\.! J\ 6Nt
Fungal
Hands frequentlg emerged in water
,!otl\ z\l tl>u\
ClP:
' Sgrnploms
, Signs
General) FAHM
local) Swelling of Nail fold
Genera!) Hectic fever, tach cardia
Local) ... Cgstic
, uellow & U-shaped
ItchingNai! becomes Whitish
coMPUCATTONS
IITIVESIIGAII0NS Cullure on Sabouraud's agar
TREATMENT: As Scheme *....rNCrSroN :
tr Oblique at lhe anlle of nail Oulerfold, excision of lhe % of nail
is all around
shaped from ihe cenler of lhe freeedge)
tr Drgness of hand
tr Topical antifungallf failed :tr Nail fold is laid open & Nail
Exlraction
rI
DEFINTTION: lnfeclion of space belween subungual epithelium &lheir periosteurn
ETIOLOGY: Prick benealh Nail
CLINICAL PICTURE:
- Severe pain, Litlle swelling
- Maximurn Tenderness) Benealh free edge of Nail
IR.EATMENT: Rernoval of small "V" From center of fiee edge of Nail

cilR+-TCrIr5 END0CRNtr ffihW
Conlentsl) Fat
2) Fibrous septae )
3) Food: D'rgifd arlerg) Thrornbosis) Osleorrgelitisof ienminal phalgnx exeepl ils epiphgsis
@ lncideRce;
@ Etiologg )Prick@ CLINICAL PICTURE: as scherne * ....
PA6h | &
@ Cornplicalions )Osleomgelitis of lerminal phalgnx excepl its epiphgsis
Treatrnenl: As scherne * ....- Anterolateral ineision on lateral side of dislal 43 ot
distal phatgnx Or al point of maximurn lenderness- For severe cases )Counier ineision
1.1 "*
- For sequeslreclorng )
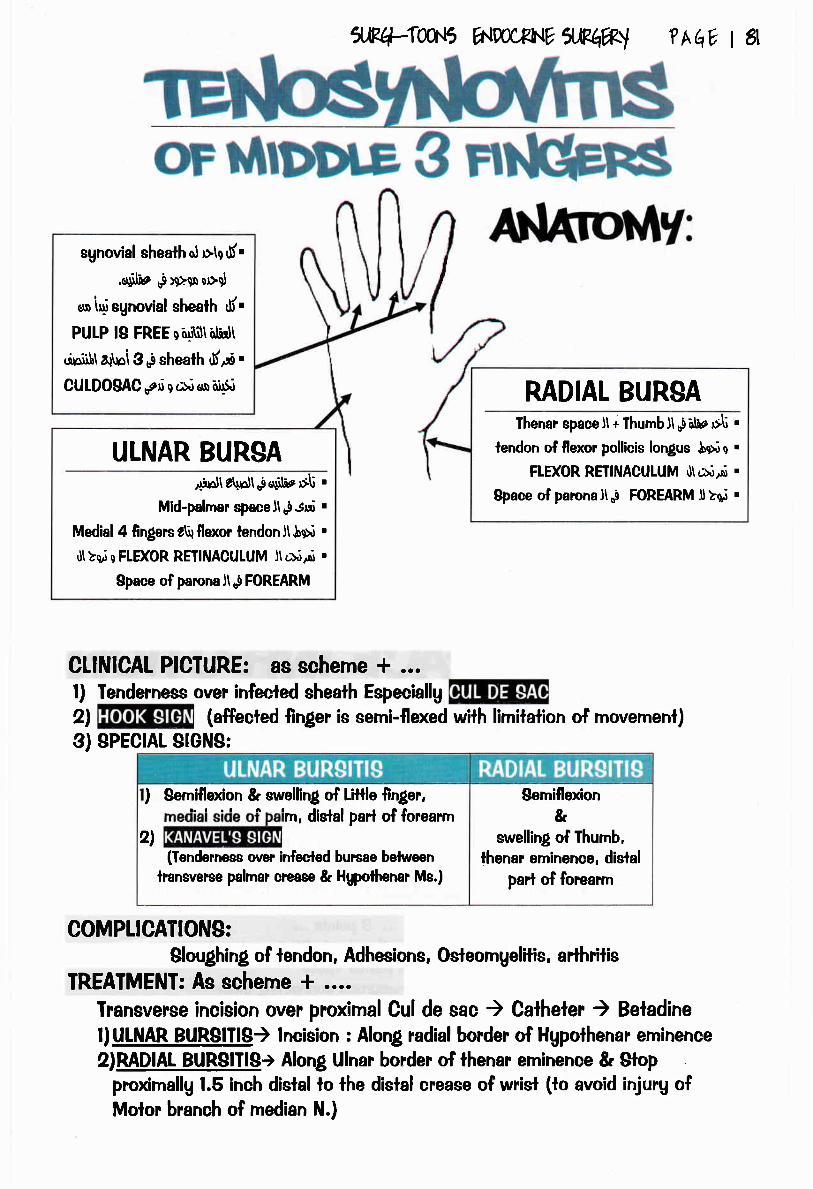
w+tw'J5 a{DocFI{E 1.8@l ?AqY I a
CLINICAL PICIURE: as scherre * ...l) Tenderness over infecled sheath Especiallg
2l (affecled finger is semi-flexed with limitalion of movemenl)3) SPECTAL STGNS:
COMPLICATIONS:$loughing of lendon, Adhesions, Osteomgelilis, arthrilis
TREAIMENI: As schenre + ....fransverse incision over proxirna! Cul de sac ) Catheter ) Betadinel) UTNAR BURSITIS) lncision : Along radial border of Hgpolhenar eminence
2)RADlAt BUR8ITIS> Along Ulnar border of thenar erninence & Slopproximallu 1.5 inch distal to the dislal eease of wrisl (to avoid injurg ofMolor branch of median N.)
sgnovial sheath ol >le 6i.
..uilie ,i>9>e!or>d
on l4i sgnovial shealh rf.PUIP l8 FREE q6,gS\iili'Jt
.lniib\ a\oi3 op shealh drrO "
CULDO$AC trri s t>i en a,ip
ULNAR BURSAAidlr\lnll oldihe$t .
Mid-palmar spacell re Jui .
Medial 4 lingers g\lllexor tendonjlSur .
tjtluj c FLEXOR REIIIIIACULUM Jt *llsr .
Space of parcnaJtop FOREARM
MDIAL BURSAIhenar spaceJl + IhumbJl0iilhe $li .
lendon of flexor pollicis lonlus 5N c .
FID(OR REIINACUTUM d\oiA .
Space of parona n o! FOREARM I >q,i .
) srTil.T?, q swelling of Little finler,'rn, dislal parl of forearrnrn, digtal paH ot rcreari
2)(fenderness over infecled burcae belween
lransverse palmar crease & Hgpottnnar Me.)
Semiflexion&
swelling of fhumb,lhenar eminence, distal
parl of forearrn
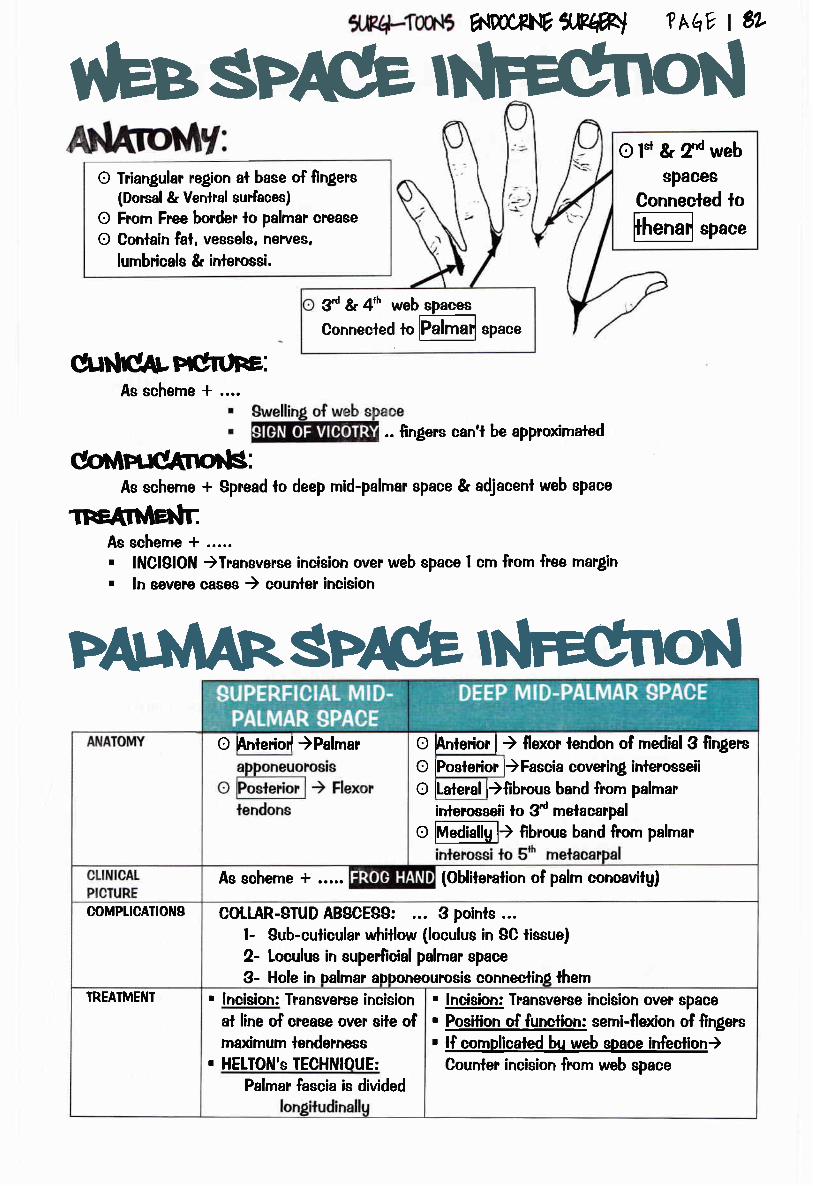
htO friangular region al base of lingers
(Dorsal & Venlra! surfaces)
O From Free border lo palmar crease
O Contain fal, vessels, neles,lumbricals & irrlerossi.
hlDoc8hlE x*#l
c[r$CArWrtrFE:As scheme + ....
@rinrdtnorts:As scherne + Spread to deep mid-palmar sPace & adjacent web space
ffiAs scheme + ...... lNClglON )Transverse incision over web space I crn from free mar$n. ln severe oases ) courrler incision
3'd & 4h web spaceg
Connecled ro Elmai space
?hEV I 6L
s#l
o t*t & ?d websPaces
Connecled lo
@space
.. {ingers can't be approximaled
O Anlerior{ )Palmar
coMPUCAilONg
TREATMENI
As scheme + ..... (Obliteration of palm concavitg)
COIIAR-STUD ABSCES9: 3 points ...l- 8ub-culicular whitlow (loculue in SC tissue)2- Leulus in superficial palmar space
O hnterior | ) {lexor lendon of medial 3 {ingers
O lPosleilor l)Fascia coverin! inlerosseii
O lLateral l){ibrous band from palmar
. lncision: Transverse incision
at line of oease ovel site ofrnaximurn tenderness
. HELTON's TECHNIOUE:
3- Hole in oalmar aDDoneourosis conneclino lhem
irrlercsseii to 3d melacarpal
o MAla[gl) {ibrous band fiom palmar
Palmar fascia is divided
. !4p!q; Transverse incision over space
. Posilion of funcfion: semi-flexion of {ingers
. lf complicaled bV web space infeclion)Counter incision from web space

lJP.q-TW-t5 ^DoCR[{V
X,WW ?hqv t 81
l. ldea! anlibiotic surgica! prophglaxis should start before skin incision and
conlinue for one dag after surgeru.
2. lndiscrirninale use of antirnicrobials can lead to the developmenl of antibiolicresislant microorganisms.
3. The rnosl important cause of posl-operaiive wound infection is presence ofdead space.
4. Fournier's lanlrene is caused bg bacteroids, califorms & peptoslreplococci,bul nol clostridia.
5. Bacteroids a?e a parl of norrnal flora of oropharunx, colon & vagina, bul nolurinarg fracl.
6. The main organisrn of endotoxin release in multiple organ dgsfunction is E.coli.7. The mosl cornrnon anaerobe in Colon is B. FRAGILIS
8. The rnost frequent cause of Endotoxic shock is E.Coli.
9. The mosl frequenl organ:sm associated with neck abscess in children is $laph.Aureus.
lo.Adequate wound debridemeni is the most imporlant measure in management
of coniaminated wounds.
ll. Cenlral venous pressure {CVP} rnag be decreased bg Grarn-negalive sepsis.
12.CLOSTRIDIUM TEIANI: has a drum stick appearance, is slrict anaerobe, and
Produces h'rghlg resislanl spores.l3.A palient who has recovered from lelanus requires a dose of loxoidl4.Gas gangrene infection is caused bg anaerobic spore-bearing closlridia, has a
veru shorl incubalion period, Cornmon lo occur in deep wounds of lhe thigh,
but nol associaled with high fever.ls.Trealment for clostridial mgonecrosis (gas gangrene) includes Adminislration of
Anlitoxin, Wide debridemenl, and Adrninislralion of hgperbaric oxggen
l6.The rnosl lelhal loxin of Cl. Welchii is LECITHINA$E (cr - loxin).17. Fool infection in diabeiic palients is predominanllg caused bg rnixed
organisms.ls.Midpalrnar spcace infection is mosl oflen due lo direct spread from inlrathecal
whillows.l9.Ihe hand infeclion which carries the highest risk of osteorngelitis is distal pulp
space infection (felon).
l. Patient complaining of lender, duskg red hol, non suPPurative area withinduraled ill-defined edge al medial aspecl of lhe leg. lnguinal LN are enlarged,
elaslic, lender, mobile.
Gelhlrtb,2. Pallent oomplaining of tender, duskg red hot, non suPPuralive area wilh
indurated well delined edge al lhe face, slighflg raised
En1srplas,3. Old patienl complains of suffooalion, severe dgspha$a, and severe dgspnea.
On examinaiion edema of the floor of lhe rnoulh, lhe longue is pushed upward
and bach,uards.
l@fi| I dtqttta4. Manual worker presenls with $a,elling in nail bed. Dull aohing pain. On
examination nail bed is induraled gellowish cgslic.
1fr+Tw'{f_ A.WCPhltr lRI#l ?hqY t e+
5. Youn! male cornplaining of neuosis of the big nail sulcus with persislenl
irrilalion of his nail.
6. Patient farmer preienls wilh conwlsion. fhe relalives $ve hislory lo severe
headache 12 hour ago. On examinalion the patient has a swollen wound and
severe pain al sile of wound.
Tetarus.7. Palienl presents with deep laceraled crush wound, lhe wound is black &
edematous with foul odour and waterg diecharge.
fias gdillroile,
hgnyyt tu- tarl @tyclrun1fiu H,
,futepnilFlk

ilPq-Twr5 ww/PNYlMW lffi
of
Discuss Aetiopathologu , ClP and TTT of acute
Puogenic abseess
r Gas gangrene
r ClP and TIT of Tetanusb4th sllafils, 2d/ )
O+i/ sfiafils,2MI Factors affecting wound healing, cornplicalions of
wound healing( r4lur)/,2M -r4ltarf,2M,2@5 -
Kasn 2@7 - Kasn 2d/ )Genera! principles in rnanagernent of hand infection
( ,4y'rar f, 2@Z 2@4 - ,4y'rar ,il, ZooA)Tenosgnovilis of lhe finlfers of the hand
G4i/ sfiafils,2M )Managernenl Pulp space infection
( Kasr ' 2@7)
Delection of wound sepsis afler surgerg and ilsrnanalfernent
( Kasn 2@n
( Kasn 2d/ )
( ,4r'tar f,2M- Arfl sfiams,zfu )
r Short account on : ergsipelas

"(g I NY I |..Aqil6 alrd?ftlM grwY?ttrE

"v-
tUbhaelAAF tth .. Altr snrversrttt

xfr+rw*1 6m,rhu xfr#ll ?hEv t *
r Polg-fraurna lized patienlr Acute woundsr Wound Healingt Hernorrhagic shockr llernomhage

resffioF .
INCIDENCE:)r Mosl cornrnon cause of death among middle aged paiients)1 3'd Mosf cornrnon cause of death among al! groups
Will die anuwauwhether theg
received medica!altention or nol
TRlr.iODAt DlsrRlBonohl . . . re OF DEJtr+t
lf resources are Iimited ) YELTOW CODES arc lrealed {irsl
Will suruive ONLY lF thegreceived timelg medicalal-lenlion in the GOLDEN
HOUR, "{irst hour"
5R4-Twr5 dwUWlJRhW
Within rninutesDue to injurg to vital
slructures
WILL survive angwagwhelher theg received
medical altention or not
Due lo hemorrhage,
i ,ii I 81
or maior fraclures
L{
-H

@
@
@
@
@
@
A: Airwag patencg & support mandible
B: Adequale breathing (look, feel, listen)C: Circulation ) Gonfrol ang bleeding
D: Drugs "Analgesics"Cover wound wilh slerile dressingAvoid flexion of spine lo avoid dislocalions
OF
M ls patienl able lo speak or not?EI Is airwag patent or nol ?
flJR+-Tour5 ENDo(xhlE ilPqW
!nspeclion - Palpation -Ausculialion
@
@
@
@
@
PffiEf.tr
gHOCK(Hemorrhagic. cardiogenic, Neurogenic)
A: Airwag
fr Breathing
Q Circulalion
D: disabilitg
f, Exposure
T[{EN.. DEFINffi\'Effi&Resuscilaiion & moniloring ...
AVPU evaluation(Alert, voca!, Painful slimulalion , Unresponsive)
gsbg
aitwag ,
HFJTDToTOE e><A.,ilNIFION@
@
@
@
@
@
@
Head
NeckNeurological ...ChestAbdornenDRE
Limbs
?hq? | 10
adg
Foleg's I
NG tubeRadiolor
@
@
@
@
@
CalhelerI
tical assessrnenl
AllergiesMedicationsPast Medical HistorgLast MealEvent of injurg
$fiPleslsron#
OFGFitrlffiAFrB,@
@
@
LAB : HB%o, Glucose, KFT, ABGs , PO2,PCOZRADIOLOGICAL : X-rag ,CT ,MRl .U/g , DuplexINSIRUMENTAL : Endoscopg, Centesis
EAslcuFE gJ'PFo'Fr

S fu Ug'=F.lr aii+{
Exlension to painful stirnulusus$hll drrSc
De-cerebraled
U g r-.llol'rll g r-llg,,iu U+rirql
W "GCS,,,
EBB Pl{AgE l<24 hours))r OEnzgrnalic activilg & OZ consurnplionE Lactic acidosis
CATABOLIC Pl{AgE (g-to dage)11 Fat, Prclein rnobilization11 4Urinary Nilrogen excretion
AilABOtlC PHA8E (tO-eO dags)tr Resloralion of Fal & prolein slores
Merarcud
'-l :r^
ilR4-Toqr5 a{DocRNr rlxt wt
Flexion lo painful stimulussr$bll rr{Sr
De-corlicaled
REsttrohlsE
Flexion *Withdrawal
srt+ll
plgl +Iiii 9 r.lLip
?nqe t 7
al
Orienfed, Norrnal
arra,,-
Localize painfulslirnulus
ffil\IEOSecreliontr Aldoslerone) 4Na, HzO
reabsorplionrr CA) V.C., Tachgcardiatr ADH) H2O retention!r GH, Prolacfin, ACTH
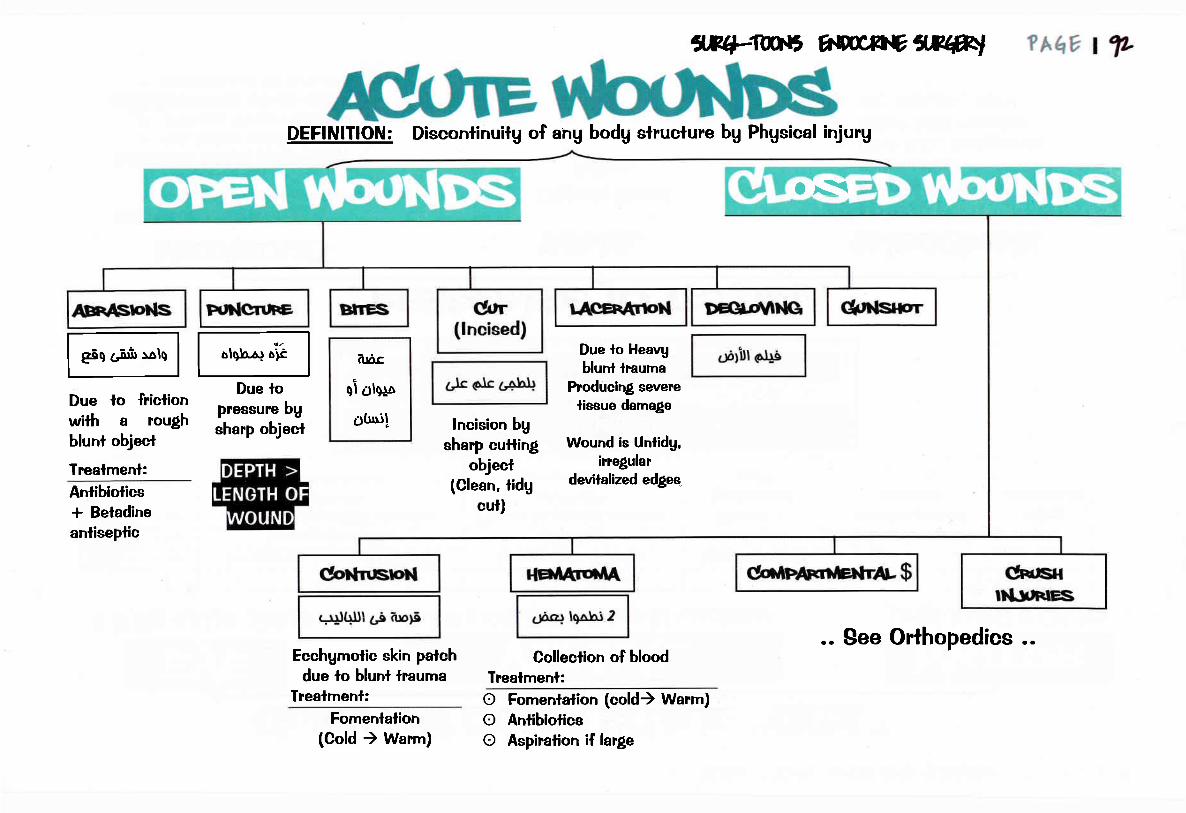
DEFINITION: Discontinuitg of ang bodg structure bg Phgsical injurg
Due lo friclionwith a roughblunt objecl
frealmenl:Antibioticst Betadineanliseplic
Due lopressure bgsharp object
arac
qi olerp
oUui!
AB+TUD{r, E\m,fbEAE#t
lncision bgsharp cufling
object(Clean, tidg
cut)
Due lo Heavgblunl lrauma
Producing sevene
lissue damage
Wound is Untidg,irregular
devilalized edges_
Ecchgmotic skin patchdue lo btunt lrauma
Trealrnenl:
os(
Fomentalion(Cold ) Warm)
Collection of bloodfreatmenl:ooo
Fomenlalion (cold) Warm)AntibioticsAspiralion if large
.. See Orthopedics ..

HgpovolemicSeptic
Neurogenic
ENBAT
@ SPECTFTC(TB, gas gangrene)
@ NON-gPEC!F|C(Seplicemia)
@
oFnlooxp
Crush injurgCompartmenlal $
lnvesligations :lr Hgperkalemia* CK > IOOO U/L* Mgo$obinuria
Complicalions :
Acule renal failureTrealrnenl :
B Resuscitation & Anti-shock rneasures
n Alkalinization of urine. Fluid
ci,Rl4*TC0r5 ftlgpc*tlE ilRqWJ
@
@
Staph.Strept.
Pseudornonas
. Diuretics (lV mannitol)
. Vilamin Kfr Fasciotomg
?AqY I T
TelanusGas-gangrene
@lipucAnoNsOF HEJUTNC
O ContractureO Chronic ulcerO KeloidO DisfigurementO Lgmphederna
Management of Polglraum alized palient..(see before)..
Management of Wounds..(see Vascular surgerg)..

@
@
PRIMARY SURVEY ... ABCDE ...SECONDARY SURVEY& Examination from head lo toe* Resuscilalion* lnvesligationst MoniloringSYSTEMIC THERAPY@
cilP+:fmr5 ENDOCFNV 1JPqW
@ IRRIGATION WITH SALINE
@ DEBRIDMENT* Skin )Excision ol l-2 mm of edges* Fascia )Fasciotomg* Muscles )Excision of dead muscles* Bones ) Deconlaminalion bg cureltage* Nerve )Mark wilh black silk lhen delaged repair* Blood vessels ) (nT=!oni,.,,,,'u,Ir) Ligalion or rr* Skin closure ) Accordino {o slalc of worrnd
3J+JItito0lb
?hq, I T
* Blood vessels ) (nT=!oni,.,,,,'u,Ir) Ligalion or repairSkin closure ) According to slale of wound
Closure withoulTension
@ IMMOBILIZATION & POST.OPEMTIVE CARE* Observafion* Antibiotics* Anti-letanic serurn* Anti-Gas gangrene serum
Delaged closureor gra$]ing

@ tidg wounds, slrong scarc@ Seals l-2 dags@ Heals l-2 weeks@ Full power 3-6 Ms
SECONDARY INTENTION: <lpral! r-r h@ Unlidg wound with gapping edges@ Weak scar@ Takes much rnore lirne
TERIIARY INTENTION:.l.rLiGil Ufyfg Lir.#ai iir'i6 3i-i{
Wound is lefl open for 5 dags then requires adelaged prirnarg sulure after being clean.
fuxp NG,NfENTION: EsririrroJl r'S
DEFINITION:
FACronS AFrECTING HEATI}G'
Mechanisrn bg which bodg reslores integritg of injured part
@ TUp" of wound (Tidg. untidg)@ Site of wound
(Wounds over flexures )lension)@FB@ Vascularinsufficiencg
fl/F4-ToohlS g{rucxlNE lJ?qw
t{EAtlNqSrAH: x4INFLAMMATORYVascular responseCellular response :
Following bg Neulrophils, Masl cellstAG PHASE (3rd -Sth)
Endothelium, Collagen , MPs
PROLIFEMTIVE PHASE (sth -2lst )Epithelial regeneralionGranulalion lissue forrnalion (healthg, unhealthg)Conneclive lissue repairWound Conlraclion
REMODELING PHASE (> Igear)TUp" lll Collagen )Tgpe I
PHASE (lsf 4 dags)(hemoslasis * Vasodilatation)
@
@
@
@
@
@
Age of patientObesitgMedical condilionsMalnulrilionMedicalionsSmoking
?hh6 115
@rtlpucArloNs oF r{EArrNG,
WoundConlraction
tigfr ii+trWound
Conlraclureii rfr rg ii?Lt
lnfeclion,hernalornaDehiscence
iijglUuLtll 1,i [r,Ul iir..rfil@
@
@
@
ScarsHgperlrophic scarsKeloidsMarjolin ulcer

HE
Phgsiological rnechanisrns
To reslore blood volurne
Fail if blood Loss > 15%
clo:tr Weakness, fainlingtr Palienl feels Cold ,fhirslgOlEz
tr Altered rnenlal slalustr 9BP, Weak lhread pulse, 9PPtr Hgpolhermia
tr Tachgpnea, air hunlertr Skin becomes pale,
tr Capillarg refilling > 2sectr Oliguria )Anuria & Renal failure
Exclude bleeding lendencgCBC, ABG, Electrolgfes, PH,
KFT. LFI
wp.q-rw$ 1aJlw*Nexww ?hqY t fu
State of peripheral circulalorg failure due to sudden bloodloss or shift from peripheral circulalion.
V Blood volurne due lo :fl Whole blood lossg Plasma lossg Waler & elecirolgte loss
g Delerioralion offunclions ofbrain, kidneg,
Hearl, lung
(lf Treatment fails)
Exlernal Hge
lnlernal Hge
Burnslntestina!
obstruclion
A Mu[i-organ failure
Anuria
ARDS
trtr
trtrtrtr
nGrunei,
OF COMPLICAIIONS
COMPTICATIONSORGAN PR.OFILE DETECT THE CAUSEf prJl lJt+3
tr Abdorninal US
tr Head CT scan

E ABCDtr Airwag )patenttr Breathing )Mainlainedtr Circulalion)Slop bleeding
tr Drugs )Morphine lo relieve neurogenic shock
tr 3 ANII - : Anlibiotics, Anli-Gas gangrene, Anli-Telanic serurn
E FIRST AlD
1Tr. OF
FLUID REPLACEMENT:tr Slart with Crqstalloids
Until blood lgping, cnoss rnatching are done
t) Norrnal saline
tr Elevalion of tegs ..
trtr
lmmobilizalion of fracluresWarming
3) Ringer laclate (+ Buffer)
N.B. :O Crgstalloids mag be given alone )Pf. with
Hgpovolemia due lo waler & Electrolgte imbalance
O # Glucose 5% )leads lo dilutiona! hgponalremia
tr Colloids:
l) Plasma subsilitues
2) Dextran
tr Blood ) in hemorrhagc Shock if HCI <gO 7"
2) Ringer
ilE+TW A{poCXt\tE ilR(#l
(+K*t
ew
MONITORINGtr Viial data
ArHcFrrAt(td{r)
E STOP HEMORRHAGE
E RESUSCITATION:tro/2tr RYIE )evacuale slornachtr LINE >2 Cannulas for fluid
replacernenl & Samplint
trtrtrtr
"Pulse, BP, Ternp. Respiration"
ABGs , ECG
Urine OulputCenlral venous Pressure
Pulrnonarg arterg wedge pressure
totearlg delection of Lt side HF in
old pafients.
Arlerial Line )Monilor ABP,
essessrnent of ABG
?Aqv t T
SUPPORT
m oF cAusEtr lnjured vessel)surgical repairtr Burns) fluids, wound care
m OF COMPtlCATlOttlgtr DIC) fresh frozen plasrna
SECONDARY SURVFTAfter stabilizafion..

ilRq-Twr5 flW47NY 1'RhW
Accordin! lo tirne of Hernorrhage:
gaV
ggV
Venous blood : dark, profuseArlerial Blood: red, spurling, oscillalingCapillarg Blood: red, oozin!
Bleeding:
Prirnaru Hernorrhage : al sarne lime of operalionReaclionarv Hernorrhaqe: within 24 hoursSecondaru Hernorrhaoe : within 7-14 dags ... main cause is infeclion
frealrnentl. $loD hemorrhaoe: (posilion - pressure - packia$ e.g.
- Elevalion of the limb above the heart level , Balloon larnponade
[email protected]. Optimize oru{en deliveru: 4O% oxggen is $ven for class ll and IOO% for classes Ill and lV.
4. General care of lhe patienl: absolule bed rest and analgesia(Morphine is contraindicated in head injurg and in oases of respiralorg and liver insufliciencg)
5. @gI!Dg:- Urine output, core lernperalure, hernalocril and cardiac moniioring- ECG for earlg deleclion of shock-induced arrhgthmias is important).
- ln class lll or lV hemorrhage ) as above + CVP, ABGs and PH
?hqv t r
't'-ht
Normal Sgstolic BP
ODiaslolic BP
Capillary re{ill
Replacemenl bg
Ringer laclale 3 timesdelicit
M Hernalocril SO %g urine oulpul SOm7hourg CVP rises lo lhe upper /z of norrnal range
lf CVP is risin! & Patient is NOT imprcvin! (Shock + zfCVP)
) search for:a) fension pneumolhorax
b) Cardiac larnponadec) Heart failure

ilRq-Twr5 nDgcRNV il?4ry Thh'* I fl
"MOST SERIOUS WPE OF SHOCK',,,MOST
DIFFICULT WPE TO BE IREATED"
ETIOLOGY:Etr Or(anism: MOST COMMON ORGANI$M lS GRAM -VE BACILLI
E Source of infecfion: Perilonilis, Cholangitis, UTI
E Predisposin{ faclors: Exlrernes of Age, DM, Irnrnune-comprornisalion, Malnulrilion
CLINICAL PICTURE ... 2PHASES ...
$FS(sYsTEMrC r NFLAMMATORY
RESPONSE SYNDROME)Etiologg:
a ffir@g Polg-lraumalized patienlg Major burng Acule pancrealitisg Neglected hgpovolemia
CRITERIA FOR DIAGNOSIS:
a) Iemp >38c , <36cb) HR >90 bpm
c) RR >20 breath/mindl WBCs >12000 , <4000 lmmS
INVESTIGATIONS:tr FOR GENER.AL CONDIIION:
tr CBC: 0TLC, V Platelets
tr ABG, Electrolgles, Blood sugar
tr FOR EIIOLOGY: lsolalion of organisrn, C&S, Localizalion of seplic focus
tr FOR COMPLICATIONS: KFT, LFT, ECG, Coagulalion profile
. Reslless & confusion
. gKlN) Flushed, warrn, drg
. VITAL DATA:
x Fever >38tr Tachgcardia
tr Tachgpnea.
^COP
. SKIN) Cold, Clammg
. VITAL DATA:
tr Oliguria
tr Sgstolic BP<90 mmHg
tr lachgcardia11 Tachgpnea. vcoP
g Evidence of infeclion ... *ve Blood cullureg Refraciorg Hgpolension
+ Ang 2 wltefia of the following ...V Hgpervenlilation (RR,>20 breaths/min)V ABG (PCO? <32 mmHg)
A WBCs <4000- >12,000 cd!s/mm3
80% MORTATITYg MOFg Dtc

ilRI4-T1a.t5 ,NDocE[.], ilRhw
TREATIVIENT.. ADMISSION TO ICU THEN ...
? hhv I r00
RESUSCITATION
CIRCULATORY SUPPORItr FTUID REPLACEMENT:
RINGER LACIATE
tr DRUoS
(if Patient rernains HYPOTEN$IVE
despite {luid replacernenl)
Dopamine, Dobularnine
REPIRATORY SUPPORT
tr O2 bg mask
tr lf PO2 < 60 mmHg
) Mechanical venlilalion
RENAL SUPPORT
ERAD!CATION
OF INFECTION
tr Eradicalion of sepsis
E Parenieral anlibiotics
MONITORING
tr Vital silnsE Urine output
E ABGs, CBC,
Coagulation profile
tr CVP, Arlerial line
tr Prophglaxis against
DW, slress Ulcers
Hemodialgsis in ARF
DIC? Fres.h frozen plasma
ffiffioFCmuoqpt{CstlodKg MOSI COMMON CAUSE Ig MYOCARDIAT
INFARCTION
CtINtCAt PICIURE:
CONGESTED NECK VEINS + ACVP
TR,EATMENT:g TTT oflhe cause
A Dobulamine (inolropic agent)
ffileSHocKEflOTOGY:
. High spinal aneslhesia,, Transaciion of spinal
cord
CLINICAL PICTURE:
. BMDYCAR,DIA
. WARM SKIN
. LOW BP
PROGNOSIS: 80% MORTALITY
EI Most imporlanl lrealmenl ofAnaphglactic shock is lV
hgdrocorlisone
M Mosl importanl causes ofEndocrinal shock : DKA, Addison,
Mgxedema
M Ang prolonged hgpovolemic shock
)seplic shock
EI Ang prolonged hgpovolemic shock
in elderlg )cardiogenic shock

?hqv I ureg suruive in slored btood from llfi
Blood group mismalching can be accepled in LIVER lransplanlation
Donor & recipienl are onlg malched for ABO compalibilitgAll componenls for slored whole lend lo Vovertime excepl Polassiurn
Donaled blood should be roulinelg screened for Hepatitis B, C, HIV
CMV is screened :n high risk groups (Ex: lC palienls)
Best guide for blood transfusion in hernorrhagic shock is " CVP "
aagg
FEERITEa
a
TTT : stop lransfusion, Anfi-hislaminic, Hgdrocorlisonetrtr
trtr
trtr
trtr
AII^BCICREACTIoN.C/P: urticarial palches up lo Iargngeal edema.
TII; Anlihislaminics & corlisone, slop the lransfusion.
HEitolr/rlcREAcrloN:tr ETIOLOGY: lncornpalible blood transfusion
tf patient is under anesthesia or comatosedlncompalibilitg is suspecled bg:. Bleeding tendencg (oozing of blood). Progressive uneplained hgpolension, fachgcardia.
tr TREATMENT:. Slop lhe transfusion irnmediatelg.. lV fluid(ringer laclale* corticosleroid).. Alkalinizalion of urine bg NaHCoS. Mannilol20% l0O ml (forced alkaline diuresis).. Repeal palienl's blood lgping & matching.
Noll+MComplication of maseive blood lransfusion
. Acidosis, Hgperkalemia, Circulatorg overload,
Hgpothermia, Cilrale toxicilg, Bleeding lendencg
Z-Ait embolism.
3-Thrombophlebitis at the site of injeclion.4-Complicafion of lranefusion of stored blood
Acidosis, Hgperkalernia, f O2 affiniig
1JP4-Tw.t5 1a{lw*Nv lJRhRl
Transfusion of 2500m1 of blood
al one lirne or 5000 ml or more
over 24 hours
fficArDelaged hemolgsis
Post-lransfusion purpura
a-lron ovedoad (Hemosidrosis).b-fransmission of diseases as:. AlDg.. Brucelloeis.. CMV (Ihe MOBI C0MMOttl). Malaria(onlg bg RBCs). Viral hepatitis.. Sgphilis.
tr CLINICAL PICIURE:
. Fever & rigors.
. Hgpolension, Tachgcardia.
. Cganosis.
. Ol[luria.
. Renal failure.
Fever & r'lgors
Chesl, lurnbar pain.
Dgspnea.Headache.
trWHOtE BLOOD: Hernorrhage,
operalive replacernenl, severeburns
trPACKED RBCs: severe anernia
trPI.AIELETS:
I'u or 2's lhrombocglopenia,platelet dgsfunction
trFRESH FROZEN PLASMA:
burns, rnalnulrilion,coagulopathies
trCRYOPR,ECIPITATE:
hemophilia, DlC, Wt/D
TFIBRINOGEN: DIC
trLEUCOCYTES: Severeleucopenia, Agranulocgtosis

lJRq-Taq'$ E{Docxhly XMR'I ? hqv I WL
r Hernoslasisr Bleedinlf disordersr Bodg Walerr Sodiurn, Potassiurn, Calciurnr Acid base balancer Nutrition (Enieral, TPN)r Posl-operative cornplicalions

Cornrnon pathwag:V Faelor l, 2,5,10, l3g Assessed bg PT, PTT
Exlrinsic pathwag:g Faclor 7g Assessed bg PT
V Affects Oral anfi-coagulanlsV Prolonged in Liver disease,
Vilamin K malabsorplion(obslruclive jaundice)
tnlrinsic palhwag:g 8,9,11,12g Assessed bg PTIg Affecls Heparin
tr Half-life of factor I is 8 hourstr Mosl cornrnon cause of defeclive
hemostasis is fhrombocglopenia
cilRt4-Iwr5 A{D0CEI{E IJP^W ?AqE t w
EI Vilamin K is essential for aclivation ofFactor 2 ,7 ,g ,lO
Iheg are prolonged in Liver disease, Vitamin Krnal-absorption (obslructive jaundice)
M Cournadin effect can be reversed bg Vitamin (M Anti-thrornbin 3, Pr.otein C, S, Faclor 5 leiden
have anli-coagulanf effecl(Measured in a recurreni DW in a goun! patienl)
lnlrinsic pathwagogq ++lJl
CLOTTING CASCADE:O INTRINSIC PAIHWAY
O EXTRINSIC PAIHWAY
viltxxtxil
INTR!NgIC
PATHWAY \.^'
v
lt
!
vil
EXTRINgIC
PAIHWAY
(Prothrombin)
(Fibrinogen)
xlll
Wthin fewminules
Within fewseconds
ooooo
O 4BT (platelels) , 4PTT
Long aclingacls on factor Xa
Given once dailg
Eliminated via kidnegs
Causes no bleeding lendencg:NORMAL PTT(better in
Reduce lhe concenlrationVitamin K dependent cloftingfaclorsHalf-life : 36 hoursCrosses lhe placenta (Should be
avoided in pregnancg)
Doses should be reduced in Liver
disease
Controlled bg lNR, (aboul 2-3iirnes double the norrnal value)

gdga
Vgg
V
lRq,'IWr5 A\$gCRtl, flRqW ?AqY I w+
Deficiencg of faclor 13) A , Faclor 9) B
Sex linked
Bleeding during circurncisionPosl-lraurnatic bleeding (e.g. Hemo-arlhrosis)INVE$TIGATIONS: value of faclor = 5-2OTo Normal value
TREATMENT: lnfusion of deficient facfors, FFP, Crgoprecipitate!M lnjeclions ::
De{iciencg of Factor I , Aulosomal dominanlCLINICAL PICTURE: Echgmosis, Purpura, Bleeding from orificesINVESTIGATIONS: ABT, 4PT, APTT, De{iciencg of factor 8TREATMENT: lnfusion of Deficient VW factor
Mosl cornmon cause : SEPTICEMIA
CtlNlCAt PICTURE: PARADOX.. Thrombosis Bul bleeding rnag occurINVE8IIOATIONS:- VPlatelels, 4PT,PTT, VFibilnogen, 4FDPsIREAIMENT: TREAIMENT OF UNDERLYING CAU8E, FFP, ugoprecipitate
NG,Dgggggg
REJECIIONChronic reieclion is the
[[[
lRq-TwV 1a{lwC*NY,',RqAl
Total bodg waler = of Bodg weight We1
?hqv I w
rcF (As)40% of adultbodg weight
EcF lt/3)20% of adultbodg weight
. lnsensible water loss (t2Oornl)- 8oOml)perspiration lhrough skin- 4o0ml) Expiration through lungs
. Urine (l600rnl), 0lT (2Oornl)
lnterslitial fluid lAq Intravasoular fluid (t/g)lO% of adull bodg weight 5% ol adult bodg weight
Waler balanoe is maintained bg adjusting waler intake & waler loss..
EXOGENOUS
(2500 ml)ENDOGENOUg
(soO ml)
LOgS
M Osmolaritg of BLOOD depends on PROTEIN
M Osmolaritg of ECF depends on Na, Cl, HCO3EI Osmolarilg of ICF depends on K, Organic phosphorus
.BODY O$MOIARIW = 300 mosrno7Kg ..(Double Na leve!)
'ADH is conlrolled bg Plasma osmolarilg , ALDOSTERONE is
Conlrolled bU Na*, K+, Renin
. VTNTAKE:
- V availabilitg- Difficullg to swallow
. AOUTPUT:Fever, Osmolic diuresis
. AINTAKE:- Pre-operafive waler enema. TURP $
- Posl-operalive over infusion of Glucose 57" lV- Neurosis
rlprallEpJiirfhirsl, weakness, OliguriaHgpoiension, Tachgcardia
MODEMTE: 4udne volume, OBodg weightMARKED: Brain edema, Nausea, vomiling
TREAIMENI R.eplace bg Na free waler .MILD TOXCITY: V waler inlake.BEM!IA!!!!BE Dialgsis.EBA!UEDE@, Mannilol, Cortisol,Hgpertonic saline (lf lhere're CNS
manifeslations)
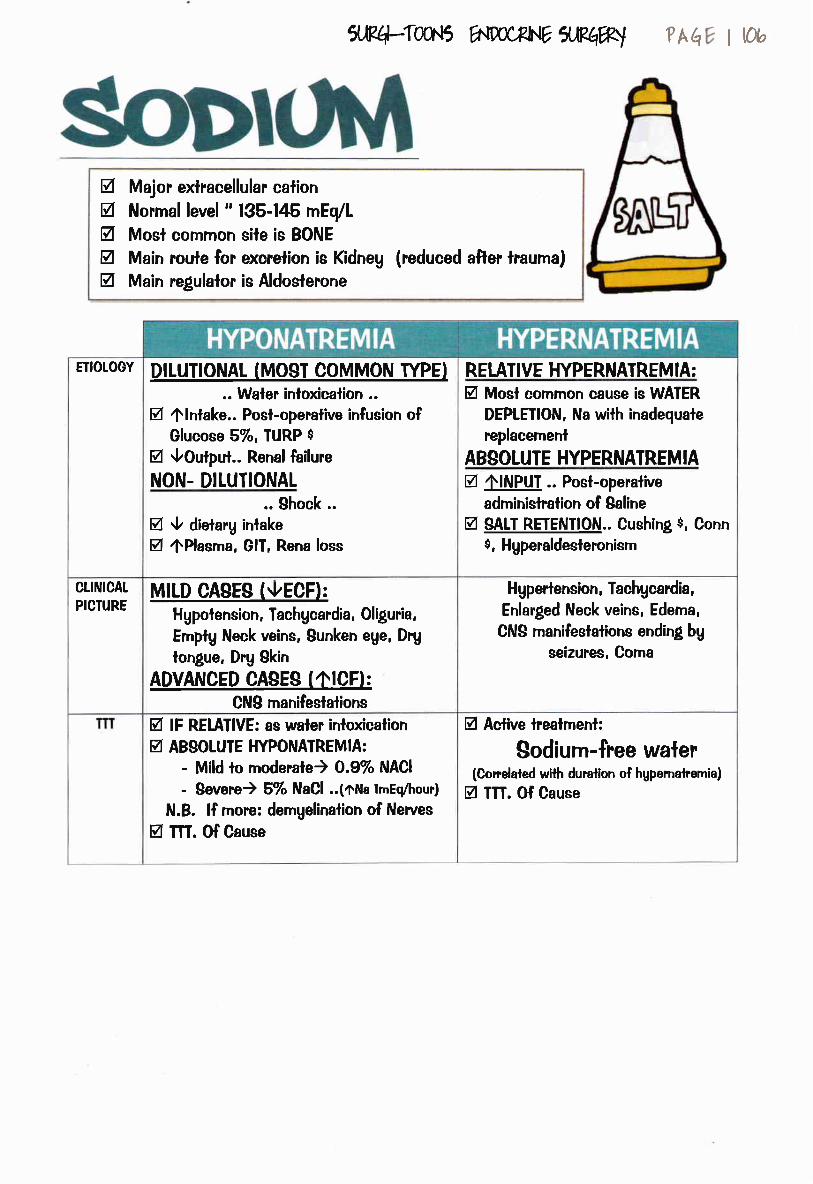
crffi4-Twfi ww*wflMw ?Aq I ttu
gVgVa
Major exlracellular calionNormal leve! " 135-145 mEq/L
Mosl comrnon sile is BONE
Main route for excrelion is Kidneg
Main regulalor is Aldoslerone(reduced after lrauma)
ETIOTOGY DITUTIONAT (MOST COMMON TYPEI.. Waler inloxicalion ..
EI 4lntake.. Post-operative infusion ofGlucose 5%, IUR.P $
EI VOuQut.. Rena! failure
NON. DILUTIONAL.. Shock ..
EI V dietarg inlakeEI 4Plasma, GlT, Rena loss
RETATIVE HYPERNATREMIA:EI Mosl common cause is WAIER
DEPLEIION, Na wilh inadequale
replacemenl
ABSOIUTE HYPERNATREMIAEI AINPUT .. Post-operalive
adminislralion of Saline
EI $ALT RETENIION.. Cushing $, Conn$, Hgperaldesteronism
MIID CASES (VECFI:Hgpolension, Tachgcardia, Oliguria,
Emptg Neck veins, Sunken eUe, DrU
longue, Drg Skin
ADVANCED CA$ES (OICFI:CNS manifeslalions
H gpertension, Tachgcardia,
Enlarged Neck veins, Ederna,
CNS manifeslations ending bg
seizures, Corna
CLltrllCAL
PICIURE
EI lF REIAIIVE: as waler inloxicaliong AB$OIUTE HYPONATREMIA:
- Mild lo rnoderafe) 0.9% NACI
- $evere) 5% NaCl ..(oNa lrnEq/hour)
N.B. lf more: demgelination of Nerues
EI TII. Of Cause
EI Active lrealrnenl:
Sodium-free waler(Correlaled wllh duralion of hgpernalremia)
M m. Of Cause
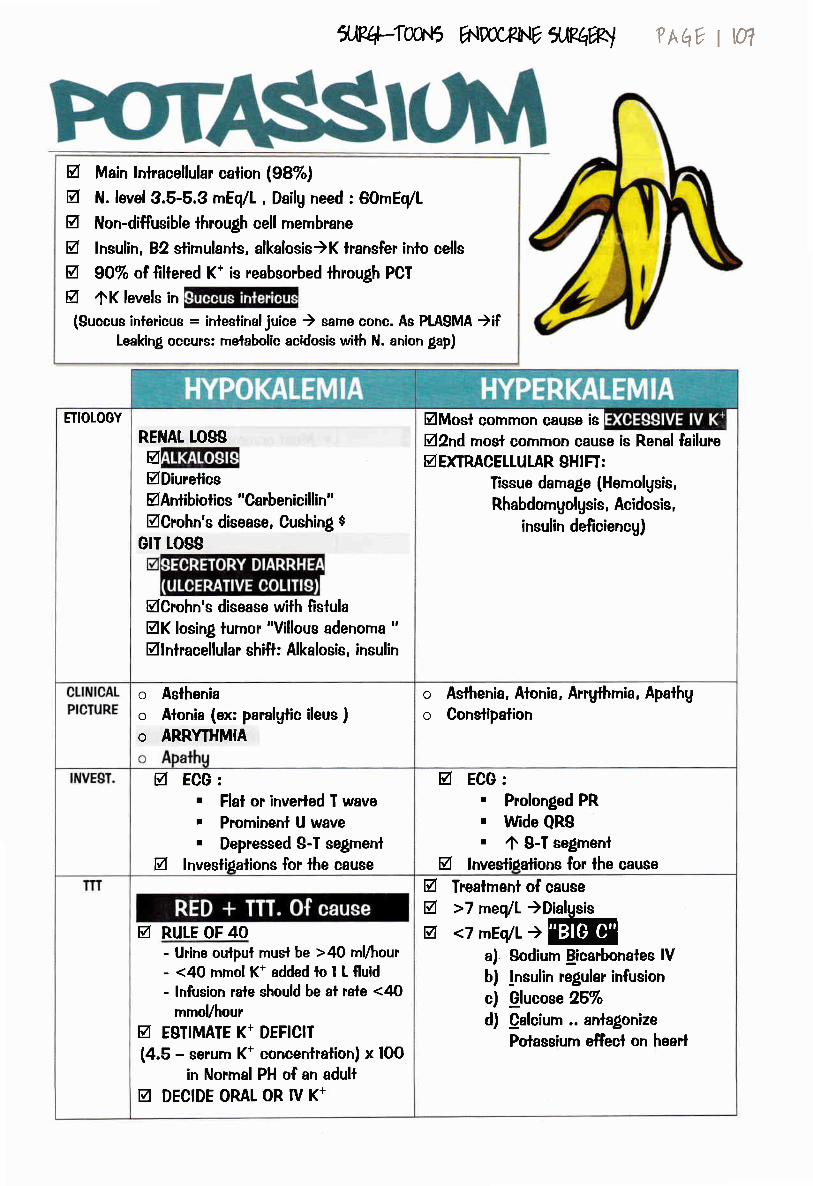
ilRq-Twr-5 ANDoC4qhE ffiqw ?Aqv I w
V Main lnlracellular calion 198%)A N. level 3.5-5.3 mEq/L , Dailg need : 60rnEq/Lg Non-diffusible lhrough cell rnernbraneg lnsulin, 82 slimulanls, alkalosis)K lransfer inlo cellsg 9O% oI {illered K* is reabsorbed through PCT
g 4K levels in
(Succue intericus = inleslinaljuice ) sarne conc. As PLASMA )ifleaking occurc: rnelabolic acidosis with N. anion gap)
ETIOLOGY
RENAT tOgSgElDiurelicsMAntibiolics "Carbenicillin"MCrohn's disease, Cushing $
GrT tosg
EICrohn's disease with {istulaEIK losing tumor "Villous adenorna "Mlnlracellular shift: Alkalosis, insulin
MMost cornmon cause is
VBnd rnost cornrnon cause is Renal failureEIDfiRACETLULAR, SHIFI:
Tissue damage (Hemolgsis,
Rhabdomgolgsis, Acidosis,
insulin de{iciencg)
o Astheniao Alonia (ex: paralgtic ileus )o ARRYTHMIA
o Asthenia, Alonia, Arrgfhmia, Apathg
o Conslipalion
g ECG:. Flal or inverled T wave, Prorninenl U wave. Depressed S-T segmenl
g lnvestipalions for lhe cause
V ECG:. Prolonged PR. Wde QRSr zfr S-I segment
g lnveslioalions for lhe cause
EI RULE OF 40- Urine oulpui musl be >40 mlhour- <4O rnrnol K* added to I L {luid- lnfusion rale should be al rale <40
mmoUhour
E ESTIMATE K+ DEFICIT
(4.5 - serurn K* concentration) x IOO
in Norrnat PH of an adullEI DECIDE OML OR IV K*
@ Trealrnenl of causeV >7 meq/L )Dialgsis-=---E
a) Sodium licarbonates lVb) lnsulin regular infusion
c) Olucose 25%d) Calcium .. anlalonize
Polassiurn effecl on heart

ilR4,-ToAr5 E{DoCFNY rJ,l?4W
V N level : 8.5 -10.5 m7dl
V Mosl cornmon sile is BONE$g Serurn calciunr exisls in 2 forrns:
- 50% ionized) ACTIVE FORM
- 50% Non-ionized ... l4O% of which is bound to albumin)
V Albumin's half-life in circulalion is 15 dagsg Delerrninalion of Prolein level is essenlial
in analgsis of Calcium levels
?hq* | 08
IT r1 IIrIrl Ig 1[' l7t : Il2: :IglITD: ill7t
ETIOTOGY ' Mosl cornrnon cause is
after thgroideclomg. Alkalosis. Hgpoalburninemia. Acule pancrealilis
Mosl cornrnon cause is
Hgper-parathgroidism
Thgroloxicosis
CLINICAT
PICIURE:
. Carpopedal spasm, $lridor, Convulsions
LATENT HYPOCALCEMIA:. CHOVESTECH SIGN: tapping over branches
of Facial)twilches in facial Ms. TRAUSSAU SIGN
BONE, MOOD, STONE, GIT
:: see clinical picture ofhgperparalhgroidism : :
lnvesli-gations
. Measure serum Calciunr . Measure serum Calcium. lnvestilations for cause:
- HVDerDaralhqroidism
:: see invesl'lgations ofhgperparalhgroidism : :
-Bone secondaries) Bone scan
TTI Vg
lO% : l0 ml lV slowltTTT. Of cause
MEDICAL TREATMENTg lV fluids , Bisphosphonales
TREATMENT OF CAUSE:fl Hgperparalhgrcidism
:: see lrealrnenl ofhgperparalhgroidism ::
V Bone secondaries:- lf operable) R.adical reseclion- lf inoperable) Palliative
reseclion, chernolherapg,
Radiotherapg
M Patient with Hgperparathgroidism
,exposed lo slressEI CLINICAL PICIURE:
- Polg-urea, Sevete dehgdration
M TREATMENI:
a) Ringer Laclaie
b)
c)

ffi(rTwt5 E{Docxht, ilEqw ? AEe I q
ACIDP/ISE CE, Producls of melabolism are predominafelg ACIDS (CO2, organic acids). Mainlenance of slable PH is achieved bg BUFFER 8YSTEM. Mosl imporlanl buffer is HCOS ... (easilg manipulated bg lungs & kidneg). HCOS is controlled gtOWLY bg KIDNEfS ... Change is MEIABOUC
PCOZ is controlled RAPIDLY bg TUNGB ... Change is RESPIMTORY. Blood Pll , Elecfrolgles are assessed bg ABG
. NORMAL VALUES: PH :7.95 -7.4HCO. : 22-26 mmoUl
PO2 75-l00mmol/L , PCO2 95-42 mrnol/L
PH = Pka + Log HCO/H2Co"
Bicarbonale, Carbonic acid ratio is 2O:l
. ln ang melabolic or respiralorg disorder...
OMPENSAITON will reslore Normal arlerial PH PARTIAILY
Metabolic acidosis) Hgpervenlilalion (VPCOJ
Metabolic alkalosis) Hgpoveniilalion (APCOr)
Respiralorg acidosis) HCO, produclion bg kidneg
Respiratorg Alkalosis) HCO. excretion
Eliologg: vPH, V HCO3
4Production o{ H+:
-DKA, Mgocardial
infar"ction
-lacllc acidosis
-Seplicemia, seplic
shock
HCO" Loss:
-aa--Renalfailurc
-Diarrhea, inielinal{istula
- Urelro-sigmoidostomg
^PH, 4HCO3
loss of H+:
-VOMITIN0, diarrhea
-Paradoxical aciduria
(CHP8, Pgloric slenosls)
-Diurelic therapg
(Ihiazide, loop diurclics)
O HCO,:
-44 inlake ofarrlacids (NaHCO")
4PCO2
lmovE[il.ATtoNCN0 depression,
Ms. Weakness
(Mgathenia
gravis), COPD
^PH, VPCO2
HYPERVETII.ATION
Hgslerioal,
Hgperpgrexia
Clinical
piclure:4Raie, depih of
Breathing..KUSMMEL'g BR.EATI{"
- C.P. of cause
- lfsevere) Ielang
- Cganosis
- lrrilabilitg4 Respimiorg rale
(Tetang, Respiratorg
anesl)
TTT. -m. Of cause
-lf severe) NaHOO,
(Bodg weighl x 0.3x Base deficient)
-m. Of cause
-!V saline
-lf severe) Arnrnoniurn
chloride Slowlg
Mechanical
venlilalion
Palienl respirc irrlo
a Paper bag

Cornoensalion:-oPco2(Hgpoventilaiion)
-VHCO. (Renal)
Xeq-fwg ,NDoCFNE X,V^W
Cornpensalion:-fHCO' (Buffer
sgslem)
-VH* (renal lossl
?hqv I m
UEq GJ
CornDensalion:-0PCO,
(Hgperventilation)
-VH* lRenal lossl
RESPIRATORY,
METABOTIC ALKALOSIS
aHco3, vPcoz
Other alkaline juices :
. Succus entericus
. Bile i
ANa,ACl, AH*, No HCO.
METABOLIC DISORDER, RESPIMTORY DISORDER
vPH, 4 PCO2 ^PH,
VPCO2VPH, V HCO3
^PH, 4 HCOs
MIXED DISORDER euiq lJlllft COz, HCO3 Jl eJ
RESPIRATORY,
]VIETABOLIC ACIDOSIS
VHCO3, 4PCO2
. Represenls Anions NOT usuallg measured
. Value: 10-19 mmo7lilre
. Calculalions: CAfIONB (Na, lq - ANIONS (Cl, HCO3)
. MEIABOLIC ACIDOSI$:
- Due to VHOOa.. NORMAT ANION GAP 1XCO, srii)(RF, diarrhea, Inteslinal fistulae)
- Due to 4 H* .. 4ANION GAP lncia tusi)(DKA, Lactic acidosis, Septic shock)

c*fr.4:lw.t5 ww*NY 1.R@l ? h{10 | lll
INDICATION$ OF ENTEMT NUITRITION:V In Palienls where ORAL inlake is inadequale :
(Cornalosed patienl, Severe dgsphagia, Neck surgeru, Burns)
PATIENT REQUIREMENTS:M Stp FEEDING: Whole food bg mouth (fluid formuta)EI Tueg FEEDING TECHNIQUES:
- NGT: Rgle'e tube- GASTROSTOMY) Liquid diel, Juice, Milk- JEJUNOSTOMY) Partiallg digested or elernenla! formulae
OOMPTICATION$ OF EIITEMI NUITRITION:- MECHANICAL: Malposition, displacemenl, BIockage, Breakage, Leakage- INFECIIVE: exogenous or endogenous- GII: Diarrhea, bloating, Nausea, vomitin!, abdominal cramps, conslipalion- METABOLIC/ CHEMICAL: Elecirolgte imbalance, malnuitrilion
TUTAt T{OMINDICAIIOIUS OF TPN:
M Blocked GlT... Slricture, Neoplasm, Exlrinsic rnass
M Shorf GlT... Short Gul sgndromeEI Fistulated GlT... Enteroculaneous {istulaEI lnflammed GlT... lnflammalorg Bowel disease
EI Unsuilable condition... GIT can'l cope as in severe traurna, hgper-catabolic slate
PAIIENT REQUIREMENTS:EI Suqical patient needs 40 KcallKg bodg weighl,24OO Kca7dagM Energg given:
(lgm CHO=4Kcal, lgm Protein=4Kcal, lgm Fat=9Kcal)EI Ratio in a well-balanced diel is .. (CHO 5OTo, Prolein 157o, Fal g5%)
M Requirernenls are liven in 2-4liters of Fluids as following:- CHO) Glucose 5O% + lnsulin- Prolein ) Varnine or Tolarnine- Fat) lntra-lipid l0%
COMPTICATIONS OF TPN:
- Nutritional & melabolic cornp!!ca]!ons;,(Hgperglgcemia, Hgpokalemia, Hgponalremia, Hgpercsmolar coma)
- Cenlral venous Catheter comPlicalions: (Hemolhorax, Pneurnofhorax,
Nerue injurg, Cenlral venous calheler infection & Sepiic thrombophlebitis)

1.R4-Toq..t5 1^m,RNY 1JWW ?hqv I w
GENEML COPLICATIONS:- Fever (Most cornrnon 4O%), Bed sores, Confusional slaleLOCAT WOUND COMPLICATIONS
OTHER gYgTEMg COMPLICATIONS
- ResDiralorv ... $ee Cardiolhoracic surlery ...- Cardiovascular cornplications:
Hgpotension, Hgperlension , DVT
- Gasiro-inteslinal cornplicalions:Posl-operalive Nausea, vorniling!, lnleslinal obslruclion, jaundice
- UrinargcomDlicafions:Renal failure, Acule relenlion, UTI
tr
trtr
DAYS (Reactionarg- Lung - Urine- wound)EI 0-l )Reaclionaru : Ebb phase of inflammalionfl 2-S ) Atelectasis of Lun!V 3-S ) Thrombophlebitis at the site of cannulafl5-7)DW,UTtV > Tdags) Wound infeclion or sub-diaphragmalic abscess
FOR UNCOMPTICATED PATIENTS) 3 LITERS OF FLUIDS
EI 5OO ml saline lO.9% NaCl)g 2.5 Lilers iYo Dexlrcse (Glucose)
V K* is liven afler 48 hours:- Saline is replaced bg KADALEX (Contains 27 mmolK+ll)- Polassium Chloride supplemenls
N.B. Correclion fluids irnbalance should be lo avoid fluid overload
CONTM-indications:EI Biliarg operationsM ComaEI CNg problems
EI Respiralorg depression
Withdrawal effects:Agitation, Vomiiing, Diarrhea
.riiill gJorJl.cl+i Ef pto!rJrk

?hqt t v
l. Focused abdominal sonograrn for iraurna(FAST) assesses for blood in pericardial sac,
hepalorenal pouch, pelvis & spleno-renalpouch, bul NOT in relroperilonea! space.
Small inlesline is the rnosl commonlg affecled organ in penelrating injurg of abdomen.The rnosl irnporlanl slep in lreatrnenl of septic shock is drainage of septic collecfions.Allowing blood which is readg for lransfusion lo remain for 4 hours in warm environrneniencourages bacterial proliferation & septicemia.Donaled blood is nol roulinelg screened for CMV.
The mosl cornrnon problem resulting in hernoslasis is lhrombocgtopenia.Warfarin has half-life of about 36 hours.Warfarin crosses the placenta & should be avoided in pregnancg.
Half-life of faclor Vlll is 8 hours.
l. Newborn infants have the lrealesl proportion of total bodg waler (total bodg walerdecreases steadilg wilh age).
2. Females & obese persons have a decreased percenlage of TBW.
3. ln a healthg adull, exlracellular osmolarilg is lhe same as inlracellular osrnolaritg.4. Norrnal saline conlains 154 mmd Sodiurn & 154 rnmol Chloride.5. HARTMANN'S $OLUTION conlains calcium bicarbonale.6. The major anion in lhe inlracellular fluid is PHOSPHATE .
7. Sodium urinarg excrelion is reduced after lraurna.
8. lnlracellular concenlralion of K* is 150 mEq/1.
9. The averuge dailg need of K* is aboul 60 mEq/I.lO. The rnosl serious consequence of K* irnbalance is cardiac abnorrnalilies.ll. Magnesiurn is lhe 2^d rnosl abundanl inlracellular calion.12. Ihe cardiovascular effects of hgpomagnesaemia are similar lo those of hgpokalemia.
13. The rnosl significanl inorganic plasma buffer is bicarbonale.14. The 3 mosl important buffers in bodg fluids include: bicarbonate, phosphale & prolein.15. Ihe ideal infusion fluid for correclion of hgpokalemic alkalosis due lo pgloric obslruclion is
norrnal saline.
Locallg invasive lurnors include basal cell carcinorna, rnixed salivarg lumor, bronchial
adenorna, adamanlinorna & osleoclaslorna.Genelic predisposition to cancer is relaled lo inueased chrornosomal fra$litg & defect in
DNA repair enzgmes.
Thgroid, breasl & lung cancers are cornrnonlg melaslasizing bg blood.
cJJR{+-TooN5 1r"l{[rr'*Nv ARqW
2.g.
4.
5.6.7.
8.9.
2.
3.

leq4w-tS ,ND0CRNY l"RqW ?h I r[4
Clinical picture of seplic shockKasnZM )
Managernenl of septic shockG4ilar trl, zoll
Patienl wilh seplic shock have athose with hgpovolernic shock
(Kasn 2M )Discuss Etiopaihologg and clP of hgpovolernic shock
Kan 2o// - 5u sfiams, zoo/, znz - Alur rlrL zo/, zmlTgpes of Hernomhage and their rnanalernenl
( Kasn 2@7 )Factors affectin! wound healing
( ,4ilar rlr1,2W - A** f,2@6,2@5 - Kasn 2@f )Cornplications of wound healingf
( Kasn 2d )r Cornplicalions of Blood TransfusionKan 2@f 2M-,4lr sfiarrls, 2W, zfu
- r4y'ur f, 2@f Z@4, 2@/, 2fu5, 2M -,4y'rar rl/, zmz 2@6, 2@4, 2@5, 2@/1r Cornplications of spina! anesthesia
Kar, z@r- ,4y'rar ril,2@2,2@/,2m -,4y'ar F,2@22@6,2Ut4 )r Cornplicalions of general aneslhesia
( Ailar f,2@O - Ay'rar rl/, Zm/ )r Enurnerate posl-operaiive cornplicalions( Ailar f,2@7)r Posl-operative pulrnonarg cornplications
( ,4ilar f,2@4 - r4y'rar rl/, ZnC)r Post-operalive fever(Kasn2M )
worse prognosis than
aa



Brain
Ji,gi;ietr r'ell
Arms
rilbrtael Safwat/1ABBClt - slaws
SLrtertor !8lia taYa
',-.,i2('ot .iefia Q'!a
lleoa',lc ', elr
Hepaiic c0ta1 'jerii
i-iver
?e.tall ie::l
!i,aa':e,,.
Lo!"jea ;!Cv :i':S rels

Severe, in lhe rnosl peripheral part of limbPallor
l) Marble white2) Mottled ,pp. After 6-12 hours3) Fixed blue slaining of skin ........
IR.R,EI/ER.SIBLE
Pulselesness dislal lo sile of embolisalion
ParalgsisEarlg in arterial, lale in venous obslruclion
Paraslhesia (Anesthesia)LATE, bul reversible after TfT for few monlhs
Progressive Coldness
@
@
VIAEI-E THRPtTBIED lffi
leq-fw$ EFTDtrXNE g,^?4W ? hh ! tq
E Young agetr lncidence: FlA, Fernoral l4o%)tr PDF:
. Mitral slenosis with AF
. Lefl alrial Mgxorna
. Mural lhrornbosis
. Frorn Larle arteries)Alherosclerosis, aneurusrns
. Veins) Venous thrornbi,VSD, ASD, Eisenrnenger $
tr LIMB :/ $udden onsel/ Pale, while,
DEFINIIION: Lack of blood flow due toeudden occlusion of previouslg patent artergwith NO lirne for collalerals fo open.
Fixed color changes
:
trtr
///
OLD agePDF :
tr s acc.To affecled arterq :
. Brain )TlA, Stroke
. Relina )Arnaurosis Fulax
. Mesenleric vessels)Gangrene
. Spleen ) Loca! pain
. Kidnegs ) Hernaluria
. Alherosclerosis
. Slasis,Hgper-viscosilg(Diarrhea, polgcgthemia)
tr LIMB :
/ Acule bui less drarnalic/ Pale, white/ TROPHIC CHANGES
// ANGTO> +VECOLTATERALS
/ Pasl Hislorg oflnlerrnitlent
ETIOLOGYE OpenE ClosedEtr lalrogenicE lntra-arterial
drug lnjectionclo:E Historg of
lraurnatr Bleedingo/E:tr Shocktr Hard signs vs.
Soft signsclaudicali

Srrpor rMpIGnoN
g Block of mainarterial lree
V PRE.OPg INTRA.OP)For fhreatened limb
oFETpl.Oq/ggV
ECHO, ECG)Deiect AFX-rag ) lnjuriesUS ) Aneurgsrn
a&q'-tw.$ 6{Doc^PI.lE IJRqW
A +VE collalerals
oFffi
FERIPHERATffi
tr
tr
Muscle Necrosis :4TLC, 4CPK, AcidosisHgpovolemia :4Hb, Crealinine, BUN
? AqY t Ytn
H/AFD StqlUS vS sEoFT sltGIUS
tr 6Pstr Pulsatile Hemorrhagetr Pulsalile Hernalomatr Palpable thrill, bruit
trtrtrtr
Hernaloma non pulsaling, non-expandingNerve injurgWound is near a rnajor vascular slructureDelaged capillarg refilling time
Urgent lnvestigations

PREoffigggdd
HospitalizalionOxggen, d'rgiialisAnlibioticsMorphineHeparin : SOOO units lV
eMgo;StJltr lf wiihin 6 hours:URGENT EMBOLECTOMY (Fogerrg catheler)
l) Fernoral arterg) Cornrnon femorallransverse arteriotomg
2) Aortic bifuricalion) Bilateral Femoralarteriolomies
tr lf Late :
nfrnAcrffi
Fasciolomg(To prevent cornpartmental $)
tr S'rgns of adequale emboleclorng:. Pulse fell. Color, ternperalure. Fleverse bleeding. lnlra-Op angiographg
lLlq.q:l}r/,.r5 1^9rr/PNY IJRqW
eryleoust/ltr Anli-coagulantstr Anti-arrglhrnics
oFCAGEE
ffi
MCSI
Follow up clinicallg and
VIAETE
Podroffi
angiographu
-
T{roMBocllsEleclive BYPASS
?AEi; I Wl
T{FEATEDbUrgenl ANGIO+ URGENT
R.EVASCULAR.IZATION
SURGERY
AI{IERLIIL $[rt,FI/
OFGOME
No wlFno\lErllntrI
URGENTRe-vascularization
tr GangreneArnpulafionVolkrnan'scontraclureTendon lransferCrush $
lV fluids,
Alkalanizalion
of urine
tr
lffiAMPUTATION
tr
trtr
tr
Streplokinase Pulse sprag or lVLoading dose, followed bgrnainlenanceR.ecenl) Recornbinant Tissueplasrninogen aclivator

TIT oF FERIF|{ERAL AnrrmrAU INJ,F!/nfr
PRIMARY SURVEY: ABCDE .... Airurag, breathing, circulation, Drugs, eXposureSECONDARY suR.vEY : Head lo loe Exam, AMPLE Hislorg , lnvesligalions (An$o ,Doppler)
MOFAIilEFRACTT'RE
Pulse relurns
DEAL WITH THE FRACTURE
lrrigate wilh saline &Wound debridrnent
Skin) Excision of l-2cmFascia) Open lense fascia
Mg.) Excision of dead Ms.
Nerue) Mark with black silk
Blood vessel ) Deal asClo.sed injurg wilh tear...
trtrtrtrtr
ODEN
WAII fior 20 rninutes
1R{4:locllt5 .^*,,*NYilPq*'
t{tfttourrE(R
SpasrttI
Painting Orlntra-arterialpapaverine
No pulse
D(PLORE & DEAL
? hq t w,?-
CortnstoNI
Excision of theconlused
segmenl andsaphenous graft
ch.m
PAXTIAT,
<l/2circumference
IRepair with
proline sulures
I{ITHTEAR
>l/2circumference
I
Treal as
Cornplete
Corinerer)
2)3)4)
Repair inobligue mahherMobilize artergCul branchesBaphenousvein grafl

cqnoN penrPl+*ALffiDlslEASE
.ASJMTMdUS
chrNrcAr srAgEs (Fs,trAllG)
TYPE OF PAIIENTtr Aiherosclerosis ) Male>S0 Uears wiih risk
faclors (DM, HfN, Obesitg)tr Buroer's ) Male 2O-4O Year. Heavg smokergYMPIOMg
tr Cramp-like PAIN, ,1. bg walking, V bg & resli tr Prcgression ) shorter claudication dislance,
4Period of resttr Affection of other sgsierns
, r CNS : TlA, slroke. ryq HF. Kidneq : Pain. hernaturia, hgpertension. @!!g!.;. Leriche sgndrome
OENERAL EXAMINAIIONtr Vilal s'rgns :
. Bgslolic Bruit )(Aneurgsrn)
. Conlinuous Bruil )(arterio-vehous fislula)LOCAL EXAMINAIION) LIMB IIII LAYERS
lJ?q,-Toqr5 E{D0CXNE ilRhW
DIAEEf,ICPRESENILE
AIHEROSCLEROSIS
CI.AUDICANT LIMB
WPE OF PAIIENTtr Alherosclerosis ) Male>SO
gearc wilh risk faclors (DM, HTN,
Obesitg)tr Burper's )Male 2O-4O Yr ,
Heavg srnokerI- REST PAINtr Severe pain lhal awakens Pl.
from sleeptr 4bg REST, AT NIGHT,
ELEVATING LEG
tr Vbg Hangn! foot downtr NEI/ER above Ankletr Drg gangrene ...... (Wef if
HF, lnfection)2. ABSENCE OF PERIPHEMT
PULSATION
BrrItcFRS ffi'Sffiffi
?hh? t w7
I. UICER, RESISIANTFOR, HEATING:
tr Tender ulcer BetweenToes, dorsurn of foot
tr Edge ) Punched oultr Margin ) Black,
rnumrniftedtr Floor ) Granulationtr Base ) Diflicull to
palpate2. GANGRENE

DOPPIER. i..
, r.al1-r4l
Biphasic flow(Collaterals)
,-l
DrrPl^D(
iiqLitABP!
. Normal >l
. O.5 : CLI
ln diabelics )foe Brachial index
PFEOFENffi\IEW.ADVANTAGES:
- Site of slenosis- Exlenl of stenosis- Collalerals- Run in & off
.TECHNTQUES:
- Direct femoral arleriographg- Trans-lurnbar arteriographg(if bofh femoral pulses aren't pulsable)- frans-axillarg arleriographg(if fhe whole dislat aoria is occluded)
. COMPLICATIONS:- Neurologica! deficit- Hernorrhage- Pulsalile rnass- lnfeclion al punclure sile- Allergic reaction to lhe conlrast
rnedia- Thrornbosis
1Rt4-{our5 E{DocxhrE 1,^Phwl
lFITF)MRA
CBO)Anernia, Polucvlhernia(Anernia eggravaled ischernia)FBS >DMKFt >Alherosclerolic kidnegLFt ) lrnpairedECG )IHDCXR )Promineni aorlic knuckle.
tr
trtrtrtrtr
?A6F I W
trcalcified atherornaL:pid profile

BES;rMDIGATTITtr RISK FACTORS MODIFICATION
. Cessation of srnoking
. Proper conlrol of DM
. Conlrol BP
. Lipid loweringtr ANTI.PIATELETS
. Aspirin 75 mgldag(lf patient is inloleranl) Plavix)
' Clopidogreltr VASO ACIIVE DRUGStr CARE OF FOOT
tr DGRCI$E (to Oclaudicalion distance)
rMffir{o{+Mffi
1JP,440qr5 AWOC*hIE 1,,RqW
S${oncrSrcfiertrg EndartereclorngV Balloon Angioplastg
Wth or wilhoul Stenl
+\,E DISTALFTJNoFF
PFEffiAT.IGIW
roD.Gsrciltatr
ARTERIAL BYPASS
AFO/E${qor.lALuqAirrtr
aV
?k e I w
Aorto- Bifernoral BgpasslF UNFIT (e.g. cardiacpatient)) Axillo-Bifemoral Bgpass
Sgnthefic graft
- \rEDlsrALlg6laryp
SYNTHETICKNITTED
DACR.ON
*:Htfl#.DtSAN PGUI SYMPATHECIOMYEI Arnputalion
EE.olr,h.lclorl.htTEAFJtT
(,i[r.ArmAu. lF Hf) Aorto-
fernoral bgpass. IF UNFI'
Fernoro-FernoralBgpass
Saphenous Graft
D{sm, FartsnsED
Femoro-distal
bgpass
Femoro-Poplitealbgpass
fuJl a#hifuJl g +.r-tll
+i.lall
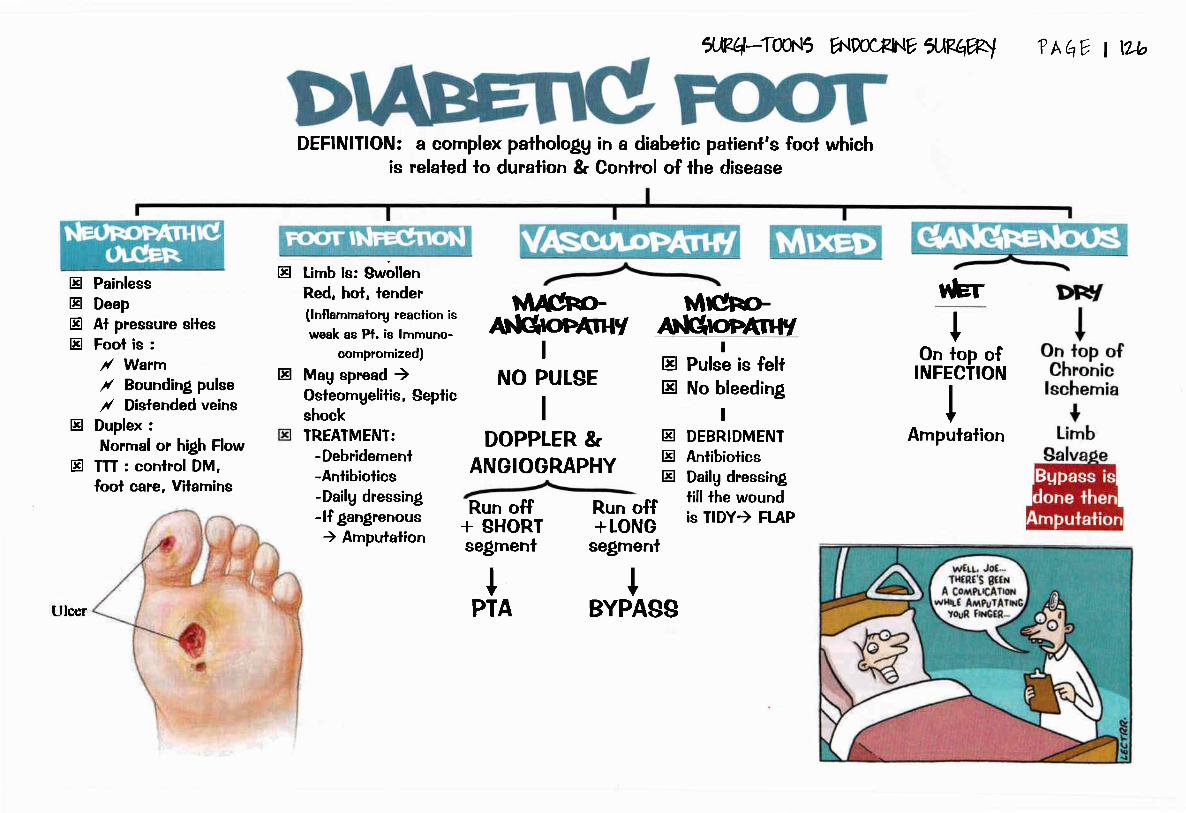
trtrtrtr
PainlessDeepAl pressure silesFool is :/ Wann/ Bounding pulse
/ Dlslended veinsDuplex :
Norrnal or high FlowTTT : conlrol DM,fool care. Vilamins
DEFINITION:is
tr
tr
tr Lirnb is: SwollenRed, hol, lender(lnflammalorg reaclion isweak as Pt. is lrnmuno-
compromized)
tr Mag spread )Osleorngelitis, Septicshock
a cornplex pathologg in a diabetic patient's fool whichrelaled to duralion & Control of the disease
Ulcer
TREATMENT:-Debridernenl-Antibiotics-Dailg dressing-lf gangrenous) Amputaiion
5E44wr5 ENDOCXI{E IJRqW
tvlrchoraNGretuy
I
NO PULSE
I
DOPPLER &ANGIOGRAPHY
Mrcho.aN6ontn+r
Run off+ SHORIsegrnent
trtr
!Pulse is fellNo bleeding
IDEBRIDMENIAntibiolicsDailg dressingtill the woundis TIDY) FLAP
IPTA
?Aqv t wo
Run off+LONG
segmenl
tBYPASg
trtrtr
trler
tOn top of
INFECTION
IArnpulalion

vAso€PAsrl
//DtS=.(Sri
ETIOLOGY:
- 'lt sgmpathelic lone- Psgchologicalinslabilitg- Abnorma! sensilivilg of hand to coldnessCLINICAT HCTURE:
- Youn! fernale "ii'lUrilrr Jsgl{JI r-".s ldf 11| iiJ:ro fi 16rJl lJ, tli{
- [[ tuophic changes- Peri-pheral Pulsatiohs are trE
Care ofPatienl
. Slop smoking
. Avoid coldweaiher
. TTT. of anerniaif preseni
lJpq-Taqr5 A{DOoFINE *PqW ? AqV I W
Care ofHand
. Drgness
. Woolen gloves
. Exercise
DEFINITION: Recurrenl ischernical-lacks precipilated bg exposureto coldness or emolional slress
DrugsI
. Vasodilalors
. Babg aspirin
. CCB
,/ ETIOLOGY:
- CollaAen: 9LE, Scleroderma
. &&()YAW, Sgmpalhectomg is EFFECfNE
. EpI$I-EIIE Emerlencg m) lmrnersion of affecied parl in Warrn waler l40-44o)
Surterg
Sgmpatheclomg(Cervico-dorsall
Arlerial obslruclion: Burger's disease
Nerve injurg: fhoracic oullel $, Carpa! tunnel $
Druss: Beta Blockers
// CLINICAL HCIURE:- [email protected] @ Trophic chanles- [EP"ripheralPutsalions
TTf ofCAUgE
Vasodilalors(Avoid BelaBlockers)
Sgmpathectorng
NO BENEFIT D(CEPT:. lf vasculilis occur. Crgo-anlibodies(Makes sgrnpalheclorng
ineffecfive)

M
yoot{GpffiED{rI
@Affects Big
vesselse.g. aorta
Cr-lpNlc
Surgica! iniervention* lndication: >7O7o slenosis if Sgmptomatic or
>8O% if Asgmplomatic* Method :t) Carotid Angioplasig & Stenting2l Endartereclomg
oLD PArlED{rI
@
lJPr+-Twr5 r^Jiw*Nr.eruW
Biopsg jl 69iao g Angio g .-otluiSOther Narnes:
@ Chernodecloma@ Polato Turnor
Angiographg:
@ Widening of the Carotid Artergbifurcation
?Aqv I w3
Excision or ligation, wilh presen ation of ICA
@ HgpertensionNOT respondinglo medication
@ freatrnenl:Balloon dilatation& Stent dlte efnraya been a hlgh addever, alwayc crrlvlng 6oc
blggcr, hcH, grrcaer.-.rrd now audden[r lrrr cqioliledto c.ltle for &hycri blood prrer{}unc and lers cholcstcroI?t,

BOUNDARIES OF IHECOMPREggINO
IRIANGLE:-Scalenus anlerior-ecalenus rnedius-Firsl rib
Cornpression of Lower lrunkof brachial Plexus
1r{oRA(,lC,
On Ulnar sideof Hand &
Forearm
SylbnoMeDEFINITION: Cornpression of N. (Brachial plexus)& arterg (Subclavian A.) while crossing through
lhe narrow triangle ir;the base of Neck
Small MusclesOf Hand )Alrophg &Weakness
1,,Rq-IC[/,f5
Angiographg:- Cornpression of $ubclavian arterg on Elevalion of arm- There'sPosl-slenoiicdilatationPlain x-rag) Cerivcal ribNerve conduclion velocilg is prolonged
GltpNtclscltBtlA
oF(LClaudication 2rg Ragnaud
pain with Phenornenonexercise
SIGNS:
trtr
Cornpression of Subclavian Arlerg
a{DocPtE apawEtiologg
E Cervical ribE Scalene $ o+lvrr#slJltr Hgperabduciion $ Uirl6illtr Mal-union of ClavicleEI Pencosl lurnor
FGTSnED{snCDlrArffioN
Emboli to lndex &middle {inger
(DrGrrAr GANGRENE)
? Ah[, I W1
Compression of Subclavian Vein(Rare as il's oulside lhe triangle)
Effort fhrornbosis&DW
M!LD (NEUROLOGTCAL)
tr Phgsio & Shoulder exercise
) Radial pulse becornes weak
gEvERE (ARTER|AL)
tr R.eseciion of Ceruical ribor lsl rib
tr Scalenotorng

ilPq,-Twr5 wwIJNYxMRJ
ETIOTOGY:
Congenital, Atheroselerosis, Sgphilis, Traumalic
TYPE OF PATIENT:- Old patienl (Atherosclerolic)- Yount palient (Traumafic, congenital)
SYMPTOMS:- MrU be asgmptornalic ...- Swelling, Pressure & lschemic rnanifeslalions
SIGNS:
Tfi{1V I W
DEFIN!IION:l- Sac {illed with blood comrnunicaiing with an arlerg2- Permanent localized dilatation of an arlerg l-5 limes lhe norrnal ,{
I
I
I
I
I
COMPTICATIONS:I
I
T
I
t
INVESTIGATIONS
CgsticAlong course of arlergMoves the artergCornpressible or partiallg cornpressible (thrombosis)Auscullalion) Bruil
Pressure rnanifeslalions) V,A, N.
lschemia
Ihrombosis, Embolism,Alherosclerosislnfection) Rupture, secondarg hemorrhage
Follow up everg 3 months bg U/S
. Screening) @, Diagnoslic). Best pre-operalive lnvestigations)
N.B. Angiographg doesn'f show lhe true diameter of aneurgsrn
r-TREATMENT-rConservative Surgerg if indicated
. INDICAIONS OF SURGERY
- lf sgmplomatic
- Diarneter)Scrn
- High risk palient
'SURGICAI PROCEDURES
Excision & grafl
Exclusion graft
lnlra-luminal self-
inflatable graft

cilq.q-Tmr5 flpmxnr rtlBt w ?hqv t vl
ABDOMN{ALAOFilC
INCIDENCE:- 95% due io alherosclerosis- g5% below origin of Renal arleries. 75% ASYMPTOMATIC
CLINICAL PICTURE:- Vague abdominal pain with backache
COMPLICATIONS:* RUPTURE:
Shock, acule abdominal pain, Pulsating epigaslric rnass* Dista! ernbolization
l) Sponlaneous) Blue loe $
2) lalrogenic) Trash Fool
INVE$TIGATIONS:- For aneurgsrn) U/9, CT, MRA, Anliolraphg- For olher sgslerns) ECG, CBC, Lipid profile
Surgerg if indicaled. INDICAIONS OF SURGERY
- lf sgrnplomalic, Diarneler>Scm,High
risk patienl
. SURGICAL PROCEDURES
- Excision & grafi
- Exclusion grafl
- lnlra-lurninal self-inflalablegraft
r-TREATMENT_rConservative
Follow up every 3 monlhs bg U/S
. INTRA-PERITONEAL:Fatal
. RETRO-PERITONEAL (IEAKING A.A.): Epigastric pain & thock
O/E: Pulsating popliteal A. in a palienl who's nol thinCOMPLICATIONS:
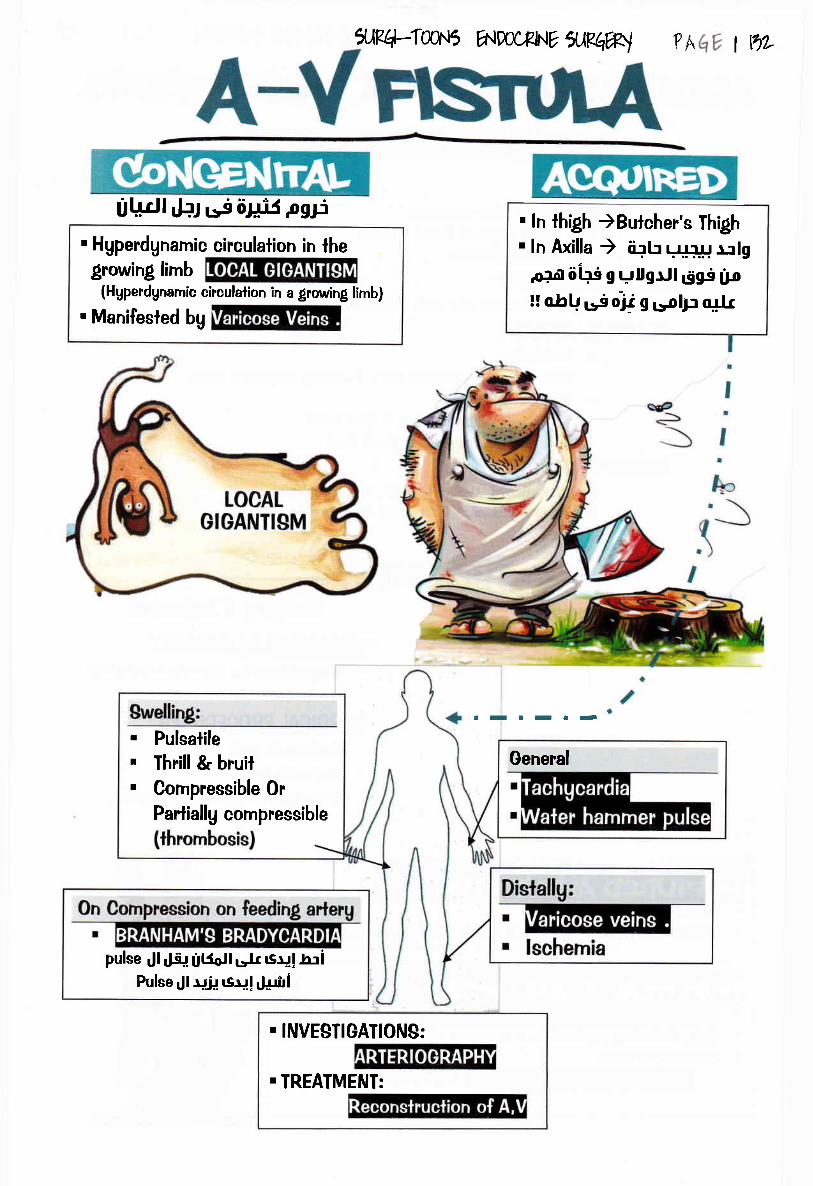
il?4-Tw\5 A{DocEN? "ilK#,] ?& | t1?-
Ul,;dl rF.t r-g tir+ij pgF. Hgperdgnamic circulation in thegrowing lirnb
(Hgpendgnarnic circulation in a growing lirnb)
. Manifesied bg
pulse Jl rJs{ fil5otl sfr rsrl!Ir:iPulse rll ujf rsu! rJ+iri
. ln thigh )Butcher's Thigh
. ln Axilla ) ii+h r,',!r$l r:lg.ofar iiirs g uUgrJl dgs lJo!l oJrU *j rji g rsplp "$r
IIIITT.
. Pulsalile
. Thrill & bruit
. Cornpressible Or
Partiallg compressible
General
. INVESTIGATIONS:
.IREATMENT:

ilPq4wt5
E[]OLOGY: l. lschemic ) thrombosis, embolisrn, vasospaslic disease.
2. Neuropathic ) sgrinlomgelia, leprosg.
3. Venous Ganglrene (see below)
4. fraumalic ) direct (bed sores),or indirecl (aderial injuries)
5. lnfective ) Epecific infeclion or Non-specilic infeclion
6. Phgsiochemical ) burns, caustics, froslbile,...
TYPE$ OF GANGRENE:
?h I wnrccFNtr lRh%l
Mauoscopic dealh of tissues due lo loss of blood supplg and is usuallgassocialed with baclerial invasion
Causes Chronic ischemia - Acule ischemia
- Chronic ischemia wilhpre-existing ederna
(cardiac, DW).
- PRIMARY: lnfection of lissueswith virulenl organisms leading togahgrene
- $ECONDARY: lnfection of slerile
Qan{renePalhologg
Putrefaclion Minimal Manked
Odor liftle or no odor Veru offensive
Gross picfure - DrU,Wrinkled,Murnmified.
- Hard, Dark
- Ihe part remains oflhe same size and
consislencg.- Color: dead white
)purple or greenish
black.
Line ofdemarcalion
well de{ined ill delined (no lime forevaDoralionl
Fale Separalion ) Leaving
a conical slumpSpread )
SKIPPED LESIONS
clP l. The five cardinal s'rgns of local death :
Lost (pulsation, Sensalion, Heaf, Funclion ofaffecled part, fxed color changes)
..... Press & see How Color fades .....
- fhe affected limb beeomes
swollen, edemalous and markedlg
inflamed.
- Ihe skin )moisl wilh bullae
- offensive odour & mag crcpilale
2. Minimalloxernia )betler general
condition.
3. Severe loxemia )poor genera! condition.
Trealmenl - Limb salvage(conservaliveamputalion).
- Non-conservaliveampulalion.
- Ampulalion tillihelevel of pulsalion
- Ttt of lhe cause ifpossible.

. Sudden onsel of scrolal inflarnrnalion
. sudden onsel ofgangrene
. Mag be associated wilh necroiizingfasciilis
Trealrnenl.l) Antibiolics & wide surlical excision.
2) Laler) skin graft lo cover lhe leslis.
?hqv t w
. Caused bg exlensive lhrombosis of lhernajor peripheral veins (phlegrnasia ceruleadolens)
. flealmenl:l) Elevate limb
2) Anticoagulanl lherapg is started.3) Thrombeclorng or fibrinolglic lrealrnenl
should be considered.
ilPq-Tou\5
OF
- $ite> over, bong prominence(sacrum, ischial luberositg or heels)
Etiologg- Prolonged pressure.- After irnrnobilizalion of paraplegic palienls,
elderlg & diabetics...Bong prominence culs the blood supplg of
Trealrnenl
,ND0CRN? ileqW1
PROPHYLACTIC TREATM ENT ACTIVE TREATMENT- Air rnallress- Skin should be kept drg & clean.- Frequenl change of posilion everg 2
hours.
- Debridemenl- Leave lhe wound open unlil healing- Repeated dressing with llgcerin rnagnesia
- Anlibiotics

5UP.4-Tffi\5 ENmflf.lV5WR1 ?h lW

5R4:lwr5 ^',,*NY
lRqW ?hqY t ttu
TI{FOMBO$SN.B. VTRCHOW IRIAD: VELOCITY, VlgCOglTY, VEggEL WAIL
lJlI;el uri !VeinsJI
DEEP T]IROMBO$SCLINICAL PICIURE:. ASYMPTOMATIC: Mosl cases are silenl bul are suspected bg unerylained
Posl-operalive fever,. gYMPIOMAIIC:
- GENEML C/P: Fever, T,
. LOCAT C/P:
COMPLICATIONS:* GENEML: Pulmonarg Embolism
* LOCAL:
- EARTY: Phlegmasia ALBA dolens, Phlegmasia CERULA dolens
- LATE: Post-phlebitic limb leading lo 2rg Varciose veins, Venous gangrene
INVESTIGATIONS:. FOR DIAGNOBIS:
- Colored Duplex- Recenllg: SPIML CI, Radioactive Fibrinolen
. FOR PULMONARY EMBOLI$M:- SPIRAL CT, V/Q LUNG SCAN, Angiographg, Chesl X-rag
. INVESTIOATIONS OF DW IN YOUNG PATIENI OR RECURRENT CASES:. PROIEIN C&S, ANTI.IHROMBIN-3 , LUPUS ANIICOAGULANI
TIRoMBoP+lr-EErilS TGRAD,ISDEFINITION:
A tgpe of superlicial thrombophlebitis lhal resolvessponlaneouslg in few weeks then appear in anolhet a?ea
OCCURS WIIH:- Visceral cancer "The Earliest sign"
- Burger's disease
- Polgcgthemia, PAN
- Ulcerative colilis, SLE

FOR ALL
PAIIENT
tr Earlg ambulaliontr Active exercisetr Post-op. Hgdration
FOR HIGH
RISK GR,OUPS
E lnlra-Op InlermitlenlPneurnalic Cornpression
tr Prophglactic LMW heparin
? AEV t t1l
FOR COMPTICAIIONS
gURGICAL
Ind'rcalions:. Confra-indication to
Anlicoagulanls e.g. :- Hgpertension
- Past Historg ofMigraine, On
NAglDs) PU. RECURRENCE OF P.E.
inspite of ful!heparinizalion
DW
GENERAL
Bed rcst for 7-lOdags, Vilamin E,
Elaslic slockings
DRUG
FIBRINOTYTICg
. ln lhe lirsl 3 dags
9treplokinase, urokinase
Rece
. lNDlCATlOItlS:- lsolaled llio-femoral DW- lmpending venous gang€ne
"Phlegmasia cerula dolens". CONIRAINDICAIIONS:
- Wthin lO dags of rnajor
operalion- Wrthin 2 monlhs frorn sfioke
TTI OF COMPLICAIIONS:- PUTMONARY EMBOLISM: Morphine, O2, Thrombolglics,
Anticoagulants, Emboleclorng
- POBI PtltEBlIlC LIMB: Compression Bandage
ANII.COAGULANTS
. Heparin for lO dags
. lnfroduce Oral anli-coagulanlsat the 7* drg
' Elop heparin at lhe lOrh and
conlinue oral anlicoagulanls{or 3-6 ms (tf l't DW), I gear
(if 2"d), or For life (if 3d)
l0 mg Loading then 5 mg/dag
P[, INR (2.5-3.5 times)
N :ll-14 secPTI
lwice normal :25-36 sec

StilArerylpur
Etr lmpacled in theeripheral arlerioles
E Recurrence)Pulrnonarg hgpertension ClP:
- Severe pleurilic pain
- Dgspnea- Hemoplgsis
ETIOLOGY:. Secondarg lo DW, lnfeclive endocardilis, Other emboli
INVESTIGATION$:. SPIML CT: ... Clot appears as lilling defecl ...
Pulrnonarv anoio(raphu: "Mosl accurale bul "D.DIMER: -ve) Sfop)
Blood lesls:- 4LDH, Serum Alkaline phosphatase
- Norrnal Bilirubin .... (,1.1t HF occurs)- ABG) Hgpoxia, Norrnal PCO2
Radioloou:- ECG) P-Pulmonale, Axis devialion to lhe R''ghl
- CXR) Normal inSO% of cases, Wedge shaped peripheral capacilg
TREAIMENT:
' Prophglaxis & TTT. of DW. frealment of pulmonarg embolism:
CURATIVE
$MALL & MEDIUM SIZED EMBOLI) Anticoagulants
MASSIVE PULMONARY EMBOTISM
l- Cardiac cathelerizalion2- Thrombolgtics) $lrepfokinase3- Assess Cardiac function/G hours
lf NO irnprovernenl ) urgenl pulmonarg emboleclorng after 6 hours
R,ECURRENCE
- Prophglaxis bg IVC Filter
I nches of
(if +ve) Conlinue invesfigalions,
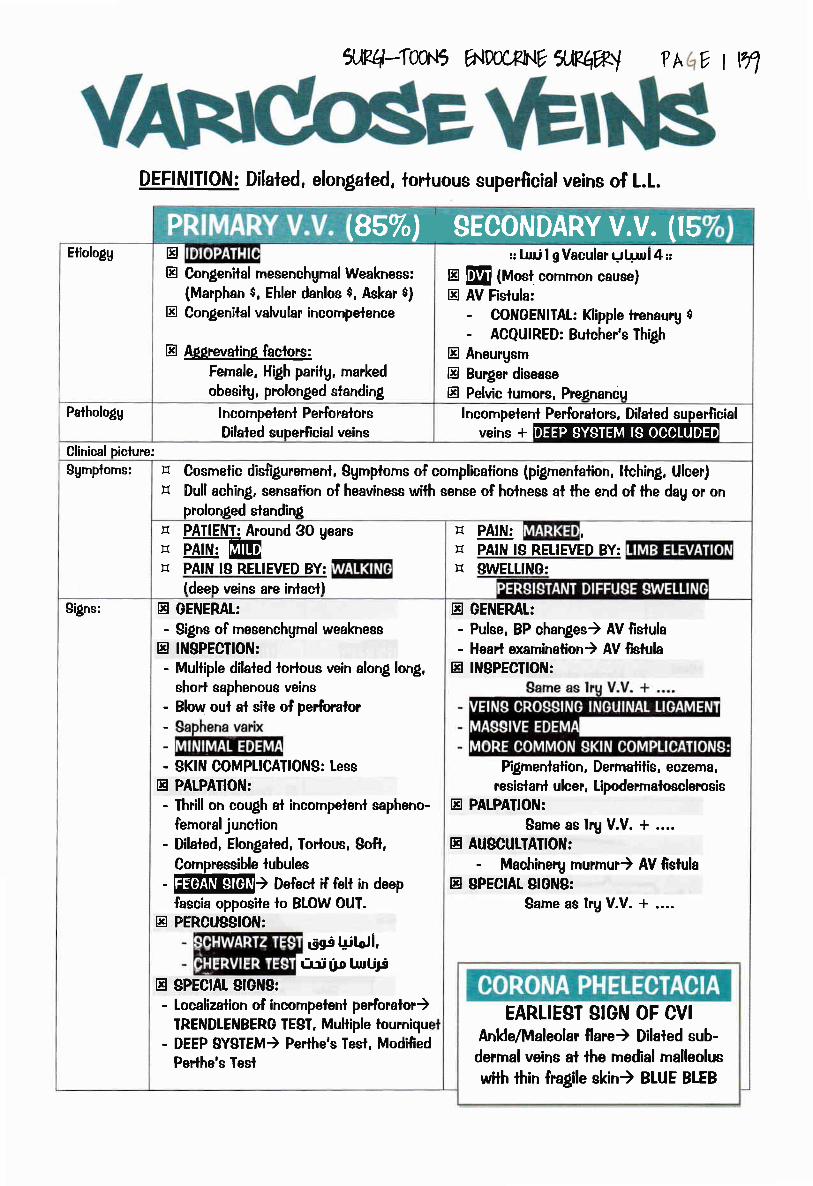
cJ'R4-TWr5 1allw*UVfl,Rqw ?h 0lln
DEFINITION: Dilaled, elongafed, lorluous superficial veins of L.L.
)a [iffi Lq {II rt I FI t YIrr-[EEtiologg tr
E Congenilal rnesenchgrnal Weakness:(Marphan $, Ehler danlos $, Askar $)
tr Congenital valvular incornpetence
E AElrevatin( faclors:Fernale. High paritg, marked
obesilg, prolonged standing
:: llri I g Vacular gl ! r,rl{;3
tr M (Most common cause)tr AV Fistula:
- CONGENIIAL: Klipple lrenaurg $- ACQUIRED: Butcher's Thigh
E Aneurgsrn
E Burger diseaseE Pelvic lumors, PreAnancu
Pathologg I ncornpelent PerforatorsDilated superficial veins
Incornpeleni Perforafors, Dilaled supeilicialveins*ffi
Clinical piclure:
Sgtnplorns:
trtr Cosmelic dis{igurernenl, Sgmplorns of complicalions (pigmentafion, ltching, Ulcer)
Dull aching, sensalion of heaviness with sense of holness al ihe end of ihe dag or onprolonged slandin[PATIENI: Around 3O gearsPAtN,:[@
trtrtr PAIN IS RETIEVED BY:
(deeo veins are inlacll
E PAIN: r
tr PAIN Ig RETIEVED BY:}1 SWE[[!NG:
S'rgns: tr GElrlERAt:
- Signs of mesenchgmal weakness
tr IN$PECTIOIII:
- Multiple dilated tortous vein along long,short saphenous veins
; Blow oul al sile of perfioralor
- SKIN COMPLICAIIONS: tesstr PATPATIOIII:
- Ihrill on cough al incornpelent sapheno-
fernoral junclion- Dilaled, Elongaled, fodous, Soft,
Compressible lubules- EiliflftIs) Defect if felt in deep
fascia opposile lo BLOW OUI.tr PERCUSSIOII|:
dgs Ujlori,i',ri [o UrrUJs
tr gPECtAt StGrrtS:
- Localizaiion of incompelenl perforalor)TRENDTEilBERG IE8I, Multiple tourniqut
- DEEP 8YSTEM) Perthe's Tesl, Modi{iedPerlhe's fesl
tr GEIIIEMI:- Pulse, BP changes) AV fistula- Hearl examinalion) AV lislula
tr lilSPECIrOtrl:
P'lgmenlation, Derrnalilis, eczema,resielanl ulcer, Lipodermalosclercsis
tr PATPAIIOIII:
Sarne as lrg V.V. + ....tr AUSCUTIAIION:
- Machinerg murmur) AV ftstulatr gPECrAr SrGil8:
Sarne as lry V.V. + ....
EARLIEST SIGN OF CVIAnkle/Maleolar flare) Dilated sub-
dermal veins at the medial malleolus
wilh thin fra$le skin) BIUE BLEB

x,Rq-Tw.6 1aJlw*NvrRflw ? v tw0
lnvesligalions E DOPPLER, DUPLD(- R.eversa! of Blood llow wilh Vlasalvamaneuy$ ol Muscle squeeze
-Thrornbosis- Dilated Tortuous veins, lncompetenlvalves
tr INVESTIOATIONS FOR COMPTCIATIOIIIS:
-Plain X-mg) Varicose ulcer iPerioslills
I1 ARTERIOOMPHY (A-V Fistula)
PH}iAFYUNCOMPTICATED
& ASYMPIOMAIIC
CONgERVAIIVE
UNCOMPTICAIED
& DISFIGUREMENI
INJECTION
COMPTICATED
OR PAINFUT
SURGICAL
rTT. OF THE CAUSE
ON,EFS
tr IAUPUS EQUTNUS
E [L edema
Etr Posl-lraurnaticHemorrhage
tr EuperlicialThrombophlebitis
tr Pigmentalion,derrnaliiis, eczerna
E Varicose ulcertr Lipodermaiosclercsis
. Earlg,uncomplicated
. un{il for operalion
. Moderale cese
. C/O: Disligurcrnenl
. RedisualV.V. a#ter
r larte prirnarg W. Complicaled cases
R.e-assurance
m. Of PPI faclorsElasiic stocking
LL elevation
Warnins,vEilolotrllcS
lf Al! Perforators)
trEtr
Bruisee, discomfort , Pain
Nerve injurg (sensory, molor)Venous lhrornbosis
Cleanlinees, Rest, Limb elevalionCotisone, Znc 0xide
Earlg) Consenvalive ITT.
Recunenl) Cockel& Dodd Operation
If failed)Excision& flap

*+:f30{f, 6.m,FM XP#l ?AqY I H
DEFINITION: Disconlinuitg of epithelium resuliing in a 3D conicaldefecl in relalion fo high venous pressure on L.L.
ETIOLOGYAclivalion of the enlrapped WBCs in the
fortuous capillailes
Ftogrir ffldri
COMPLICATIONS:E lnfecfion, Hemorrhage, Osleomuelllis,
Perostitis, Marjolin ulcer
INVE$TIGAIION$:E For lhe cause: Doppler, Duplex
ffi sGgraArE Resl, elevation of limb
E Compression slockingstr Dressing with saline, anli-
septicstr Debridemenl
tr lF FAILED: Excision &Covering bg Cross leg
skin Flap
VAtr'CGE\EINSE Trendlenberg's Operation
tr SC Slripping
FOR, PREVENTION OF RECURRENCE:
E Conlinous usage of elaslicslockings
tr Leg elevalion
tr SITE: Gailer area fusl above the medial rnalleolus)tr 9lZE: Variable
tr NUMBER: Solitargtr EDGE: lrregular)Sloping, serraled) Punched oultr FLOOR: Granulation iissuetr BABE: lnduraledtr MARGIN: Plgmenlalion & dermalitistr LNS: Enlarged if there's secondarg infeclion


(sun, air, nuifuifion)
Anli-TB drugs
(lNH + Rifampicin *Streptomgcin )
s:* Failure of medical TT
* Biopsg
* Single accessible group of LNe
ldrNlegfions:* Multiple grcups (BLOOD BORNE)
* Bad general condilion
?AEV I W)
*Banalorial &MedicalTTI
tRepeateddressing wtthStreplorngcinPowder
*Excision
Banalorial &MedicalTTT
Aspiralion bgZ-lechnique*lnjection ofBlreptomgcin
OR
lncision wilhNo applicationof drains
tr GEI\IERALIZED AFFECTION:- Miliarg TB
- Pulmonary, rcnalIB
tr IOCAIZED AFFECTION:
Mediaetinal [NeMesenteric Utle
Pathologg tr Organism reaches LNs fhrcugh
tr Affectstr NO ...
Affectbn of capsule, Matfin!,Caseation, Cold abecess
ASecls
Affection of bapsule, Maftin!,Casealion, Cold abecess
tr ... perforates deep fascia
Clinical pic{ure
tr Manifeslalions of Pulmonarg IB..Dgspnea, Gcough, Epecforalion,
hemoplgeis
tr Affected Lftls:
Nol lender
tr IB foxemia, manifeslations of Pulmonarg TB
tr Affected Lltls:
- Enlarged.MtrI- Nol fender
tr Cold abscess) Flucluanl
tr Egslemic spread
tr Cold abscess, 8inus, l{OT COLD abscess (2rg infeclion)E hessu?e manifestaiionsE Caloilicalion
lnvesfigalions tr TABOMTORY:- Leuoopenia with relalive Lgmphocgtosis- f EgR>100
tr FOR tNS) Aspiralion, 8mear, Biopsg under O.A.
tr FOR PULMOITIARY IB) X-rag, fuberculin fesl, Sputum analgsis
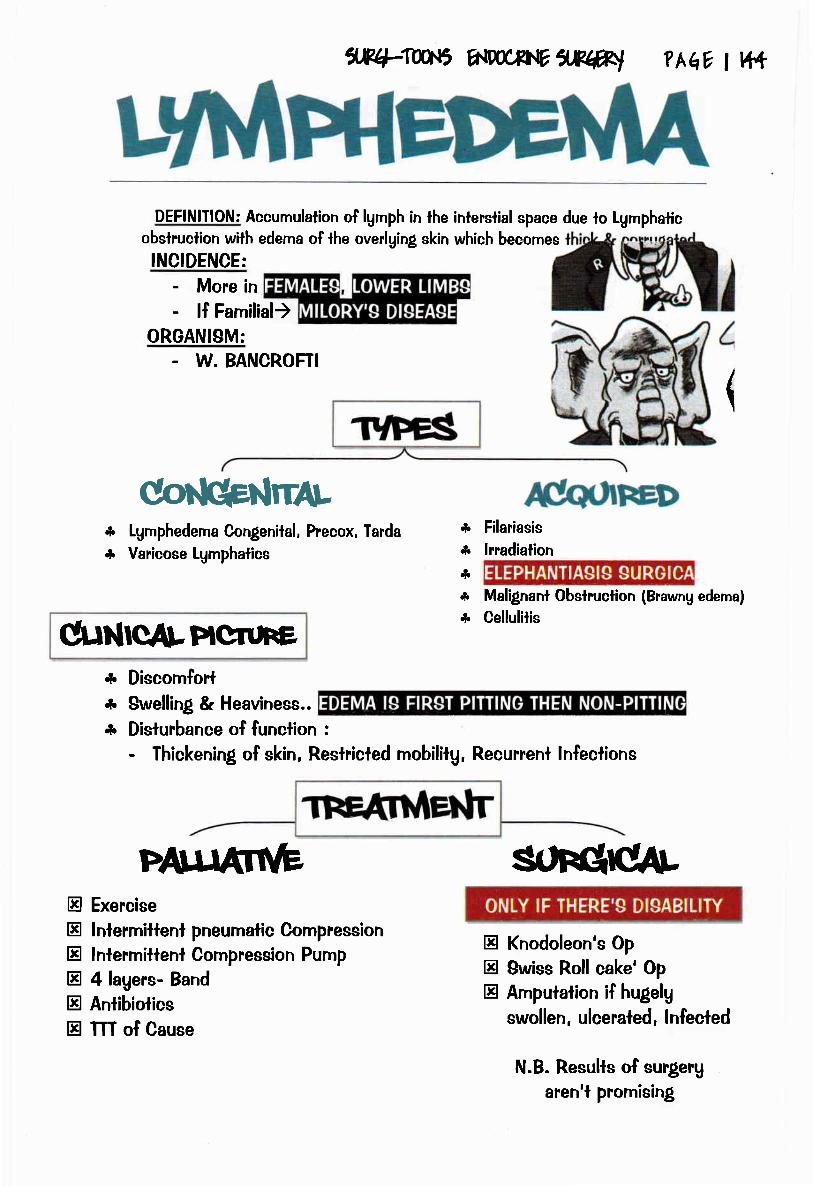
1*+4W'{r, A{W*IV7'.E#I ? hEY I vf1
DEFINITION: Accumulalion of lgmph in lhe interstial space due lo Lgmphaticobslruclion with edema of +he overlging skin which becomes
INCIDENCE:
- More in- !f Familial)
ORGANISM:. W. BANCROFTI
(
ffirrrrLLgmphedema Congenilal, Precox, Tarda
Varicose Lgmphatics
C TNCAtPICf,UFE* Discomforl* Swelling & Heaviness..
* Disturbance of function :
- Thickening of skin, Reslricled mobililg, Recurrent lnfeclions
Pffi soFqrcArEtr Exercise
E lnlermiftenl pneumalic CompressionE lntermitlenl Compression Pump
A 4lagers- Band
tr Anlibiolicstr TTT of Cause
***.f*
*t
Filariasis
lrradialion
Malignant Obslruclion (Brawng edema)
Cellulitis
Etr Knodoleon's Op
Etr $wiss Roll cake' Op
tr Ampulalion if hugelg
swollen, ulceraled, lnfecled
N.B. Results of surgeruaren't promising

tr gtage l) Enlarged I group of Lil. above or below diaphragm
tr Stage tl) Enlarged more > I group of LN. above or below
diaphragmtr Btage lll) Enlarged L[tl. above & below diaphragm
tr Sfage lV) Extra-nodal afleclion (liver & bone marrow)
? hEv I v15
tr Highlg rnalignanl B-celllumortr Eliologg : EBV, Malaria
Easlern Afiicatr Sile: t
E MicroscoDic Diclure:
,rco.6 a.|m,Phvilgw
Paihologg tr TYMPH NODEB:
- $lTE$: @[! llower deep ceMcal) Axillarg) Mediastinal LNs)
tr MACRO$COPIC PICIURE:
- Enlarged, discrete earlg) mafted laler- Rubberg- CUT SECTION: Pink homogenous with loss
of archileclure, lnlacl capsulegPtEEItl) Tofree Alrnond appearance
tr MICRO8COPIC PICIURE:. REED.SIERNBERG CETLB. PLEOMORPHISM
- loss of archilecfi.re
tr LYMPH NODES:
- 9ITEB: More ihan I group(MULTTCENTRTc)
tr MACROSCOPIC PICTUR,E:
- Earlg discrele) Amalgamated
Clinicalpicture
ACE& BD(: Adolescenl & middle age male
CONSIITUTIONAT SYMPIOMS:- Fever, llching, loss of weighf- Anernic rnanifeslalions.
SWEILING:
- 9lowlg progressive, rubbetg) mattedtr PAIN:
- Pain & itching (Affet alcohol inlake
"Gordon's leslo or lale afrer in{iliration)tr PRES8URE MANIFEEIAIIONS:
- Mediastinal L.Ns ) dgspnea, dgspha$a,
hoarseness & Horner's.
tr ABDOMINAT 8WELLINO:
- Splenornegalg, Para-aorlic 1.N., inleslina!Obslruclion & obslruclive
ACE& 8EX: Exlremes of age, Male
- As Hodgkin's bul more common
tr SWEILING:
- Rapidlg progressive,Hard) Amalgarnalion lafer
tr PAIN:
- Pain & itching (After alcohol
"Gordon'g tesl" or lale afterin{ihralion)
tr ABDOMINAL SWETLING:
lnvestigalion o For diagnosis ) excision biopsg if t.N. is involved.
o For D.D. & staging:a. CBC ( pancgrlopenia, & ESR > 100)
b. LFt (Obilirubin due lo obelruclive, HC or hemolgrtic)
c. KFf (t uric acid due lo lumor lgsis $)
d. CXR, Abdominal U/B & C.f., BM puncture.
e. Staging laparolorng is rarelg used (replaced bg SPIRAI CI Scan).
CHEMOTHERAPY
...(Multi-centric)...As Hodgkin's lgmphorna *...tN NODUTAR [YPE) Chlorambucil
IN DIFFUSE TYPE )Cgclophosphamide,
Vincilsline & hednisone.
frealmenl I. GENERAL IREATMENT:
Vrtamins, Blood lransfusion, lron lherapg
2. DEFINIIIVE IREAIMENI... according to siage...
- la, lb, lla) Radiother.apg
- Ilb) Radiotherapg + Chemotherapg- ll!, lV) Chemotherapg

oF HoDqKll.l Ln lH{otr/h
la,lb,llaRADIOTHERAPY
INFRA.DIAPHRAGMATIC
LNs
IINVERTED "Y"
THERAPY
IIbRADIOTHERAPY
( ACCoRDINq ro s:Ac,lhlc, )
ilE+:IW'{r, htm*tfiilP#l ?hq7 I W
gUPRA.
DIAPHRAGMATICLNs
tMANTLE
THERAPY
III, M
r)
2)3)4l
MuslineVincrisline "Oncovin"Pro-carbazine
Prednisolone in ld, 4ft
l) Cgclophosphamide(2-5) ... Vinuisfine, Pro-catbazine, Prednisolone ...
@
Vgg
Lowers Hgpercalcemia in late slagesRelieve itching
Raises lhe moodlmproves CBC, appetite
EI BiopsgEI Laparolomgg lnleslinal ObslructionM Jaundice
M SUPRA.DIAPHRAGMATIC M INFRA.DIAPHRAGMATIC
- Cervical- Mediasiinal- Axillarg
- Para-aoriic- Pelvic- lnguinal- Bplenic axis

X.E+:IW{r, A'.W;fN,VXf.#I
ARTERIAL SYSTEM. lnlermittent claudication Mag be an indication for bgpass surgerg if it
interfere which the palient normal life.. Sensorg loss mag be reversible after revascularization.. ln diabetic fool infeclion drainage through a small incision over lhe
pointing area is enough in most patient and debridement should beavoided especiallg in presence of good vascularizafion lo avoid excessive
bleeding.. The presence of osteomgelitis of small bones of the foot might be an
indicalion for ampulalion in Septic fool infection in diabeiics.. Allen lesl is done lo detecl Dominant blood supplg of the hand.
VENOUS SYSTEM. Acule severe deep venous lhrombosis can present bg the limb. A-Warm, swollen with tur$d calf muscles.r B- Cold, swollen wilh sever cganosis.. fhe main line of lreatmeni of lipodermatosclerosis is Cornpression elaslic
slockings.
LYMPHATIC SYSTEM. Hodgkin's disease can presenl wilh 2rg lgmphedema if the inguinal LNs
are involved.. Purilies is nol a marker of poor prognosis in Hodgkin's lgmphoma.. Werghl loss more than lO%in the Iasf six monlhs, Night sweals, and
Reed-gternberg cells in the bone marrow are markers of poor prognosis
in Hodgkin's lgmphoma

,4cntc isctlaflh2. Old aged paiient wifh positive hisiorg to D.M , smoking, or hgpertension,
dgslipidemia & alherosclerosis presenls wilh cramping pain cornes on walking&exercise ai {irsl with cerlain distance , relived bg stopping now lhe pain getworse and forces him to stop associated with cramping pain in abdomen in
relation to meals.
6ltmb ll rbclteuia dssutilttd lfffi pst +ba/ ailgrla,
Old aged patient with positive historg lo D.M, smoking, or hgperlension,dgslipidemia & alherosclerosis presenls with persistent resl pain, presence ofischemic ulcer or small gangrenous pafches.
Grfiical lmb bclwtrkYoung female presenls with bilateral pain and cganosis in tip of her fingersprecipitated bg exposure to cold or emolional slress. No irophic changes withinlacl peripheral pulsation.
Rqruns dbasa/ n7
Youn! male heavg smoker complaining of chronic ischemia in a Iimb
ilP+Imfi A.mcrhEwwl ? hqv t v+8
l. Palient wilh historg of mifra! slenosis&AF presenfs with sudden onset of severe
pain in his lower limb, toes cannol be
moved, complele loss of sensalion, pallor
and pnogressive coldness of the limb.O/E absent peripheral pulsation. No pasl historg lo claudication pain.
3.
4.
Brgr s dbwa6. 7- Uoung female complaining of tingling and numbness along the ulnar side of
lhe hand and forearm with weakness of small muscles of the hand also
claudicalion pain in upper limb with exercise.
Tltwanb atlet sytdrulla
7. Middle aged male or female presenls wiih slowlg growing swelling adjacenl lothe hgoid bone, anterior lo slernomasloid, compressible, pulsalile, moves from
side to side not verlical.
GarotilMl fuma ( clte,nfutwttd.
8. Old age palienl with posilive hislorg to afherosclerosis or sgphilis presents with
cgslic compressible swelling a cross of arlerg, gives expansile pulsafion.
*fer,,U ailqolstt/

1e,q*Twt5 ww/J.t71Rqw ?hqvtw
ioNaa
,
DW " PDFs , C/P, lnvesligations, Fale & cornplicaiions"(Kasn 2@Z 2W- Au shams, 2@5,2d/-
Azlur f,2@Z 2@4,2M-Azhar rl/, 2ob, 2M, 2mL/)
Acute ischernia(Kasn 2M. 2d/- Au sl/afils, 2@2, 2M, 2M -
Ay'rar f,2@6,2M- ,4y'tar ril, Zd, ZWSManifeslalions, Cornplicalions and TTT. of varicose veins
6i/ siafils,2W - Ay'rar f,2@5,2@4 -,42/rar ril, 2oh, 2@Z 2@/)
r Diagnosis & fTT. chronic ischernia
r Chronic Venous insufficiencg
r Eiio-pathologg of lgrnphederna
Uh sfiart/s, 2@5,2fu)
( Ailar f,2@7)
( Kasn 2d/ )

5JP4-T0UI5 ww,Btrtv 5ll?q%l I t60
ilao


















