
MARKETPLACE MATTERS Products and Pricing
46
This presentation is a high-level summary and for general informational purposes only. The information in this presentation is not comprehensive and does not constitute legal, tax, compliance or other advice or guidance. A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association MARKETPLACE MATTERS Products and Pricing 092713
Transcript of MARKETPLACE MATTERS Products and Pricing

This presentation is a high-level summary and for general informational purposes only. The information in this presentation is not comprehensive and does not constitute legal, tax, compliance or other advice or guidance.
A Division of Health Care Service Corporation, a Mutual Legal Reserve Company,
an Independent Licensee of the Blue Cross and Blue Shield Association
MARKETPLACE MATTERS Products and Pricing
092713
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
In order for a producer to sell Health Insurance Marketplace plans (and receive compensation) in Illinois, a producer must register as an agent/broker with the Centers for Medicare and Medicaid Services (CMS). 1. Producers who are CMS-certified in the Individual Marketplace can sell and
receive compensation for both Marketplace retail plans and non-Marketplace retail plans.
2. Producers who are NOT CMS-certified in the Individual Marketplace can only sell and receive compensation for non-Marketplace retail plans.
In addition, all under 65 retail producers must complete the additional Blue Cross and Blue Shield of Illinois (BCBSIL) product training included in this deck, Marketplace Matters: Product and Pricing, and affirm that they have done so. This training includes important product, benefit and rate information to ensure your success when helping clients with 2014 products.
This training assumes you have already either completed the CMS individual curriculum Marketplace training or the BCBSIL Marketplace Matters: Producer Prep Program.
Training Requirement to Sell Individual
2
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Training Topics
3
Products
Product Overview • Naming Structure • Plan Design Components
Major Medical Products • Marketplace Plans Comparison Charts • Non-Marketplace Plans Comparison
Charts • Catastrophic Plans
Additional Benefits / Ancillary Products • Prescription Benefits • Pediatric Vision Benefits • Dental Benefits • Wellness Benefits
Network Information • Network Coverage • Out-of-Network Benefits • Blue Distinction Centers • Prior Authorizations
ID Cards
Rates & Pricing
Rules Affecting Rates 1. Age Bands 2. Family Demographics 3. Benefit Design 4. Tobacco Use 5. Geographic Rating Areas
Out-of-pocket Costs • Deductibles • Out-of-Pocket Limits • Copayments
Retail Shopping Cart (RSC) • Marketplace Shopping • Non-Marketplace Shopping • Retail Shopping Cart Videos
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Product Overview

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 5
Product Overview
Naming Structure BCBSIL is offering several new major medical products in the under 65 retail market. These products were developed to give consumers many options. The naming structure will help you find the product best suited for your clients. For the product named, “Blue Choice Silver PPO 004,” the naming structure breakdown is as follows:
Branding All names start
with “Blue”
Network Name Indicates the name
of the network
Metallic Level Indicates the metal level of the product: Bronze, Silver, Gold or Platinum. Catastrophic products
are also available Network Type
HMO, PPO
Modifier Differentiates
between plans on the same network in the
same metal level
Blue Choice Silver PPO 004

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 6
Product Overview
Plan Design Components 1. Essential Health Benefits 2. Deductibles 3. Out-of-Pocket Costs 4. Per Occurrence Deductible 5. Out-of-Network Benefits 6. Copayments 7. Prescription Tiers
Name Ded OPX Coins OV / SPC ER RX
Sample Plan $1500 $3000 80% $30/$55 $300 $0 / $10 / $35 /
$75 / $150

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Major Medical Products

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 8
Major Medical Products for BCBSIL
Marketplace Plans: PPO
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
PPO
Gold Blue PPO Gold 001 $3,250 $3,250 100% $30/ $50 $400 $200 $150 $6,500 $6,500 80% NA $300 $250 $0/$10/$35/
$75/$150
Gold Blue PPO Gold 002 $1,500 $3,500 80% $10/ $60 $400 $200 $150 $3,000 $7,000 60% NA $300 $250 $0/$10/$35/
$75/$150
Silver Blue PPO Silver 004 $3,000 $6,350 80% $35/ $55 $500 $250 $200 $6,000 $12,700 60% NA $350 $300 $0/$10/$50/
$100/$150
Silver Blue PPO Silver 003 $6,000 $6,000 100% $30/ $50 $500 $250 $200 $12,000 $12,000 80% NA $350 $300 $0/$10/$50/
$100/$150
Bronze Blue PPO Bronze 005 $5,000 $6,250 80% NA NA NA NA $10,000 $12,500 60% NA NA NA 80% after Ded x
Bronze Blue PPO Bronze 006 $6,000 $6,000 100% NA NA NA NA $12,000 $12,000 80% NA NA NA 100% after Ded x
Note: ER, In-Patient Admissions, and Outpatient Surgery are all per-occurrence-deductibles and not true copayments"
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 9
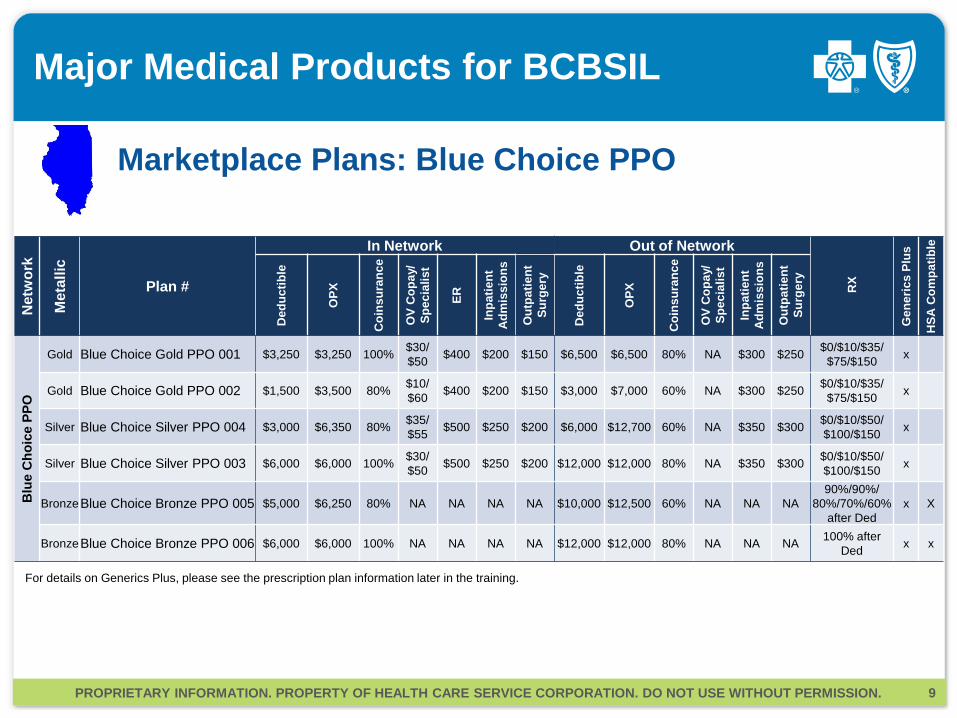
Major Medical Products for BCBSIL
Marketplace Plans: Blue Choice PPO
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Blu
e C
hoic
e PP
O
Gold Blue Choice Gold PPO 001 $3,250 $3,250 100% $30/ $50 $400 $200 $150 $6,500 $6,500 80% NA $300 $250 $0/$10/$35/
$75/$150 x
Gold Blue Choice Gold PPO 002 $1,500 $3,500 80% $10/ $60 $400 $200 $150 $3,000 $7,000 60% NA $300 $250 $0/$10/$35/
$75/$150 x
Silver Blue Choice Silver PPO 004 $3,000 $6,350 80% $35/ $55 $500 $250 $200 $6,000 $12,700 60% NA $350 $300 $0/$10/$50/
$100/$150 x
Silver Blue Choice Silver PPO 003 $6,000 $6,000 100% $30/ $50 $500 $250 $200 $12,000 $12,000 80% NA $350 $300 $0/$10/$50/
$100/$150 x
Bronze Blue Choice Bronze PPO 005 $5,000 $6,250 80% NA NA NA NA $10,000 $12,500 60% NA NA NA 90%/90%/
80%/70%/60% after Ded
x X
Bronze Blue Choice Bronze PPO 006 $6,000 $6,000 100% NA NA NA NA $12,000 $12,000 80% NA NA NA 100% after Ded x x
For details on Generics Plus, please see the prescription plan information later in the training.
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 10
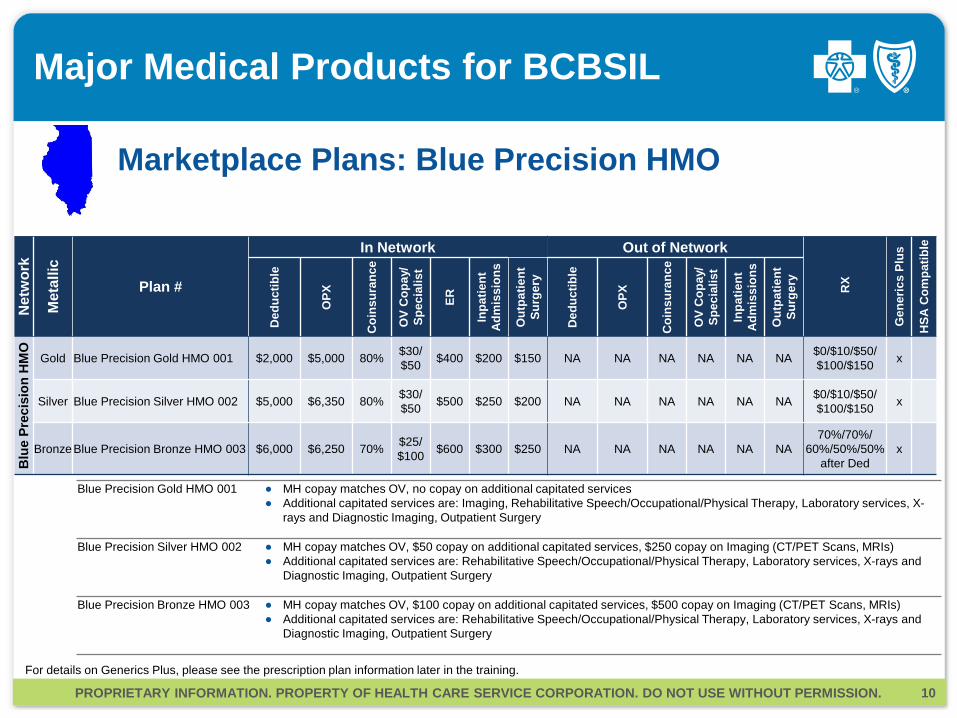
Major Medical Products for BCBSIL
Marketplace Plans: Blue Precision HMO
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Blu
e Pr
ecis
ion
HM
O
Gold Blue Precision Gold HMO 001 $2,000 $5,000 80% $30/ $50 $400 $200 $150 NA NA NA NA NA NA $0/$10/$50/
$100/$150 x
Silver Blue Precision Silver HMO 002 $5,000 $6,350 80% $30/ $50 $500 $250 $200 NA NA NA NA NA NA $0/$10/$50/
$100/$150 x
Bronze Blue Precision Bronze HMO 003 $6,000 $6,250 70% $25/ $100 $600 $300 $250 NA NA NA NA NA NA
70%/70%/ 60%/50%/50%
after Ded x
Blue Precision Gold HMO 001 ● MH copay matches OV, no copay on additional capitated services ● Additional capitated services are: Imaging, Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-
rays and Diagnostic Imaging, Outpatient Surgery
Blue Precision Silver HMO 002 ● MH copay matches OV, $50 copay on additional capitated services, $250 copay on Imaging (CT/PET Scans, MRIs) ● Additional capitated services are: Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-rays and
Diagnostic Imaging, Outpatient Surgery
Blue Precision Bronze HMO 003 ● MH copay matches OV, $100 copay on additional capitated services, $500 copay on Imaging (CT/PET Scans, MRIs) ● Additional capitated services are: Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-rays and
Diagnostic Imaging, Outpatient Surgery
For details on Generics Plus, please see the prescription plan information later in the training.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 11
Major Medical Products for BCBSIL
Non-Marketplace Plans: PPO
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
PPO
Gold Blue PPO Gold 012 $1,000 $3,000 80% $30/ $50 $400 $200 $150 $2,000 $6,000 60% NA $300 $250 $0/$10/$50/
$100/$150
Gold Blue PPO Gold 002 $1,500 $3,500 80% $10/ $60 $400 $200 $150 $3,000 $7,000 60% NA $300 $250 $0/$10/$35/
$75/$150
Gold Blue PPO Gold 001 $3,250 $3,250 100% $30/ $50 $400 $200 $150 $6,500 $6,500 80% NA $300 $250 $0/$10/$35/
$75/$150
Silver Blue PPO Silver 004 $3,000 $6,350 80% $35/ $55 $500 $250 $200 $6,000 $12,700 60% NA $350 $300 $0/$10/$50/
$100/$150
Silver Blue PPO Silver 003 $6,000 $6,000 100% $30/ $50 $500 $250 $200 $12,000 $12,000 80% NA $350 $300 $0/$10/$50/
$100/$150
Bronze Blue PPO Bronze 005 $5,000 $6,250 80% NA NA NA NA $10,000 $12,500 60% NA NA NA 80% after Ded x
Bronze Blue PPO Bronze 006 $6,000 $6,000 100% NA NA NA NA $12,000 $12,000 80% NA NA NA 100% after Ded x

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 12
Major Medical Products for BCBSIL
Non-Marketplace Plans: Blue Choice PPO
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Blu
e C
hoic
e PP
O
Gold Blue Choice Gold PPO 007 $1,000 $3,000 80% $30/ $50 $400 $200 $150 $2,000 $6,000 60% NA $300 $250 $0/$10/$50/
$100/$150 x
Gold Blue Choice Gold PPO 002 $1,500 $3,500 80% $10/ $60 $400 $200 $150 $3,000 $7,000 60% NA $300 $250 $0/$10/$35/
$75/$150 x
Gold Blue Choice Gold PPO 001 $3,250 $3,250 100% $30/ $50 $400 $200 $150 $6,500 $6,500 80% NA $300 $250 $0/$10/$35/
$75/$150 x
Silver Blue Choice Silver PPO 004 $3,000 $6,350 80% $35/ $55 $500 $250 $200 $6,000 $12,700 60% NA $350 $300 $0/$10/$50/
$100/$150 x
Silver Blue Choice Silver PPO 003 $6,000 $6,000 100% $30/ $50 $500 $250 $200 $12,000 $12,000 80% NA $350 $300 $0/$10/$50/
$100/$150 x
Bronze Blue Choice Bronze PPO 005 $5,000 $6,250 80% NA NA NA NA $10,000 $12,500 60% NA NA NA 90%/90%/80%
/70%/60% after Ded
x x
Bronze Blue Choice Bronze PPO 006 $6,000 $6,000 100% NA NA NA NA $12,000 $12,000 80% NA NA NA 100% after Ded x x
For details on Generics Plus, please see the prescription plan information later in the training.
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 13
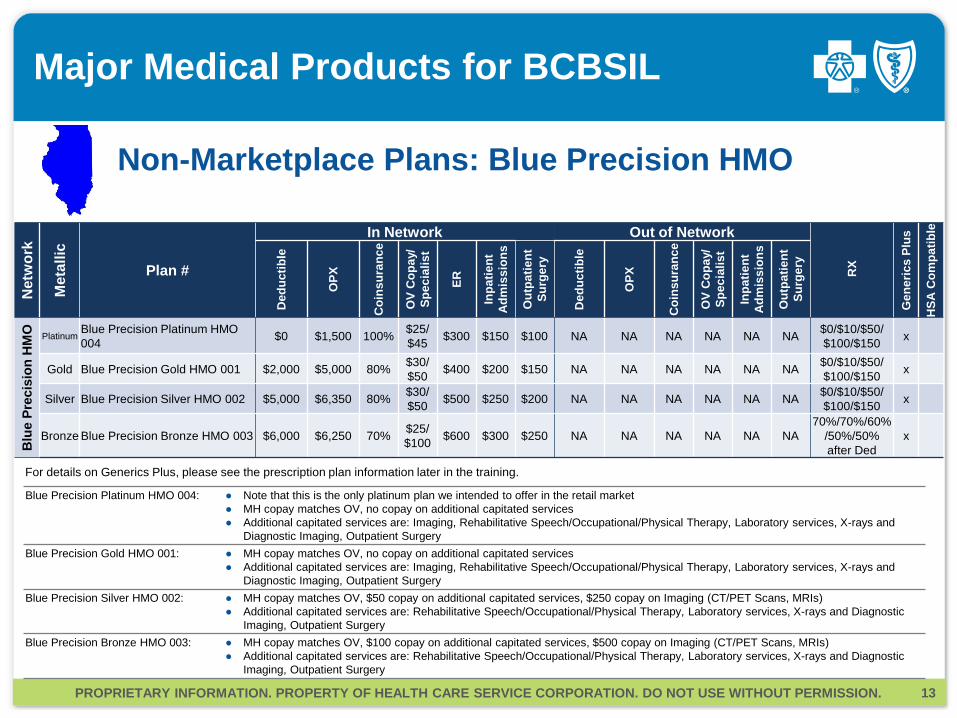
Major Medical Products for BCBSIL
Non-Marketplace Plans: Blue Precision HMO
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Blu
e Pr
ecis
ion
HM
O
Platinum Blue Precision Platinum HMO 004 $0 $1,500 100% $25/
$45 $300 $150 $100 NA NA NA NA NA NA $0/$10/$50/ $100/$150 x
Gold Blue Precision Gold HMO 001 $2,000 $5,000 80% $30/ $50 $400 $200 $150 NA NA NA NA NA NA $0/$10/$50/
$100/$150 x
Silver Blue Precision Silver HMO 002 $5,000 $6,350 80% $30/ $50 $500 $250 $200 NA NA NA NA NA NA $0/$10/$50/
$100/$150 x
Bronze Blue Precision Bronze HMO 003 $6,000 $6,250 70% $25/ $100 $600 $300 $250 NA NA NA NA NA NA
70%/70%/60%/50%/50% after Ded
x
Blue Precision Platinum HMO 004: ● Note that this is the only platinum plan we intended to offer in the retail market ● MH copay matches OV, no copay on additional capitated services ● Additional capitated services are: Imaging, Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-rays and
Diagnostic Imaging, Outpatient Surgery Blue Precision Gold HMO 001: ● MH copay matches OV, no copay on additional capitated services
● Additional capitated services are: Imaging, Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-rays and Diagnostic Imaging, Outpatient Surgery
Blue Precision Silver HMO 002: ● MH copay matches OV, $50 copay on additional capitated services, $250 copay on Imaging (CT/PET Scans, MRIs) ● Additional capitated services are: Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-rays and Diagnostic
Imaging, Outpatient Surgery Blue Precision Bronze HMO 003: ● MH copay matches OV, $100 copay on additional capitated services, $500 copay on Imaging (CT/PET Scans, MRIs)
● Additional capitated services are: Rehabilitative Speech/Occupational/Physical Therapy, Laboratory services, X-rays and Diagnostic Imaging, Outpatient Surgery
For details on Generics Plus, please see the prescription plan information later in the training.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 14
Major Medical Products for BCBSIL
Catastrophic Plans
Net
wor
k
Met
allic
Plan #
In Network Out of Network
RX
Gen
eric
s Pl
us
HSA
Com
patib
le
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
ER
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
Ded
uctib
le
OPX
Coi
nsur
ance
OV
Cop
ay/
Spec
ialis
t
Inpa
tient
A
dmis
sion
s
Out
patie
nt
Surg
ery
PPO
- Blue Security PPO 010 $6,350 $6,350 100% $40* NA NA NA $12,700 $12,700 80% NA NA NA 100% after Ded
*$40 Copay for first 3 office visits, then ded/coins
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Additional Benefits / Ancillary Products
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 16
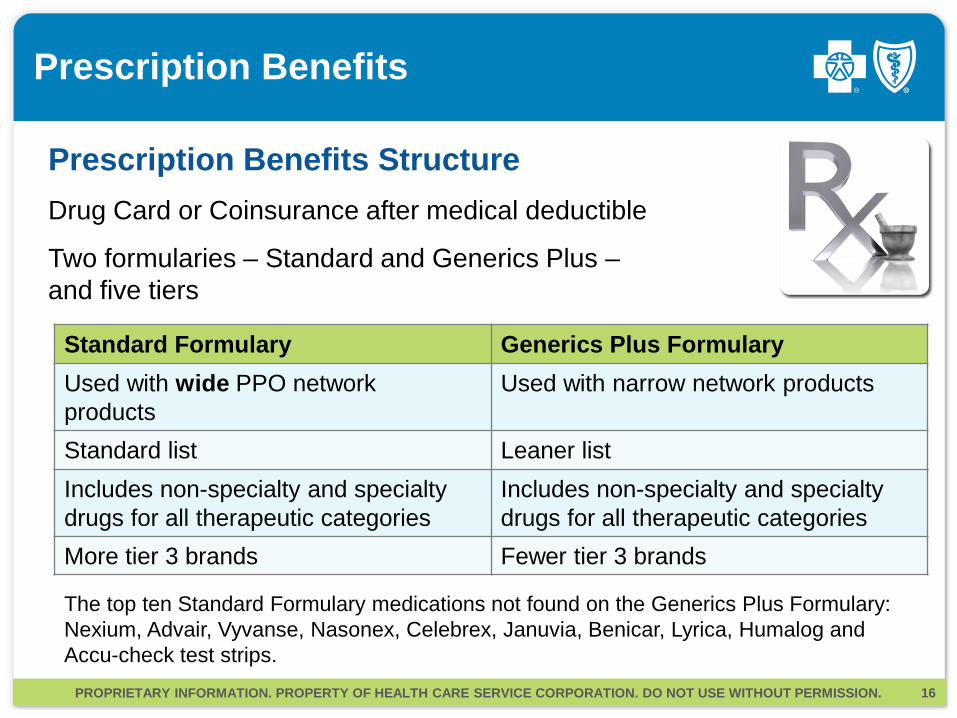
Prescription Benefits
Prescription Benefits Structure
Drug Card or Coinsurance after medical deductible
Two formularies – Standard and Generics Plus – and five tiers
Standard Formulary Generics Plus Formulary Used with wide PPO network products
Used with narrow network products
Standard list Leaner list Includes non-specialty and specialty drugs for all therapeutic categories
Includes non-specialty and specialty drugs for all therapeutic categories
More tier 3 brands Fewer tier 3 brands
The top ten Standard Formulary medications not found on the Generics Plus Formulary: Nexium, Advair, Vyvanse, Nasonex, Celebrex, Januvia, Benicar, Lyrica, Humalog and Accu-check test strips.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 17
Prescription Benefits
Prescription Benefits Structure We are utilizing a five-tier prescription benefit structure, with two of those tiers for generics (preferred and non-preferred).
The five-tier structure drives utilization towards generic prescriptions.
Prescription Tiers Cost Example 1 Generic: Preferred $0 Hydrochlorathiazide 2 Generic: Non-Preferred $10 Valsartan-Hydrochlorathiazide 3 Brand: Formulary $35 Crestor 4 Brand: Non-Formulary $75 Diovan 5 Specialty $150 Humira

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 18
Pediatric Vision
Pediatric Vision Benefits Available to children up to age 19
Embedded in each medical product, premium is included in medical rate
Davis Vision will administer vision products and adjudicate all claims
Vision offerings are based off of benchmark plans identified by HHS. They include:
● Offerings include Eye Exams (one annually) and Frames (one pair in a category of frames) or Contact Lenses
● No member cost sharing for vision services, except for HSA plans with cost sharing for frames and contact lenses

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 19
Ancillary Products: Dental
• Family and child-only dental products are available.
• Marketplace dental products and non-Marketplace dental products available.
• Dental product deductibles and out-of-pocket maximums are separate from major medical product deductibles and out-of-pocket maximums. There is no cross accumulation.
• ACA regulations define pediatric dental as necessary up to age 19 but these have been adjusted to age 21.
Dental Products Overview

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 20
Ancillary Products: Dental
Routine Dental Services • Diagnostic evaluation • Diagnostic radiograph • Preventative
Basic Dental Care • Miscellaneous preventive services • Basic restorative • Non-surgical extractions • Non-surgical perio • Adjunctive services • Endodontics • Oral surgery • Surgical perio
Major Dental Care • Major restorative • Prosthodontics • Miscellaneous restorative and
prosthodontic services Orthodontia Added Provisions with Pediatric Dental • Unlimited annual and lifetime maximums
applied both in and out of network • No waiting periods for in network benefits • Medically necessary ortho • Out-of-pocket maximum applied for in
network only
Dental Benefits The following benefits are covered for both Family and Pediatric products and are subject to coinsurance and deductibles. There are two types of dental plans. Both cover everything listed here, but “high” plans cover them at a higher rate.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 21
Ancillary Products: Dental
Marketplace Dental Plans • We will offer family and child only dental products. • Offering dental plans is enough to maintain compliance of the medical plan.
Non-Marketplace Dental Plans • After a buyer selects a medical plan, he/she will have the option to purchase a stand-
alone dental plan. • If a buyer chooses not to purchase a stand-alone dental plan then reasonable
assurance must be captured that he/she already has an ACA compliant dental plan. • A child only dental plan (pediatric benefits) will be added with the medical product if we
do not receive “reasonable assurance” from the buyer that they already have an ACA compliant dental plan.
• Once we receive the confirmation that they have an ACA compliant dental plan, the child only product will be removed.
• Dental products can be purchased without purchasing medical Marketplace plans or non-Marketplace plans.
Pediatric Dental Rules

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 22
Ancillary Products: Dental
2013 Dental Products used tier-based rating
2014 Dental Product will move to member-based rating
Maximum of 3 dependents (age 0-20) will be rated on a family plan, additional children are added at no charge
Dental Pricing

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 23
Wellness Benefits
Wellness Offerings Condition Management ● Asthma ● Diabetes ● Coronary Artery Disease ● Low Back Pain ● Depression ● Substance Abuse
Care Coordination Early Intervention ● Case Management ● Alerts (ER/Transportation) ● Potential High Dollar ● Actual High Dollar ● Integrated Grand Rounds
Leading Indicators ● Chronic Kidney Disease/End Stage Renal
Disease ● Hip/Knee ● Multiple Co-morbidities (3 or more)
24/7 Nurseline Special Beginnings Core Behavior Health Wellness Offering ● Health Assessment ● Health & Wellness Content ● Wellness Portal ● Fitness Program ● Self Directed Courses (online) ● Medical Utilization Management ● Integrated Grand Rounds ● Longitudinal Care Management Program ● My Care Profile ● Life Points
Community Partnerships to support member engagement and education Care onTarget

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Network Information

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 25
Network Information for BCBSIL
Network Coverage The following BCBSIL Networks are featured in both Marketplace and non-Marketplace Products.
Network Offering Service Area Metallic Levels
PPO Statewide Gold, Silver, Bronze
Blue Choice PPO • Chicago • Quad Cities Rating Areas
Gold, Silver, Bronze
Blue Precision HMO • Chicago Rating Area • Rockford Partial Rating Area
Platinum, Gold, Silver, Bronze

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 26
Network Information for BCBSIL
Out-of-Network Benefits Out-of-Network Benefits for PPO plans ● Out-of-network office visits (primary and specialist) are subject to deductible and
coinsurance, no copayments are applied ● Inpatient admission copayment and outpatient surgery copayments: $100 increase
over in network copayment, per occurrence copayment in addition to deductible and coinsurance
● All other out-of-network services are subject to deductibles and coinsurance ● Deductible: 2x in network up to $25,400 ● Out-of-pocket maximums: 2x in network up to $25,400 ● Coinsurance: 20% differential from in network level with a floor of 50% ● Emergency room services will be the same as in-network
Out-of-Network Benefits for HMO plans ● HMO plans have no out of network benefits ● No away from home benefits for HMO plans, only BlueCard for emergency/urgent care

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 27
Network Information for BCBSIL
Blue Distinction Centers BCBSIL utilizes a soft steerage towards Blue Distinction facilities ● There are no penalties to members for not using these facilities
● BCBSIL promotes its Blue Distinction Centers for knee and hip replacement
● BCBSIL promotes its Blue Distinction Centers for spine surgery
Prior Authorizations Prior authorization will be required for certain services.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
ID Cards

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 29
ID Cards
Changes to ID Cards for 2014 There will be several changes to 2014 ID Cards
● Copayments for five-tier prescription plan will be listed
● Network Values will be displayed
● HMO plan logo updated
● Pediatric dental ID cards will be printed at subscriber level
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Rules Affecting Rates

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 31
Rules Affecting Rates
Rating Characteristics 1. Age Bands
• Age 0-20 is one age band • Age 21-64 have single year age bands • Age 65+ is one age band
2. Family Demographics
• The maximum number of dependents (age 0-20) that will be rated on a family plan is capped at 3
• Dependents age 21+ do not count toward the cap • Spouses under age 21 do not count toward the cap
3. Benefit Design
• Metallic Level & Actuarial Value • Cost Sharing • Network

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 32
Rules Affecting Rates
Rating Characteristics 4. Tobacco Use
• Two Tiers: tobacco use vs. non-tobacco use • “6 month look back” to qualify • Our tobacco rates are 10-33% higher than our
non-tobacco rates (permitted to rate up to 50% higher)
• Rates are subject to the 3:1 rating ratio
5. Geographic Rating Areas • Geographic rating will be by county,
not zip code • Based on the address of the primary insured -
even if any member on a policy has a different address than the primary insured
• To see the Illinois rating areas, visit http://www.cms.gov

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Out-of-pocket Costs
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 34
Out-of-Pocket Costs
Deductible and Out-of-Pocket Limits Overview ● Family deductible and out-of-pocket maximums can be any amount, up to the
mandated out-of-pocket maximum limits ($6,350 for individuals and $12,700 for families).
● For our plans, family deductible and out-of-pocket maximum amounts can be up to 3x that of an individual, but no more than the family out-of-pocket maximum of $12,700. When a family out-of-pocket maximum has been met, all members are considered
to have met the out-of-pocket maximum, regardless of whether or not an individual has met their deductible.
When an individual hits his/her own deductible, the coinsurance benefits kick in, even if a member has family coverage.
● Out-of-network out-of-pocket limits will be 2x in-network out-of-pocket limits. ● Pediatric dental plan deductibles and out-of-pocket maximums are separate
from major medical plan deductibles and out-of-pocket maximums. There is no cross accumulation.
● There are per occurrence deductibles for emergency room, inpatient admissions and outpatient surgery services.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 35
Out-of-Pocket Costs
Deductibles (In-Network)
Out-of-Pocket Maximums (In-Network)
All Medical expenses excluding Copayments and Per-Occurrence Deductibles
● Deductibles ● Per-Occurrence Deductibles ● Copayments (including Rx) ● Coinsurance
What counts toward Deductibles and Out-of-Pocket Maximums?
What is excluded from Deductibles and Out-of-Pocket Maximums? > Premiums > Claims for uncovered services > Preauthorization penalties

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 36
Out-of-Pocket Costs
Copayments Overview Office Visit copayments will cover everything billed as part of Office Visit (if performed in the same office on the same day).
● Exceptions: surgery, physical, occupational, and speech therapies, chiropractic and osteopathic manipulation
● If services are performed in a separate office or facility and billed separately, coinsurance and deductible apply
Mental Health and Substance Abuse will be covered the same as any other medical service

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Retail Shopping Cart (RSC)

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 38
Retail Shopping Cart
Marketplace Shopping: Two Pathways Producers intending to work with consumers in Illinois, which is a State Partnership Marketplace state, will be able to assist consumers to apply for and purchase Marketplace plans in two ways:
(a) an issuer-based pathway, through which a producer uses an issuer’s website, such as the BCBSIL Retail Shopping Cart, to assist the consumer, or
(b) a Marketplace pathway, through which a producer assists the consumer by directly accessing the Get Covered Illinois website.
Both pathways transmit producer identifying information to us so that you will be compensated for sales of BCBSIL Marketplace plans.
Both pathways allow a producer to assist a qualified individual with initial enrollment and changes during the coverage year, including changes that impact eligibility.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 39
Retail Shopping Cart
Before You Begin: What Your Clients Need for Marketplace plan shopping 1. Social Security Numbers or document numbers for legal
immigrants (proof of U.S. citizenship or legal residency)
2. Proof of state residency may be required
3. Valid email address is highly encouraged
4. Employer and income information for every household member (pay stubs, wage and tax statements)
5. Policy numbers and information for current health insurance plans covering members of a household
6. A completed Employer Coverage Form tool.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 40
Retail Shopping Cart
• Shopping begins on BCBSIL.com Retail Shopping Cart website
• BCBSIL and the Health Insurance Marketplace interact to determine eligibility to: • Purchase a Marketplace plan • Receive a premium tax credit • Receive a cost-sharing subsidy
• User completes enrollment on BCBSIL.com website
• Shopping begins on BCBSIL.com Retail Shopping Cart website
• Member is able to shop and enroll through BCBSIL.com website
• No interaction with the Health Insurance Marketplace
Express Link works with the Retail Shopping Cart and supports enrolling consumers in both Marketplace and non-Marketplace plans.
Process when shopping Non-Marketplace products
Process when shopping Marketplace products

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 41
Retail Shopping Cart
Retail Shopping Cart
Enter census details
Enrollment Directed to Enrollment
Form End
Plan results for non-
Marketplace
Connects Member to RSC
Express Link
Shop with
credit?
Use estimate
or get official
Credit Estimator
Official Determination
No
Yes
Confirm & Apply
Create an account
or log in Select a plan
Plan Results for “pre
shopping”
This flow charts depicts a Producer-led or Producer-generated process from Express Link through to enrollment.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 42
Retail Shopping Cart
Retail Shopping Cart
Asked to create an account or
log in
The Get Covered Illinois Health Insurance Marketplace
Directed to “send off” with
prep info
Directed back to RSC to log
in
User registers
Completes eligibility
application (see the next page)
User confirms shopping
information
Directed to Plan Results
Directed to Complete Enrollment
Selects a Marketplace
plan
This flow charts depicts a consumer process for shopping on BCBSIL, finding a Marketplace plan, completing Marketplace eligibility and shopping up to enrollment. See the next page for interacting with the Marketplace.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 43
Retail Shopping Cart
BCBSIL Pathway Consumers complete the Marketplace eligibility application process. When complete, they are moved back to the BCBSIL shopping website and producers can help them enroll in a plan.
The Get Covered Illinois Health Insurance Marketplace User
registers
Completes eligibility
Marketplace Application

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION. 44
Retail Shopping Cart
View ALL NEW Retail Shopping Cart videos For more details on the Retail Shopping Cart, go to the BCBSIL Blue Access for ProducersSM website. Log in to your account. 1. Select the green Training and Administration button from the left navigation
menu bar. 2. Click on the Individual tab. 3. Scroll to the blue Individual Products Training bar and view the shopping
videos, which are accessed via Dropbox.
1.
3.
2.

PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Training Affirmation Form
PROPRIETARY INFORMATION. PROPERTY OF HEALTH CARE SERVICE CORPORATION. DO NOT USE WITHOUT PERMISSION.
Affirmation Form: Completed Training
46
Thank you for completing the Marketplace Matters: Product and Pricing training.
In order to receive credit for your training, you must complete and submit the correct BCBSIL Training Affirmation form.
Complete the Option A Training Affirmation Form if you will sell both Marketplace and Non-Marketplace plans.
Complete the Options B Training Affirmation Form if you will sell only Non-Marketplace plans.


















