MAPLES’ MUSINGSMAPLES’ MUSINGS CONFLICTS OF INTERESTS Michael D. Maples, MD, Medical Director...
6
Third Quarter 2012 MAPLES’ MUSINGS CONFLICTS OF INTERESTS Michael D. Maples, MD, Medical Director Most of you are so busy trying to make sure you have all of the lab results from the last patient’s visit or that the arrange- ments have been made for home care that you have little time to worry about the big picture. To most of you it is abundantly clear that you have no conflict of interest with the patient in front of you. Both of you seem interested in the patient’s welfare. The conflict of interest arises regarding the payment of said services and the value of same. Posting an intermediary between the patient and doctor necessarily creates a conflict. This is not readily apparent until one of the parties in this transaction balks at payment or compli- ance. Then the conflict surfaces. We at MACM have established a Young Physicians Advisory Council to try to understand the outlook of this age group and to help them learn about MACM. As an aside, we have learned that about 50 percent of our insureds were not in practice prior to 2002. We understand that the future of the Company is with the young, and we want them to under- stand MACM. I have been very impressed with the group as a whole and with their grasp of the big picture, despite their relatively short time in practice. Once again, I have been impressed that intelligence combined with manners and hard work leads to very successful people. It is quite reassuring. One question which we posed to this young group was their view of the future of medicine. In particular we wanted to see if they understood the implications of working for a hospital or insurance company versus owning their own practice. Most of them had already pondered the possibility or were already working for a non-professional corporation and they understood the conflict that exists implicitly. What’s more, they recognized the real problem was for the patient. We at MACM are not sure if the independent practice of medicine will survive, but we are indeed encouraged that this young group identifies the centrality of the patient. MANDATORY ORIENTATION PROGRAM FOR NEW PHYSICIANS Each year, the Risk Management Department hosts a series of meetings throughout Mississippi for the purpose of educating our newly insured physicians about Medical Assurance Company of Mississippi. This mandatory pro- gram provides valuable information on the Underwriting, Claims, and Risk Management philosophies of the Company and gives our insureds the opportunity to ask questions and meet the MACM staff. Failure to attend one of these live activities scheduled within the first year of an insured’s time with MACM will result in a 5 percent premium surcharge or $1000, whichever is greater. Continued failure to attend through the next policy period will result in a 10 percent surcharge or $1000, whichever is greater. If the requirement is not met within the third policy period, the physician will be considered for non-renewal. For more information on the orientation program and a list of meeting dates remaining for this year, please visit our web site at www.macm.net.
Transcript of MAPLES’ MUSINGSMAPLES’ MUSINGS CONFLICTS OF INTERESTS Michael D. Maples, MD, Medical Director...

Third Quarter 2012
MAPLES’ MUSINGSCONFLICTS OF INTERESTS Michael D. Maples, MD, Medical Director
Most of you are so busy trying to make sure you have all of the lab results from the last patient’s visit or that the arrange-ments have been made for home care that you have little time to worry about the big picture. To most of you it is abundantly clear that you have no conflict of interest with the patient in front of you. Both of you seem interested in the patient’s welfare. The conflict of interest arises regarding the payment of said services and the value of same. Posting an intermediary between the patient and doctor necessarily creates a conflict. This is not readily apparent until one of the parties in this transaction balks at payment or compli-ance. Then the conflict surfaces.
We at MACM have established a Young Physicians Advisory Council to try to understand the outlook of this age group and to help them learn about MACM. As an aside, we have learned that about 50 percent of our insureds were not in practice prior to 2002. We understand that the future of the
Company is with the young, and we want them to under-stand MACM. I have been very impressed with the group as a whole and with their grasp of the big picture, despite their relatively short time in practice. Once again, I have been impressed that intelligence combined with manners and hard work leads to very successful people. It is quite reassuring.
One question which we posed to this young group was their view of the future of medicine. In particular we wanted to see if they understood the implications of working for a hospital or insurance company versus owning their own practice. Most of them had already pondered the possibility or were already working for a non-professional corporation and they understood the conflict that exists implicitly. What’s more, they recognized the real problem was for the patient.
We at MACM are not sure if the independent practice of medicine will survive, but we are indeed encouraged that this young group identifies the centrality of the patient.
MANDATORY ORIENTATION PROGRAM FOR NEW PHYSICIANSEach year, the Risk Management Department hosts a series of meetings throughout Mississippi for the purpose of educating our newly insured physicians about Medical Assurance Company of Mississippi. This mandatory pro-gram provides valuable information on the Underwriting, Claims, and Risk Management philosophies of the Company and gives our insureds the opportunity to ask questions and meet the MACM staff.
Failure to attend one of these live activities scheduled within the first year of an insured’s time with MACM will result in
a 5 percent premium surcharge or $1000, whichever is greater. Continued failure to attend through the next policy period will result in a 10 percent surcharge or $1000, whichever is greater. If the requirement is not met within the third policy period, the physician will be considered for non-renewal.
For more information on the orientation program and a list of meeting dates remaining for this year, please visit our web site at www.macm.net.

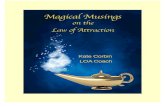
PRACTICE-RELATED CONCERNS 80%SURGERY/DELIVERY INJURY 33%
POST-OP/POSTPARTAL COMPLICATION 24%
INAPPROPRIATE TREATMENT 21%
FAILURE TO/DELAY IN/INAPPROPRIATE FOLLOW-UP 13%
DIAGNOSIS-RELATED CONCERNS 40%FAILURE TO/INAPPROPRIATE DIAGNOSIS 49%
INAPPROPRIATE/DELAYED EXAMINATION 23%
DELAY IN DIAGNOSIS 16%
OVERLOOKED LAB/DIAGNOSTIC STUDY/CONSULT 14%
RISK MANAGEMENT ANALYSIS OF CLAIMS COMMITTEE FILESby Beth Easley, RHIASenior Risk Management Consultant
Every month, one of the two MACM Claims Committees of physicians assesses files presented to them from our Claims Department. Physicians, who belong to the same specialty as the defendant physician, thoroughly “peer-review” the cases and inform the committee physicians and staff of their clinical concerns.
A total of 1,166 cases were reviewed during the time period between January 1, 1996 and December 31, 2011. The Risk Management Department evaluated these records in order to monitor the risk management issues associated with the cases.
As is done each year, the concerns identified with the cases are categorized by clinical issues, risk management issues and “other” issues. Chart 1 All three groups of issues remain fairly constant. Clinical matters accounted for 64 percent of the issues identified in the overall time period while risk manage-ment concerns were detected 85 percent of the time. Various “other”concerns were recognized in 83 percent of the cases reviewed.
The clinical issues (identified by physicians) are categorized by diagnosis-related concerns, which occurred 40 percent of the time, and practice-related concerns, which occurred 80 percent of the time. See Chart 2 for a grouping of the more prevalent of those issues.
The Risk Management Department reviews all claims which go before the MACM Claims Committees each month. The purpose of this review is to identify risk management issues that contributed to the claim and/or impact the defensibility of the claim. Following is information on the risk issues found in these claims over the period January 1, 1996 through December 31, 2011.
Chart 2
CLINICAL ISSUES RISK MANAGEMENT ISSUES
“OTHER” ISSUESChart 1
1996-2011 1996-2000 2001-2005 2006-2010
CLAIMS REVIEWJANUARY 1, 1996 - DECEMBER 31, 2011
0%20%40%60%80%
100%

“Other Issues”
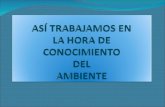
AUTOPSY
UNAVAILABLE RESOURCES
PATIENT/FAMILY IN HEALTHCARE
PATIENT FAILURE TO COMPLY WITH TREATMENT
INCOMPLETE/LOST RECORDS
ANOTHER PROVIDER’S MISADVENTURES
INADEQUATE STAFF PERFORMANCE
VENUE
0% 10% 20% 30% 40% 50% 60% 70%
16%
17%
19%
19%
29%
43%
62%
14%
The percentage of cases with risk management issues remained relatively stable from year-to-year at 85 percent. Of those, the more common concerns were general documentation in the medical record and of the informed consent process, communication breakdowns, and system failures in the office setting. Chart 3
The Risk Management Department reviews all claims which go before the MACM Claims Committees each month. The purpose of this review is to identify risk management issues that contributed to the claim and/or impact the defensibility of the claim. Following is information on the risk issues found in these claims over the period January 1, 1996 through December 31, 2011.
Chart 4
SYSTEM FAILURE (OFFICE)
INFORMED CONSENT
COMMUNICATION MEDICALRECORD
DOCUMENTATION
RISK MANAGEMENT ISSUES
Chart 3
0%10%20%30%40%50%60%70%
By referencing the allegations of these lawsuits, we are not stating that the allegations are true. We are only providing the allegations in order to show what the plaintiffs claimed, which were generally unsupported as shown by the defense verdicts.

“Other issues” were described in 79 percent of the claims reviewed. This miscellaneous and varied category includes system failures in the hospital setting, legal matters, and various other concerns. The information in Chart 4 indicates some of those that are seen more often.
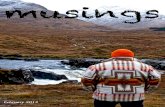
The majority of claims still develop in the hospital setting (in-patient or out-patient). Prior to 2001, the hospital location for incidents was not differentiated by inpatient or outpatient.
While gender and age fluctuate from year to year as one might expect, the claimants were female by majority and were approximately 43 years old. The principal payment source of the claimants continues to be private insurance.
The Risk Management Department will continue to follow and trend data retrieved from analyzing claims presented to the Claims Committees. We believe it gives areas of focus for the consultants to continue to monitor.
MALE 38%
FEMALE 62%
INCIDENT BY GENDER
OUTPATIENT 13%
OFFICE 21%
HOSPITAL 22%INPATIENT
42%
OTHER 2%
LOCATION OF INCIDENT
PRIVATE INS 54% MEDICARE 21% MEDICAID 18% SELF-PAY W/C 6% OTHER 1%
PAYMENT SOURCE
Figure 5
Figure 6
Figure 7

5
2012 Office Staff Program ScheduleProgram # Date Time Place LocationS12-6 Thurs, 09/20/2012 11AM - 1PM Tupelo Bancorp South Convention Center
S12-7 Thurs, 09/27/2012 11AM - 1PM Greenville Delta Regional Pavilion S12-8 Thurs, 10/04/2012 11AM - 1PM Pascagoula Singing River Hospital - Turner Center
S12-9 Tues, 10/16/2012 11AM - 1PM Columbus Fairfield Inn
S12-10 Fri, 10/26/2012 11AM - 1PM Ridgeland/Jackson Copeland, Cook, Taylor, Bush Conf Ctr
S12-11 Tues, 11/13/2012 11AM - 1PM Brookhaven Poppa’s Fish House Meeting Room
Registration Form
Attendee Name/Title:Attendee Name/Title: Attendee Name/Title:
Office/Clinic Address:
Phone: Fax: Email:
I wish to register for Program #: Place: Program Date:
any cancellations must be received prior to the day of the program. cancellations the same day of the program or “no-shows” will generate a $10 invoice per person (to cover the expense of lunch) to the macm-insured physician.
Medical Assurance Company of Mississippi Attn: Risk Management Department P: (601) 605-4882 F: (601) 605-8849
each individual must be registered by name. you may substitute registrations, if needed, closer to meeting date. an email/fax info reminder will be sent to you approximately two weeks before each program.
Don’t short-circuit when it comes to EMRs and technology!The MACM 2012 Office Staff Program will help you work through the issues related to technology in the medical office. We have fused the experience of all the MACM departments to give you important information on the relationship between technology and medical liability.
This program is for ANYONE in your office that would benefit from hearing this information.
EMRs are affecting your practice, even if:• You have an EMR firmly in place.
• You are in the process of getting your EMR up and running.
• You are trying to decide which EMR will work best for your practice.
• You are trying to decide if you are going to an EMR or staying with paper.
No matter where you are in the process, there is information you need to know.
LUNCH WILL BE PROVIDED.
EMR and Other Electrifying Concerns: Fact, Fiction, and
Frustration

MEDICAL ASSURANCE COMPANY OF MISSISSIPPI404 West Parkway PlaceRidgeland, Mississippi 39157
601.605.4882800.325.4172macm.net
Information contained in this publication is obtained from sources considered to be reliable. However, accuracy and completeness cannot be guaranteed. Information herein should not be regarded as legal advice.
The Risk Manager is a publication of Medical Assurance Company of Mississippi.Editor: JoAnn Bienvenu
PRST STDU.S. POSTAGE
PAIDJackson, MS
Permit No. 775
ELECTRONIC HEALTH RECORDS :
Does your practice periodically print out a patient’s entire record as part of your quality monitoring process? Do you know what the record looks like on paper? Is it all there? Unfortunately, although the record one sees on the com-puter screen is easily read and navigated, the printed record may be so “busy” and confusing that any other healthcare provider relying on your printed copy may not be able to make any sense of it. It doesn’t have to be this way, al-though one might think, based upon the ridiculously confusing printouts we have seen while trying to evaluate claims, that this is the norm. There are EHR systems available which have outstanding printed records that are easy to read with the entries organized and labeled, e.g. “Laboratory Results”, “Progress Notes”, “Medication Record”, etc., with each section chronologically arranged. What do yours look like? Do you have an option?
Some EHR systems may not automatically print out the entire record. For example, when a document is produced from an EHR, the notes that were entered in association with that document do not get reproduced, e.g. physician’s review is not documented, any calls or discussion entered into the note electronically attached to that screen may not
be produced. Again, as part of your clinic’s quality moni-toring, periodically print out a screen or patient record to evaluate this area for completeness.
Do you participate in another entity’s electronic health record system? If so, you must understand the content and scope of the agreement you have with the entity which owns and operates the system. One area of importance, among many, involves the security of the record and who has the responsibility and authority to mete out disciplinary action to those who breach confidentiality. Your office may find that, as part of your agreement with another entity, you have ceded all of this responsibility to the other entity. Make sure you and your staff understand the ramifications of this agreement and the fact that the penalties invoked may be entirely out of your clinic’s hands. Have you checked on this?
For more information on the various pitfalls of E-Medicine and technology, attend MACM’s Program, “EMR and Other Electrifying Concerns: Fact, Fiction, and Frustra-tion!” (see page 5 for details and registration).
A FEW QUICK THOUGHTS