Massive Hemorrhage in Facial Fracture Patients
11
PEDIATRIC/CRANIOFACIAL Massive Hemorrhage in Facial Fracture Patients: Definition, Incidence, and Management Nicola R. Dean, Ph.D., F.R.A.C.S.(Plas.) James P. Ledgard, M.B.B.S. James Katsaros, M.B.B.S., F.R.A.C.S.(Plas.) Adelaide, Australia Background: Significant hemorrhage from fractures of the midface is a recog- nized phenomenon, but because it is an uncommon occurrence, there is little in the literature to guide management of these patients. Methods: The authors performed a retrospective study of life-threatening hem- orrhage in facial fracture patients attending the Royal Adelaide Hospital over 20 years and report four recent cases. Results: The incidence of massive hemorrhage was found to be 0.33 percent of patients with fracture of the midface or skull base over the 20 years before 2004 and 1.7 percent in the subsequent year. Of the 19 patients identified from case notes and recent experience, seven died. In terms of management of hemor- rhage, three patients had packing alone, 10 had balloon catheters inserted, and five had ligation of a vessel. Most patients had multiple other injuries, including six patients with head injuries. The mean number of units of packed red cells transfused was 9.5 (median, 7.5). In five of the cases identified, there was a delay in recognizing that facial fractures were the major source of hemorrhage. Conclusions: Massive hemorrhage from facial fractures is an underrecognized and inconsistently managed phenomenon. Although low in incidence, its timely recognition and better management may reduce the high mortality rate in this group of patients. (Plast. Reconstr. Surg. 123: 680, 2009.) H emorrhage from facial fractures can threaten life by causing hypovolemic shock or by contributing to airway obstruction. Few studies have described the incidence of this phenomenon. 1–4 It is not mentioned in the Ad- vanced Trauma Life Support handbook, 5 and hence specific management of severe bleeding from facial fractures is not routinely taught. This study was initiated after the death of a patient from massive hemorrhage from facial fractures. Its aim was to determine the incidence of this condition and analyze its management and outcomes. The Royal Adelaide Hospital treats approximately 60,000 inpatients and 200,000 outpatients per year and treats between 100 and 150 patients with skull or facial fractures per year. This article reports the results of a 20-year retrospective study and outlines the four cases that occurred in the following year. PATIENTS AND METHODS To accurately measure the incidence of a con- dition, that condition must first be well defined. As there is no established definition of massive hem- orrhage from facial fracture, we devised a defini- tion as follows: Fracture of the midface or skull base plus hemor- rhage into pharynx • Causing tachycardia (pulse rate 100) and hy- potension (systolic pressure 100) with no other cause identified, or From the Flinders Medical Center, Flinders University; and Royal Adelaide Hospital. Received for publication April 15, 2008; accepted August 4, 2008. Presented at the Royal Australasian College of Surgeons Annual Trainees Conference, in Wellington, New Zealand, 2005, and awarded best clinical paper prize. Copyright ©2009 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e31819565da Disclosure: None of the authors has any commer- cial association with any products described in this article and has no financial conflicts of interest. This research was not formally funded. It was ini- tiated by the corresponding author while she was a trainee and all authors have performed the research either in spare time or during time employed at the Royal Adelaide Hospital (a public sector hospital). www.PRSJournal.com 680
-
Upload
macarena-miranda -
Category
Documents
-
view
214 -
download
0
description
Massive Hemorrhage in Facial Fracture Patients: Definition, Incidence, and Management Background: Significant hemorrhage from fractures of the midface is a recognized phenomenon, but because it is an uncommon occurrence, there is little in the literature to guide management of these patients.
Transcript of Massive Hemorrhage in Facial Fracture Patients

PEDIATRIC/CRANIOFACIAL
Massive Hemorrhage in Facial FracturePatients: Definition, Incidence,and Management
Nicola R. Dean, Ph.D.,F.R.A.C.S.(Plas.)
James P. Ledgard, M.B.B.S.James Katsaros, M.B.B.S.,
F.R.A.C.S.(Plas.)
Adelaide, Australia
Background: Significant hemorrhage from fractures of the midface is a recog-nized phenomenon, but because it is an uncommon occurrence, there is littlein the literature to guide management of these patients.Methods: The authors performed a retrospective study of life-threatening hem-orrhage in facial fracture patients attending the Royal Adelaide Hospital over20 years and report four recent cases.Results: The incidence of massive hemorrhage was found to be 0.33 percent ofpatients with fracture of the midface or skull base over the 20 years before 2004and 1.7 percent in the subsequent year. Of the 19 patients identified from casenotes and recent experience, seven died. In terms of management of hemor-rhage, three patients had packing alone, 10 had balloon catheters inserted, andfive had ligation of a vessel. Most patients had multiple other injuries, includingsix patients with head injuries. The mean number of units of packed red cellstransfused was 9.5 (median, 7.5). In five of the cases identified, there was a delayin recognizing that facial fractures were the major source of hemorrhage.Conclusions: Massive hemorrhage from facial fractures is an underrecognizedand inconsistently managed phenomenon. Although low in incidence, its timelyrecognition and better management may reduce the high mortality rate in thisgroup of patients. (Plast. Reconstr. Surg. 123: 680, 2009.)
Hemorrhage from facial fractures canthreaten life by causing hypovolemic shockor by contributing to airway obstruction.
Few studies have described the incidence of thisphenomenon.1–4 It is not mentioned in the Ad-vanced Trauma Life Support handbook,5 andhence specific management of severe bleedingfrom facial fractures is not routinely taught. Thisstudy was initiated after the death of a patient frommassive hemorrhage from facial fractures. Its aimwas to determine the incidence of this conditionand analyze its management and outcomes. TheRoyal Adelaide Hospital treats approximately60,000 inpatients and 200,000 outpatients per yearand treats between 100 and 150 patients with skullor facial fractures per year. This article reports the
results of a 20-year retrospective study and outlinesthe four cases that occurred in the following year.
PATIENTS AND METHODSTo accurately measure the incidence of a con-
dition, that condition must first be well defined. Asthere is no established definition of massive hem-orrhage from facial fracture, we devised a defini-tion as follows:
Fracture of the midface or skull base plus hemor-rhage into pharynx• Causing tachycardia (pulse rate �100) and hy-
potension (systolic pressure �100) with noother cause identified, or
From the Flinders Medical Center, Flinders University; andRoyal Adelaide Hospital.Received for publication April 15, 2008; accepted August 4,2008.Presented at the Royal Australasian College of SurgeonsAnnual Trainees Conference, in Wellington, New Zealand,2005, and awarded best clinical paper prize.Copyright ©2009 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31819565da
Disclosure: None of the authors has any commer-cial association with any products described in thisarticle and has no financial conflicts of interest.This research was not formally funded. It was ini-tiated by the corresponding author while she was atrainee and all authors have performed the researcheither in spare time or during time employed at theRoyal Adelaide Hospital (a public sector hospital).
www.PRSJournal.com680

• Necessitating acute transfusion with two ormore units of packed red cells, or
• Where blood loss from that source was mea-sured as greater than 500 ml.
The Australian health care system has a uni-fied discharge coding system containing codes forboth diagnoses and procedures.6 The dischargecoding data system was used to identify all thosepatients who, over a 20-year period (January 1,1984, to December 31, 2003), had been dis-charged with diagnosis codes for malar bone, max-illary, or skull base fractures (mandible fractureswere not included in the population). This patientlist was then cross-referenced with the names ofthose discharged with a diagnosis code of epistaxisor procedure codes of arrest of hemorrhage, nasalpacking, or blood transfusion. The resultant list ofpatients was then used as the base population forstudy. The medical records of these patients wereexamined for criteria for massive hemorrhagefrom facial fracture as defined above. If the criteriawere met, the patient was designated as a “case”and the medical records were further examinedfor the following details: presentation, includingage and sex, mechanism of injury, fracture pat-tern, concurrent injuries, and blood pressure andpulse; and management, including airway man-agement, arrest of hemorrhage, and volume ofblood products given. Any apparent delay in man-agement of the facial fracture hemorrhage andthe outcome of the patients were also noted. Datawere recorded and analyzed and an incidence ofmassive hemorrhage from facial fractures was cal-culated. A further 50 sets of case notes were ran-domly selected from the population of facial frac-ture patients to assess the rate of false negatives(patients recorded as a noncase when they were infact a case). In addition, the hospital “miscode”rate was also examined as a potential source oferror.
In addition to the retrospective study, the de-tails of any new cases of massive hemorrhage infacial fractures were documented over an addi-tional 1-year period. The incidence of cases wascalculated for both the 20-year period and thesubsequent 1-year period. The clinical presenta-tion, management, and outcome data of caseswere analyzed as a whole, with those of the retro-spective cases being combined with those of therecent cases. The results were tabulated for com-parison of case features (Table 1). Individual datafor incidence and mortality, clinical presentation,and management of hemorrhage are presented inthe Results.
CASE REPORTS
Case 1Case 1 involved a 62-year-old male driver in a head-on motor
vehicle accident who had significant facial trauma and wastrapped in his vehicle for more than 1 hour by intrusion ofmetalwork into the driver’s compartment. He was intubatedbecause of massive facial bleeding. No past medical history wasavailable, but he was noted to have a median sternotomy scar.He had had one cardiac arrest before referral to the plasticsurgery team and had another cardiac arrest on the way to theoperating room to stop the facial fracture hemorrhage. Hereceived 15 units of packed red cells but died on the operatingtable from continuing hemorrhage and cardiovascular decom-pensation, despite attempts at balloon tamponade of his frac-tures. It was later found that he had been taking anticoagulantsfollowing coronary artery bypass surgery. His death was re-ported to the coroner but no postmortem examination wasperformed. No facial radiographs or computed tomographyscans were performed due to his hemodynamic instability. Theoperating surgeon had noted that on clinical examination hehad a Le Fort I–type fracture and a sagittal split of his hardpalate.
Case 2Case 2 was that of a 25-year-old male driver who had collided
with a concrete post. His car turned over and he was trappedupside down in his vehicle. He sustained complex Le Fort facialfractures plus a sagittal split of his hard palate, as well as bilateralcondyle fracture dislocations and a parasymphyseal mandiblefracture (Fig. 1). He was intubated in the resuscitation roomand immediately transferred to the operating room. Foley cath-eters were inserted and the balloons were inflated in the phar-ynx. Moderate traction was placed on the catheters and thenmaintained by means of an umbilical cord clamp (Fig. 2). Theoral cavity and remainder of the pharynx were then packed withgauze. These procedures arrested the hemorrhage and thepatient went on to have the remainder of his trauma survey. Herequired transfusion with 9 units of packed red cells. His non-facial injuries were a small subdural hematoma and fracturedribs. He proceeded to have a tracheostomy and plate fixationof his panfacial fractures without further complication andmade a good recovery, returning to full employment (Fig. 3).
Case 3Case 3 was that of a 78-year-old male driver involved in a
head-on collision who was trapped in his car by intruding met-alwork and bleeding from his face. He also had major lowerlimb injuries. He had continuing hypotension after splinting ofhis lower limbs, and a fast scan of his abdomen was negative.Nasopharyngeal balloon catheters had been inserted but hecontinued to bleed from his face and had a clinically obviousLe Fort I fracture. He was taken to the operating room forligation of his external carotid hemorrhage (Fig. 4). Ligation ofthe external carotid on the left side only reduced his facialbleeding, but he was then found to have an avulsed internalmammary artery that was bleeding into his thoracic cavity. Thiswas embolized radiologically and he became hemodynamicallystable. He received 45 units of packed red blood cells in totaland had a long course of treatment in intensive care. Fixationof his Le Fort fracture was straightforward. He was eventuallydischarged from the hospital to a rehabilitation center and thenhome, where he returned to good function.
Volume 123, Number 2 • Massive Hemorrhage in Facial Fracture
681

Table 1. Summary of Cases
Management of Bleeding
Case DescriptionMechanism
(categorized)Airway
Management Description Categorized
1 64-yr-old man in head-on collision trapped incar by face; taking anticoagulants; cardiacarrest before arrival; died on operatingtable attempting to arrest facialhemorrhage
Automobile accident Emergency intubation Nasal packing and ballooncatheters
Balloon catheters but novessel ligation �/�packing
2 25-yr-old man in motor vehicle accident;trapped in vehicle upside down; airway fullof blood; two unsuccessful attempts atintubation at scene
Automobile accident Emergency intubation Balloon catheter and nasalpacking
Balloon catheters but novessel ligation �/�packing
3 78-yr-old man in motor vehicle accident;during arrest of hemorrhage from facialfractures still unstable; had avulsedinternal mammary artery; blood in thorax
Automobile accident Emergency intubation Nasal packing and ballooncatheters then externalcarotid ligation
Ligation of vessel �/�other measures
4 37-yr-old man on motorbike vs. car Motorcycle accident Emergency intubation Balloon catheter andpacking
Balloon catheters but novessel ligation �/�packing
5 69-yr-old pedestrian hit by car; facialfractures and skull base fractures, tibialfracture, hemopneumothorax, subdural;underwent negative laparotomy after dropin BP
Pedestrian struck byautomobile
Emergency intubation Packing of anterior andposterior nasal spacethen oropharynxpacked
Packing only
6 54-yr-old male front-seat passenger in carthat collided with rear end of truck
Automobile accident Emergency intubation Foley catheters plus gauzepacking
Balloon catheters but novessel ligation �/�packing
7 21-yr-old female pedestrian hit by car;profuse bleeding from nose and mouthrequiringd intubation and 7-unittransfusion
Automobile accident Emergency intubation Foley catheters and nasalpacking
Balloon catheters but novessel ligation �/�packing
8 28-yr-old man cycling home from pub hit bycar; agitated, with significant bleedingfrom nose; transferred from rural townshocked (systolic BP of 70); 1100 ml ofblood aspirated from NG tube
Bicycle accident Emergency intubation Brighton tubes and nasalpacking
Balloon catheters but novessel ligation �/�packing
9 19-yr-old in motor vehicle accident with LeFort I plus II plus open fracture ofmandible and head injury; arrived at 0030hr from peripheral hospital; Hb droppedfrom 100 to 60 g/liter by 0330 hr fromcontinuous bleed from mouth; by 0430 Hbhad dropped to 42 g/liter; nose andmouth packed; facial wounds sutured;external carotid explored but not ligated;at 1000 hr left external carotid ligated
Automobile accident Emergency intubation Nasal packing and ligationof external carotid
Ligation of vessel �/�other measures
10 18-yr-old in motor vehicle accident; drivernot wearing seatbelt; car vs. tree; panfacialfractures
Automobile accident Emergencytracheostomy
Foley catheters and nasalpacking
Balloon catheters but novessel ligation �/�packing
11 24-yr-old man on motorbike in head-oncollision with car; found in middle of roadin large pool of blood
Motorcycle accident Emergency intubation Throat and nasal packing;taken to OR fortracheostomy andinsertion of ballooncatheters and packing
Balloon catheters but novessel ligation �/�packing
12 83-yr-old man fell down 3 steps Fall No acute intubation Nasal packing withparaffin gauze
Packing only
13 48-yr-old woman shot in face Gunshot wound Emergency intubation Taken to OR for packingand ligation of maxillaryartery
Ligation of vessel �/�other measures
14 62-yr-old man fell from a bicycle while ridingdownhill
Bicycle accident Emergency intubation Nasal packing and Foleycatheters
Balloon catheters but novessel ligation �/�packing
15 26-yr-old male assault victim attendedemergency with epistaxis; had nasalpacking and Foley catheters, then anteriorethmoidal artery ligation
Assault No acute intubation Foley catheters and nasalpacking, then anteriorethmoidal arteryligation
Ligation of vessel �/�other measures
16 63-yr-old backseat passenger in motor vehicleaccident
Automobile accident Emergency intubation Not documented Not known
17 78-yr-old pedestrian hit by car; “blood inairway” at scene and hemodynamic statedeteriorated; underwent negativelaparotomy; died
Pedestrian struck byautomobile
Emergency intubation Nasal packing Packing only
18 75-yr-old man clubbed around face in homeinvasion and shot in groin/abdomen
Assault No acute intubation Foley catheters and nasalpacking
Balloon catheters but novessel ligation �/�packing
19 41-yr-old male assault victim Assault No acute intubation Foley catheter and nasalpacking with kaltostat,then anterior ethmoidalartery ligation
Ligation of vessel �/�other measures
BP, blood pressure; Hb, hemoglobin; NG, nasogastric; OR, operating room; MI, myocardial infarction; PMH, past medial history; COAD,chronic obstructive airways disease.
Plastic and Reconstructive Surgery • February 2009
682
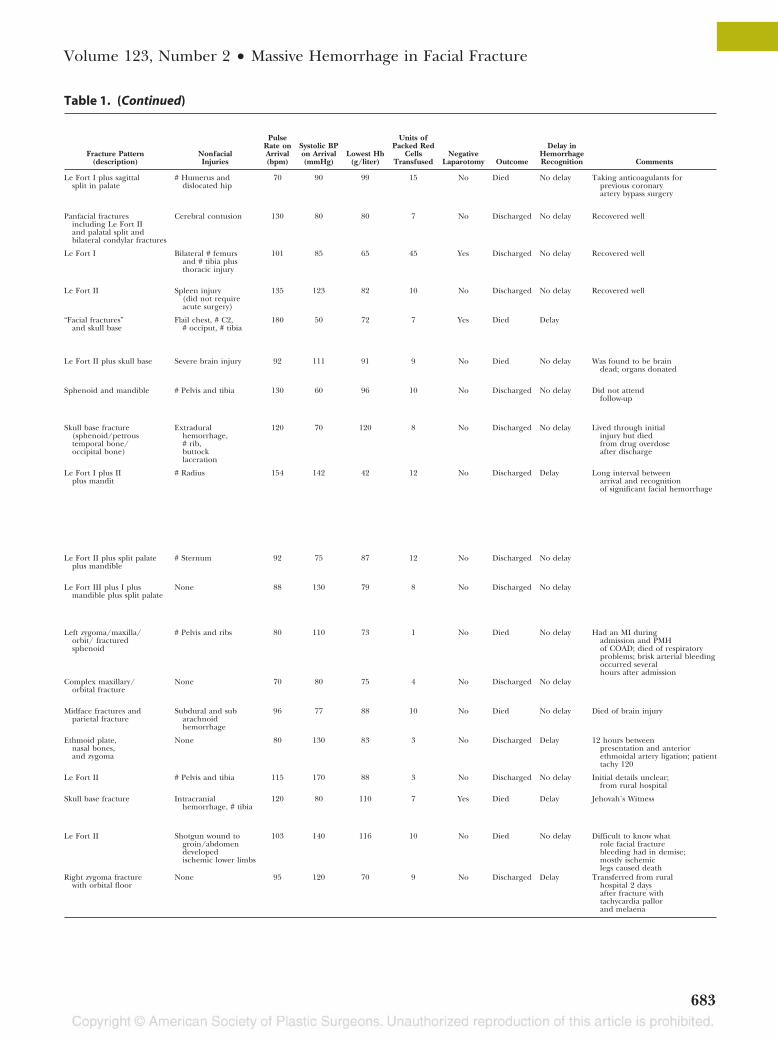
Table 1. (Continued)
Fracture Pattern(description)
NonfacialInjuries
PulseRate onArrival(bpm)
Systolic BPon Arrival(mmHg)
Lowest Hb(g/liter)
Units ofPacked Red
CellsTransfused
NegativeLaparotomy Outcome
Delay inHemorrhageRecognition Comments
Le Fort I plus sagittalsplit in palate
# Humerus anddislocated hip
70 90 99 15 No Died No delay Taking anticoagulants forprevious coronaryartery bypass surgery
Panfacial fracturesincluding Le Fort IIand palatal split andbilateral condylar fractures
Cerebral contusion 130 80 80 7 No Discharged No delay Recovered well
Le Fort I Bilateral # femursand # tibia plusthoracic injury
101 85 65 45 Yes Discharged No delay Recovered well
Le Fort II Spleen injury(did not requireacute surgery)
135 123 82 10 No Discharged No delay Recovered well
“Facial fractures”and skull base
Flail chest, # C2,# occiput, # tibia
180 50 72 7 Yes Died Delay
Le Fort II plus skull base Severe brain injury 92 111 91 9 No Died No delay Was found to be braindead; organs donated
Sphenoid and mandible # Pelvis and tibia 130 60 96 10 No Discharged No delay Did not attendfollow-up
Skull base fracture(sphenoid/petroustemporal bone/occipital bone)
Extraduralhemorrhage,# rib,buttocklaceration
120 70 120 8 No Discharged No delay Lived through initialinjury but diedfrom drug overdoseafter discharge
Le Fort I plus IIplus mandit
# Radius 154 142 42 12 No Discharged Delay Long interval betweenarrival and recognitionof significant facial hemorrhage
Le Fort II plus split palateplus mandible
# Sternum 92 75 87 12 No Discharged No delay
Le Fort III plus I plusmandible plus split palate
None 88 130 79 8 No Discharged No delay
Left zygoma/maxilla/orbit/ fracturedsphenoid
# Pelvis and ribs 80 110 73 1 No Died No delay Had an MI duringadmission and PMHof COAD; died of respiratoryproblems; brisk arterial bleedingoccurred severalhours after admission
Complex maxillary/orbital fracture
None 70 80 75 4 No Discharged No delay
Midface fractures andparietal fracture
Subdural and subarachnoidhemorrhage
96 77 88 10 No Died No delay Died of brain injury
Ethmoid plate,nasal bones,and zygoma
None 80 130 83 3 No Discharged Delay 12 hours betweenpresentation and anteriorethmoidal artery ligation; patienttachy 120
Le Fort II # Pelvis and tibia 115 170 88 3 No Discharged No delay Initial details unclear;from rural hospital
Skull base fracture Intracranialhemorrhage, # tibia
120 80 110 7 Yes Died Delay Jehovah’s Witness
Le Fort II Shotgun wound togroin/abdomendevelopedischemic lower limbs
103 140 116 10 No Died No delay Difficult to know whatrole facial fracturebleeding had in demise;mostly ischemiclegs caused death
Right zygoma fracturewith orbital floor
None 95 120 70 9 No Discharged Delay Transferred from ruralhospital 2 daysafter fracture withtachycardia pallorand melaena
Volume 123, Number 2 • Massive Hemorrhage in Facial Fracture
683
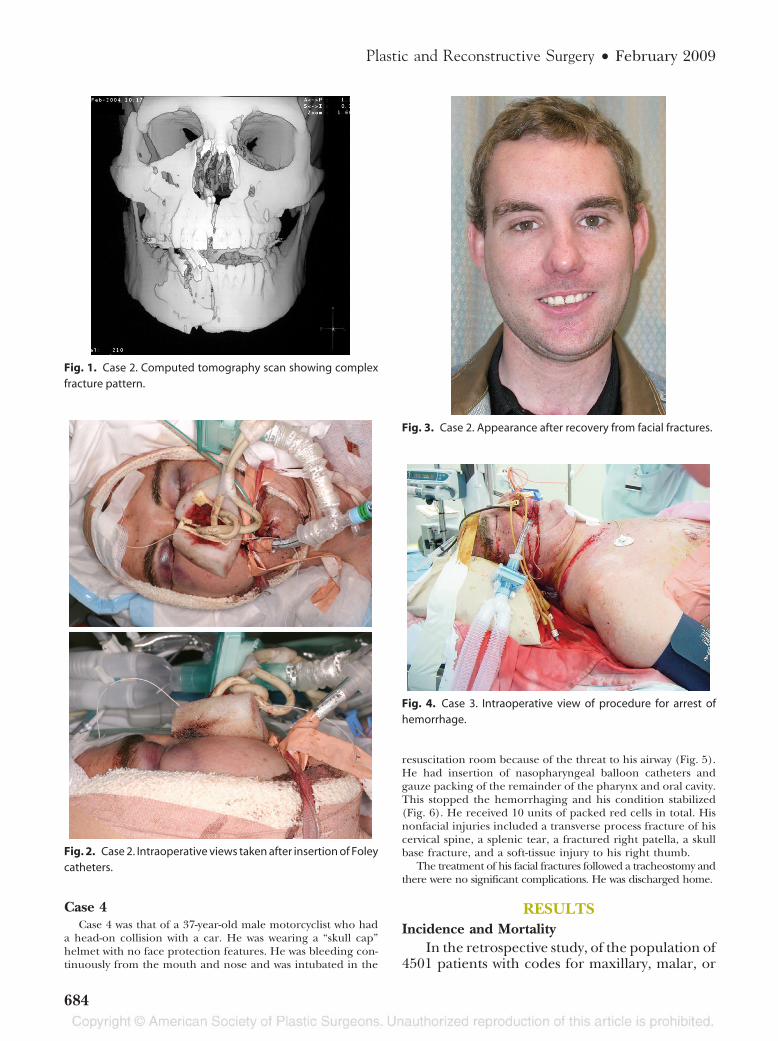
Case 4Case 4 was that of a 37-year-old male motorcyclist who had
a head-on collision with a car. He was wearing a “skull cap”helmet with no face protection features. He was bleeding con-tinuously from the mouth and nose and was intubated in the
resuscitation room because of the threat to his airway (Fig. 5).He had insertion of nasopharyngeal balloon catheters andgauze packing of the remainder of the pharynx and oral cavity.This stopped the hemorrhaging and his condition stabilized(Fig. 6). He received 10 units of packed red cells in total. Hisnonfacial injuries included a transverse process fracture of hiscervical spine, a splenic tear, a fractured right patella, a skullbase fracture, and a soft-tissue injury to his right thumb.
The treatment of his facial fractures followed a tracheostomy andthere were no significant complications. He was discharged home.
RESULTSIncidence and Mortality
In the retrospective study, of the population of4501 patients with codes for maxillary, malar, or
Fig. 1. Case 2. Computed tomography scan showing complexfracture pattern.
Fig. 2. Case 2. Intraoperative views taken after insertion of Foleycatheters.
Fig. 3. Case 2. Appearance after recovery from facial fractures.
Fig. 4. Case 3. Intraoperative view of procedure for arrest ofhemorrhage.
Plastic and Reconstructive Surgery • February 2009
684

skull base fractures, 18 had a code for epistaxis, 29had a code for transfusion, and 16 had a code fornasal packing or control of epistaxis. In total therewere 50 patients with codes for both facial frac-tures and at least one of the codes indicating
bleeding. On review of the medical records, 15 ofthese patients met the constructed definition ofmassive hemorrhage from facial fractures. An ad-ditional four cases occurred during the study pe-riod, yielding a total of 19 cases. The hospitalmiscode rate (i.e., the proportion of patient epi-sodes that were given an incorrect code) wasfound to be nonsignificant (1.2 percent) at theannual audit of the hospital coders.7 Of the 50randomly selected case notes, there were no casesthat met the criteria for massive hemorrhage fromfacial fractures (i.e., no false negatives). The in-cidence of massive hemorrhage in malar, maxil-lary, or skull base fractures in the 20-year periodwas 0.33 percent. The incidence in the 1-year pe-riod during the study was 1.77 percent (four pa-tients of 226 with midface or skull base fractures).In the combined data set, seven of the 19 patientsdied during the hospital admission in which theyhad the facial fractures. In many cases, cause ofdeath was difficult to attribute to one pathologyalone since those who died all had multiple inju-ries.
Clinical PresentationIn most cases, the patients were male; the me-
dian age was 48 years (range, 18 to 83 years) (Ta-ble 1). The causes of injury varied, with the mostcommon being motor vehicle accident. Most pa-tients had other injuries besides the facial fracture,including significant head injuries. Crude data forhemodynamic status–-systolic blood pressure(mean, 101 mmHg) and pulse (mean, 108 bpm)–-indicated that most patients had significant hypo-volemia on presentation. Descriptions of facialfracture patterns in the case notes and radiologyreports were heterogeneous and in some cases noteasily classified. Five patients were described ashaving skull base fractures or Le Fort III fractures,with an additional three patients reported as hav-ing fractures of individual bones of the skull base(sphenoids or ethmoids). Four of these eight pa-tients died. Of the 10 patients identified with a LeFort fracture, five died.
ManagementRecognition of Facial Fracture Hemorrhage
as SignificantIn five cases there appeared to be a definite
delay in recognition of the magnitude of the facialfracture hemorrhage. For example, one patientwas referred nonurgently from another hospitalwhile tachycardic, hypotensive, and with melaena.Three negative laparotomies were performed in
Fig. 5. Case 4. Patient before insertion of Foley catheters.
Fig. 6. Case 4. Patient after tongue retraction suture and Foleycatheter insertion.
Volume 123, Number 2 • Massive Hemorrhage in Facial Fracture
685

attempts to identify an abdominal source of bleed-ing. In two of the cases where there was an iden-tifiable delay, the patient died. In other cases theremay also have been some element of delay in di-agnosis, but unless it was clearly identified fromthe medical records, a descriptor of “delay” wasnot used.
Arrest of Hemorrhage MethodIn three patients, arrest of hemorrhage was
attempted with nasal/oral/pharyngeal packingalone. All three patients died. As all three hadmultiple injuries, the contribution of the facialfracture hemorrhage to death was difficult toquantify. Ten patients had insertion of ballooncatheters of some sort–-Foley catheters or Brigh-ton epistaxis catheters–-and no vessel ligation.Four of these patients died; again, each of thedeaths occurred in the context of polytrauma. Fivepatients had ligation of a vessel, either the externalcarotid, maxillary, or anterior ethmoidal, with orwithout other measures. None of these patientsdied. No patients had radiological embolization ofvessels to the face.
Airway ManagementFour patients had no intubation of their air-
way, and of these, two subsequently died. Fourteenpatients had emergency intubation either at thescene of the accident or in the emergency room,and one patient had an emergency tracheostomy.
Blood TransfusionAll patients were given a transfusion of packed
red cells. The median number of units given was9 and the mean number was 10. The mean wasskewed by one case in which 45 units of packed redcells were given. One transfusion was commencedin a Jehovah’s Witness before the discovery of thepatient’s religious beliefs and was ceased imme-diately when this information emerged.
DISCUSSIONIncidence
This study showed that the incidence of mas-sive hemorrhage in facial fractures is low but thatthe phenomenon carries a high risk of death. Thisis in agreement with the findings of others. Gwynet al. pointed out in 1970 that many patients withfacial fractures were multitrauma patients and thatthe incidence of hypovolemic shock was small butsignificant (1.4 percent in their series ofpatients).2 Cannell et al. described 34 patients withmaxillofacial injuries in a cohort of emergencyhelicopter transfer patients, with “severe hemor-rhage” occurring in seven patients, six of whomdied.4 As with our group of patients, many had
concomitant head injuries, making the contribu-tion of the facial hemorrhage difficult to assess. Intheir review of life-threatening complications inmaxillofacial trauma, Ardekian et al. showed avariability in the reported incidence of massivehemorrhage from 0 percent to 11 percent of facialtrauma.8 Bynoe et al.1 examined 912 cases of facialinjuries and found the incidence of life-threaten-ing hemorrhage to be 1.2 percent. Buchanan andHoltmann3 highlighted the danger of epistaxis infacial fracture patients and reported an incidenceof 11 percent of 312 midface fracture patients ashaving “significant epistaxis.” There was, however,no definition of what was considered significantepistaxis. The true incidence of massive facial frac-ture hemorrhage in different centers is not clearbecause there is no agreed upon definition of thephenomenon at present. To make meaningfulcomparisons among experiences, both the numer-ator and the denominator must have agreed def-initions (i.e., what is massive facial fracture hem-orrhage and which facial fractures should beincluded in study populations). We propose thata classification of facial fracture hemorrhage (Fig.7) be adopted and the term “massive facial frac-ture hemorrhage” be used to mean hemorrhageof a defined type as described in the Patients andMethods section of this article and in Figure 7.Creating such a classification would improveawareness of the need to look for and treat facialfracture hemorrhage within the framework of theAdvanced Trauma Life Support survey, would aidfurther research in this field, and would allowbetter communication between referring physi-cians about such patients.
The increased number of cases of massive fa-cial fracture hemorrhage in the 12 months fol-lowing the retrospective study may represent a realincrease in incidence. Improved paramedical andretrieval services could be factors contributing tothis pattern. The veracity of this trend needs to beverified by further study.
Delay in Appropriate TreatmentThis study highlights the fact that hemorrhage
from facial fractures is sometimes underestimatedas a cause of hypovolemia and consequently notarrested early. This can have potentially fatal con-sequences for patients. Perry et al.9 commented intheir review of facial injuries that unrecognizedbleeding was common and that this was often be-cause a significant amount of blood can be swal-lowed by the patient. Tung et al.10 also reporteddelayed recognition of severity of facial fracture
Plastic and Reconstructive Surgery • February 2009
686

hemorrhage and attributed two of the five deathsin their cohort to this delay in diagnosis. Theyfound that 19 of 64 patients with facial fractureshad hemorrhagic shock. As in our study, they re-ported one patient whose nasopharyngeal bleed-ing was treated with nasal packing alone; the pa-tient proceeded to negative laparotomy before themagnitude of the bleeding from the face was rec-ognized.
Delay in diagnosis may be due in part to therarity of facial fractures being the main source ofbleeding in multitrauma patients. Perry et al. com-mented, “When hypovolemic shock is present, fa-cial injuries are unlikely to be the sole cause.”9
While it is true that in any large group of multi-trauma patients only a few will have hypovolemicshock due to facial fracture bleeding, we wouldsuggest that this does not mean that it should beassumed that the hypovolemic shock is due tosome other injury. We have shown that this as-sumption leads to delayed treatment of the facialfracture hemorrhage, with significant conse-quences.
Method of Arrest of HemorrhageAlthough there were few patients in this study
who were treated with nasal packing alone, nonesurvived. In Tung et al.’s series,10 a patient treatedinitially with nasal packing alone also died, and itseems reasonable to conclude that nasal packingalone is an inadequate treatment for patients withmassive hemorrhage from facial fractures. Thecase studies described showed that balloon cath-eters can be effective for arresting hemorrhage,either alone or in combination with other maneu-vers. Cannell’s group also adopted the use of bal-
loon catheters (epistats) and sometimes usedthese in conjunction with looped wire reductionof the fractures and mouth props.4 Perry et al. alsoadvocated the use of mouth props and wires tohold fractures in reduction.9 We did not use in-termaxillary fixation or plate-and-screw fixation offractures acutely. It was contemplated in case 1,but the degree of hemorrhage precluded the vi-sualization necessary for accurate fracture reduc-tion and placement of small screws and plates.Although we understand there may be a place forintermaxillary fixation in holding the reduction ofsome maxillary fractures, it is important to con-sider that in most of our cases the site of thefracture (and bleeding) was between the maxillaand the skull base or upper face and that securingthe maxilla to the mandible cannot compress thissite. In addition, the logistics of intermaxillary fix-ation can be difficult; placement of full wire in-termaxillary fixation is time-consuming and de-pendent on good dentition. Quicker “four-screw”intermaxillary fixation is likely to be insufficientwhen both the mandible and maxilla are frac-tured.
Lynham et al. briefly describe the manage-ment of bleeding in the facial fracture patient,mentioning reduction and wire fixation and nasalpacking and balloon catheters as well as vesselligation.11 Yang et al. advocate an algorithm forearly embolization, although their recommenda-tion is based on a single case.12
None of these studies had enough patients fora statistical comparison of methods. Bynoe et al.have, however, shown some evidence that embo-lization of facial vessels by radiological methods isat least as effective as vessel ligation.1 The avail-
Fig. 7. Classification of facial fracture hemorrhage.
Volume 123, Number 2 • Massive Hemorrhage in Facial Fracture
687

ability of these techniques will vary among hospi-tals, but it would seem, from the evidence in thisstudy and in other literature, that what is impor-tant is the early recognition of the magnitude ofthe hemorrhage and the early arrest of hemor-rhage by some means. Our group would advocateearly orogastric intubation with a large-bore tube.This allows aspiration of swallowed blood andhence more accurate assessment of blood loss, anddoes not incur the risks of nasogastric intubation.We would agree with Perry et al. that facial hem-orrhage should be treated at the “C” stage of theAdvanced Trauma Life Support survey9 and treat-ment should not wait for secondary surveys and soon, by which time the patient may be irreversiblyhypovolemic.
As massive hemorrhage from facial fractures isan unusual occurrence in the experience of indi-vidual treating doctors, we would agree with Yanget al.12 that a guiding algorithm or protocol wouldbe helpful. We have developed guidance for arrestof bleeding in facial fracture hemorrhage and abroader protocol for emergency management ofpatients with facial fracture hemorrhage (Figs. 8through 10). It should be noted that our protocoladvocates embolization in cases of persistentbleeding. This is because although there were nocases of embolization in our series, we were con-vinced that it was the occlusion of the bleedingvessels that was the important factor in success,
rather than the mechanism by which the occlusionwas achieved; in addition, the literature indicatesthat radiological embolization is just as effective assurgical ligation and has less morbidity.1
There was a high rate of tracheal intubation inthis group of patients, and early airway protectionwas obviously an important element of their care.Two patients in this group who were not intubateddied, although it was difficult to assess whether lossof airway control was a contributing factor todeath. Ardekian et al. pointed out the variation in
Fig. 8. Procedure for arrest of facial fracture hemorrhage.
Fig. 9. Position of catheters (note that the endotracheal tube isalso likely to be present).
Plastic and Reconstructive Surgery • February 2009
688

percentage of tracheostomies carried out (be-tween 0.9 percent and 12.3 percent) and them-selves discussed the problem of the heterogeneityof the facial fracture populations studied. Theycame to the conclusion that earlier diagnosis andtreatment would improve the prognosis of thosewith life-threatening complications of maxillo-facial trauma.8
The common thread through all the literatureon hemorrhage in facial fractures is that it is rarebut life-threatening and that its life-threateningnature is often not perceived by the doctors look-ing after these patients. This failure of recognitionleads to failure to arrest the hemorrhage in atimely manner. We believe that the key to improv-ing the prognosis of this group of patients is to
Fig. 10. Protocol for emergency management of facial fracture hemorrhage.
Volume 123, Number 2 • Massive Hemorrhage in Facial Fracture
689

promote awareness of this phenomenon and pro-mote a safe and straightforward primary manage-ment protocol. Classification of hemorrhage infacial fractures should be used in all patients witha midface or skull base fracture. Recording a classof hemorrhage in each of these patients will en-sure the treating primary doctor will properly as-sess this aspect of the facial injuries. Protocols forassessment and treatment of this condition shouldbe included and taught in Advanced Trauma LifeSupport courses. We propose a classification offacial fracture hemorrhage and a definition ofmassive facial fracture hemorrhage as described inthe Patients and Methods section of this article.We recommend that these be adopted for thepurposes of further research and interhospital au-diting and communication, as well as for optimiz-ing the management of individual patients.
Nicola R. Dean, Ph.D., F.R.C.S.(Eng.), F.R.A.C.S.(Plas.)Department of Surgery
Flinders Medical CenterBedford Park
Adelaide SA 5042, [email protected]
ACKNOWLEDGMENTSThe authors acknowledge the contribution of the
patients who gave their consent for photographs to be usedin this article. They also acknowledge the contributionsof Lesley Ward, Department of Medical Records, RoyalAdelaide Hospital, and the photographers of the Depart-ment of Clinical Photography, Royal Adelaide Hospital.
REFERENCES1. Bynoe RP, Kerwin AJ, Parker HH, et al. Maxillofacial injuries
and life-threatening hemorrhage: Treatment with transcath-eter arterial embolization. J Trauma Injury Infection Crit Care2003;55:74–79.
2. Gwyn PP, Carraway JH, Horton CE, et al. Facial fractures:Associated injuries and complications. Plast Reconstr Surg.1971;47:225–230.
3. Buchanan RT, Holtmann B. Severe epistaxis in facial frac-tures. Plast Reconstr Surg. 1983;71:768–770.
4. Cannell H, Silvester KC, O’Regan MB. Early management ofmultiply injured patients with maxillofacial injuries trans-ferred to hospital by helicopter. Br J Oral Maxillofac Surg.1993;31:207–212.
5. American College of Surgeons. Advanced Trauma Life SupportCourse for Doctors. 7th ed. Chicago: American College of Sur-geons; 2004.
6. National Centre for Classification in Health. The InternationalStatistical Classification of Diseases and Related Health Problems,Tenth Revision, Australian Modification (ICD10AM). 5th ed.Sydney, Australia: National Centre for Classification inHealth; 2006.
7. South Australian Department of Health. South Australian De-partment of Health Audit of Clinical Coding Practices (2006).South Australia, Australia; 2006.
8. Ardekian L, Rosen D, Klein Y, et al. Life-threatening com-plications and irreversible damage following maxillofacialtrauma. Injury 1998;29:253–256.
9. Perry M, Dancey A, Mireskandari K, et al. Emergency care infacial trauma: A maxillofacial and ophthalmic perspective.Injury Int J Care Injured 2005;36:875–896.
10. Tung T-C, Tseng W-S, Chen C--T, et al. Acute life-threateninginjuries in facial fracture patients: A review of 1,025 patients.J Trauma Injury Infection Crit Care 2000;49:420–424.
11. Lynham AJ, Hirst JP, Cosson JA, et al. Emergency departmentmanagement of maxillofacial trauma. Emerg Med Australasia2004;16:7–12.
12. Yang W-G, Tsai T-R, Hung C-C, et al. Life-threatening bleed-ing in a facial fracture. Ann Plast Surg. 2001;46:159–162.
Plastic Surgery Educational Foundation Mission StatementThe mission of the Plastic Surgery Educational Foundation® is to develop and support the domestic andinternational education, research, and public service activities of plastic surgeons.
Plastic and Reconstructive Surgery • February 2009
690