Marian University - inosteo.org Annual...“Under Foot! OMM Clinical Pearls” Indiana Osteopathic...
28
“Under Foot! OMM Clinical Pearls” Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM) 1 Michael L. Kuchera, DO, FAAO Professor Osteopathic Manipulative Medicine [email protected] Marian University – C ollege of O steopathic M edicine Marian University College of Osteopathic Medicine & Home Office of the Indiana Osteopathic Association
-
Upload
truongdang -
Category
Documents
-
view
215 -
download
0
Transcript of Marian University - inosteo.org Annual...“Under Foot! OMM Clinical Pearls” Indiana Osteopathic...
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
1
Michael L. Kuchera, DO, FAAO
Professor Osteopathic Manipulative Medicine
Marian University –College of Osteopathic Medicine
Marian University College of Osteopathic Medicine& Home Office of the Indiana Osteopathic Association

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
2
Dozen (+/-) Clinical Pearls to Toss Out
Use in 3 Common Conditions
Multi-Task; Multi-Use
Exposure to Multiple Methods
Short Time so 3 Labs to Practice
Clinically-Useful Stuff
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
3
1. Clinical pearls that “stick” with you
2. Something practical that you can
take back to your patients
3. Integrate structure & function for OMT
4. Provide ongoing resource options
◦ Myofascial TrP electronic text
Other: Lower Extremity
information (Foundations for
Osteopathic Medicine - LE author)
5. Sneak in some EBM
Caught You Flat Footed! Know Your “Arch Nemesis”◦ Lab 1a: “Bootjack” Technique Hindfoot-Midfoot Integration
◦ Lab 1b: Hiss Whip & Locke Technique Navicular-Cuboid-Cuneiform
◦ Lab 1c: Soft Tissue OMT Arches
Malicious Malalignment Syndrome: Are These Knees
Made for Running?◦ Lab 2a: Counterstrain Vastus medialis & patella
◦ Lab 2b: BLT Tibiofemoral joint
Recurrent Ankle Sprains◦ Lab 3a: BLT Talocalcaneal through Fibular Head
◦ Lab 3b: Muscle Energy & HVLA Talus-in-the-Ankle-Mortis
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
4
“Because my genetic programmingprevents me from asking directions…
...that’s why!!!”
After: [email protected] to MU-COM SAAO
The Lower Extremities are the Foundation of body & a major
determinant of posture, balance, gait, etc
Talocalcaneal = “Shock Absorber” ◦ Functional Demand Can calculate “Accumulated Impact
Loading”
Major Biomechanical Risk Factors: ◦ Malicious (“Malignant”) Malalignment Syndrome: Predictable
Somatic Dysfunction; Coxa varus with Genu valgus with Increased
Q-angle; Pronated Foot (“highest risk for runners” plus arch problems);
High Levels of Accumulated Impact Loading (AIL)
◦ Supination Ankle Sprain: Most common ankle sprain; Predictable
Somatic Dysfunction; Posterolateral glide of T-C joint; plantar
flexion of ankle joint; posterior fibular head (etc); high AIL
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
5
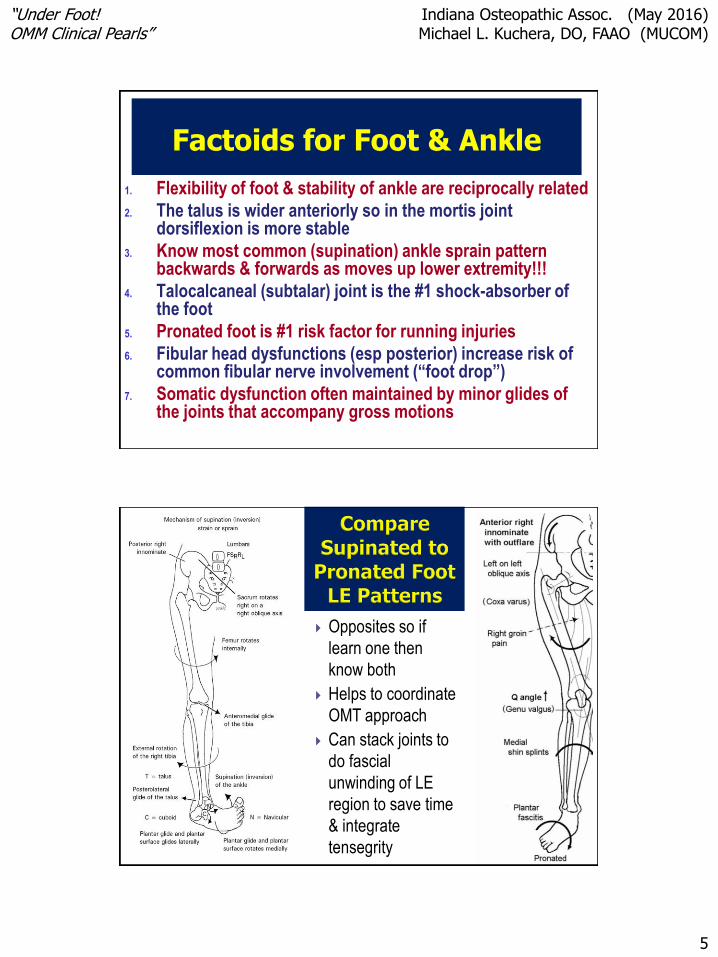
Factoids for Foot & Ankle
1. Flexibility of foot & stability of ankle are reciprocally related
2. The talus is wider anteriorly so in the mortis joint dorsiflexion is more stable
3. Know most common (supination) ankle sprain pattern backwards & forwards as moves up lower extremity!!!
4. Talocalcaneal (subtalar) joint is the #1 shock-absorber of the foot
5. Pronated foot is #1 risk factor for running injuries
6. Fibular head dysfunctions (esp posterior) increase risk of common fibular nerve involvement (“foot drop”)
7. Somatic dysfunction often maintained by minor glides of the joints that accompany gross motions
Opposites so if
learn one then
know both
Helps to coordinate
OMT approach
Can stack joints to
do fascial
unwinding of LE
region to save time
& integrate
tensegrity

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
6
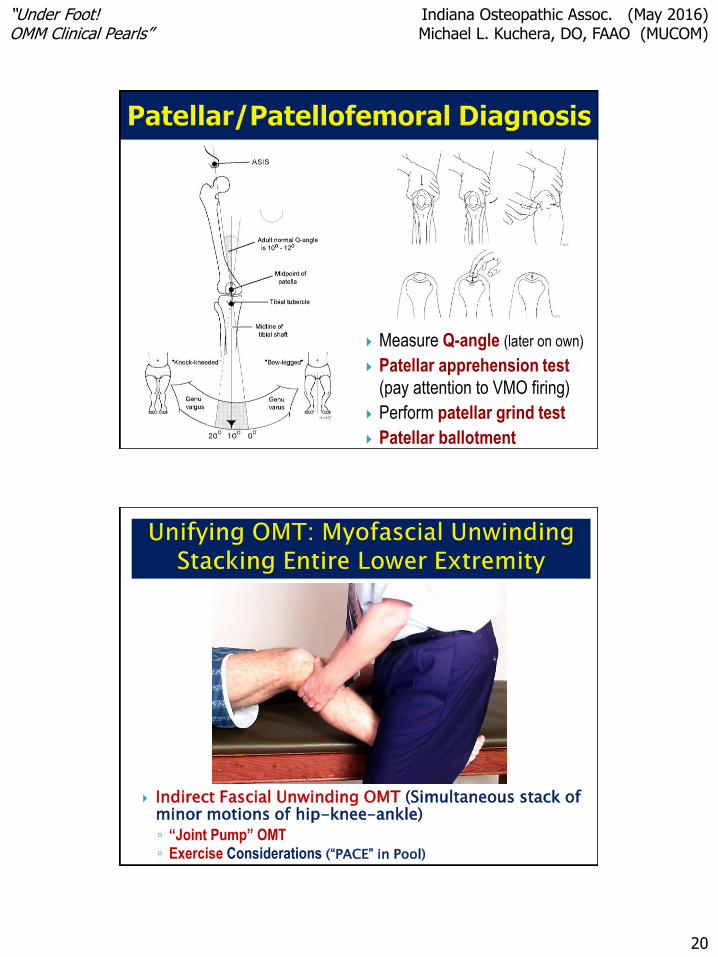
Note the following elements:◦ Wide hips
◦ Coxa varus (angle < 120o) … n = 120-135o
◦ Genu valgus (Q-angle > 15/20o) … n = 0-20o (age)
… adult Q-angle usually 10-12o
◦ Pronated foot with pes planus (flat-footed)
◦ Talocalcaneal joint SD (anteromedial)
⇧Risk:◦ ⇧Accumulated impact loading with ⇧ascending
injury risk if run (distanceXweight is involved)
◦ Patellar tracking problem/Chondromalacia patellae
Knock-kneed
Flat footed
Memory NOTE = SD opposite supination sprain pattern
Pes planus: “Foundation”
affects posture above; rigidifies
ankle joint; changes functional
leg length; gait; biomechanics
of shock absorption (&
therefore risk of ascending
injury)
Genu recurvatum (concern
about hypermobility, Ehlers-
Danlos, etc; may wish to stick
to indirect OMT; somatic clues
to systemic issues like Marfan
Syndrome)
Dudley J. Morton Foot
Foot-Ankle Relation
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
7
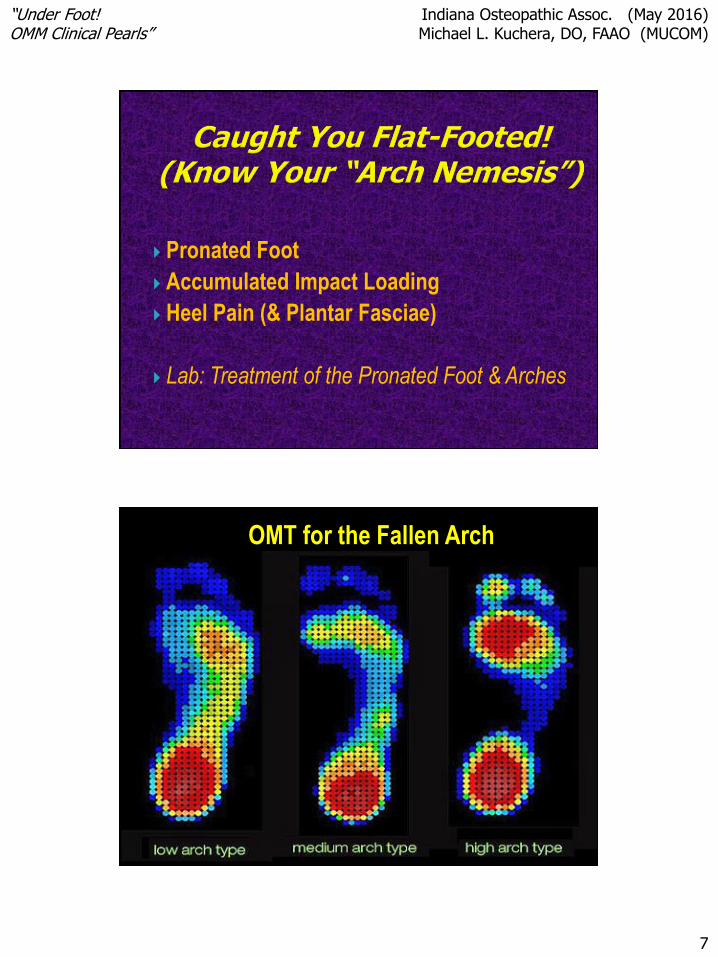
Pronated Foot
Accumulated Impact Loading
Heel Pain (& Plantar Fasciae)
Lab: Treatment of the Pronated Foot & Arches
OMT for the Fallen Arch

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
8
(Mechanoreceptor& Proprioceptor Input)
Chopart
Joint
Lisfranc
Joint
Hindfoot
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
9
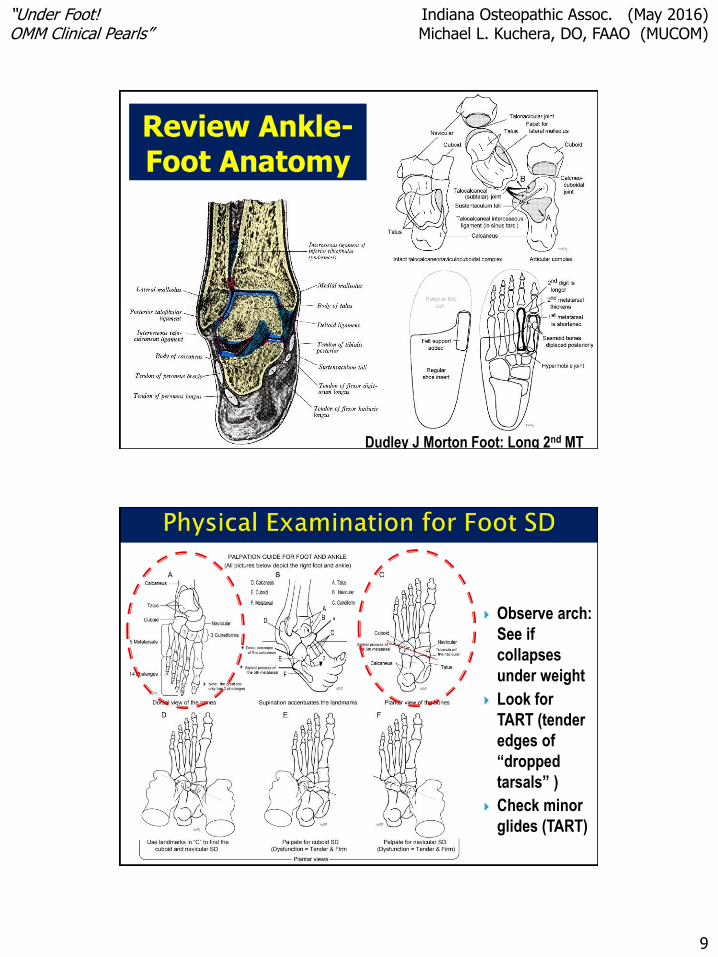
Review Ankle-Foot Anatomy
Dudley J Morton Foot: Long 2nd MT
Observe arch:
See if
collapses
under weight
Look for
TART (tender
edges of
“dropped
tarsals” )
Check minor
glides (TART)

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
10
Redoming Plantar Arches
Patient Coop (Toes Up & Down)
Pivot on bottom
Pull edges around
Transverse
Arch
Note importance of
L5 & of peroneus muscles
in both (Note peroneus &
fibular head relationship)

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
11
Visualize
anatomy
Cuboid &
Navicular
drop & roll
2nd cuneiform
drops
inferior
Dropped edge
very tender
Specific Mid-Foot Joint Somatic Dysfunction
◦ Fallen Tarsal or Transverse Arch Muscle Energy & Articulatory
◦ “Dropped” Navicular
◦ “Dropped” Cuboid
◦ “Dropped” 2nd Cuneiform
Specific Forefoot Joint Somatic Dysfunction
◦ Tarsal – Metatarsal Anterior or Posterior Glide
HVLA (“Dr. Locke”) OMT
◦ MTP, PIP & DIP
BLT (Stacking) or FPR
HVLA – Hiss Whip}
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
12
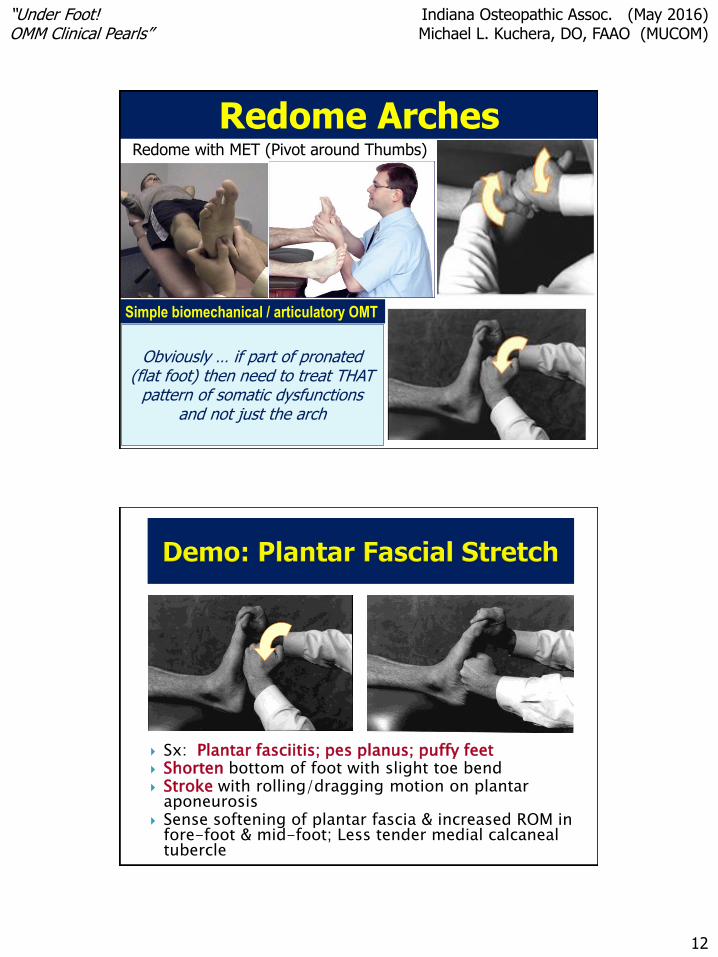
Redome ArchesRedome with MET (Pivot around Thumbs)
Obviously … if part of pronated (flat foot) then need to treat THAT
pattern of somatic dysfunctions and not just the arch
Simple biomechanical / articulatory OMT
Sx: Plantar fasciitis; pes planus; puffy feet Shorten bottom of foot with slight toe bend Stroke with rolling/dragging motion on plantar
aponeurosis Sense softening of plantar fascia & increased ROM in
fore-foot & mid-foot; Less tender medial calcaneal tubercle
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
13
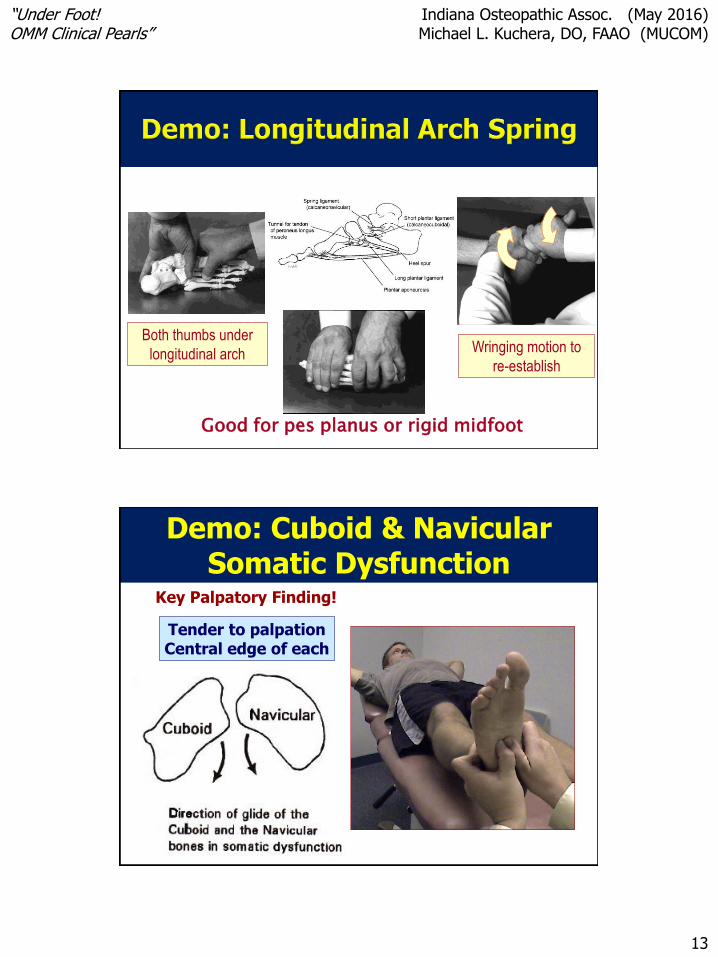
Good for pes planus or rigid midfoot
Both thumbs under
longitudinal arch Wringing motion to
re-establish
Demo: Cuboid & Navicular Somatic Dysfunction
Tender to palpationCentral edge of each
Key Palpatory Finding!
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
14
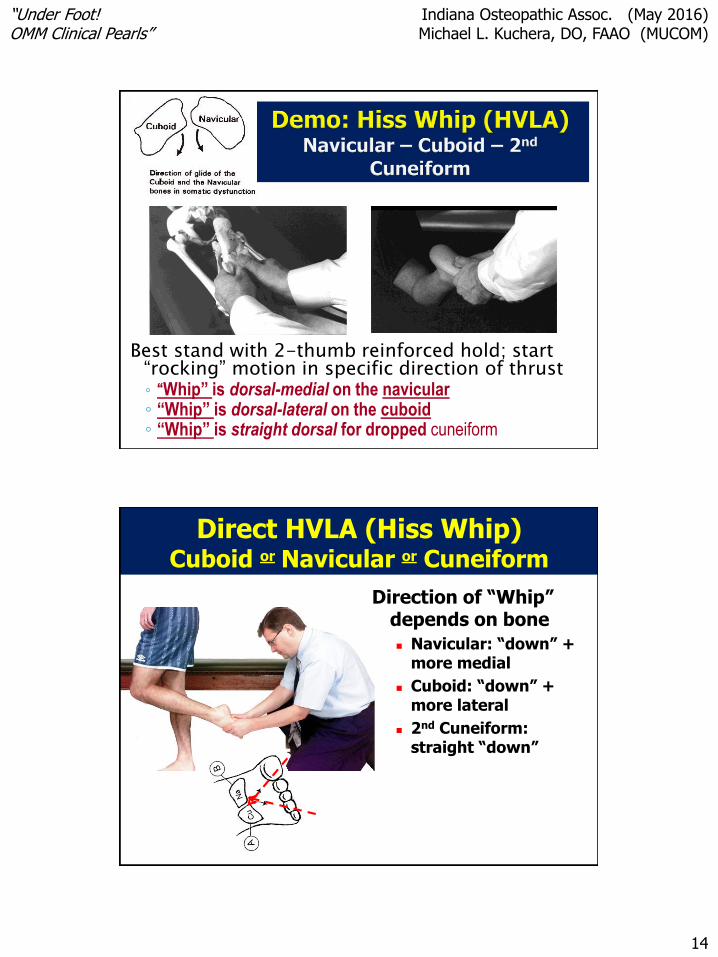
Best stand with 2-thumb reinforced hold; start “rocking” motion in specific direction of thrust◦ “Whip” is dorsal-medial on the navicular◦ “Whip” is dorsal-lateral on the cuboid◦ “Whip” is straight dorsal for dropped cuneiform
Direct HVLA (Hiss Whip)Cuboid or Navicular or Cuneiform
Direction of “Whip” depends on bone
Navicular: “down” + more medial
Cuboid: “down” + more lateral
2nd Cuneiform: straight “down”

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
15
Direct HVLA
Metatarsal Glide SD
Emphasis on Glide
Short Lever vs Long Lever
Dr. Locke Technique for 1st
Metatarsal
5th MT
Also demo for MTP’s using toe traction
with pressure over metatarsal heads
“Heel Spur” – Sign of failing biomechanics ◦ Treat problem prior to considering
treating spur
Plantar fasciitis
Shoe problem?
Somatic dysfunction foot/ankle
Myofascial TrP’s◦ Quadratus Plantae
◦ Soleus could also cause
Quadratus plantae
MTrP
Soleus MTrP

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
16
Supination with TC
Posterolateral Glide
Pronation with TC
Anteromedial glide
Talus gliding along
articulation on the
calcaneus (Review)
Direct Talocalcaneal
Gap OMT Use traction to unlock
and stabilize the hind-
foot
PLUS Indirect BLT of
Foot/Ankle & MFR
Plantar Fascia Curl toes & use indirect
MFR to balance hind-foot
to rest and release
plantar fascia

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
17
1. Hiss Whip (HVLA: Navicular; Cuboid;
2nd Cuneiform)
2. Locke Glide (HVLA @ foot division)
3. “Bootjack” (Direct talocalcaneal;
Indirect forefoot/midfoot)
4. Redome Arches (MET/Artic/SoftTs)
Choose 1-4
OMT for the
Knee
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
18
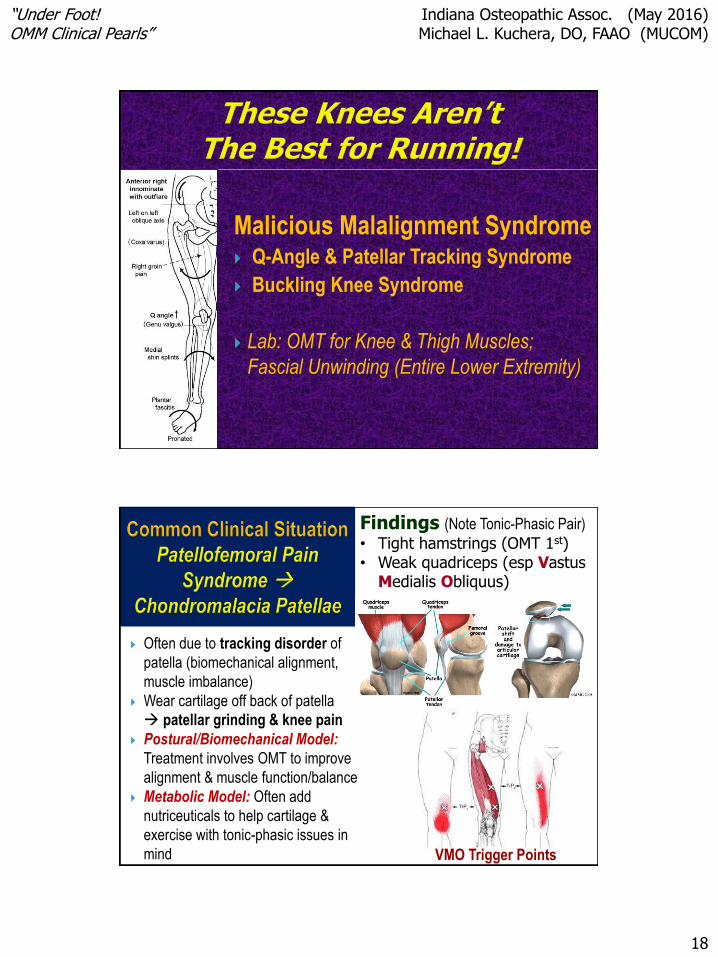
Malicious Malalignment Syndrome Q-Angle & Patellar Tracking Syndrome
Buckling Knee Syndrome
Lab: OMT for Knee & Thigh Muscles;
Fascial Unwinding (Entire Lower Extremity)
Often due to tracking disorder of
patella (biomechanical alignment,
muscle imbalance)
Wear cartilage off back of patella
patellar grinding & knee pain
Postural/Biomechanical Model:
Treatment involves OMT to improve
alignment & muscle function/balance
Metabolic Model: Often add
nutriceuticals to help cartilage &
exercise with tonic-phasic issues in
mind
Findings (Note Tonic-Phasic Pair)
• Tight hamstrings (OMT 1st)• Weak quadriceps (esp Vastus
Medialis Obliquus)
VMO Trigger Points

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
19
Biomechanical Alignment: Optimize Q-Angle (OMT to hip &
knee joints; foot mechanics)
Muscle Imbalance: Stretch hamstrings (tonic) strengthen
quadriceps-VMO (phasic); alternatives MET, counterstrain, etc◦ Professional equipment vs simple home exercises
Ergonomic: Educate to reduce kneeling / overuse
Nutritional: Glucosamine – Chondroitin Sulfate
Tensegrity/Balance goal for lower extremity addressing muscles &/or using lower extremity
stacking / unwinding OMT is helpful
PEARL: 1st stretch/tx
Hamstrings; then OMT
Quadriceps; then
strengthen quadriceps
CS opposite MET
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
20
Measure Q-angle (later on own)
Patellar apprehension test
(pay attention to VMO firing)
Perform patellar grind test
Patellar ballotment
Indirect Fascial Unwinding OMT (Simultaneous stack of minor motions of hip-knee-ankle)
◦ “Joint Pump” OMT◦ Exercise Considerations (“PACE” in Pool)

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
21
1. Muscle Balance
(MET Hamstrings)
2. Muscle Balance
(Counterstrain Vastus Medialis)
3. LE Unwinding
(Indirect stacking hip, knee, ankle)
CS: Vastus medialis
LE Unwinding
Supination Sprain Pattern
Addressing Joint &
Muscle Stability
Labs: OMT for Ankle &
Foreleg

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
22
Supination ankle sprain
Most common sports injury in LE
Implications for total body
Predictable somatic dysfunction
pattern
Failure to correct SD recurrence
Ankle Sprain Clinical Discussion:◦ Ottawa Ankle Rule Examination
◦ Classifications (varies # ligs; degree of tear; etc)
◦ Imbalance
Tonic (Gastroc/Soleus)
Phasic (Peroneus/TA)
Section #3a

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
23
Pain in Malleolar Zone or
Midfoot Zone
PLUS one of following … Inability to bear weight
immediately & in EM Dept
A or B Bone Tenderness
(posterior or tip of either
malleolus)
C or D Bone Tenderness
B
D
C
A
97% Sensitivity
Tuning Fork Pearl
Classification by
amount of tear
(Strain Partial
Complete Tear)
Classification by
number of
ligaments
affected (ATF
CF PTF)
Foundations for
Osteopathic Med
Ant Draw(er) Test for ATF Ligament

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
24
Eversion TalarTilt Test
Strong ligament … often bone will fracture before ligament fully torn
BLT
Wrap (RICE):
Talus wider in
front so more
stable in
dorsiflexion (with
posterior glide)Plantar flexion + anterior glide
Dorsiflexion + posterior glide
LAB: Anterior Drawer + Talar Tilt + Ottawa Rule Check + Glides BLT
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
25
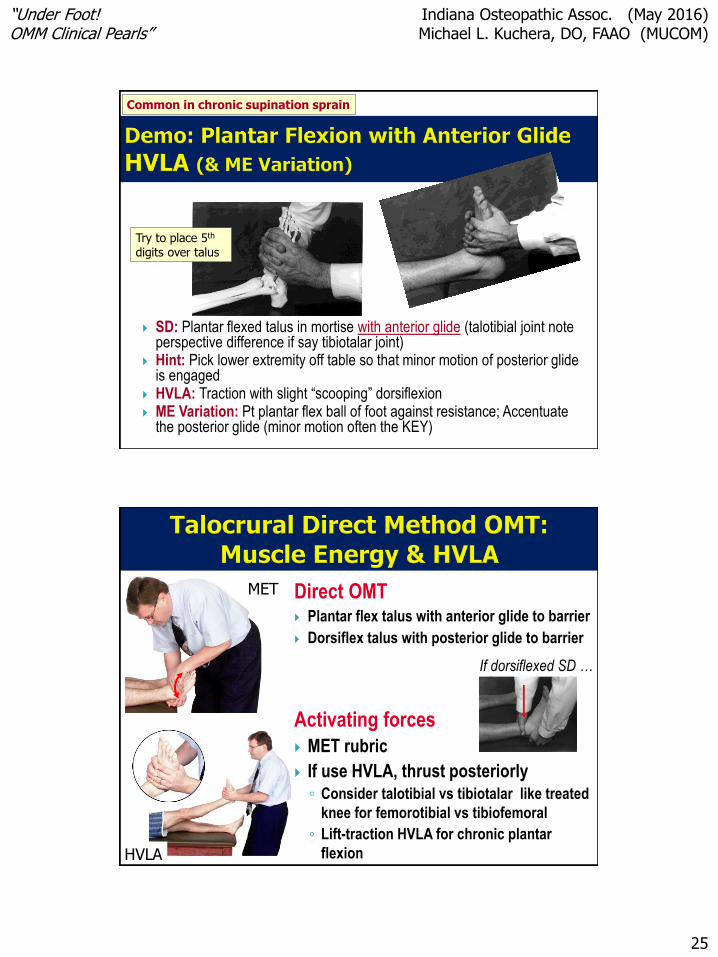
SD: Plantar flexed talus in mortise with anterior glide (talotibial joint note perspective difference if say tibiotalar joint)
Hint: Pick lower extremity off table so that minor motion of posterior glide is engaged
HVLA: Traction with slight “scooping” dorsiflexion ME Variation: Pt plantar flex ball of foot against resistance; Accentuate
the posterior glide (minor motion often the KEY)
Try to place 5th
digits over talus
Common in chronic supination sprain
Direct OMT Plantar flex talus with anterior glide to barrier
Dorsiflex talus with posterior glide to barrier
Activating forces
MET rubric
If use HVLA, thrust posteriorly◦ Consider talotibial vs tibiotalar like treated
knee for femorotibial vs tibiofemoral
◦ Lift-traction HVLA for chronic plantar
flexion
MET
HVLA
If dorsiflexed SD …

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
26
Direct or Indirect OMT Supination with posterolat TC glide
Pronation with anteromed TC glide
Activating forces BLT review – take to balance point
(glide PL or AM); use respiratory
cooperation with air hunger
HVLA rubric AM or PL thrust through
talus while stabilizing calcaneus
HVLA
BLT
Fibular Head Often Posterior in Supination Sprain Pattern
Diagnosis & Treatment(Reciprocal Motion of Fibula)
Also longitudinal for Interosseous Membrane
Fibular head
possible impact
on common
peroneal
(fibular) nerve
“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
27
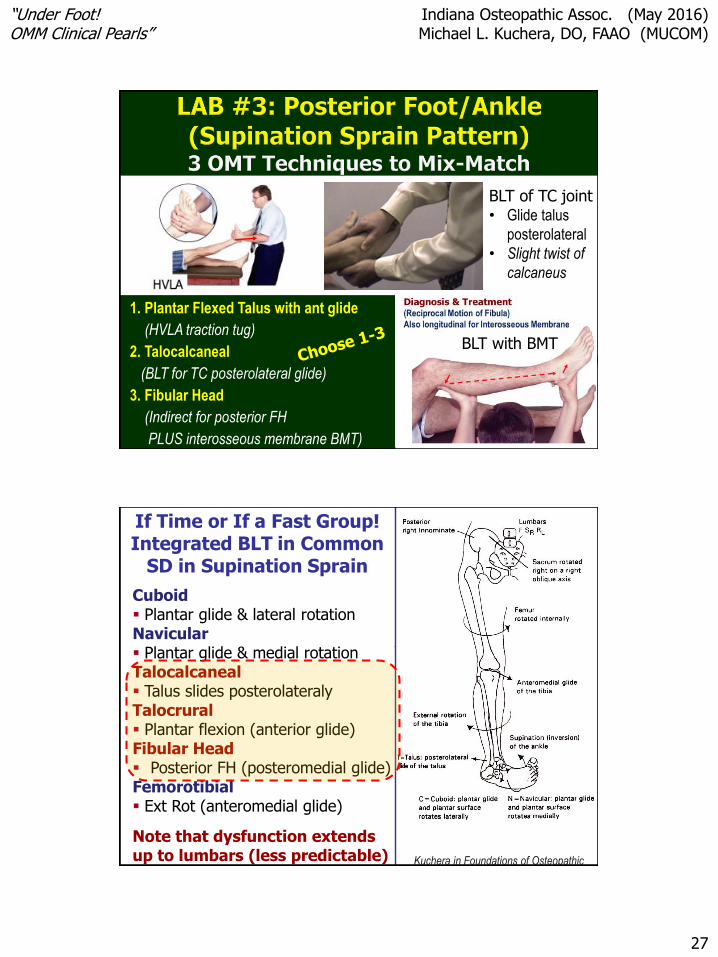
1. Plantar Flexed Talus with ant glide
(HVLA traction tug)
2. Talocalcaneal
(BLT for TC posterolateral glide)
3. Fibular Head
(Indirect for posterior FH
PLUS interosseous membrane BMT)
BLT with BMT
BLT of TC joint• Glide talus
posterolateral
• Slight twist of
calcaneus
If Time or If a Fast Group!Integrated BLT in Common
SD in Supination Sprain
Cuboid Plantar glide & lateral rotationNavicular Plantar glide & medial rotationTalocalcaneal Talus slides posterolateralyTalocrural Plantar flexion (anterior glide)Fibular Head Posterior FH (posteromedial glide)Femorotibial Ext Rot (anteromedial glide)
Note that dysfunction extends up to lumbars (less predictable) Kuchera in Foundations of Osteopathic
Medicine

“Under Foot!OMM Clinical Pearls”
Indiana Osteopathic Assoc. (May 2016) Michael L. Kuchera, DO, FAAO (MUCOM)
28
Congratulations!
“The regimen I adopt will be for the benefit of my patients according to my abilities and judgment.”
--Hippocrates
“Dig On!”
--A.T Still