MAPPING THE DIABETES HEALTH PROFILE (DHP-18) ONTO THE EQ-5D AND SF-6D GENERIC PREFERENCE BASED...
14
MAPPING THE DIABETES HEALTH PROFILE (DHP-18) ONTO THE EQ-5D AND SF-6D GENERIC PREFERENCE BASED MEASURES OF HEALTH Brendan Mulhern 1 , Keith Meadows 2 , Donna Rowen 1 & John Brazier 1 1 Health Economics and Decision Science, University of Sheffield 2 DHP Research & Consultancy Ltd, London Contact: [email protected]
-
Upload
august-daniels -
Category
Documents
-
view
218 -
download
2
Transcript of MAPPING THE DIABETES HEALTH PROFILE (DHP-18) ONTO THE EQ-5D AND SF-6D GENERIC PREFERENCE BASED...

MAPPING THE DIABETES HEALTH PROFILE (DHP-18)
ONTO THE EQ-5D AND SF-6D GENERIC PREFERENCE BASED
MEASURES OF HEALTH
Brendan Mulhern1, Keith Meadows2, Donna Rowen1 & John Brazier1
1 Health Economics and Decision Science, University of Sheffield2 DHP Research & Consultancy Ltd, London
Contact: [email protected]

Contents
• Introduction• Measurement of HRQL and cost utility in diabetes
• Methods• Data
• Mapping techniques
• Results• Mapping functions developed to estimate EQ-5D utility
scores
• Mapping functions developed to estimate SF-6D utility scores
• Discussion19/04/23 © The University of Sheffield

Introduction• Diabetes interventions place a significant burden on health resources
• Approx 10% of the NHS budget
• Resource allocation informed by economic evaluation of new treatments
• Quality Adjusted Life Year (QALY) a recommended measure of outcome (NICE, 2008).
• Value for ‘quality’ derived using generic preference based measures• EQ-5D and SF-6D
• Generic measures should be included in trials to facilitate economic evaluations but are often not used
19/04/23 © The University of Sheffield

Mapping
• Mapping used to:• Predict generic measure utility values from existing condition
specific measures of HRQL using regression modelling
• Mapping is possible when • The generic measure performs well in the disease area
• EQ-5D and SF-6D validated in diabetes populations
• There is a correlation between the generic and condition specific HRQL measures
• This study predicts EQ-5D and SF-6D utility values scores using the Diabetes Health Profile-18 (DHP-18)
19/04/23 © The University of Sheffield

Generic preference based measures
19/04/23 © The University of Sheffield
• SF-6D• Derived from SF-36/SF-12
• 6 dimensions• physical functioning• role limitations• social functioning• pain• mental health• vitality
• Generates 18,000 health states
• 249 states valued using Standard Gamble
• Utility score range 0.29 to 1
• EQ-5D• Recommended by NICE for use
in cost utility analysis
• 5 dimensions with 3 response levels
• Mobility/self-care• daily activities• pain/discomfort• anxiety/depression
• Generates 243 (35) health states
• Selection of states valued using Time Trade Off
• Results modelled to produce single figure utility score, range -0.594 to 1

Diabetes Health Profile-18• Measures HRQL in diabetes
• Psychological distress
• Barriers to activity
• Disinhibited eating
• Demonstrates reliability, validity and patient acceptability
• 26 translations
• Completed using a range of media
• Diabetes-specific measure selected for the UK Department of Health PROMs Pilot for Long Term Conditions in Primary Care
• Visit www.diabeteshealthprofile.com for more information
19/04/23 © The University of Sheffield

Mapping specifications
19/04/23 © The University of Sheffield
• Model type• OLS; RE GLS; Tobit; Two part models
• Model performance indicators:• R2, Walt chi squared
• Mean absolute error and mean squared error
• Plots of observed and predicted scores
Number Model specification
1 DHP dimension scores
2 DHP dimension scores, DHP dimension scores squared
3 DHP dimension scores, DHP dimension scores squared, DHP dimension score interactions
4 DHP dimension scores, DHP dimension scores squared, DHP dimension score interactions, Age, Gender
5 DHP item scores
6 DHP item scores, DHP item scores squared
7 DHP item scores, DHP item scores squared, Age, Gender

Sample
• UK longitudinal dataset of a community-based postal survey• ≥18 years of age
• Data collected at baseline and 1 year
• Pooled data used for mapping
• Type 1 n=286; Type 2 n=2755
19/04/23 © The University of Sheffield
Characteristic Type 1 Type 2
M (SD) Range M(SD) Range
Age 59.65 (15.62) 18-93 66.19 (11.32) 26-98
Male 38.46% 60.87%
Diabetes related health complications 59.44% 38.05%
Other health complications 78.32% 79.79%
EQ-5D index (pooled) 0.60 (0.37) -0.59 to 1 0.65 (0.32) -0.43 to 1
SF-6D index (pooled) 0.66 (0.16) 0.35 to 1 0.69 (0.16) 0.35 to 1
DHP-18 Psychological distress (pooled) 28.16 (24.7) 18.61 (20.7)
DHP-18 Barriers to activity (pooled) 35.58 (21.2) 21.90 (19.4)
DHP-18 Disinhibited eating (pooled) 36.43 (23.2) 35.78 (22.8)

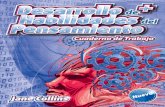
Results: Measure distributions
19/04/23 © The University of Sheffield
05
10
15
20
25
Pe
rcen
t
-.6 -.4 -.2 0 .2 .4 .6 .8 1EQ5Dindex
05
10
15
20
25
Pe
rcen
t
-.6 -.4 -.2 0 .2 .4 .6 .8 1EQ5Dindex
05
10
15
20
25
Pe
rcen
t
-.6 -.4 -.2 0 .2 .4 .6 .8 1SF6D
05
10
15
20
25
Pe
rcen
t
-.6 -.4 -.2 0 .2 .4 .6 .8 1SF6D
EQ-5D type 2
SF-6D type 2
EQ-5D type 1
SF-6D type 1

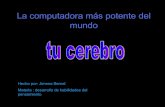
Model specifications: EQ-5D
19/04/23 © The University of Sheffield
• RE GLS model 7 (DHP-18 items, items squared, age and gender) performed best
Actual vs. predicted utility values
Actual vs. predicted utility values
• Type 1 (R2: 0.50) Type 2 (R2: 0.29) Mean absolute error Mean absolute error

Model specifications: SF-6D
19/04/23 © The University of Sheffield
Actual vs. predicted utility values (type 1)
Actual vs. predicted utility values (type 2)
• RE GLS model 7 (DHP-18 items, items squared, age and gender) performed best• Type 1 (R2: 0.65) Type 2 (R2:
0.40)

Discussion (1)
• Mapping an increasingly popular method for deriving utility scores
• EQ-5D and SF-6D utility scores can now be estimated for type 1 and type 2 diabetes
• GLS model 7 (DHP-18 items, squared item scores and demographics) performed best
• Type 1 predictions perform better than type 2 predictions
• SF-6D predictions perform better than EQ-5D predictions
• Over predicts utility for severe states and under predicts utility for mild states
19/04/23 © The University of Sheffield

Discussion (2)
• Using mapped values is second best to the direct inclusion of generic measures
• Lack external validity if not validated on external sample
• Using mapped values increases the error of the estimates
• How can mapping function precision be improved?
• Analyses using predicted values should consider the precision of the estimates.
19/04/23 © The University of Sheffield

Any questions?
Mapping algorithms available at: www.diabeteshealthprofile.com
19/04/23 © The University of Sheffield