Massive Intrathoracic Malignant Peripheral Nerve Sheath Tumor with Tracheobronchial Obstruction...
19
Massive Intrathoracic Malignant Peripheral Nerve Sheath Tumor with Tracheobronchial Obstruction Bryan Barnosky, DO; and ArunabhTalwar MD. North Shore University Hospital, Manhasset, NY. Division of Pulmonary and Critical Care Medicine.
-
Upload
diana-hood -
Category
Documents
-
view
216 -
download
2
Transcript of Massive Intrathoracic Malignant Peripheral Nerve Sheath Tumor with Tracheobronchial Obstruction...

Massive Intrathoracic Malignant Peripheral Nerve Sheath Tumor
with Tracheobronchial Obstruction
Bryan Barnosky, DO; and ArunabhTalwar MD.
North Shore University Hospital, Manhasset, NY.
Division of Pulmonary and Critical Care Medicine.
Case Presentation
• 23 year old male with progressive dyspnea for approximately one month.
• Subjective fever, sore throat, and a non-productve cough.
• Right sided chest pain, night sweats, and a 10 – 15 lb. unintentional weight loss.
• No significant medical or surgical history.• Non-smoker.
Case Presentation
• Vital signs: T 36.3, HR 100, RR26, BP 132/67, and SaO2 96% on room air.
• Mild respiratory distress at rest.
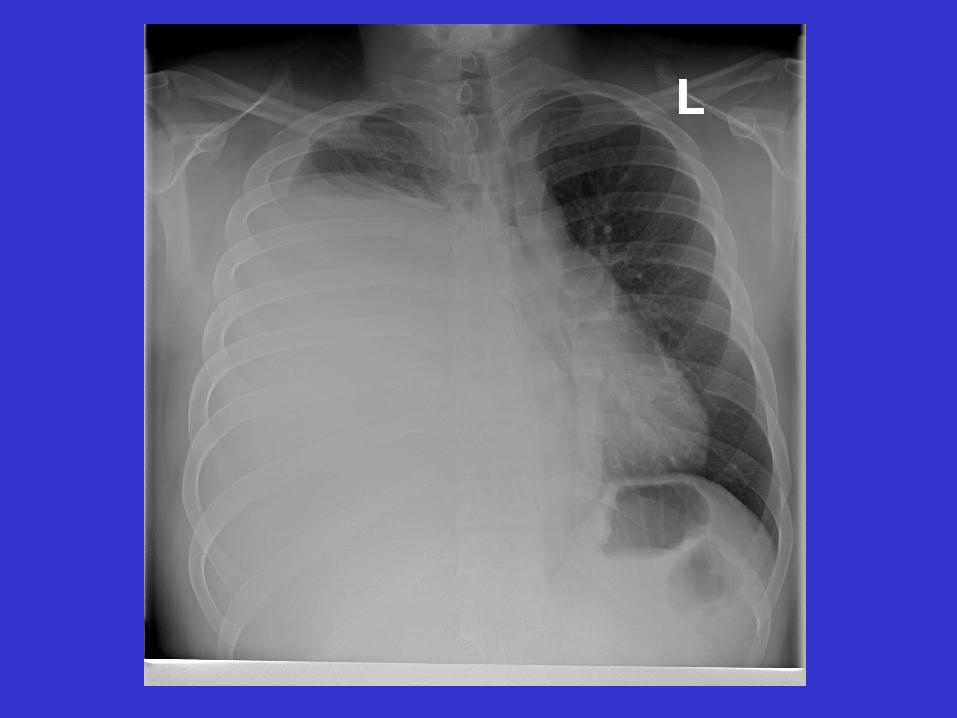
• Physical examination revealed markedly diminished breath sounds over the right hemithorax and tenderness to palpation of the right lateral chest wall.
Laboratory Data
• WBC 9700
• Hgb 12.9
• Hct 38.7
• Platlets 387000
• PT 14.4
• INR 1.27
• PTT 26.7
• ESR 77
• LDH 1092
• Na 136
• K 3.4
• Cl 104
• CO2 26
• BUN 4
• Cr 0.7
• AST 44
• ALT 15
• Alk Phos 77



Hospital Course
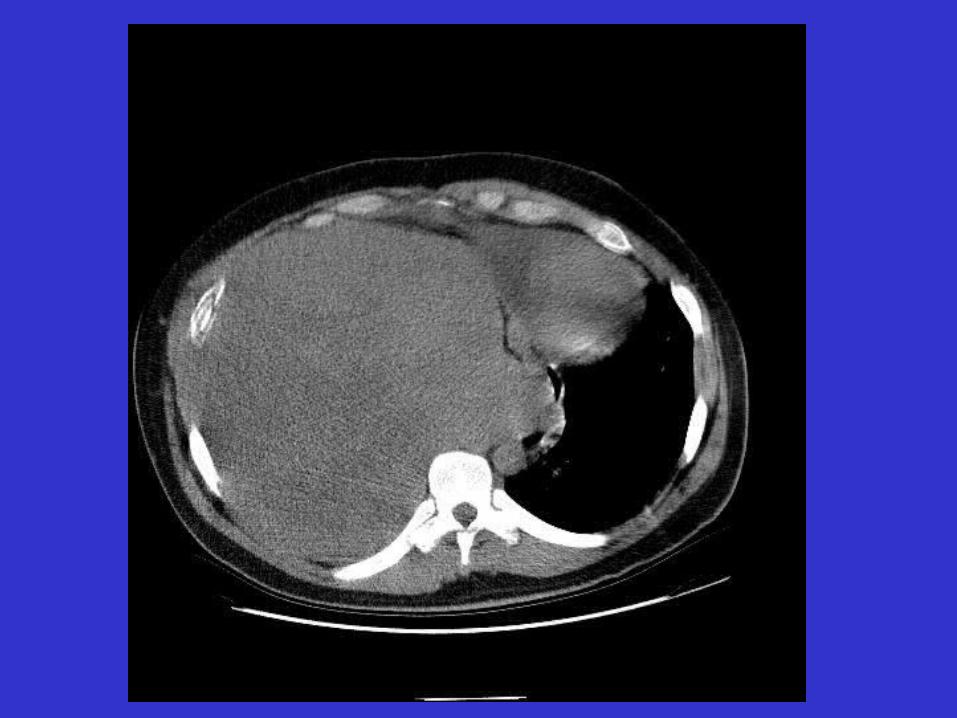
• The patient’s respiratory status progressively worsened and he was taken to surgery for exploration and biopsy.
• The mass was deemed unresectable and post-operatively the patient remained on the ventilator.
• Subsequent weaning trials were unsuccessful and the patient underwent bronchoscopy to evaluate the utility of endobronchial stenting.

Bronchoscopy
• Extrinsic compression of the distal trachea and right mainstem bronchus with resultant collapse of the the right middle and lower lobes.
• Extrinsic compression of the left mainstem bronchus at the carina and extending approximately 1.5cm distally.

Bronchoscopy
• The left mainstem bronchus was dilated to 13.5mm via balloon.
• Under fluoroscopic guidance an Ultraflex distal release, covered stent was placed.
• Post-procedure the left mainstem bronchus and all distal segments were completely patent.
Hospital Course
• The patient was weaned from the ventilator the following day.
• The final pathological diagnosis was malignant peripheral nerve sheath tumor.
• The patient was then transferred to another facility for the initiation of chemotherapy.
• Shortly thereafter the patient’s condition rapidly deteriorated and he expired.
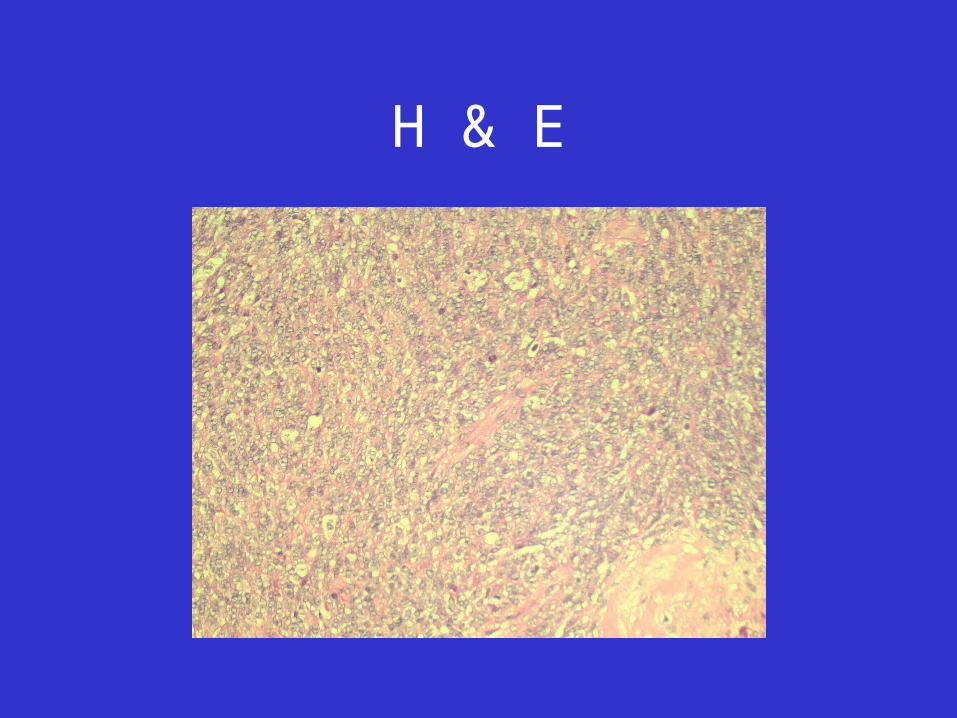
H & E

S-100

Thoracic Neurogenic Tumors
• Neurogenic tumors of the thorax can arise from any tissue of the neural crest (peripheral, autonomic, or paraganglionic nervous systems).
• Most commonly found in the costovertebral sulcus arising from the sympathetic chain or one of the rami of the intercostal nerves.
• These tumors are most often asymptomatic although infrequently dyspnea, cough, or other respiratory symptoms may be noted.
• In adults, the malignancy rate of neurogenic tumors is less than 10% (and probably only 1 to 2%).
Malignant Peripheral Nerve Sheath Tumors
• Spindle cell sarcoma arising from a nerve, neurofibroma, or demonstrating nerve tissue differentiation.
• Previously referred to as malignant schwannoma, neurogenic sarcoma, and neurofibrosarcoma.
• Estimated frequency in the general population is 0.001% compared with 2 to 5% in patients with Neurofibromatosis type I.
Malignant Peripheral Nerve Sheath Tumors
• Histological analysis reveals unencapsulated infiltrating tumors composed of spindle cells arranged in a sweeping fascicles with densely cellular areas alternating with less cellular ones.
• Mitotic figures are readily visible and 50-90% of cases are immunoreactive with S-100 protein staining.
• Highly malignant, locally invasive and with a high likelihood of producing local recurrence and distant metastasis.
• Surgical resection with postoperative radiation and/or chemotherapy is the usual mode of treatment.

Indications For Endobronchial Stents
• Intrinsic airway obstruction from benign or malignant diseases.
• Extrinsic stenosis of central airways from benign or malignant diseases.
• Sealing of airway fistulas.• Tracheobronchial malacia. • Complex, inoperable tracheobrochial
strictures.
CONCLUSION
• Although relatively rare, malignant peripheral nerve sheath tumors must be included in the differential diagnosis of a massive intrathoracic mass.
• While ultimately not improving outcome, we believe that the endobronchial stenting procedure performed in this case did facilitate weaning from the ventilator which improved our patient’s quality of life.