Mapping and Comprehensive Assessment of Blood Transfusion ... · PDF fileMapping and...
35
Mapping and Comprehensive Assessment of Blood Transfusion Services in Nepal REPORT: 2011
-
Upload
nguyendiep -
Category
Documents
-
view
225 -
download
3
Transcript of Mapping and Comprehensive Assessment of Blood Transfusion ... · PDF fileMapping and...
Mapping and Comprehensive Assessment of
Blood Transfusion Services in Nepal
REPORT: 2011
ii
Acknowledgements
National Technical Advisory Committee Dr Geeta Shakya, Chairperson, Director, NPHL
Prof Dr HG Shrestha, Dean, Janaki Medical College
Prof Dr RP Singh, Clinical Haematologist
Dr Ashok Joshi, HOD, Dept. of Pathology, Bir Hospital
Dr SN Jha, In‐charge Pathology, Koshi Zonal Hospital
Dr Lata Bajracharya, Director, Maternity Hospital
Dr Ramesh Kharel, Director, National Centre for AIDS and STD Control
Dr Manita Rajkarnikar, Director, Central BTS Centre, Nepal Red Cross Society
Mr MB Joshi, President, Blood Donors Association of Nepal
Dr BR Marasini, Senior Health Administrator, MoHP
Dr Mukunda Sharma, Member Secretary, Co‐Chief Consultant Pathologist, NPHL
WHO‐HQ Dr Neelam Dhingra, Coordinator, Blood Transfusion Safety
WHO Nepal Dr Lin Aung, WHO Representative
Dr Nihal Singh, Medical Officer
Dr Prakash Ghimire, National Professional Officer Blood Safety & Laboratory
National Consultants Dr Palpasa Kansakar
Mr Anil Maharjan
All Central, Regional, District, Emergency and Hospital based Blood Transfusion Service Centres that participated in the study.
All those who provided help during field visits and workshops to finalize this report.

iii
Acronyms
BLODAN Blood Donor’s Association of Nepal
BTSC Blood Transfusion Service Centre
CBTSC Central Blood Transfusion Service Centre
CDR Central Development Region
CEOC Comprehensive Emergency Obstetric Care
DBTSC District Blood Transfusion Service Centre
DPHO District Public Health Office
EBTSC Emergency Blood Transfusion Service Centre
ELISA Enzyme Linked Immunosorbent Assay
EDR Eastern Development Region
EQAS External Quality Assessment Scheme
FFP Fresh Frozen Plasma
FWDR Far‐Western Development Region
GoN Government of Nepal
HBV Hepatitis B Virus
HCV Hepatitis C Virus
HIV Human Immunodeficiency Virus
HMG His Majesty’s Government
KOICA Korean International Cooperation Association
MWDR Mid‐Western Development Region
NBA National Blood Authority
NBP National Blood Policy
NCASC National Centre for AIDS and STD Control
NPHL National Public Health Laboratory
NRCS Nepal Red Cross Society
NRL National Reference Laboratory
NTAC National Technical Advisory Committee
MBOS Maximum Blood Ordering Schedule
MOHP Ministry of Health and Population
MOU Memorandum of Understanding
OFID OPEC Fund for International Development
PRP Platelet Rich Plasma
RBTSC Regional Blood Transfusion Service Centre
SOP Standard Operating Procedure
TTI Transfusion Transmissible Infection
TUTH Tribhuvan University Teaching Hospital
UNDP United Nations Development Programme
VNRBD Voluntary Non‐remunerated Blood Donation
WDR Western Development Region
WHO World Health Organization
iv
Contents
Acknowledgements ii
Acronyms iii
1 Introduction and Background 6
2 Objectives 9
3 Methodology 10
3.1 Pre‐visit activities 10
3.2 Field visit and data collection 10
3.3 Data analysis and report writing 11
4 Results 12
4.1 Assessment of Blood Centres 12
4.1.1 Types of blood centre assessed 12 4.1.2 Geographical distribution 12 4.1.3 Number of hospitals served by BTSCs 12 4.1.4 Management and regulation 13 4.1.5 Financial resources and support to BTSCs 13 4.1.6 Quality system 13 4.1.7 Human resources and training 13 4.1.8 Equipment and supplies 14 4.1.9 Procurement system 14 4.1.10 Health and safety 15 4.1.11 Basic infrastructure and facilities 15 4.1.12 Donor recruitment, screening and blood collection 15 4.1.13 Screening for transfusion transmissible infections 16 4.1.14 Blood group serology and compatibility testing 16 4.1.15 Blood component preparation 17 4.1.16 Blood storage, transfusion, inventory and distribution 17
4.2 Assessing transfusion process & clinical use of blood in hospital facilities 18
4.2.1 Assessing policy & management at central administrative level 18
4.3 District responses regarding need for BTSCs 19
5 Discussion 20
6 Recommendations 22
7 Action plan 23
v
Figure
Figure 1: Geographical distribution of Blood Transfusion Service Centres in Nepal 8
Tables
Table 1: Types of BTS centre 12
Table 2: Staff trained at national / international workshops / courses 14
Table 3: List of centres providing component services 17
Table 4: Total supply of blood and blood products by level of blood centre 17
Annexures I (a): List of BTS centres assessed (location, GPS, respondents, contact number) 24 I (b): List of BTSCs not involved in the study 28 I (c): List of districts without BTS facility 29 I (d): District responses regarding need of BTSCs in 12 districts 30 II: Composition of National Steering Committee (NSC) 34 III: Composition of National Technical Advisory Committee (NTAC) 35
6
1 Introduction and Background Nepal remains among one of the poorest and least developed countries in the world with almost one‐third of its population of 29.3 million living below the poverty line (Ministry of Finance, 2006). The per capita income for 2009 was approximately $ 427 (World Bank, fiscal year 2009). The life expectancy rate was 60.1 for males and 60.7 for females (Census 2001). The highest risk group for poor health remains children under five (particularly girls) and females of reproductive age. Three main factors that negatively impact state of health in Nepal are the high rate of poverty, illiteracy, and physical geography. Poor literacy compounds the health status of a population as preventive health care measures, control of communicable diseases, and nutritional programmes are based on education level. With 80% of the population living in rural areas, there is a lack of distribution not only of medicine and medical supplies, but other essential health care needs. Millions of people are at risk of various infections and thousands die every year due to communicable diseases, malnutrition and other health‐related problems, especially those living in rural areas. According to a 1996 report (Nepal Living Standard Survey), only 41% of households have access to a health facility within a walking distance of 30 minutes. The maternal mortality rate in Nepal is 281/100 000 live births, which is amongst the highest in the world, and accounts for 18% of total female deaths. Globally, more than 80% of maternal deaths occur due to haemorrhage, infection, unsafe abortion, eclampsia, and obstructed labour. About 61% of these maternal deaths occur in the post‐partum period, more than half of which take place within the first day of delivery. Blood transfusion has been identified as one of the life‐saving interventions and has an essential role in patient treatment and management. The Blood Transfusion Service (BTS) should be available in all health care facilities providing Comprehensive Emergency Obstetric Care (CEOC). Access to a safe and sufficient blood supply could help to prevent the death of a significant number of mothers and their newborn infants each year.
BTS is one of the priority programmes of the Government of Nepal (GoN). In Nepal, the Nepal Red Cross Society (NRCS) began to provide institution‐based BTS through the Department of Pathology at Bir Hospital in 1964 and the first BTS was established as Laxmi Blood Bank in 1966. In recognition of the pioneering and long service of NRCS, His Majesty’s Government of Nepal (HMG/N) mandated NRCS as the sole agency to conduct the blood programme in Nepal in March 1992. A national policy on BTS was developed and approved by HMG/N through a cabinet decision in 1993. The mission statement of Nepal’s blood programme is to ensure an adequate, safe and timely supply of blood and blood products to meet the transfusion requirements of the people of Nepal in an equitable and affordable manner. The guiding principles which govern Nepal’s BTS are as follows:
The collection of blood is based on voluntary non‐remunerated blood donation.
The provision of blood and blood products must be on a non‐profit basis.
No harm should be caused to the donors or recipients of blood and blood products.
Every citizen of Nepal who needs blood or blood products as recommended by the treating
physician in any health care facility in Nepal should have equal, prompt and affordable access to
blood and blood products.
The partnership between the Ministry of Health & Population (MOHP) and NRCS for blood donor
recruitment, collection, processing, storage, supply and overall management for the provision of
safe blood is vital and must therefore be strengthened at all levels; central, regional, districts,
and smaller, by the formation of joint committees as guided by a regulatory body.
7
National blood service standards must ensure that products and services conform to high quality
standards.
Blood transfusion is a medical intervention that should be indicated and prescribed by medical
practitioners registered with the Nepal Medical Council.
The rights and duties of blood donors, staff of the blood programme, patients and physicians
should be observed.
Minimum wastage of blood should be ensured through effective supply and demand
management.
The National Blood Authority (NBA) should develop an appropriate legal framework for the
enforcement of provisions of the National Blood Policy.
During the initial years, BTS in Nepal was available only in Kathmandu but over the years, it has been expanded to 70 BTS Centres (BTSC) in 50 of the 75 districts of the country. Of these 70 centres, one is functioning as NRCS Central BTS Centre (CBTSC), 4 as NRCS Regional BTS Centres (RBTSC) and 21 as NRCS District BTS Centres (DBTSC), delivering a fully‐fledged BTS. In addition, there are 19 BTSC operating as emergency service units and 25 hospital based centres, based at various government and private hospitals, functioning full time. The supply of safe and adequate blood and blood products has remained one of the main goals of the National Blood Programme. Commercial blood donation is banned and blood collection is mainly through voluntary non‐remunerated blood donation (VNRBD). About 85% of blood is collected from VNRBD and the remaining 15% from replacement donors. In 2009/10, a total of 156 278 units of blood were collected which is approximately 0.62% of the total population of the country. According to World Health Organization (WHO) recommendations, at least 2% of the population is required to donate blood to meet the basic transfusion needs of a country, indicating a need to strengthen the VNRBD programme in Nepal. Component separation accounts for 26.5% of total collections and 210 215 units of blood components were supplied in 2009/10. The provision of safe and efficacious blood and blood components for transfusion or manufacturing purposes involves a number of processes, from selection of blood donors and blood collection, processing and testing of donated units to testing of patient samples, issue of compatible blood and its administration to the patient. There is a risk of error at each link in this “transfusion chain” and a failure at any of these links can have serious implications for the donor or the recipients of the blood and blood products. Thus, while blood transfusion can be life‐saving, there are also associated risks, particularly the transmission of blood‐borne infections. One of the key aspects of blood safety is implementation of a quality management system at all stages of the transfusion chain. Quality assurance along the entire length of the transfusion chain, from collection to transfusion, is vital for safeguarding the life of patients receiving blood. WHO has recommended an integrated strategy for a safe and adequate blood supply which includes establishment of a well‐organized and nationally coordinated BTS; collection of blood from VNRBD using stringent donor selection criteria; testing and good laboratory practice in all aspects of the preparation of blood and blood products for use; reduction of unnecessary blood transfusions through appropriate clinical use of blood; and implementation of an effective quality management system in all areas. However, in Nepal, owing to limited infrastructure and resources, and an inadequate number of well‐trained staff and limited implementation of a quality assurance system in BTS, the quality of the service provided is compromised. Although all blood units are screened for transfusion transmissible infections (TTI), i.e. HIV, HBV, HCV, and syphilis, different assays of variable sensitivity and specificity are in use at BTSCs

8
in the absence of a specific, nationally approved list of kits/assays. However, most BTSCs claim to use WHO recommended kits for TTI screening. In order to run the BTS in an efficient manner and to enhance the quality of service with long‐term sustainability, long‐term planning is crucial. In 2009, in order to strengthen the capacity of the BTS in Nepal, GoN/ MOHP, in close coordination with the National Public Health Laboratory (NPHL) and NRCS, developed a five‐year national strategic plan (2009‐2013) for safe BTS. This national strategy document is expected to serve as a blueprint for implementation. In order to upgrade the current capacities of BTS in Nepal, it is important to assess the basic infrastructure and technical competency of existing human resources of BTSCs and hospitals offering transfusion services in Nepal. Such assessment will provide baseline data and identify gaps related to the implementation of recommended standards on blood safety. Hence, this comprehensive study was carried out to gather information on the policy, organization, management, and technical aspects of BTSCs in the country. Laboratory practices on screening for TTIs, blood group serology, compatibility testing, blood component preparation and maintenance of cold chain during the collection, storage, packaging, transportation and distribution, were also assessed. Despite the presence of a BTSC in 50 districts of Nepal (Figure 1), BTS facilities are still lacking in the remaining 25 of the 75 districts. Hence, assessment of the need for BTS facilities in those 25 districts was also conducted to help plan for expansion of new BTSCs in the country. Figure 1: Geographical distribution of Blood Transfusion Service Centres in Nepal
9
2 Objectives
The study was carried out with the following objectives:
Map the number and category of BTSCs and hospital facilities providing BTS in the country.
Review the existing status of blood centres in terms of infrastructural facilities, human
resources, managerial and technical aspects.
Establish baseline data for the national BTS, as of 2010.
Identify gaps between current practices and recommended standards.
Limitations of the study
The study team planned to collect questionnaire‐based data from all 70 BTSC, currently existing
in 50 of the 75 districts of the country. However, only 61 centres responded; the remainder,
whose questionnaires were delivered by courier, did not respond.
Responses to some of the questions posed, such as sufficiency of necessary equipment and staff,
were based entirely on the assumptions/ perceptions of respondents.
Supporting literature in relation to the study was limited.
Responses to some questions could not be produced by respondents due to lack of proper
documents or records.
Seven blood centres that were in the process of becoming established (Dhading BTSC; Dhankuta
BTSC; Sarlahi BTSC; Hospital based BTSC at AMDA Hospital, Damak; Bajhang BTSC; Hospital
based BTSCs at Kathmandu Institute of Science and Technology Medical College; and Lumbini
Medical College) could not be included in the study.
Operational Definitions Stand‐alone blood centre: A blood centre which is located within/outside the hospital premises; however, its day‐to‐day operational management is independent from the hospital management committee. Hospital based blood centre: A blood centre which functions as one of the units or is a part of laboratory services within the hospital and operates under the hospital management system.
10
3 Methodology
An assessment team consisting of two consultants (Dr Palpasa Kansakar and Mr Anil Maharjan) was formed to map existing BTSCs and perform a comprehensive assessment of existing BTSCs, adapted the WHO FRAME tool. This team worked in close coordination with the Director NPHL; Member Secretary of NTAC; Director, CBTS; and the National Professional Officer, WHO Nepal. 3.1 Pre‐visit activities The following activities were carried out before assessing BTSCs:
Adaptation of WHO structured FRAME tool to collect information on the capacity of existing
BTSCs, transfusion practice at hospitals, and available policy/ guidelines/ SOPs for BTS and
organizational management at NPHL/CBTSC.
Identification of 70 BTSCs in five regions of the country and scheduling of visits to these centres.
Prior to visits to the BTSCs, the sending of a letter from NPHL/ NRCS, together with the survey
questionnaire, to all centres to notify them of the objectives of the study and enable them to
prepare/ collate information needed.
Twenty five of 75 districts do not have a BTSC [Annex I (c)]. For these, a letter enquiring about
the need for a BTS was sent to respective NRCS district chapters and District Public Health
Offices (DPHO).
3.2 Field visit and data collection The team surveyed 70 BTSCs located in 50 districts of Nepal using the WHO FRAME tool. The information provided is based on BTS data for 2010. The data/information from BTSCs was gathered using the following approaches:
The relevant sections of the questionnaire were sent to the BTSC by courier; all accessible BTSCs
were visited by the consultants, and the data was gathered by means of the following:
- BTSC personnel were interviewed. - On‐site observation by consultants to verify information provided.
For those BTSCs where study team members could not visit in person due to difficult
geographical location and non‐availability of transportation (hilly and mountainous where blood
collection, processing and distribution is minimal and access by team members was limited due
to topography/ environmental factors), information was gathered by telephonic interview with
local blood bank technicians.
The choice of data acquisition, either through direct on‐site visit to the BTSC or interviewing by
means of telephonic communication, was based on the transportation accessibility of the site.
11
The study team also conducted an on‐site survey using the WHO FRAME tool to acquire information on transfusion practices at selected health care facilities without a blood bank but which provide a transfusion service (Kathmandu Model Hospital and Star Hospital in Kathmandu, Bhim Hospital in Rupandehi and Koshi Zonal Hospital in Biratnagar). Assessment of transfusion practice was also carried out at selected health care facilities with a blood bank (Nepal Medical College and Shahid Gangalal Heart Centre in Kathmandu). To assess the need for a BTS in districts without a facility, letters enquiring about the available health care facilities in the districts and their need for a BTS were sent by the Director, NPHL to the respective NRCS District Chapters and DPHO. The expected respondents were as follows:
For BTSCs: BTSC in‐charge/ NRCS authorities
For health care facilities: Medical superintendent/ surgeon/ nurse / pathologist/ BTSC in‐charge.
3.3 Data analysis and report writing Data entry was done using Microsoft Access Software made available by WHO Nepal and the analysis was done using SPSS and Microsoft Excel. Analysed data were tabulated and presented in narrative report form.
12
4 Results
4.1 Assessment of Blood Centres
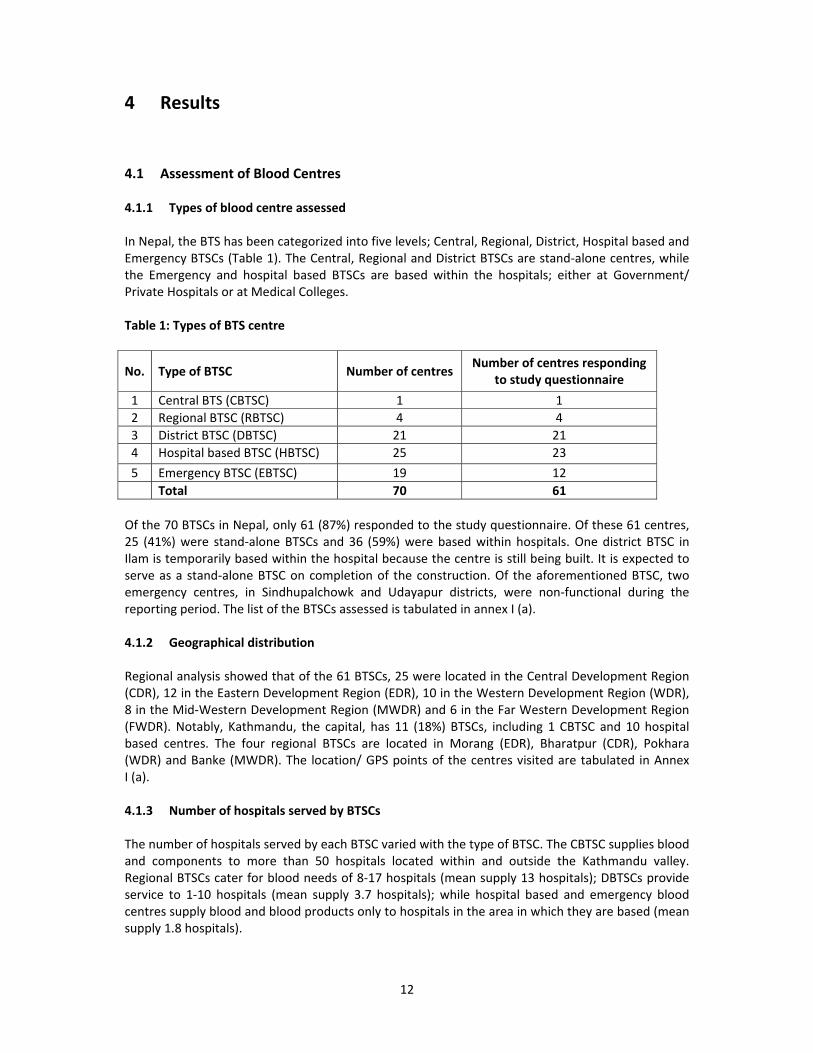
4.1.1 Types of blood centre assessed In Nepal, the BTS has been categorized into five levels; Central, Regional, District, Hospital based and Emergency BTSCs (Table 1). The Central, Regional and District BTSCs are stand‐alone centres, while the Emergency and hospital based BTSCs are based within the hospitals; either at Government/ Private Hospitals or at Medical Colleges. Table 1: Types of BTS centre
No. Type of BTSC Number of centres Number of centres responding
to study questionnaire
1 Central BTS (CBTSC) 1 1
2 Regional BTSC (RBTSC) 4 4
3 District BTSC (DBTSC) 21 21
4 Hospital based BTSC (HBTSC) 25 23
5 Emergency BTSC (EBTSC) 19 12
Total 70 61
Of the 70 BTSCs in Nepal, only 61 (87%) responded to the study questionnaire. Of these 61 centres, 25 (41%) were stand‐alone BTSCs and 36 (59%) were based within hospitals. One district BTSC in Ilam is temporarily based within the hospital because the centre is still being built. It is expected to serve as a stand‐alone BTSC on completion of the construction. Of the aforementioned BTSC, two emergency centres, in Sindhupalchowk and Udayapur districts, were non‐functional during the reporting period. The list of the BTSCs assessed is tabulated in annex I (a). 4.1.2 Geographical distribution Regional analysis showed that of the 61 BTSCs, 25 were located in the Central Development Region (CDR), 12 in the Eastern Development Region (EDR), 10 in the Western Development Region (WDR), 8 in the Mid‐Western Development Region (MWDR) and 6 in the Far Western Development Region (FWDR). Notably, Kathmandu, the capital, has 11 (18%) BTSCs, including 1 CBTSC and 10 hospital based centres. The four regional BTSCs are located in Morang (EDR), Bharatpur (CDR), Pokhara (WDR) and Banke (MWDR). The location/ GPS points of the centres visited are tabulated in Annex I (a). 4.1.3 Number of hospitals served by BTSCs The number of hospitals served by each BTSC varied with the type of BTSC. The CBTSC supplies blood and components to more than 50 hospitals located within and outside the Kathmandu valley. Regional BTSCs cater for blood needs of 8‐17 hospitals (mean supply 13 hospitals); DBTSCs provide service to 1‐10 hospitals (mean supply 3.7 hospitals); while hospital based and emergency blood centres supply blood and blood products only to hospitals in the area in which they are based (mean supply 1.8 hospitals).

13
4.1.4 Management and regulation NRCS has been mandated by the GoN to conduct all programmes related to blood transfusion in Nepal. Hence, all BTSCs operating in the country were required to sign a Memorandum of Understanding (MOU) with NRCS/CBTSC before initiating the service.
4.1.5 Financial resources and support to BTSCs The funding source for operation of most BTSCs is primarily based on a cost recovery system (75%), with some additional support from NRCS, National Societies of International Red Cross and External Development partners. The estimated budget for the 2009/2010 operation of CBTSC was NPR 40 000 000 (i.e. US$ 555 555.55 using US$ 1 to NPR 72). Of this budgetary requirement, 75% was collected through cost recovery acquired through screening service charges from patients requiring blood, 12.5% from external developmental partners (International Organizations including WHO and UNDP) and the remaining 12.5% from external donors (Luxembourg and other International Red Cross Societies). Operating budget for RBTSC ranges from NPR 5.4‐14.5 million per annum, with a mean budget of NPR 8.3 million, and the source of funding was based solely on cost recovery. Information on annual budget was available for only 11 DBTSCs and their operating budget was approximately NPR 1.85 million/annum (range NPR 0.4‐6 million). Financial information was available for only 17 DBTSCs, of which 9 reported to operate at a total cost recovery basis and 8 DBTSCs operated at 85% cost recovery basis. Overall, 83% of funding for DBTSCs was from cost recovery. Government funding was not provided to stand‐alone BTSCs except for the DBTSC in the Bardiya district where a part of the staff salary was supported by the District Development Committee. Among the hospital based blood banks, 8 were based at medical colleges or private hospitals, 16 were based at non‐government/ non‐profit organizations and the operational cost of such BTSCs came partly from cost recovery and partly from NRCS and hospital support. For some BTSCs based at government hospitals (number =13), a part of the funding (e.g. cost of staff salary, space and other facilities such as power/water supply) was supported either by the hospital’s development board or directly by the government.
4.1.6 Quality system BTSCs are expected to implement a quality system as stated in the National Guidelines for BTS Management in Nepal. However, the quality policy document has not yet been developed. Only 22 centres have delegated a person responsible for quality management. Fifty seven centres have SOPs (developed by CBTSC) for blood donor recruitment and selection, blood collection and donor care, component preparation, TTI screening and blood group serology. Three centres do not have SOPs for blood storage, transportation and BTS waste management. Only 30 (50%) out of 61 centres have an individual responsible for data management. Records of donor recruitment and selection, blood collection and donor care were maintained by only 48, 51 and 54 centres respectively. Almost all centres, i.e. 58/61 (95%), maintained records of laboratory tests for TTI screening and blood group serology. 4.1.7 Human resources and training Considering that blood transfusion is an important, lifesaving and emergency service, an adequate number of well‐trained staff is essential to operate a BTSC with a 24‐hour service. Existing man‐power in CBTSC includes 2 medical officers, 12 nurses, 1 donor recruiter, 14 laboratory personnel and 18 administrative support staff. Apart from some hospital based centres, most BTSC (number = 57) do not have a medical officer or doctor recruited for the purpose of the blood bank. The total number of technical and administrative supportive staff at RBTSC ranged from 7‐11 and 1‐3
14
respectively. In 9 centres (6 DBTSCs and 3 EBTSCs), there was only one member of staff for all blood bank related activities. Overall, the existing number of staff seemed inadequate to run a blood bank with a 24‐hour service. Of the total 216 technical staff working in BTSCs throughout the country, 149 received national training and attended workshops related to blood transfusion, while only 12 staff members received international training. The categorization of staff who received blood transfusion related training according to the type of BTSC is shown in Table 2. Table 2: Staff trained at national / international workshops / courses
Type of centre
BTS technical staff trained
National level training International level training
Numbers %
Numbers %
Actual Total Actual Total
CBTSC 14 14 100 9 14 64
RBTSC 33 37 89 4 37 11
DBTSC 43 51 84 1 51 2
EBTSC 12 18 67 0 0 0
Hospital based BTSC 47 96 49 7 97 7
Total 149 216 69 21 216 10
4.1.8 Equipment and supplies
- Equipment in BTSC
Assessment of available equipment in BTSCs revealed that CBTSC and RBTSCs were well equipped with most of the equipment listed in the questionnaire. Basic equipment like donor bed, weighing scale, sphygmomanometer, and refrigerator (either blood bank or domestic) was available in all blood banks though their number varied according to workload. However, lack of some basic equipment was also observed in some district and EBTSCs. For example, 3 BTSCs did not have a water bath, 36 did not have an Rh view box, 8 did not have a hot air oven, 12 did not have a thermometer and 11 did not have a blood bank refrigerator. Cold boxes for transportation of blood units were not available in 14 centres, mostly hospital based units, where mobile collection of blood is not practiced and transfusion is conducted in the health care facility located within or nearby the blood bank premises. Computers were available only in 20 BTSCs. Most centres (36/61, 59%) reported that the existing equipment in their centre was inadequate for their workload.
4.1.9 Procurement system
- Equipment
Almost all BTSCs use locally purchased equipment. However, 29 (48%) and 32 (52%) centres received equipment support also from CBTSC and international donor organizations respectively. Staff from 49 (80%) centres mentioned that they are given training on operating new equipment installed in the BTSC. Only 15 (25%) centres reported having an equipment maintenance programme.
15
- Reagents and other key supplies
Test kits and other key supplies for BTS operation such as blood bags, TTI kits, blood grouping reagents and laboratory items in most BTSCs (51/61, 84%) were procured locally through the respective NRCS district chapter. Supply through central level and/or upper level agencies was also reported by 20 (33%) centres. Only 14 (23%) centres evaluated the supply before procurement, using known local controls, and kits for procurement were selected based on recommendations made by CBTSC. Only 19 centres (31%) validated their key supplies. Forty‐nine (80%) centres maintained stocks of key supplies. No centre reported functional difficulties due to depletion of supplies during the study period.
4.1.10 Health and safety A programme on health and safety was in place at 17 (28%) centres. This included vaccination of staff, health insurance, and an allowance for laboratory hazards, medical leave, and hazard training.
4.1.11 Basic infrastructure and facilities All stand‐alone BTSCs have at least one separate room for BTS‐related activity. Of the 33 functional hospital based and EBTSCs located within government or private hospitals, 11 (33%) were operating as a separate unit or department in the hospital. The remaining 22 (67%) were operating as part of the hospital’s pathology or emergency laboratory. In 6/61 (10%) of BTSCs, respondents reported that available space in the centre was inadequate for donor selection, whereas 7/61 (11%) reported that premises were unsuitable for blood collection and 3 centres reported that premises were inadequate for blood processing, testing, storage and distribution. Facilities such as access to water and power supply, transportation system and telephone services were available in most centres (in >85%). However, frequent interruptions to power and/or water supply due to load shedding were reported by centres. Fax and internet access were available in only 56% and 36% of centres respectively. 4.1.12 Donor recruitment, screening and blood collection Of the 61 centres engaged in this study, 87% were involved in donor education, recruitment, pre‐donation counselling and blood collection and supply. All centres engaged in these activities claimed that staff members were trained. Three centres were not involved in any of the above‐mentioned activities during the study period. Most centres (44/61, 72%) do not have a specific budget for the donor programme. Promotional and educational materials for public awareness and educating blood donors on the importance of voluntary blood donation were in use at 43/61 (70%) of centres. All of these 43 centres also made use of materials developed by CBTSC. Three of 61 centres (5%) also used locally developed materials. Standardized criteria for donor suitability are used country‐wide. These include donor age, weight, haemoglobin level, medical history, menstruation cycle, and foreign visit history. All facilities involved in blood collection assessed donor suitability by means of a donor questionnaire, pre‐donation interview and physical examination. Estimating the haemoglobin level of donors was not routinely done; only when physical examination indicated the need. Haemoglobin estimation was done either by the copper sulphate or cyan‐methemoglobin method, or by using a haemoglobinometer.
16
Records in the donor database were maintained by 53/61 (87%) of centres and manual entry was most frequently practiced. Only two (3%) centres maintained data in electronic format. Blood collection at centres varied from 9‐60,000 units/annum. Blood collection at CBTSC and RBTSCs was mainly from VNRBD (85%), while replacement donations accounted for 15% of collections. Blood collected from VNRBD in DBTSCs accounted for 77% and the remaining 23% was collected from replacement donations. However, in hospital based centres and EBTSCs, collection from VNRBD was 55‐67%, while replacement donations accounted for 45‐33%. No evidence exists to suggest that blood collection facilities pay donors. The age range of blood donors was 18‐60 years and the majority of donors (approximately 85%) were male. Data on donors by their type; e.g. new or regular, was not maintained at any centre. Most centres practiced one standard volume collection (350 ml), whereas those involved in component preparation (8 centres) also practiced 400/450 ml collection. One centre, based at the Paediatric Hospital (Kanti Children’s Hospital, Kathmandu), also used 100 ml paediatric blood bags. All centres used sterile, single‐use plastic bags for blood collection. Apheresis collection was not practiced at any centre. Only one centre reported autologous collection (one collection in the reported period). Systems for donor feedback and complaints were in place in 40/61 (66%) of centres. Sixteen centres reported having a system of follow‐up for seroreactive donors. 4.1.13 Screening for transfusion transmissible infections Screening of donated blood for TTIs including HIV I & II, Hepatitis B & C and syphilis, was carried out universally. There was no evidence that collected blood units were issued without TTI testing during the study period. Only 3 centres mentioned using the national algorithm for TTI screening. However, this algorithm is intended for laboratory diagnosis of HIV, developed by the National Centre for AIDS and STD Control (NCASC). A national algorithm for TTI screening of donated blood is yet to be developed. Most blood centres used rapid test methods to screen for TTI markers, while only four centres used both rapid and ELISA techniques. Since rapid techniques were used routinely in most centres, inclusion of control samples with each test run was not practiced. Controls were included only when testing a large number of samples, e.g. testing blood units collected from mobile camps. There was no external quality assessment scheme (EQAS) at national level for TTI testing. Only CBTSC participated in an EQAS at international level with the National Reference Laboratory, (NRL) Australia. The overall prevalence of HIV among blood donors was 0.08%; HBV was 0.36%, HCV was 0.25% and syphilis was 0.15%. Regarding TTI positive cases, all centres confirmed samples with repeated tests using a different assay and most centres were also involved in providing counselling services and referring donors to referral laboratories for further investigation and confirmation. . 4.1.14 Blood group serology and compatibility testing ABO and Rh grouping was done using slide and tube techniques. Apart from CBTSC which participated in the international EQAS of the NRL, Thailand, there was no EQAS programme in blood grouping at a national level for BTS. The number of cross matches performed at CBTSC during the reporting period was 36 923. For RBTSCs, the annual number of cross matches performed ranged from 7 000‐18 623 (mean=12,703). Cross matches performed annually at DBTSCs varied from 10‐12 560 (mean=1 874), at EBTSCs from 18‐1 678 (mean=238) and at hospital based BTSCs from 13‐13 662 (mean=2 928).
17
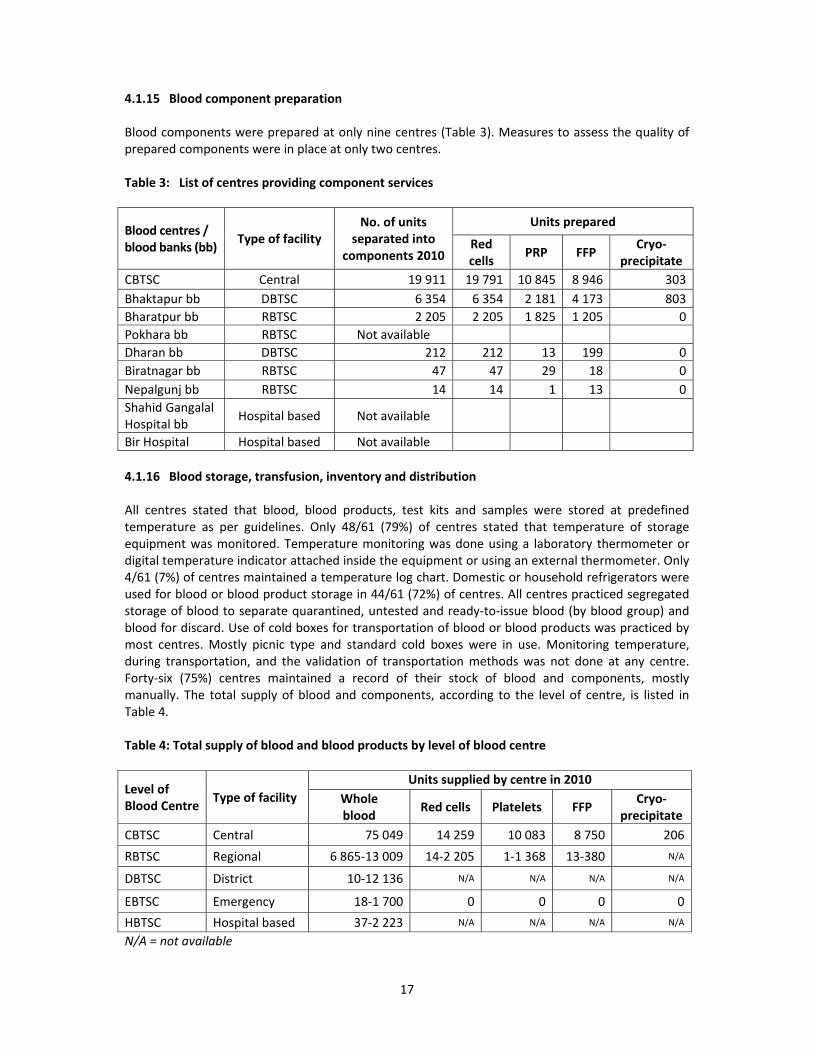
4.1.15 Blood component preparation Blood components were prepared at only nine centres (Table 3). Measures to assess the quality of prepared components were in place at only two centres. Table 3: List of centres providing component services
Blood centres / blood banks (bb)
Type of facility No. of units
separated into components 2010
Units prepared
Red cells
PRP FFP Cryo‐
precipitate
CBTSC Central 19 911 19 791 10 845 8 946 303
Bhaktapur bb DBTSC 6 354 6 354 2 181 4 173 803
Bharatpur bb RBTSC 2 205 2 205 1 825 1 205 0
Pokhara bb RBTSC Not available
Dharan bb DBTSC 212 212 13 199 0
Biratnagar bb RBTSC 47 47 29 18 0
Nepalgunj bb RBTSC 14 14 1 13 0
Shahid Gangalal Hospital bb
Hospital based Not available
Bir Hospital Hospital based Not available
4.1.16 Blood storage, transfusion, inventory and distribution All centres stated that blood, blood products, test kits and samples were stored at predefined temperature as per guidelines. Only 48/61 (79%) of centres stated that temperature of storage equipment was monitored. Temperature monitoring was done using a laboratory thermometer or digital temperature indicator attached inside the equipment or using an external thermometer. Only 4/61 (7%) of centres maintained a temperature log chart. Domestic or household refrigerators were used for blood or blood product storage in 44/61 (72%) of centres. All centres practiced segregated storage of blood to separate quarantined, untested and ready‐to‐issue blood (by blood group) and blood for discard. Use of cold boxes for transportation of blood or blood products was practiced by most centres. Mostly picnic type and standard cold boxes were in use. Monitoring temperature, during transportation, and the validation of transportation methods was not done at any centre. Forty‐six (75%) centres maintained a record of their stock of blood and components, mostly manually. The total supply of blood and components, according to the level of centre, is listed in Table 4. Table 4: Total supply of blood and blood products by level of blood centre
Level of Blood Centre
Type of facility
Units supplied by centre in 2010
Whole blood
Red cells Platelets FFP Cryo‐
precipitate
CBTSC Central 75 049 14 259 10 083 8 750 206
RBTSC Regional 6 865‐13 009 14‐2 205 1‐1 368 13‐380 N/A
DBTSC District 10‐12 136 N/A N/A N/A N/A
EBTSC Emergency 18‐1 700 0 0 0 0
HBTSC Hospital based 37‐2 223 N/A N/A N/A N/A
N/A = not available

18
A practice is in place for accepting back into stock, blood units unused after issue, within a week of issue. Re‐issue of such blood units was done only after checking that the units had not reached expiry date, and that there was no evidence of leakage, haemolysis, or signs of contamination. Most centres claimed that since the blood bank is in close proximity to the hospital, blood is issued only when needed and rarely returned to the blood bank. The total number of blood units that had to be discarded for various reasons at CBTSC was approximately 5‐7% of collections. Blood units discarded at RBTSCs varied from 241‐1 000 units/annum and at DBTSCs from 2‐275 units/annum. The reasons for discard were mainly as a result of date expiry, TTI reactivity, low volume collection, haemolysis, contamination, improper storage of issued units in hospitals and more than one week after issue from the BTSCs, i.e. delayed return of unused blood from hospitals.
4.2 Assessing transfusion process & clinical use of blood in hospital facilities In this study, attempts to assess the transfusion process and clinical use of blood in seven health care facilities were made. For this, the Shahid Gangalal Heart Centre, Nepal Medical College, Kathmandu Model Hospital and Star Nursing Home located in Kathmandu (CDR), Koshi Zonal Hospital in Biratnagar (EDR), and Bhim Hospital in Rupandehi (WDR) were visited. All these hospitals issue blood to patients, but none has a well‐defined hospital transfusion committee. Documentation of transfusion‐related activities and maintaining records of patients receiving transfusion was not practiced. Hospital authorities stated that transfusion details could be traced only from individual patient charts and that collated data or records on annual transfusions at the hospital were not available. Hence, information as demanded by the study questionnaire on transfusion practice could not be obtained. However, based on verbal exchanges with some hospital authorities, departments most commonly utilizing blood and blood components were internal medicine, surgery and gynaecology and clinical conditions indicating a need for transfusion were aplastic anaemia, haematological and other malignancies, and childbirth. Requests for blood and blood products were made by attending clinicians. These hospitals had developed a format for blood and blood component requests, and prescription was done according to guidelines on the clinical use of blood. 4.2.1 Assessing policy & management at central administrative level
Information on policy and management of the BTS in Nepal was collected from MOHP/NPHL and CBTSC. In Nepal, the national policy on blood transfusion was developed and approved by the GoN in 1993 by a cabinet decision; revised in 2006. The main objective of the National Blood Policy (NBP) is to define the organizational, financial and legal measures that are taken to ensure a safe and adequate blood supply in an equitable manner. In this regard, a National Steering Committee (NSC), which is the most influential committee on blood safety, chaired by the Director General of Department of Health Services, was formed (Annex II) by MOHP. The committee is responsible for policy level decisions on regulation, blood collection, processing, storage and transfusion, import and export and overall management for the provision of safe blood and blood products in the country. Specific national legislation covering safety and quality of blood transfusion is in the process of development. The MOHP has identified NPHL as the focal point for blood transfusion safety on behalf of the GoN and has delegated the responsibility for overseeing blood transfusion‐related activities in the country. A panel of national experts was also constituted, namely the National Technical Advisory Committee (NTAC) under the NSC, to give advice on technical issues of BTS. The list of technical experts in the NTAC is shown in Annex III. The national guidelines on management of BTS in Nepal were developed in 2008 and provide guidance on management of BTS, selection of blood donors and blood donation criteria, setting recruitment goals, rational use of blood, quality assurance for BTS, accreditation programme and waste disposal. However, national protocols for issues related to blood usage, including clinical

19
indications for transfusion, standardized blood request form, maximum blood ordering schedules (MBOS), pre‐transfusion testing, and safe blood administration, are yet to be developed. The GoN mandated NRCS the sole responsibility to coordinate and conduct the national blood programme management in 1991. CBTSC currently also functions as the national centre for manage‐ment of BTS in Nepal. There is no specific annual financial support from the GoN for NBP. However, the GoN recognizes its responsibility to ensure an adequate supply of safe blood and blood products to meet transfusion requirements and commits to provide required support to NRCS. Various international organizations such as WHO, United Nations Development Programme (UNDP), OPEC Fund for International Development (OFID), Luxembourg Red Cross, Korean International Cooperation Association (KOICA) and Japanese Red Cross have also provided technical and/or financial support to strengthen BTS in Nepal. A cost recovery system for operation of BTSCs in the country covers only the material charge. The cost for processing a unit of whole blood from donor recruitment to testing, processing, storage and distribution was estimated to be approximately US$ 15; however BTSCs charge from US$ 9.5 to US$ 12/ unit of blood.
There is a system of mandatory registration of BTSCs in Nepal. Previously, centres were assessed by the CBTSC before being permitted to practise, and were required to sign a MOU with NRCS. After the approval of National Blood Transfusion Policy 2006, NPHL became involved in the assessment and monitoring of BTSCs and submits an assessment report to NTAC – based on the report submitted by NTAC – to start a BTS. There is a centralized report collection system for BTS and all BTSCs submit reports to CBTSC on a monthly and annual basis. There is also a system for bulk procurement of supplies such as blood bags, TTI kits, grouping reagents for BTSCs in selected districts and in CBTSC. CBTSC is involved in providing key supplies to some DBTSCs. CBTSC, in coordination with NPHL and WHO, also conducts national level training/workshops in blood safety related issues. BTS‐related training materials such as training hand books, training manuals, participant's guide and participant's log book were in place and developed through the support of Nepal Health Sector Support Programme 2. However, academic programmes in transfusion medicine, leading to the generation of experts in blood transfusion, are yet to be introduced.
4.3 District responses regarding need for BTSCs
Twenty‐five districts of the country do not have BTSCs. These districts are listed in Annex I (c). On enquiring about the need for a BTS facility in such districts, 12 centres stated that the establishment of a BTS facility would be of great support in delivering a quality health service. These districts included Bara, Rolpa, Bajhang, Khotang, Sindhuli, Bhojpur, Mugu, Sarlahi, Darchula, Tanahun and Kalikot. The translated responses from individual districts are listed in Annex I (d).
20
5 Discussion
Blood transfusion is an essential part of a modern health care delivery system. Therefore, a National Blood Programme plays an integral role in the national health system and health care policy. Proper infrastructural facilities, adequate equipment, timely supply of required reagents, quality control systems and skilled trained staff form the basis of a BTSC. An attempt to assess 70 blood centres located in 5 developmental regions of Nepal was made during the study, of which only 61 centres responded to the study questionnaire. Most centres assessed in this study maintained the abovementioned functions, while two of the 61 centres were non‐functional. Component preparation was done in only nine centres; a limited component facility could lead to an unnecessary demand for whole blood. Variations were observed among centres in respect of management, infrastructure status, human resources and extent of service provided. Basic standards for infrastructure, equipment and manpower required for different levels of BTSC need to be developed and the needs of other distant/ rural hospitals, with suboptimal access to BTSCs, should be addressed. There is currently no mechanism for the hierarchical role of NRCS, CBTSC and RBTSC over other BTSCs. In spite of all BTSCs operating in the country under the NRCS umbrella, all regional and district centres run autonomously in terms of day‐to‐day manage‐ment and provision of financial resources. A well‐defined nationwide collaborative mechanism among different stakeholders including MoHP, NRCS, stand‐alone and hospital based BTSCs, and hospitals (both in the public and private sector) are yet to be established. To improve the quality of service, there should be a system for monitoring and evaluating established as well as newly established centres for renewal and licensing respectively.
It was observed that the environment and work space in some BTSCs was inadequate. While space needs to be clean and organized, measures should be taken to make the area more inviting and comfortable for donors and visitors. Steps should be taken to make blood donation a pleasant experience so that donors are more likely to return as regular blood donors. Equipment (purchased or donated) was observed at all BTS facilities, and included models of various ages and condition. Moreover, most BTSCs contained one or more pieces of equipment in a non‐functional state. Staff training on the operation of any new equipment installed in the centre should be conducted. Staff members and/or maintenance staff should also be trained in routine preventive maintenance, calibration, and QC of equipment. Suppliers of equipment could be contracted to provide initial and ongoing support for equipment sold to BTSCs. There should be provision for ongoing technical support related to troubleshooting of equipment faults and assaying performance. Most centres have SOPs (developed and provided through CBTSC) for BTS‐related procedures. An SOP is necessary to perform tests in a uniform manner throughout all centres. It is advisable to review SOPs periodically and distribute updated SOPs to all centres, ensuring that outdated SOPs are removed from circulation. Different centres used different test kits/ assays for laboratory testing. WHO recommends national procurement guidelines for the blood programme, to provide for uniformity of test kits/reagents throughout a country. A system to validate test kits and reagents should be in place to ensure the quality of reagents used. In most centres, refrigerators/ freezers used for storage of blood and reagents were simple domestic refrigerators which did not have temperature‐monitoring systems. Monitoring of these storage devices was either inconsistent or non‐existent in most facilities visited. This creates concern about the provision of a quality service because units exposed to temperatures outside of the acceptable storage range, might compromise product quality. BTS facilities need to be provided with a high standard of blood and product storage equipment, and SOPs on their use and maintenance. There is a system for the manual recording for BTS data and activities in most facilities. These documents are broadly standardized, but the practice of documentation varied amongst individual institutions. Most facilities use a simple register to

21
summarize donor information and test results. The staff complement in some BTSCs seemed inadequate to run a blood centre on a 24‐hour basis. For centres with only one staff member to oversee all blood bank‐related activities, provision for an alternative or standby member on call should be made available, considering the emergency status of the service. Despite the limited number of staff in most BTSCs, the current human resources appeared to be trained and skilled to carry out their assigned work. However, staff should be offered career development initiatives such as opportunities for advanced diplomas, degrees and/or specialist training specific to transfusion medicine and technology. Such initiatives would help to retain trained staff in the BTS.
Information on the clinical use of blood in hospitals providing transfusion facilities could not be gathered as required by the questionnaire due to the lack of a defined hospital transfusion committee in the sites visited. A hospital transfusion committee should be in place at each hospital providing blood transfusions, in order to track transfusion‐related activities. As clinicians prescribe blood and blood products, coordinating with them and providing orientation on the appropriate clinical use of blood should be done to promote rational use of blood and components. It is advisable to develop and implement national blood transfusion protocols and transfusion reaction management guidelines for standardization and quality assurance of transfusion practice.
Periodic assessment and evaluation of the BTS is essential to upgrade the quality of service and ensure safe blood transfusion practices.
22
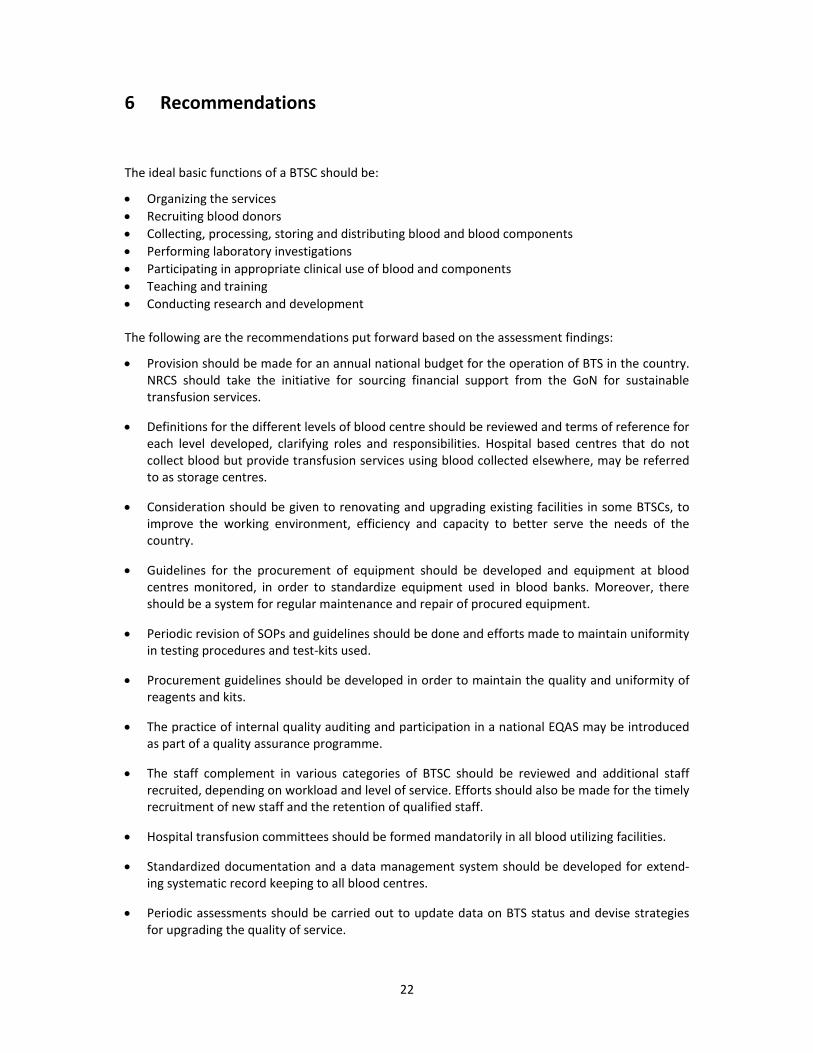
6 Recommendations
The ideal basic functions of a BTSC should be:
Organizing the services
Recruiting blood donors
Collecting, processing, storing and distributing blood and blood components
Performing laboratory investigations
Participating in appropriate clinical use of blood and components
Teaching and training
Conducting research and development The following are the recommendations put forward based on the assessment findings:
Provision should be made for an annual national budget for the operation of BTS in the country. NRCS should take the initiative for sourcing financial support from the GoN for sustainable transfusion services.
Definitions for the different levels of blood centre should be reviewed and terms of reference for each level developed, clarifying roles and responsibilities. Hospital based centres that do not collect blood but provide transfusion services using blood collected elsewhere, may be referred to as storage centres.
Consideration should be given to renovating and upgrading existing facilities in some BTSCs, to improve the working environment, efficiency and capacity to better serve the needs of the country.
Guidelines for the procurement of equipment should be developed and equipment at blood centres monitored, in order to standardize equipment used in blood banks. Moreover, there should be a system for regular maintenance and repair of procured equipment.
Periodic revision of SOPs and guidelines should be done and efforts made to maintain uniformity in testing procedures and test‐kits used.
Procurement guidelines should be developed in order to maintain the quality and uniformity of reagents and kits.
The practice of internal quality auditing and participation in a national EQAS may be introduced as part of a quality assurance programme.
The staff complement in various categories of BTSC should be reviewed and additional staff recruited, depending on workload and level of service. Efforts should also be made for the timely recruitment of new staff and the retention of qualified staff.
Hospital transfusion committees should be formed mandatorily in all blood utilizing facilities.
Standardized documentation and a data management system should be developed for extend‐ing systematic record keeping to all blood centres.
Periodic assessments should be carried out to update data on BTS status and devise strategies for upgrading the quality of service.
23
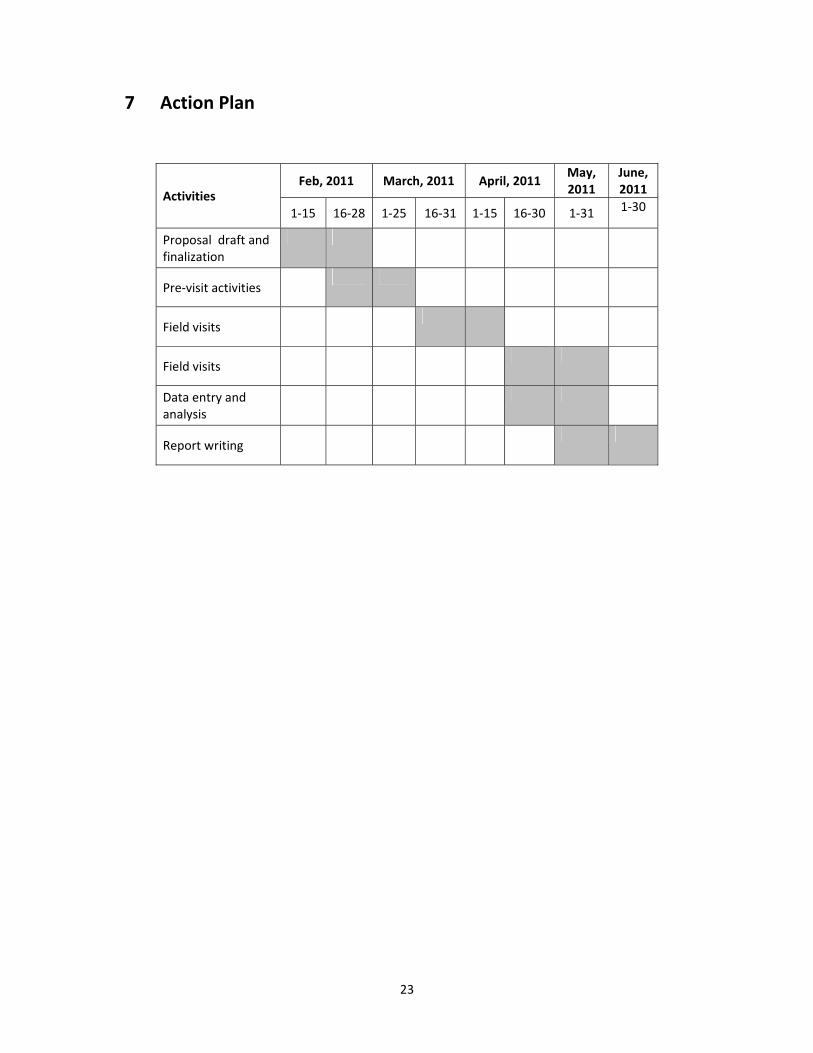
7 Action Plan
Activities Feb, 2011 March, 2011 April, 2011
May, 2011
June, 2011
1‐15 16‐28 1‐25 16‐31 1‐15 16‐30 1‐31 1‐30
Proposal draft and finalization
Pre‐visit activities
Field visits
Field visits
Data entry and analysis
Report writing

24
ANNEXURES
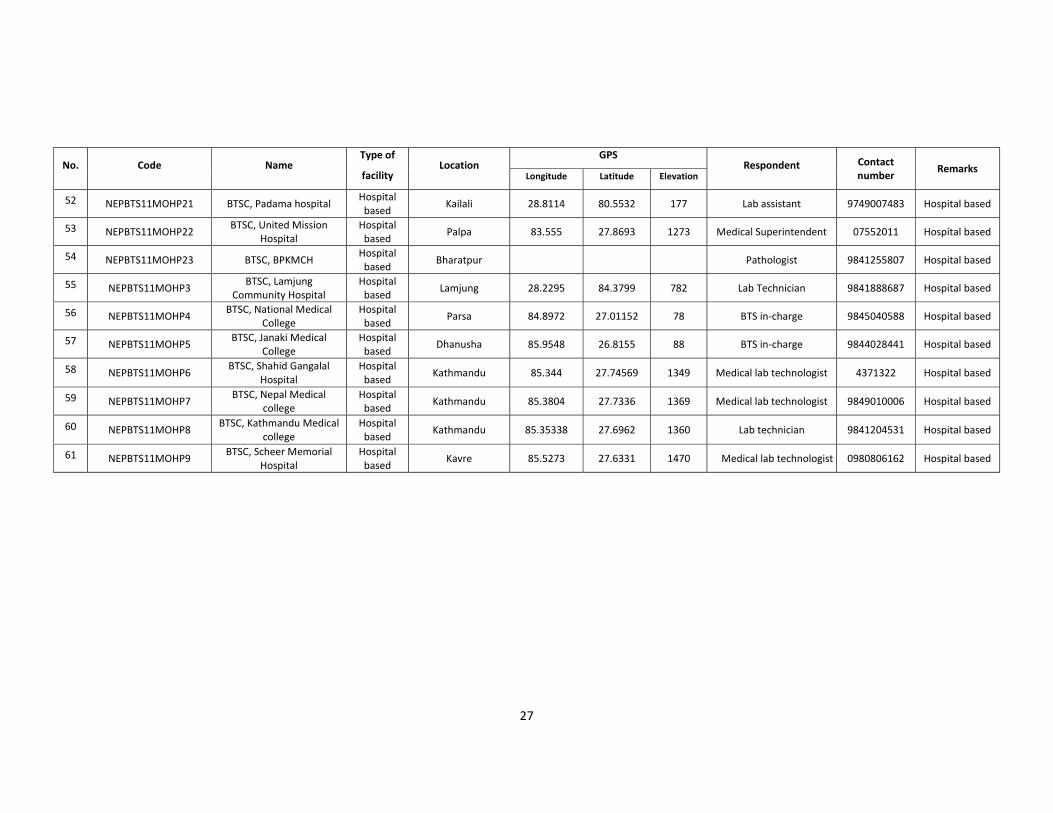
Annexure I (a): List of BTS centres assessed (location, GPS, respondents, contact number)
No. Code Name Type of
facility Location
GPS Respondent Contact
number Remarks
Longitude Latitude Elevation
1 NEPBTS11CBTSC1 NRCS Central BTSC Central Kathmandu 85.3200 27.7021 1282 Director 4225344 Stand‐alone
2 NEPBTS11RBTS1 NRCS Regional BTSC, Kaski RBTSC Pokhara 83.9945 28.2093 838 BTS in‐charge, Medical
technologist 9856021614 Stand‐alone
3 NEPBTS11RBTS2 NRCS Regional BTSC,
Haratpur RBTSC Chitwan 84.43605 27.6816 189 BTS in‐charge 9855058088 Stand‐alone
4 NEPBTS11RBTS3 NRCS Regional BTSC,
Banke RBTSC Nepalgunj 28.0524 81.6199 130 BTS in‐charge 081‐520174 Stand‐alone
5 NEPBTS11RBTS4 NRCS Regional BTSC,
Morang RBTSC Biratnagar 26.4584 87.2861 63 BTS in‐charge 021‐523326 Stand‐alone
6 NEPBTS11DBTS1 NRCS District BTSC
Nawalparasi DBTSC Nawalparasi 83.6662 27.5311 89 BTS‐ technician 9806948616 Stand‐alone
7 NEPBTS11DBTS10 NRCS District BTSC Kailali DBTSC Kailali 28.7041 80.5866 146 BTS in‐charge 9848420064 Stand‐alone
8 NEPBTS11DBTS11 NRCS District BTSC
Surkeht DBTSC Surkhet 28.6062 81.6008 707 BTS in‐charge 9848047103 Stand‐alone
9 NEPBTS11DBTS12 NRCS District BTSC,
Bardiya DBTSC Bardiya 28.2024 81.3474 129 Blood Bank Assistant 084‐420835 Stand‐alone
10 NEPBTS11DBTS13 NRCS District BTSC, Dang DBTSC Dang 28.0375 82.4911 637 BTS in‐charge 082‐561460 Stand‐alone
11 NEPBTS11DBTS14 NRCS District BTSC, Jumla DBTSC Jumla BTS‐technician 087‐520036 Stand‐alone
12 NEPBTS11DBTS15 NRCS District BTSC,
Sunsari DBTSC Sunsari 26.8108 87.2683 326 BTS in‐charge 9842041047 Stand‐alone
13 NEPBTS11DBTS16 NRCS District BTSC, Jhapa DBTSC Jhapa 26.5567 88.0891 71 BTS in‐charge 023‐520814 Stand‐alone
14 NEPBTS11DBTS17 NRCS District BTSC, Ilam DBTSC Ilam 26.9106 87.9271 1264 Lab Technician 027‐520022 Hospital based
15 NEPBTS11DBTS18 NRCS District BTSC,
Panchthar DBTSC Panchthar 27.1473 87.767 1145 BTS, Technician 024‐570273 Stand‐alone
16 NEPBTS11DBTS19 NRCS District BTSC,
Saptari DBTSC Saptari 26.5359 86.75 68 BTS in‐charge 9804708631 Stand‐alone
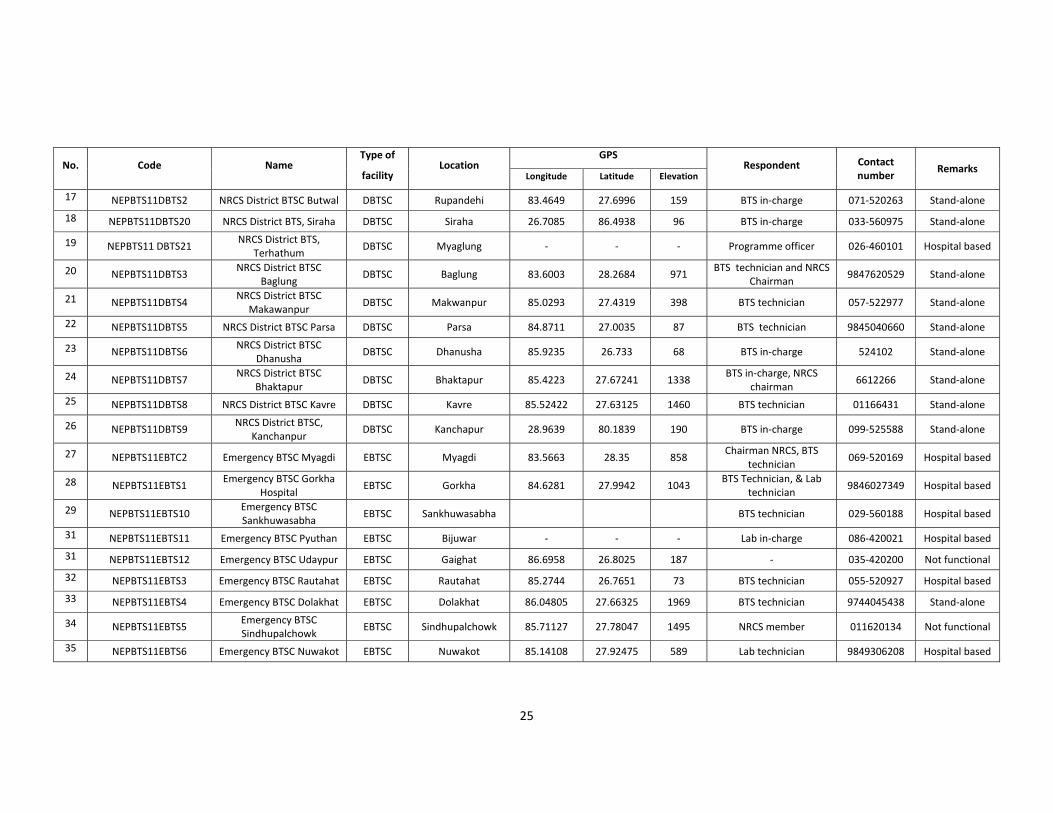
25
No. Code Name Type of
facility Location
GPS Respondent Contact
number Remarks
Longitude Latitude Elevation
17 NEPBTS11DBTS2 NRCS District BTSC Butwal DBTSC Rupandehi 83.4649 27.6996 159 BTS in‐charge 071‐520263 Stand‐alone
18 NEPBTS11DBTS20 NRCS District BTS, Siraha DBTSC Siraha 26.7085 86.4938 96 BTS in‐charge 033‐560975 Stand‐alone
19 NEPBTS11 DBTS21 NRCS District BTS,
Terhathum DBTSC Myaglung ‐ ‐ ‐ Programme officer 026‐460101 Hospital based
20 NEPBTS11DBTS3 NRCS District BTSC
Baglung DBTSC Baglung 83.6003 28.2684 971
BTS technician and NRCS Chairman
9847620529 Stand‐alone
21 NEPBTS11DBTS4 NRCS District BTSC
Makawanpur DBTSC Makwanpur 85.0293 27.4319 398 BTS technician 057‐522977 Stand‐alone
22 NEPBTS11DBTS5 NRCS District BTSC Parsa DBTSC Parsa 84.8711 27.0035 87 BTS technician 9845040660 Stand‐alone
23 NEPBTS11DBTS6 NRCS District BTSC
Dhanusha DBTSC Dhanusha 85.9235 26.733 68 BTS in‐charge 524102 Stand‐alone
24 NEPBTS11DBTS7 NRCS District BTSC
Bhaktapur DBTSC Bhaktapur 85.4223 27.67241 1338
BTS in‐charge, NRCS chairman
6612266 Stand‐alone
25 NEPBTS11DBTS8 NRCS District BTSC Kavre DBTSC Kavre 85.52422 27.63125 1460 BTS technician 01166431 Stand‐alone
26 NEPBTS11DBTS9 NRCS District BTSC,
Kanchanpur DBTSC Kanchapur 28.9639 80.1839 190 BTS in‐charge 099‐525588 Stand‐alone
27 NEPBTS11EBTC2 Emergency BTSC Myagdi EBTSC Myagdi 83.5663 28.35 858 Chairman NRCS, BTS
technician 069‐520169 Hospital based
28 NEPBTS11EBTS1 Emergency BTSC Gorkha
Hospital EBTSC Gorkha 84.6281 27.9942 1043
BTS Technician, & Lab technician
9846027349 Hospital based
29 NEPBTS11EBTS10 Emergency BTSC Sankhuwasabha
EBTSC Sankhuwasabha BTS technician 029‐560188 Hospital based
31 NEPBTS11EBTS11 Emergency BTSC Pyuthan EBTSC Bijuwar ‐ ‐ ‐ Lab in‐charge 086‐420021 Hospital based
31 NEPBTS11EBTS12 Emergency BTSC Udaypur EBTSC Gaighat 86.6958 26.8025 187 ‐ 035‐420200 Not functional
32 NEPBTS11EBTS3 Emergency BTSC Rautahat EBTSC Rautahat 85.2744 26.7651 73 BTS technician 055‐520927 Hospital based
33 NEPBTS11EBTS4 Emergency BTSC Dolakhat EBTSC Dolakhat 86.04805 27.66325 1969 BTS technician 9744045438 Stand‐alone
34 NEPBTS11EBTS5 Emergency BTSC Sindhupalchowk
EBTSC Sindhupalchowk 85.71127 27.78047 1495 NRCS member 011620134 Not functional
35 NEPBTS11EBTS6 Emergency BTSC Nuwakot EBTSC Nuwakot 85.14108 27.92475 589 Lab technician 9849306208 Hospital based
26
No. Code Name Type of
facility Location
GPS Respondent Contact
number Remarks
Longitude Latitude Elevation
36 NEPBTS11EBTS7 Emergency BTSC Dailekh EBTSC Dailekh ‐ ‐ ‐ Lab In‐charge 089‐420465 Hospital based
37 NEPBTS11EBTS8 Emergency BTSC, Doti EBTSC Doti 29.2705 80.9876 1351 BTS technician 094‐420228 Hospital based
38 NEPBTS11EBTS9 Emergency BTSC, Damak EBTSC Jhapa 26.1565 87.7037 129 BTS in‐charge 9842622446 Stand‐alone
39 NEPBTS11MOHP1 BTSC, Universal Medical
college Hospital based
Rupandehi 83.4488 27.4899 84 BTS‐ technician 9847039374 Hospital based
40 NEPBTS11MOHP10 BTSC, Patan Hospital Hospital based
Lalitpur 85.32338 27.81441 1322 Sr. Medical technologist 9851082074 Hospital based
41 NEPBTS11MOHP11 BTSC, Nepal Police
Hospital Hospital based
Kathmandu 85.32338 27.81441 1320 Chief, Dept of clinical
pathology 9851037708 Hospital based
42 NEPBTS11MOHP12 BTSC, Bir Hospital Hospital based
Kathmandu 85.3136 27.7057 1274 Head, Pathology Dept &
BTS‐ in charge 9841294942 Hospital based
43 NEPBTS11MOHP13 BTSC, Kanti Children
Hospital Hospital based
Kathmandu 85.3292 27.7346 1336 BTS‐ technician 9841381202 Hospital based
44 NEPBTS11MOHP14 BTSC, TUTH Hospital based
Kathmandu 85.3303 27.7348 1329 BTS in‐charge 9841303242 Hospital based
45 NEPBTS11MOHP15 BTSC, Birendra Army
Hospital Hospital based
Kathmandu 85.2904 27.7115 1303 Head, Dept of Pathology Hospital based
46 NEPBTS11MOHP16 BTSC, Maternity Hospital Hospital based
Kathmandu 85.3190 27.6897 1282 BTS‐ technician 9841271510 Hospital based
47 NEPBTS11MOHP17 BTSC, Dr Megh Bahadur Parajuli Community
Hospital
Hospital based
Ilam 26.9183 87.931 1194 Medical lab technologist 027‐520417 Hospital based
48 NEPBTS11MOHP18 BTSC, Nepalgunj Medical
College Hospital based
Banke 28.1988 81.6785 142 Technical Assistant 9848026720 Hospital based
49 NEPBTS11MOHP19 BTSC, Team Hospital Hospital based
Dadeldhura 29.3049 80.5889 1805 BTS in‐charge 9848487668 Hospital based
50 NEPBTS11MOHP2 BTSC, Manipal Teaching
Hospital Hospital based
Kaski 83.9969 28.2359 899 BTS in‐charge, Medical
lab technologist ‐ Hospital based
51 NEPBTS11MOHP20 BTSC, Tikapur hospital Hospital based
Kailali 28.5338 81.12 140 Lab assistant 091‐560406 Stand‐alone
27
No. Code Name Type of
facility Location
GPS Respondent Contact
number Remarks
Longitude Latitude Elevation
52 NEPBTS11MOHP21 BTSC, Padama hospital Hospital based
Kailali 28.8114 80.5532 177 Lab assistant 9749007483 Hospital based
53 NEPBTS11MOHP22 BTSC, United Mission
Hospital Hospital based
Palpa 83.555 27.8693 1273 Medical Superintendent 07552011 Hospital based
54 NEPBTS11MOHP23 BTSC, BPKMCH Hospital based
Bharatpur Pathologist 9841255807 Hospital based
55 NEPBTS11MOHP3 BTSC, Lamjung
Community Hospital Hospital based
Lamjung 28.2295 84.3799 782 Lab Technician 9841888687 Hospital based
56 NEPBTS11MOHP4 BTSC, National Medical
College Hospital based
Parsa 84.8972 27.01152 78 BTS in‐charge 9845040588 Hospital based
57 NEPBTS11MOHP5 BTSC, Janaki Medical
College Hospital based
Dhanusha 85.9548 26.8155 88 BTS in‐charge 9844028441 Hospital based
58 NEPBTS11MOHP6 BTSC, Shahid Gangalal
Hospital Hospital based
Kathmandu 85.344 27.74569 1349 Medical lab technologist 4371322 Hospital based
59 NEPBTS11MOHP7 BTSC, Nepal Medical
college Hospital based
Kathmandu 85.3804 27.7336 1369 Medical lab technologist 9849010006 Hospital based
60 NEPBTS11MOHP8 BTSC, Kathmandu Medical
college Hospital based
Kathmandu 85.35338 27.6962 1360 Lab technician 9841204531 Hospital based
61 NEPBTS11MOHP9 BTSC, Scheer Memorial
Hospital Hospital based
Kavre 85.5273 27.6331 1470 Medical lab technologist 0980806162 Hospital based
28
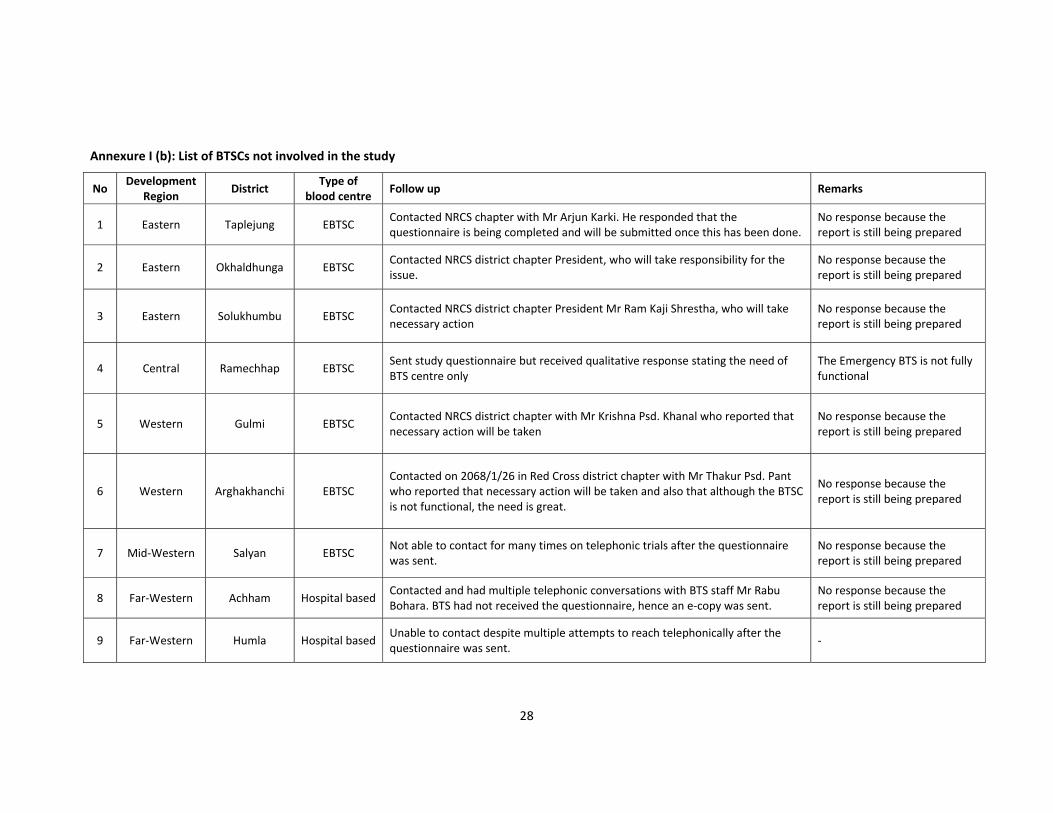
Annexure I (b): List of BTSCs not involved in the study
No Development
Region District
Type ofblood centre
Follow up Remarks
1 Eastern Taplejung EBTSC Contacted NRCS chapter with Mr Arjun Karki. He responded that the questionnaire is being completed and will be submitted once this has been done.
No response because the report is still being prepared
2 Eastern Okhaldhunga EBTSC Contacted NRCS district chapter President, who will take responsibility for the issue.
No response because the report is still being prepared
3 Eastern Solukhumbu EBTSC Contacted NRCS district chapter President Mr Ram Kaji Shrestha, who will take necessary action
No response because the report is still being prepared
4 Central Ramechhap EBTSC Sent study questionnaire but received qualitative response stating the need of BTS centre only
The Emergency BTS is not fully functional
5 Western Gulmi EBTSC Contacted NRCS district chapter with Mr Krishna Psd. Khanal who reported that necessary action will be taken
No response because the report is still being prepared
6 Western Arghakhanchi EBTSC Contacted on 2068/1/26 in Red Cross district chapter with Mr Thakur Psd. Pant who reported that necessary action will be taken and also that although the BTSC is not functional, the need is great.
No response because the report is still being prepared
7 Mid‐Western Salyan EBTSC Not able to contact for many times on telephonic trials after the questionnaire was sent.
No response because the report is still being prepared
8 Far‐Western Achham Hospital based Contacted and had multiple telephonic conversations with BTS staff Mr Rabu Bohara. BTS had not received the questionnaire, hence an e‐copy was sent.
No response because the report is still being prepared
9 Far‐Western Humla Hospital based Unable to contact despite multiple attempts to reach telephonically after the questionnaire was sent.
‐
29
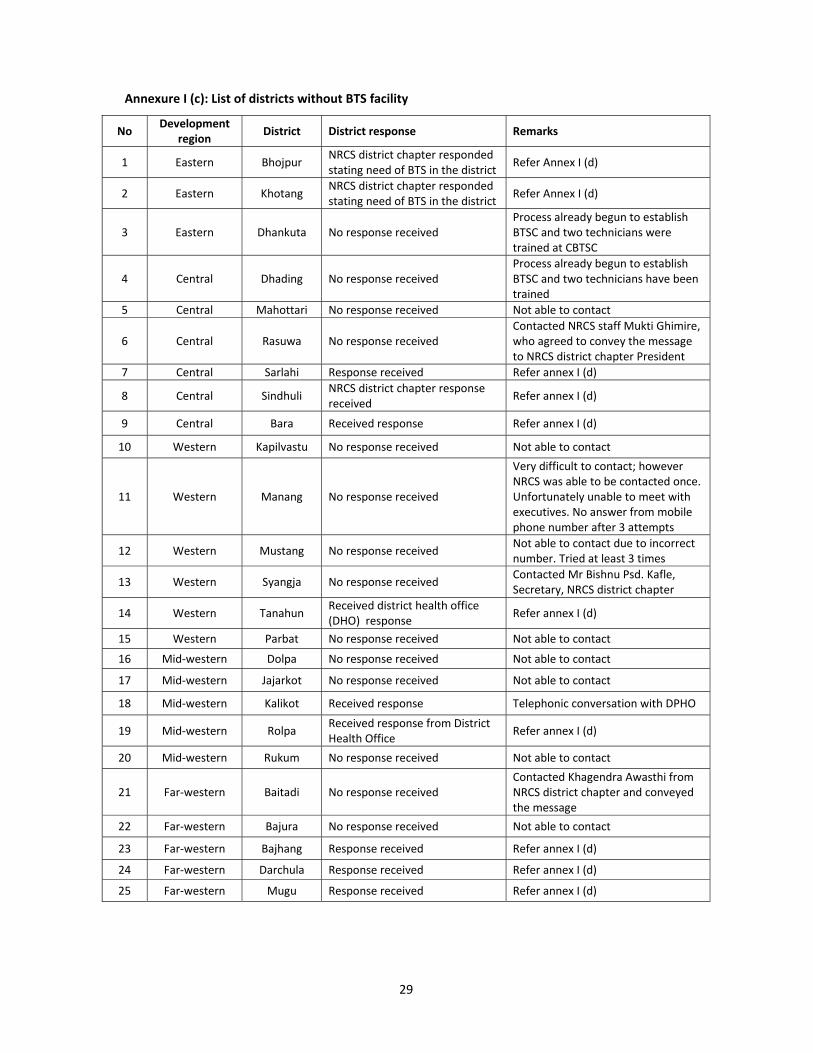
Annexure I (c): List of districts without BTS facility
No Development
region District District response Remarks
1 Eastern Bhojpur NRCS district chapter respondedstating need of BTS in the district
Refer Annex I (d)
2 Eastern Khotang NRCS district chapter responded stating need of BTS in the district
Refer Annex I (d)
3 Eastern Dhankuta No response received Process already begun to establish BTSC and two technicians were trained at CBTSC
4 Central Dhading No response received Process already begun to establish BTSC and two technicians have been trained
5 Central Mahottari No response received Not able to contact
6 Central Rasuwa No response received Contacted NRCS staff Mukti Ghimire, who agreed to convey the message to NRCS district chapter President
7 Central Sarlahi Response received Refer annex I (d)
8 Central Sindhuli NRCS district chapter response received
Refer annex I (d)
9 Central Bara Received response Refer annex I (d)
10 Western Kapilvastu No response received Not able to contact
11 Western Manang No response received
Very difficult to contact; howeverNRCS was able to be contacted once. Unfortunately unable to meet with executives. No answer from mobile phone number after 3 attempts
12 Western Mustang No response received Not able to contact due to incorrect number. Tried at least 3 times
13 Western Syangja No response received Contacted Mr Bishnu Psd. Kafle, Secretary, NRCS district chapter
14 Western Tanahun Received district health office (DHO) response
Refer annex I (d)
15 Western Parbat No response received Not able to contact
16 Mid‐western Dolpa No response received Not able to contact
17 Mid‐western Jajarkot No response received Not able to contact
18 Mid‐western Kalikot Received response Telephonic conversation with DPHO
19 Mid‐western Rolpa Received response from District Health Office
Refer annex I (d)
20 Mid‐western Rukum No response received Not able to contact
21 Far‐western Baitadi No response received Contacted Khagendra Awasthi from NRCS district chapter and conveyed the message
22 Far‐western Bajura No response received Not able to contact
23 Far‐western Bajhang Response received Refer annex I (d)
24 Far‐western Darchula Response received Refer annex I (d)
25 Far‐western Mugu Response received Refer annex I (d)
30
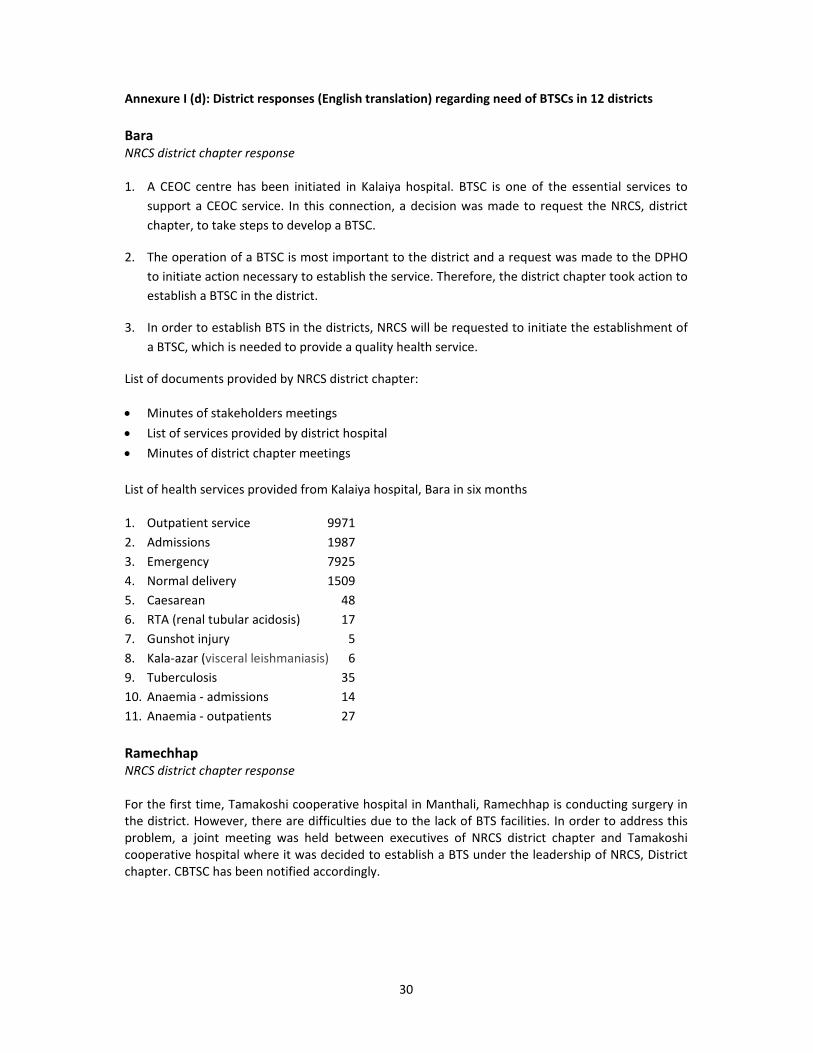
Annexure I (d): District responses (English translation) regarding need of BTSCs in 12 districts
Bara NRCS district chapter response 1. A CEOC centre has been initiated in Kalaiya hospital. BTSC is one of the essential services to
support a CEOC service. In this connection, a decision was made to request the NRCS, district
chapter, to take steps to develop a BTSC.
2. The operation of a BTSC is most important to the district and a request was made to the DPHO
to initiate action necessary to establish the service. Therefore, the district chapter took action to
establish a BTSC in the district.
3. In order to establish BTS in the districts, NRCS will be requested to initiate the establishment of
a BTSC, which is needed to provide a quality health service.
List of documents provided by NRCS district chapter:
Minutes of stakeholders meetings
List of services provided by district hospital
Minutes of district chapter meetings
List of health services provided from Kalaiya hospital, Bara in six months 1. Outpatient service 9971
2. Admissions 1987
3. Emergency 7925
4. Normal delivery 1509
5. Caesarean 48
6. RTA (renal tubular acidosis) 17
7. Gunshot injury 5
8. Kala‐azar (visceral leishmaniasis) 6
9. Tuberculosis 35
10. Anaemia ‐ admissions 14
11. Anaemia ‐ outpatients 27
Ramechhap NRCS district chapter response For the first time, Tamakoshi cooperative hospital in Manthali, Ramechhap is conducting surgery in the district. However, there are difficulties due to the lack of BTS facilities. In order to address this problem, a joint meeting was held between executives of NRCS district chapter and Tamakoshi cooperative hospital where it was decided to establish a BTS under the leadership of NRCS, District chapter. CBTSC has been notified accordingly.
31
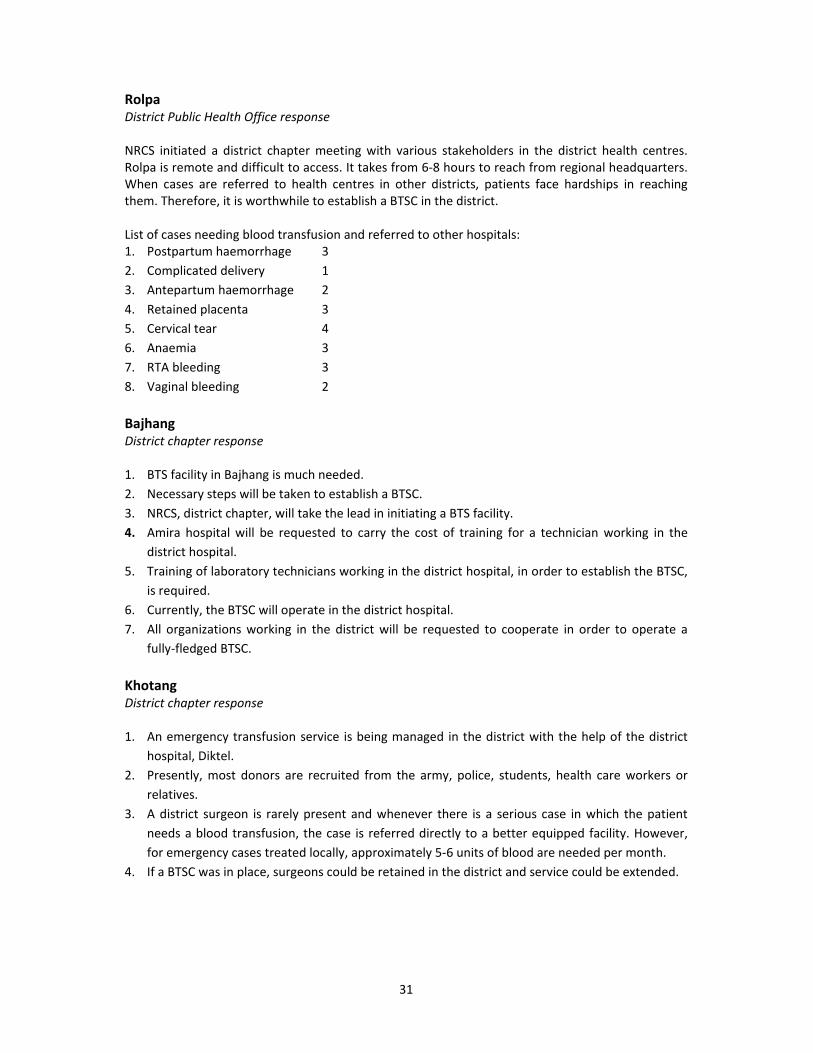
Rolpa District Public Health Office response NRCS initiated a district chapter meeting with various stakeholders in the district health centres. Rolpa is remote and difficult to access. It takes from 6‐8 hours to reach from regional headquarters. When cases are referred to health centres in other districts, patients face hardships in reaching them. Therefore, it is worthwhile to establish a BTSC in the district. List of cases needing blood transfusion and referred to other hospitals: 1. Postpartum haemorrhage 3
2. Complicated delivery 1
3. Antepartum haemorrhage 2
4. Retained placenta 3
5. Cervical tear 4
6. Anaemia 3
7. RTA bleeding 3
8. Vaginal bleeding 2
Bajhang District chapter response 1. BTS facility in Bajhang is much needed.
2. Necessary steps will be taken to establish a BTSC.
3. NRCS, district chapter, will take the lead in initiating a BTS facility.
4. Amira hospital will be requested to carry the cost of training for a technician working in the
district hospital.
5. Training of laboratory technicians working in the district hospital, in order to establish the BTSC,
is required.
6. Currently, the BTSC will operate in the district hospital.
7. All organizations working in the district will be requested to cooperate in order to operate a
fully‐fledged BTSC.
Khotang District chapter response 1. An emergency transfusion service is being managed in the district with the help of the district
hospital, Diktel.
2. Presently, most donors are recruited from the army, police, students, health care workers or
relatives.
3. A district surgeon is rarely present and whenever there is a serious case in which the patient
needs a blood transfusion, the case is referred directly to a better equipped facility. However,
for emergency cases treated locally, approximately 5‐6 units of blood are needed per month.
4. If a BTSC was in place, surgeons could be retained in the district and service could be extended.
32
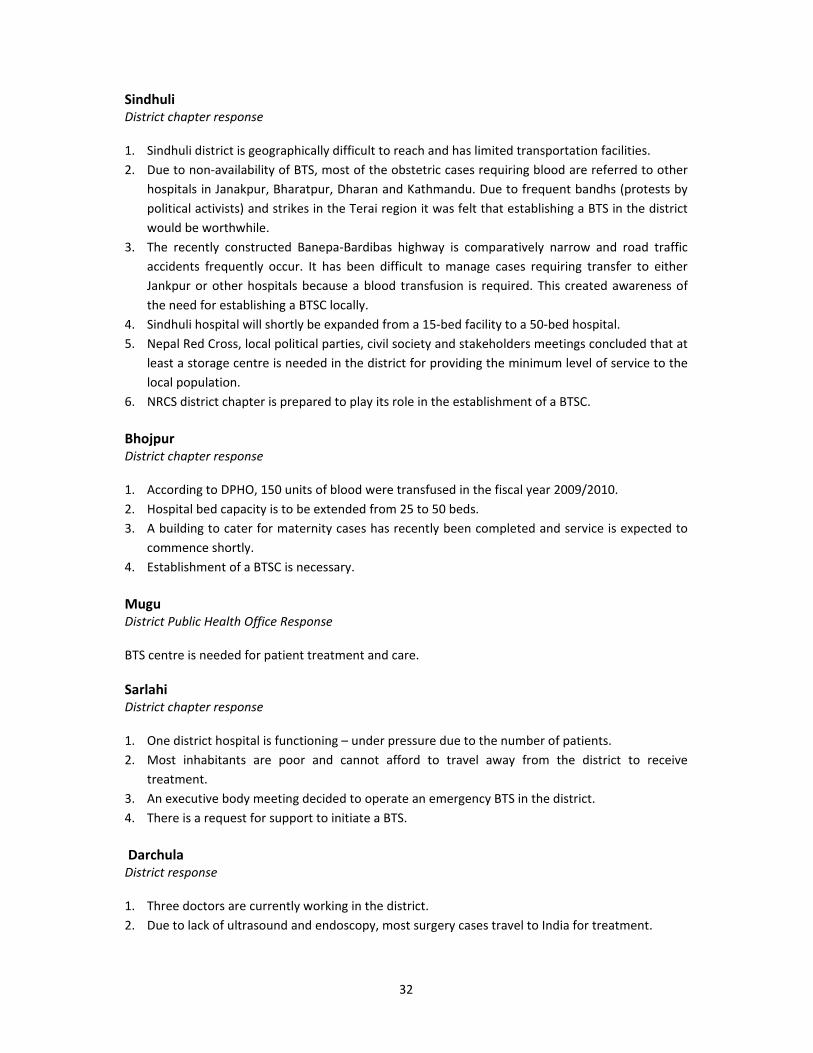
Sindhuli District chapter response 1. Sindhuli district is geographically difficult to reach and has limited transportation facilities.
2. Due to non‐availability of BTS, most of the obstetric cases requiring blood are referred to other
hospitals in Janakpur, Bharatpur, Dharan and Kathmandu. Due to frequent bandhs (protests by
political activists) and strikes in the Terai region it was felt that establishing a BTS in the district
would be worthwhile.
3. The recently constructed Banepa‐Bardibas highway is comparatively narrow and road traffic
accidents frequently occur. It has been difficult to manage cases requiring transfer to either
Jankpur or other hospitals because a blood transfusion is required. This created awareness of
the need for establishing a BTSC locally.
4. Sindhuli hospital will shortly be expanded from a 15‐bed facility to a 50‐bed hospital.
5. Nepal Red Cross, local political parties, civil society and stakeholders meetings concluded that at
least a storage centre is needed in the district for providing the minimum level of service to the
local population.
6. NRCS district chapter is prepared to play its role in the establishment of a BTSC.
Bhojpur District chapter response 1. According to DPHO, 150 units of blood were transfused in the fiscal year 2009/2010.
2. Hospital bed capacity is to be extended from 25 to 50 beds.
3. A building to cater for maternity cases has recently been completed and service is expected to
commence shortly.
4. Establishment of a BTSC is necessary.
Mugu District Public Health Office Response BTS centre is needed for patient treatment and care.
Sarlahi District chapter response 1. One district hospital is functioning – under pressure due to the number of patients.
2. Most inhabitants are poor and cannot afford to travel away from the district to receive
treatment.
3. An executive body meeting decided to operate an emergency BTS in the district.
4. There is a request for support to initiate a BTS.
Darchula District response 1. Three doctors are currently working in the district.
2. Due to lack of ultrasound and endoscopy, most surgery cases travel to India for treatment.

33
3. Cases of anaemia, maternity, RTA, and malnutrition are usually treated in the district. On
average, 10 patients a month need transfusion.
4. If BTS was available in the district, at least 10 patients would not need to be referred and could
be treated locally. Hence, a BTS is needed in the district.
Tanahun
District Public Health Office response An EBTSC is needed in the district.
Kalikot NRCS district chapter response Response was by means of telephonic communication with NRCS district chapter President, Mr Bala Prasda Sanjyal. 1. Nepal Red Cross Society, District Chapter and DPHO Kalikot will hold a meeting to establish an
emergency type BTS.
2. Nick Simmons Institute has been approached for basic equipment support and the institution
has sent the request to headquarters for confirmation of support.
3. There is a plan to recruit and send a laboratory assistant for induction training at CBTSC. For this
purpose, the district chapter has already enquired about the process and possibilities.
4. BTS will be started within the hospital pathology unit.
34
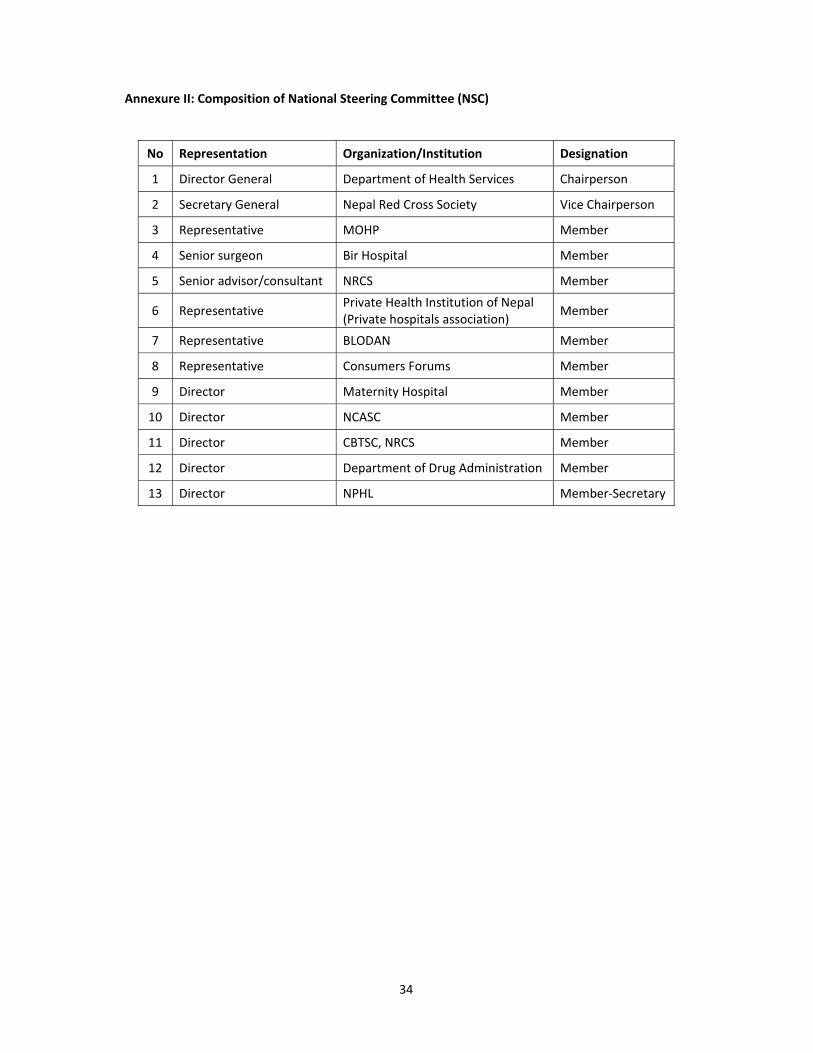
Annexure II: Composition of National Steering Committee (NSC)
No Representation Organization/Institution Designation
1 Director General Department of Health Services Chairperson
2 Secretary General Nepal Red Cross Society Vice Chairperson
3 Representative MOHP Member
4 Senior surgeon Bir Hospital Member
5 Senior advisor/consultant NRCS Member
6 Representative Private Health Institution of Nepal (Private hospitals association)
Member
7 Representative BLODAN Member
8 Representative Consumers Forums Member
9 Director Maternity Hospital Member
10 Director NCASC Member
11 Director CBTSC, NRCS Member
12 Director Department of Drug Administration Member
13 Director NPHL Member‐Secretary
35
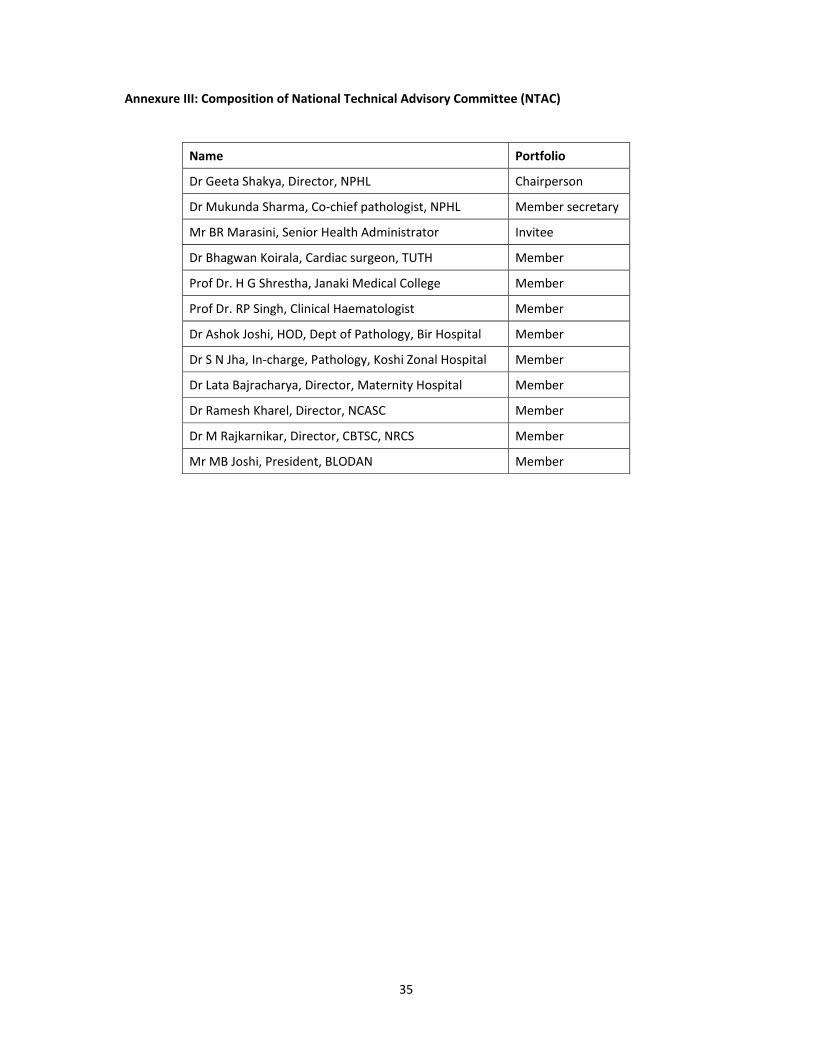
Annexure III: Composition of National Technical Advisory Committee (NTAC)
Name Portfolio
Dr Geeta Shakya, Director, NPHL Chairperson
Dr Mukunda Sharma, Co‐chief pathologist, NPHL Member secretary
Mr BR Marasini, Senior Health Administrator Invitee
Dr Bhagwan Koirala, Cardiac surgeon, TUTH Member
Prof Dr. H G Shrestha, Janaki Medical College Member
Prof Dr. RP Singh, Clinical Haematologist Member
Dr Ashok Joshi, HOD, Dept of Pathology, Bir Hospital Member
Dr S N Jha, In‐charge, Pathology, Koshi Zonal Hospital Member
Dr Lata Bajracharya, Director, Maternity Hospital Member
Dr Ramesh Kharel, Director, NCASC Member
Dr M Rajkarnikar, Director, CBTSC, NRCS Member
Mr MB Joshi, President, BLODAN Member



![Clinical Study Comprehensive Look at Blood Transfusion ... · autologous transfusion[ ]. Using autologous donations for transfusion avoids many of the adverse events associated with](https://static.fdocuments.net/doc/165x107/60c99f0bc8ad33300f37a7c4/clinical-study-comprehensive-look-at-blood-transfusion-autologous-transfusion.jpg)