Management of stroke
79
MANAGEMENT OF STROKE DR MALLUM C.B. NEUROLOGY UNIT DEPT OF INTERNAL MEDICINE JUTH
-
Upload
chindo-mallum -
Category
Health & Medicine
-
view
493 -
download
3
Transcript of Management of stroke

MANAGEMENT OF STROKE
DR MALLUM C.B.NEUROLOGY UNIT
DEPT OF INTERNAL MEDICINEJUTH

OUTLINE
• DEFINITIONS
• TYPES OF STROKE
• EVALUATION OF STROKE
• INVESTIGATIONS
• POOR PROGNOSTIC FACTORS IN STROKE
• DEFINITION OF LEVELS OF EVIDENCE/RECOMMENDATIONS
• MEDICAL MANAGEMENT
• PREVENTION AND MANAGEMENT OF COMPLICATIONS
• SURGICAL MANAGEMENT

DEFINITION
• Stroke(CVA) is defined by the World Health Organization as a clinical syndrome consisting of ‘rapidly developing clinical signs of focal (at times global) disturbance of cerebral function, lasting more than 24 h or leading to death with no apparent cause other than that of vascular origin’.
• CVD - parent term = also includes Cerebral arteriosclerosis; cerebral angioma ; Cerebral artero-venous malformation ; Subdural hematoma

TRANSIENT ISCHEMIC ATTACK(TIA)
• Transient ischemic attack is temporary focal neurological deficit of sudden onset caused by ischemia of the brain, retina lasting less than 24 hours followed by complete recovery.
• New definition: No objective evidence of acute infarction in the affected region of brain or retina; < I hour
• Therefore, CT/MRI necessary to increase diagnostic accuracy.

CLASSIFICATION OF STROKE
Stroke
Primary Hemorrhagic
(20% of Strokes)
Primary Ischemic
(80% of Strokes)
Thrombotic
50%
Embolic
30%
Intracerebral
Hemorrhage 15%
Subarachnoid
Hemorrhage 5%
5

STROKE
Which is an Ischaemic Stroke?

Causes
Destruction of brain cells and tissue

Types of Stroke
85%
Ischemic
15 %
hemorrhagic

ISCHEMIC STROKE PATHOPHYSIOLOGYThe First Few Hours
Penumbra
Core
Clot in Artery
“TIME IS BRAIN:SAVE THE PENUMBRA”
Penumbra is zone of reversible ischemia around core of irreversible infarction—salvageable in first few hours afterischemic stroke onset
Penumbra damaged by:• Hypoperfusion• Hyperglycemia• Fever• Seizure

Cerebral Arterial territory
Anterior cerebral
Middle cerebral
Posterior cerebral
Anterior choroidal
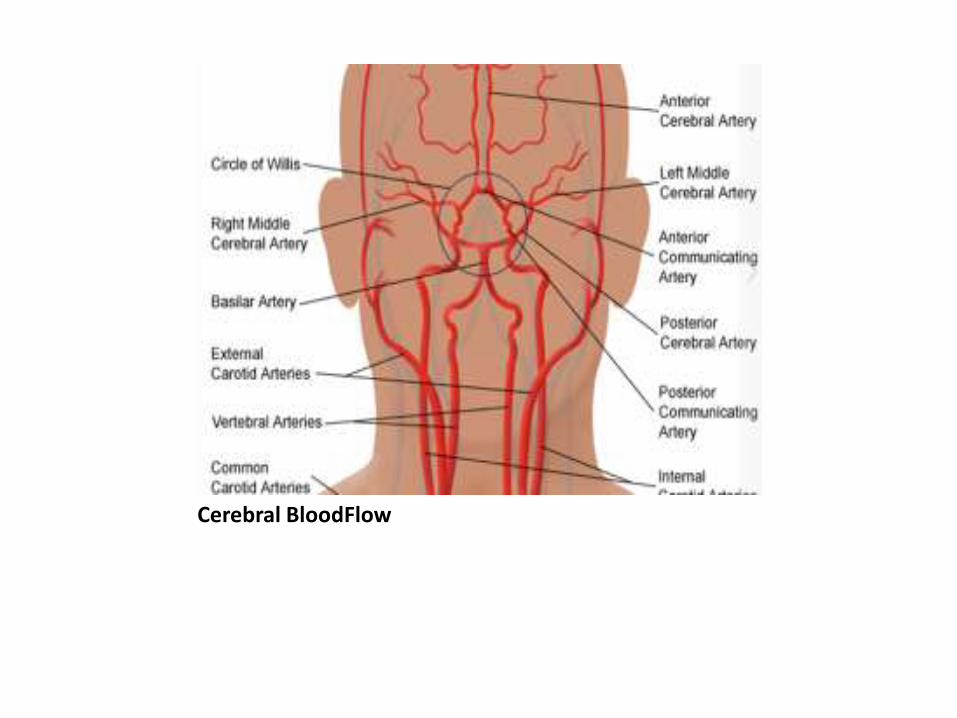
Cerebral BloodFlow

EVALUATION OF STROKE
• 1. Determine if symptoms are due to stroke• 2. Localize site of brain lesion• 3. Establish the type of stroke• 4. Ascertain the likely cause• The clinical assessment (history, general examination,and neurological examination) remains the cornerstoneof the evaluation.• The use of a stroke rating scale, preferably the NIHSS, is
recommended (Class I; Level of Evidence B).• It has been recommended that patients with acute
stroke <7 days or progressive stroke should be admitted

Stroke - questions
• Is it a stroke ?
• What type of stroke ?
• Why did it happen ?
• How does it affect the patient ?
• What is the prognosis ?

14
The symptoms of a stroke are dependant on what portion of the brain is damage.
http://www.pdrhealth.com/patient_education/images/BHG01NE13F01.GIF

1/18/2015 15
Pathological: WHO Criteria
C.I C.H• L.O.C. -ve +ve• Headache - ve +ve• Vomiting - ve +ve• T.I.A. +ve - ve• Gradual onset +ve -ve• Activity -ve + ve• HBP mild /-ve mod/severe• Bldy csf -ve + ve


EMERGENCY INVESTIGATIONS
• To establish the diagnosis of stroke
• to determine the underlying cause of the event.

Immediate Diagnostic Studies: Evaluation of aPatient With Suspected Acute Ischemic Stroke
Stroke 2007;38;1655-1711;

INVESTIGATIONS
• full blood count, serum electrolytes, renal function tests, cardiac enzymes, and coagulation studies
• Blood sugar is mandatory to exclude hypoglycemia or diagnose diabetes mellitus
• Full blood count to detect Polycythaemia,ESR for endocarditis,
• clotting studies for Hypercoagulable States• An electrocardiogram (ECG) : arrhythmias and
myocardial infarction. Baseline ECG is recommended in all patients with stroke(AHA/ASA Guidelines)
• Echocardiography : valve disease and intra-cardiac clot

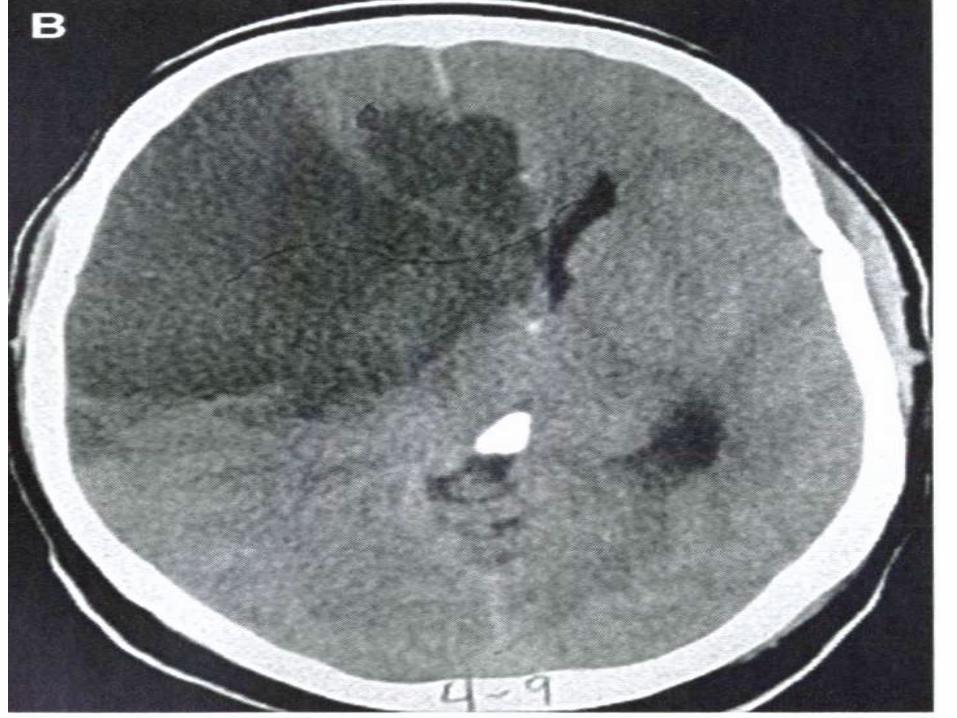
NEUROIMAGING
• Brain CT scan: CT is sensitive to the intracranial blood and is readily available.
Normal early CT therefore rules out haemorrhagic stroke. CT Scan changes in ischemic stroke may take several days to develop.
• MRI: MRI is better at detecting posterior fossa lesions especially in posterior circulation stroke such as Pons or cerebellum
• It is also recommended that all patients with transient neurologic symptoms have a neuroimaging within 24 hours or as soon as possible.(Class 1,LOE B)
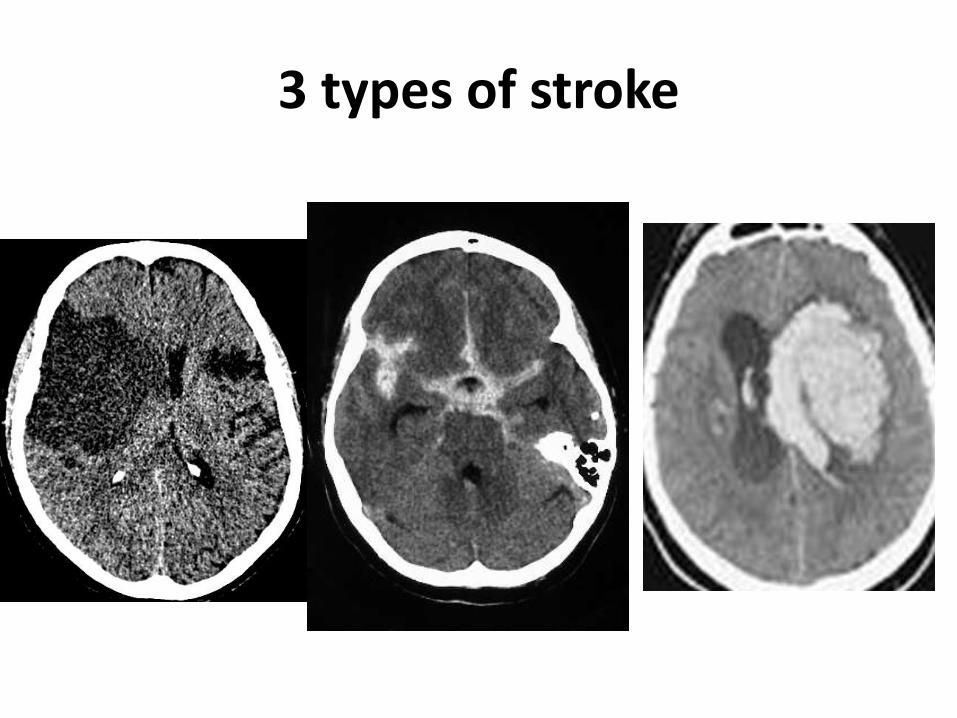
3 types of stroke




POOR PROGNOSTIC FACTORS IN STROKE
• Accompanying fever• Hypotension and severe hypertension• Low oxygen saturation• Hyperglycaemia and hypoglycemia• Total anterior circulation stroke (55% dead)• Pontine Haemorrhage• Low GCS score• heart failure• severity of hemiparesis

Total Ant. Cir. Syndrome
ALL OF THESE:-
Higher Dysfunction
Dysphasia
Visuospatial
Homonymous Hemianopia
Motor / Sensory Deficit
>2/3 Face / Arm / Leg

COMMON PITFALLS IN MANAGEMENT OF STROKE
• Aggressive early treatment of blood pressure in stroke.
• Misdiagnosis of haemorrhagic stroke as hypertensive encephalopathy.
• Failure of adequate hydration of patients
• Failure to diagnose and treat hypo/hyperglycemia
• Inability to effective diagnose and manage complications of stroke

Definition of Classes Used in AHA/ASA Recommendations
• Class I Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective.
• Class II Conditions for which there is conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment.
• Class IIa The weight of evidence or opinion is in favor of the procedure or treatment.
• Class IIb Usefulness/efficacy is less well established by evidence or opinion.
• Class III Conditions for which there is evidence and/or general agreement that the procedure or treatment is not useful/effective and in some cases may be harmful.

Definition of Levels of Evidence Used in AHA/ASA Recommendations
Therapeutic recommendations• Level of Evidence A Data derived from multiple randomized
clinical trials or meta-analyses• Level of Evidence B Data derived from a single randomized
trial or nonrandomized studies• Level of Evidence C Consensus opinion of experts, case
studies, or standard of careDiagnostic recommendations• Level of Evidence A Data derived from multiple prospective
cohort studies using a reference standard applied by a masked evaluator
• Level of Evidence B Data derived from a single grade A study or 1 or more case-control studies, or studies using a reference standard applied by an unmasked evaluator
• Level of Evidence C Consensus opinion of experts

Table 1 :PHASES OF CONTEMPORARY MANAGEMENT OF STROKE
Phases Period from onset Activities Prefered location
1Acute (emergency)
care:
hyperacute / acute
1st-7th day a)Assessment
b)Early supportive
care
Hospital
2 Early sub-
acute(supportive)
care
2nd-4th week a)prevention and
treatment of
complications
Hospital
3 Late sub-
acute(maintanance)
care
2nd-6th month a)Rehabilitation
b)Psychological
support
c)Prevent recurrence
Hospital/Community
4.Long-term (chronic)
care
7th month onwards a)Rehabilitation
b)Psychological
support
c)Social support
d)Prevent recurrence
Community
1/18/2015 31

MEDICAL MANAGEMENT1. supportive management- airway, temperature, blood pressure, blood glucose, cardiac assessement
2. thrombolysis – intravenous / intra arterial
3. antiplatelet drugs
4. anticoagulant drugs
5. hemodilution, vasodilators and induced hypertension
6. Neuroprotective agents

PREVENTION AND MANAGEMENT OF COMPLICATIONS
• Management of complications improves both short-term and long-term prognosis.
• Complications of stroke can be divided into General medical and Neurological complications.
• They can also be divided into Acute(<7 days) or subacute(>7days) based on time of occurrence.

SURGICAL MANAGEMENT
• For Ischemic stroke:A) endovascular interventions: angioplasty and stenting, mechanical clot disruption,clot extractionB)carotid endartectomyC) EC/IC bypass surgery
• For ICH: Surgical evacuation of haematoma• For Subarachnoid haemorrhage:Clipping and coiling of
aneurysm• Surgical decompression of cerebellar haematoma• Decompressive craniectomy for cerebral oedema• Ventricular drainage: pts with intra ventricular
haemorrhage and acute hydrocephalus.
EARLY SUPPORTIVE CARE
• 25 %of patients may have neurological worsening during first 24-48 hours.
• The use of stroke unit is recommended to improve general management.
• Nurse in slight head-up tilt to improve venous drainage from the head region.
• continuous monitoring of neurological deficit for deterioration, including the level of consciousness, which may herald impending herniation.
•

EARLY SUPPORTIVE CARE
• Continuous cardiac monitoring, if indicated, particularly if risk factors for coronary heart disease are present.
• Do not feed orally if patient is unconscious or drowsy. Swallowing test should be done in conscious patients before oral feeding and feed in the semi-recumbent position (450) – ensure correct consistency of food.
• Early mobilization of less severely affected patients
• Early physiotherapy should be initiated

AIRWAY AND VENTILATION
• Airway – Foreign Bodies, dentures, tongue• Patients who exhibit a decreasing level of
consciousness or signs of brain stem dysfunction are candidates for elective intubation .
• Indications for intubation- hypoxia (pO2 <60 mm Hg or PCO2 >50 mm Hg) -
risk of aspiration with or without impairment of arterial oxygenation
• elective tracheostomy should be performed after 2 weeks for prolonged coma or pulmonary complications

SUPPLEMENTAL OXYGEN
• Adequate tissue oxygenation is important to prevent further brain injury
• Current American Stroke Association recommendations call for supplemental oxygen to be given as needed to maintain an oxygen saturation of more than 95% by pulse Oximetry.

VOLUME STATUS
• Hypovolaemia has been associated with worse outcome and increased mortality in acute ischemic stroke.
• Isotonic saline, i.e. "normal" or 0.9%, should be used for volume repletion and maintenance, typically 3 litres per day is given.
• Do not give hypotonic solution, eg 5% Dextrose in water, as it may worsen cerebral oedema.

TEMPERATURE
• FEVER in the setting of acute stroke is associated with poor outcome possibly due to
• 1. increased metabolic demands• 2.enhanced release of neurotransmitters• 3.increased free radical production• Lowering acutely elevated body temperature
might improve the prognosis in stroke pateints.Antipyretic agents like acetaminophen and coolIng devices might be used .
• Relevant antibiotics might also be used.

TEMPERATURE
• Fever worsens outcome:
• for every 1°C rise in temp, risk of poor outcome doubles (Reith, Lancet 1996)
• Greatest effect in the first 24 hours
• Brain temp is generally higher than core
• Treat aggressively with acetaminophen

THROMBOLYSIS
• Thrombolysis within 1st 4.5 hrs (3-15% pts) • rtPA, alteplase; streptokinase. • Door to needle < 1 hr.• Patient
- Normal CT scan
- BP <180/100 mmHg.
- No bleeding tendency
• Dose - 0.9mg /Kg. (max 90mg)
• - 10% bolus, Rest 60 min by infusion
• Risk - ICH in 6% of patients
• - Reduced morbidity by 30%

BLOOD PRESSURE MANAGEMENT
• Reduction of BP in acute stroke phase is controversial
• BP Should be kept within higher normal limits since low BP could precipitate perfusion failure
• When treatment is indicated, cautious lowering of blood pressure by approximately 15 percent during the first 24 hours after stroke onset is suggested
• Systolic blood pressure > 185 and diastolic > 110 is a contraindication for thrombolysis

BLOOD PRESSURE MANAGEMENT
Reducing formation of brain edema
lessening hemorrhagic
transformation
preventing early recurrent stroke

BLOOD PRESSURE MANAGEMENT
HOWEVER , aggressive treatment of blood pressure may reduce the perfusion pressure to the ischemic areas of the brain
In majority of patients decline in blood pressure occurs within the first few hours of stroke even without any treatment

BLOOD PRESSURE MANAGMENT
• Some authorities believe BP should not be actively lowered in the 1st 10 days after stroke unless MAP > 145 (SBP > 220; DBP>120)
• Indications for lowering BP:-dissecting aortic aneurysm -Myocardial Ischemia or acute myocardial infarction-Acute pulmonary oedema. -Rapid decline in renal function.• Aim: MAP = 130; DBP = 105; (185/105)

BLOOD PRESSURE MANAGEMENT
In patients with markedly elevated blood pressure
who do not receive fibrinolysis, a reasonable goal
is to lower blood pressure by 15% during the first
24 hours after onset of stroke. The level of blood
pressure that would mandate such treatment is not
known, but consensus exists that medications should
be withheld unless the systolic blood pressure is >220
mm Hg or the diastolic blood pressure is >120 mm Hg
(Class I; Level of Evidence C).

BLOOD PRESSURE MANAGMENT
• Evidence from one clinical trial indicates that initiation of antihypertensive therapy within 24 hours of
stroke is relatively safe. Restarting antihypertensive
medications is reasonable after the first 24 hours for
patients who have preexisting hypertension and are
neurologically stable unless a specific contraindication
to restarting treatment is known (Class IIa; Level
of Evidence B).

BLOOD PRESSURE MANAGEMENT
• No data are available to guide selection of medications for the lowering of blood pressure in the setting of acute ischemic stroke
• If systolic BP >180–230 mm Hg or diastolic BP >105–120 mm Hg:-Labetalol 10 mg IV followed by continuous IV infusion
2–8 mg/min; or-Nicardipine 5 mg/h IV, titrate up to desired effect by
2.5 mg/h every 5–15 minutes, maximum 15 mg/h• If BP not controlled or diastolic BP >140 mm Hg,
consider IV sodium nitroprusside• use oral agents (captopril, calcium channel blockers)

BLOOD PRESSURE MANAGEMENT
• Systolic > 220 OR Diastolic 121 to 140: treat with goal of a 10% to 15% reduction in blood pressure using:
1. Labetalol 10 to 20 mg intravenously over 1 to 2 minutes (may repeat or double every 10 minutes; max dose is 300 mg) or
2. Nicardipine infusion, 5mg/hour, titrate up by 0.25 mg/hour at 5- to 15-minute intervals, maximum dose 15 mg/hour. When desired blood pressure is attained, reduce to 3 mg/hour

GUIDELINES FOR BP MGT IN HAEMORRHAGIC STROKE
• 1. Until ongoing clinical trials of BP intervention for ICH are completed, physicians must manage BP on the basis of the present incomplete efficacy evidence. Current suggested recommendations for target BP in various situations are available and may be considered (Class IIb; Level of Evidence: C). (Unchanged from the previous guideline)
• 2. In patients presenting with a systolic BP of 150 to 220 mm Hg, acute lowering of systolic BP to 140 mm Hg is probably safe (Class IIa; Level of Evidence: B).

GLYCAEMIC CONTROL
Hyperglycemia may augment brain injury by several mechanisms including
• increased tissue acidosis from anaerobic metabolism• free radical generation• increased blood brain barrier permeability.• Aggressive Glycaemic control utilizing a continuous insulin,
potassium, and glucose infusion(GKI) is feasible.• For patients with blood glucose >200 mg/dl, 6 units of
insulin hrly can be given until blood sugar is <120 mg/ dl.• GKI infusion may need to be continued in comatose
patients or those unable to swallow

GLYCAEMIC CONTROL
• HYPOGLYCEMIA- Hypoglycemia can cause focal neurologic deficits mimicking stroke, and severe hypoglycemia alone can cause neuronal injury
• Check the blood sugar and rapidly correct low serum glucose
• Hypoglycemia (blood glucose <60 mg/dL) should be treated in patients with acute ischemic stroke (Class I; Level of Evidence C).
• The goal is to achieve normoglycemia.

GLYCAEMIC CONTROL
• Evidence indicates that persistent in-hospital hyperglycemia during the first 24 hours after stroke is associated with worse outcomes than normoglycemia, and thus, it is reasonable to treat hyperglycemia to achieve blood glucose levels in a range of 140 to 180 mg/dL and to closely monitor to prevent hypoglycemia in patients with acute ischemic stroke (Class IIa; Level of Evidence C).

ANTI COAGULANTS
• Anticoagulation in acute ischemic stroke is not recommended for treatment of stroke.
• If hemiplegia is dense, commence subcutaneous Heparin 5,000 units 12 hourly(or 8hrly)
• low dose subcutaneous low-molecular-weight heparin or unfractionated heparin may be considered for prevention of DVT in patients with intracerebral haemorrhage after 4 days from onset (latest AHA/ASA guidelines)

ANTIPLATELET AGENTS
• Aspirin –within 48hrs – reduce risk of mortality/ disability in ischemic stroke
• Other antiplatelets: Abciximab - II B / III A inhibitor, Cilostazol - phosphodieterase (PDE ) type 3 inhibitor, Dipyridamole ,
• Antiplatelets contraindicated in haemorrhagicstroke

ANTIPLATELETS

Volume Expansion, Vasodilators,and Induced Hypertension
• The administration of high-dose albumin, Hemodilution by volume expansion, and administration of vasodilatory agents, is not recommended for treatment of ischemic stroke.

NEUROPROTECTIVE AGENTS
• Protect Neurones from adverse milleu created by the biochemical changes triggered by ischaemia:
attenuate neuronal injury
• Examples are free radical scavengers – Vit C ; E
encephabol (piritinol)
• At present, no pharmacological agents with putative
neuroprotective actions have demonstrated efficacy
in improving outcomes after ischemic stroke, and
therefore, other neuroprotective agents are not recommended (Class III; Level of Evidence A).

NEUROPROTECTIVE AGENTS
• In addition to their low-density lipoprotein cholesterol–lowering effects, statins, or HMG-CoA reductase inhibitors, exert acute neuroprotectiveproperties, including beneficial effects on endothelial function, cerebral blood flow, and inflammation.
• Among patients already taking statins at the time of onset of ischemic stroke, continuation of statin therapy during the acute period is reasonable (Class IIa;Level of Evidence B).

MEDICAL COMPLICATIONS OF STROKE
• Medical complications of stroke have been reported to occur in as high as 85% of patients with stroke (Langhorne et al, 2000).
• Medical complications account for at least 50% of mortality after the first week of stroke.
• The most commonly encountered complications are those related to immobility and infection.
• However, the most important causes of mortality in the early period following a stroke are cardiac (arrhythmias, myocardial infarction), infections (pneumonia, urosepsis), and venous thrombo-embolism (pulmonary embolus)

Medical Complications in HospitalizedPatients With Stroke
Complications of Immobility• Deep vein thrombosis/pulmonary embolism• Falls• Pressure sores or ulcerationInfections• Chest infection- aspiration pneumonia• Urinary tract infection• Other infectionsMalnutrition• Dysphagia• Dehydration

Medical Complications in HospitalizedPatients With Stroke
Pain• Shoulder pain (subluxation in the paretic limb)• Miscellaneous pain (headache, musculoskeletal)• Central post-stroke painNeuropsychiatric Disturbances• Depression, anxiety ,Emotional incontinence• Acute confusional states (delirium)Miscellaneous• Cardiac complications (arrhythmia, myocardial ischemia)• Gastrointestinal bleed• Constipation• Arthritis• Sleep apnea• Nutritional deficiencies

Deep Venous Thrombosisand Pulmonary Embolism
• The highest incidence occurs between the second and seventh day poststroke.(continuum)
• Estimates of early deaths attributable to PE range from 13% to 25% and occur most frequently between the second and fourth week.
• Measures to prevent DVT should be routine for all patients with ischemic stroke admitted to the hospital.

DVT PROPHYLAXIS
• Tight fitting knee-high or thigh-high antiembolicstockings reduce venous stasis in the leg.
• Pneumatic compression devices can be applied to the lower extremities of nonambulatory patients.
• The use of low-intensity anticoagulation for DVT prophylaxis is recommended for all immobilized patients with stroke. (Adams et al, 2007).
• In patients with primary intracerebralhemorrhage, initiation of anticoagulation for DVT prophylaxis is often delayed for 3 to 4 days.

DVT PROPHYLAXIS
• Early mobilization
• Mechanical compressive devices
Antiembolic stockings
Sequential pneumatic compression devices
• Subcutaneous unfractionated heparin
• Low-molecular-weight heparins
• patients with embolic infarction should not be treated with heparin or with any form of anticoagulant in the first 30 days.

2013 AHA/ASA GUIDELINES ON DVT PROPHYLAXIS
• The PREVAIL showed superiority of LMWH (Low Molecular weight Heparin)over UFH (Unfractionated Heparin)
• Early administration of Heparin for the prevention of early recurrent stroke,forimproving outcome after ischemic stroke, in patients with severe stenosis of internal carotid artery is not recommended

Malnutrition and aspiration
• Malnutrition and aspiration:
- A preserved gag reflex may not indicate safety with swallowing.
-Swallowing evaluation should be performed in all patients with dysarthria, aphasia, or facial, buccal, or lingual weakness.
-Inability to swallow safely should precipitate early placement of a naso-gastric tube in order to assure gastrointestinal access for nutrition and medications.

INFECTIONS
• Urinary tract infection:
this is common as a result of catheterization. Frequent urine culture and antibiotic treatment is required. To avoid pseudomonas infection, acidify urine by giving patient 2.4 g of vitamin C daily.
• Some specialists favour the use of parenteral Vitamin C for this purpose
• If possible the placement of indwelling bladder catheters should be avoided because of associated risk of UTI

1/18/2015 70
TABLE 2: ACUTE AND SUB-ACUTE COMPLICATIONS OF STROKE
Neurological Systemic
ACUTE (<7 days) 1.Cerebral oedema
2.Increased ICP
3.Hydrocephalous
4.Haemorrhagic
transformation
5.Seizures
6.Transtentorial herniation
1.Hypoxia
2.Hypertension
3.Hyperglycemia
4.Aspiration
5.Cardiac arrythmias
6.Inappropriate ADH secretion
SUB-ACUTE (>7 DAYS) 1.Seizures
2. Depression
1.D.V.T & Pulmonary
embolism
2.Bronchopneumonia
3.Urinary tract infections
4.Septicaemia
5.Decubitus ulcers
6.Joint stiffness

ACUTE NEUROLOGIC COMPLICATIONS OF STROKE
• This is the most common cause of deterioration in neurologic status in patients hospitalized for stroke.
• The most common neurologic complicationsCerebral edema-Mass effect and herniation- Hemorrhagic transformation- Seizures-Progressing ischemia (33%)- Recurrent stroke(11%) (Weimar et al, 2002).

TREATMENT OF RAISED ICP ANDCEREBRAL OEDEMA
• Usually occurs between 3-5 days of stroke• Clinical features include deteriorating levels of
consciousness, ipsilateral pupillary enlargement,worsening neurological status
• Patients may also have evidence of cushing’sreflex – elevated BP with bradycardia.
• Patients with intracerebral haemorrhage and large hemispheric infarcts are prone to raised intracranial pressure.
• Brain CT scan may show features of oedema or hydrocephalus(dilatation of ventricles)

TREATMENT OF RAISED ICP ANDCEREBRAL OEDEMA
• Elevation of head of the bed to 30 degrees• Pain relief and sedation• Normothermia• Hyperventilation• Administration of osmotic agents like mannitol,
hypertonic saline, glycerol,• Use of barbiturates• Surgical treatment like decompressive
craniectomy and placement of a ventricular drain in cases of hydrocephalus

TREATMENT OF RAISED ICP AND CEREBRAL OEDEMA
Intravenous mannitol is the treatment of choice to lower ICP.
It is administered as an initial bolus of 1 g/kg, followed by infusions of 0.25 to 0.5 g/kg every six hours. The goal of therapy is to achieve plasma hyperosmolality (300 to 310 mosmol/kg) while maintaining an adequate plasma volume..
Barbiturate anesthesia can be used if mannitol fails to lower ICP to an acceptable range. Barbiturate coma acts by reducing cerebral metabolism, which results in a lowering of cerebral blood flow and thus decreases ICP . Continuous electroencephalogram monitoring is suggested
The ICP lowering effect of hyperventilation to a PaCO2 of 25 to 30 mmHg is dramatic and rapid. However, the effect only lasts for minutes to a few hours.

Hemorrhagic transformation
• occurs in about 40%.• Occurs in first 2 weeks.• 10% of patients worsen.• Increased risk with antithrombotics,
anticoagulants, and thrombolytic therapy.• Size (>1/3rd) of the vascular territory and elderly
are more prone for hemorrhagic transformation. • Managed conservatively with short-term
discontinuation of antithrombotic agents and careful control of arterial blood pressure.

Seizures
• Protect patient from injury during ictus
• Maintain airway
• Benzodiazepines: – lorazepam (1-2 mg IV)
– diazepam (5-10 mg IV)
• Phenytoin: – 15 mg/kg loading dose, at 25-50 mg/min infusion with
cardiac monitor
• No need for prophylaxis

SURGICAL TREATMENT
• Surgical removal of hemorrhage with cerebellardecompression should be performed for patients with cerebellar hemorrhages greater than 3 cm in diameter who are deteriorating, or who have brainstem compression and/or hydrocephalus due to ventricular obstruction
• For patients with supratentorial ICH, current guidelines suggest consideration of standard craniotomy only for those who have lobar clots >30 mL within 1 cm of the surface.
• Mortality at 30 days in general compared with conservative management is not different.

MANAGEMENT OF SAH
• Bed rest Analgesic• Blood pressure control• TRIPLE – H therapy(hypervolemia , induced
hypertension, hemodilution )• Oral nimodipine 60mg q6hx21 days• Angiography for localization of bleeding• If aneurysm • Immediate surgical clipping for• Grade 1-3 patient without contraindication• Grade 4-5 with intracerebral clot and deterioratio

Secondary prevention of stroke
• Management of hypertension (goal <140/85 mm Hg)• Diabetes control (goal<126 mg/dL)• Lipid management: Statins (goal cholesterol<200 mg/dL,
LDL<100 mg/dL)• Anticoagulants: Warfarin (target INR 2 to 3); esp.
recommended in patients with cardioembolic stroke• Appropriate life style modification (cessation of smoking,
exercise, diet etc)• Antiplatelet agents:Antiplatelet agents such as
aspirin(300mg) reduce the risk of recurence of all ischaemicstroke & for patients with TIAs.
• Aspirin is not useful for preventing a first stroke in persons at low risk (Class III; Level of Evidence A).