Management of Recalcitrant Ulcers with 3M Tegaderm Ag … · A Scientific Perspective on the Use...
6
Management of Recalcitrant Ulcers with 3M ™ Tegaderm ™ Ag Mesh Dressing with Silver* by Salome Agbim ND, CNS, APRN, BC TH Wound Consultants Aurora, Colorado
Transcript of Management of Recalcitrant Ulcers with 3M Tegaderm Ag … · A Scientific Perspective on the Use...
Management of RecalcitrantUlcers with 3M™ Tegaderm™
Ag Mesh Dressing with Silver*bySalome Agbim ND, CNS, APRN, BCTH Wound Consultants Aurora, Colorado
1. White, RJ. et al. Topical Antimicrobials in the Control of Wound Bioburden. Ostomy Wound Management. 2006; 52 (8): 26-48.
2. Innes, ME. et al. the use of silver coated dressings on donor site wounds: a prospective, controlled matched pair study. Burns. 2001; 27 (6): 621-7.
3. Baxter, KA. et al. In vitro Assessment of the Microbidical Activity of3M™ Tegaderm™Ag Mesh Dressing with Silver Using a Short-term Time Kill Procedure. 3M 2006.
4. Burrell, RE. A Scientific Perspective on the Use of Topical Silver Preparations. Ostomy Wound Management. 2003, 5A: 19-24.
5. Fleck, CA, Paustian, C. The Use of Silver Containing Dressings: TheNew “Silver Bullet” in Wound Management? ECPN. July/August 2003; 22-25.
6. Ovington, L. The Truth About Silver. Ostomy Wound Management. 2004; 50 (9A): 1S-16S.
7. Harding, K. Non-healing wounds: recalcitrant, chronic, or not understood? OstomyWound Management. 2000; 46 (1-A Supplement):4S-7S.
References and Selected Bibliography
3M and Tegaderm are trademarks of 3M.Printed in U.S.A.© 3M 2006 All Rights Reserved.70-2009-7535-0
3
Health Care 3M Canada3M Center, Building 275-4W-02 Post Office Box 5757St. Paul, MN 55144-1000 London, Ontario N6A 4T1 USA Canada1 800 228 3957 1 800 563 2921www.3M.com/healthcare Please Recycle
ConclusionUse of this silver sulfate mesh dressing* led torapid closure of two chronic wounds thus ending acycle of expensive wound protocols and allowingpatients to regain their quality of life and dignity
once again. This easy-to-use dressing led to rapidand permanent closure of difficult wounds notachieved with a variety of other treatmentsincluding alternative silver dressings.
5 *3M™ Tegaderm™ Ag Mesh Dressing with Silver
7010053.qxd 1/4/07 2:09 PM Page 1
Management of Recalcitrant Ulcers with 3M™ Tegaderm™ Ag MeshDressing with Silver*Salome Agbim ND, CNS, APRN, BCTH Wound Consultants Aurora, Colorado
BackgroundNumerous dressings delivering ionic silver areavailable for wound care. These dressings differ inprimary material and construction, silver content,silver type, moisture management properties,versatility and ease of use.
Ability to kill or control microbes is of primaryimportance to clinicians caring for patients withrecalcitrant wounds. To achieve an antimicrobialbarrier effect, a dressing must contain a form ofsilver that readily releases soluble ionic silverwhen exposed to moisture. The greater thesolubility of the dressing’s silver compound, themore readily ionic silver can be generated.
The dressing must release enough silver to killmicrobes commonly seen in chronic wounds, e.g.S. aureus and Pseudomonas(1). Delivery ofexcessive silver is undesirable and has been shownto interfere with healing(2) and cause skin staining!
The dressing’s material and the method ofincorporating a silver compound also impactseffectiveness. Pad or fibrous dressings withembedded silver must first absorb moisture. Thesilver then must dissolve and diffuse to the surfaceof that material before being available to controlbacteria. This may impair ability of the material toprovide rapid reduction of microbes. A silvercompound on the surface of a material such asmesh or fiber, results in more silver available toreadily dissolve and generate ionic silver when itcomes into contact with moisture. Faster microbialkill will typically occur when a more water solubletype of silver is incorporated on the dressingsurface.
Versatility of the material is also important toclinicians. The ability to cut the dressing and use itin a variety of wounds is desirable. Conformability
allows packing into cavities, areas of underminingor tunnels commonly encountered in pressureulcers and open surgical wounds.
A dressing that can be moistened with normalsaline (readily available in most care settings) ismore convenient than one that requires sterilewater.
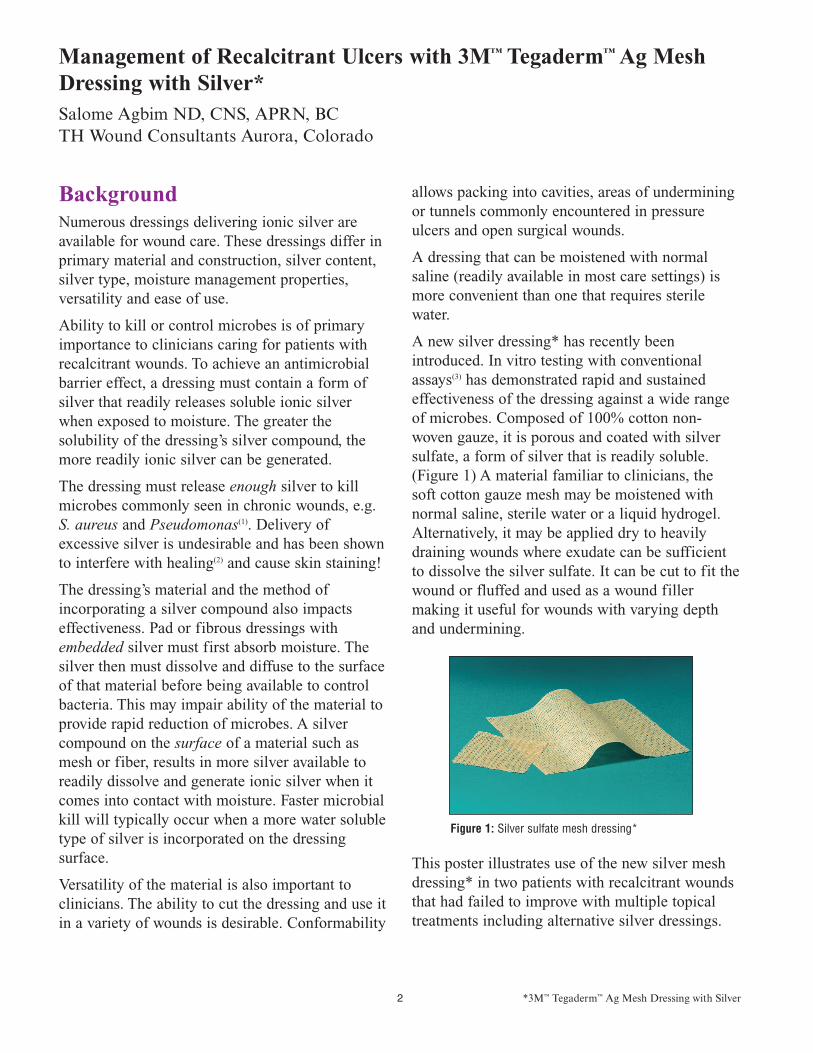
A new silver dressing* has recently beenintroduced. In vitro testing with conventionalassays(3) has demonstrated rapid and sustainedeffectiveness of the dressing against a wide rangeof microbes. Composed of 100% cotton non-woven gauze, it is porous and coated with silversulfate, a form of silver that is readily soluble.(Figure 1) A material familiar to clinicians, thesoft cotton gauze mesh may be moistened withnormal saline, sterile water or a liquid hydrogel.Alternatively, it may be applied dry to heavilydraining wounds where exudate can be sufficientto dissolve the silver sulfate. It can be cut to fit thewound or fluffed and used as a wound fillermaking it useful for wounds with varying depthand undermining.
This poster illustrates use of the new silver meshdressing* in two patients with recalcitrant woundsthat had failed to improve with multiple topicaltreatments including alternative silver dressings.
Figure 1: Silver sulfate mesh dressing*
2 *3M™ Tegaderm™ Ag Mesh Dressing with Silver 3 *3M™ Tegaderm™ Ag Mesh Dressing with Silver 4 *3M™ Tegaderm™ Ag Mesh Dressing with Silver
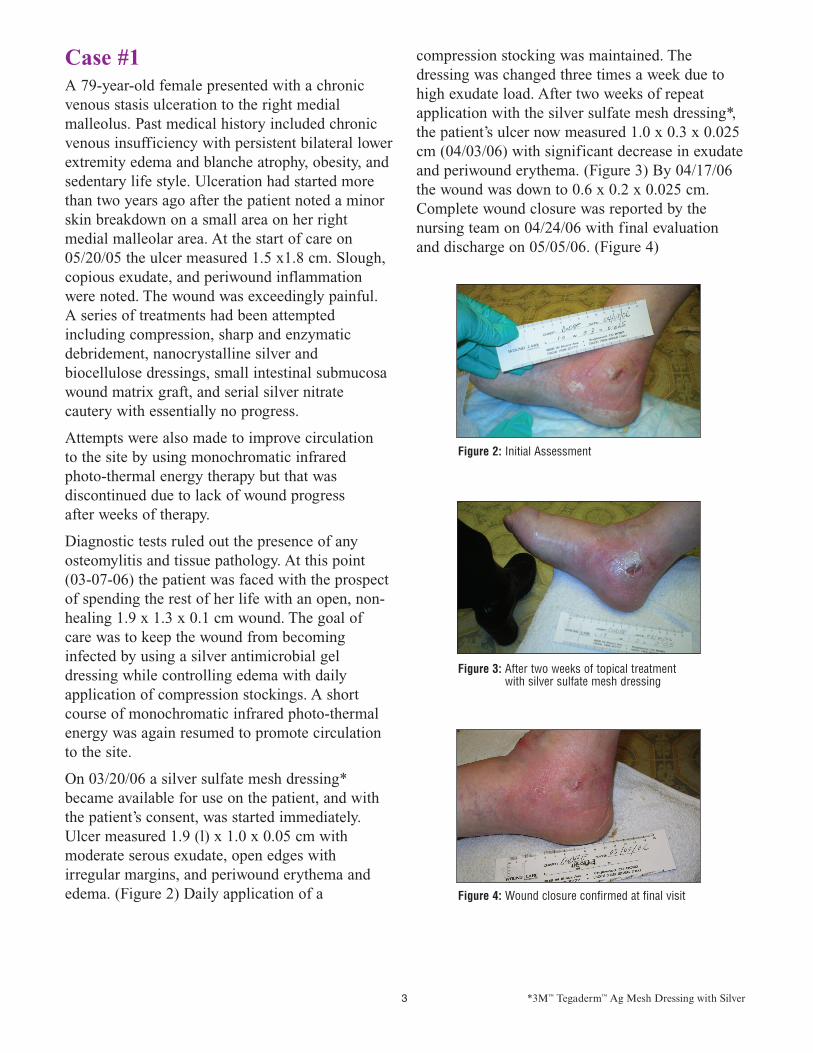
Case #1A 79-year-old female presented with a chronicvenous stasis ulceration to the right medial malleolus. Past medical history included chronicvenous insufficiency with persistent bilateral lowerextremity edema and blanche atrophy, obesity, andsedentary life style. Ulceration had started morethan two years ago after the patient noted a minorskin breakdown on a small area on her right medial malleolar area. At the start of care on05/20/05 the ulcer measured 1.5 x1.8 cm. Slough,copious exudate, and periwound inflammationwere noted. The wound was exceedingly painful.A series of treatments had been attemptedincluding compression, sharp and enzymaticdebridement, nanocrystalline silver andbiocellulose dressings, small intestinal submucosawound matrix graft, and serial silver nitratecautery with essentially no progress.
Attempts were also made to improve circulation to the site by using monochromatic infrared photo-thermal energy therapy but that wasdiscontinued due to lack of wound progress after weeks of therapy.
Diagnostic tests ruled out the presence of anyosteomylitis and tissue pathology. At this point(03-07-06) the patient was faced with the prospectof spending the rest of her life with an open, non-healing 1.9 x 1.3 x 0.1 cm wound. The goal ofcare was to keep the wound from becominginfected by using a silver antimicrobial geldressing while controlling edema with dailyapplication of compression stockings. A shortcourse of monochromatic infrared photo-thermalenergy was again resumed to promote circulationto the site.
On 03/20/06 a silver sulfate mesh dressing*became available for use on the patient, and withthe patient’s consent, was started immediately.Ulcer measured 1.9 (l) x 1.0 x 0.05 cm withmoderate serous exudate, open edges withirregular margins, and periwound erythema andedema. (Figure 2) Daily application of a
compression stocking was maintained. Thedressing was changed three times a week due tohigh exudate load. After two weeks of repeatapplication with the silver sulfate mesh dressing*,the patient’s ulcer now measured 1.0 x 0.3 x 0.025cm (04/03/06) with significant decrease in exudateand periwound erythema. (Figure 3) By 04/17/06the wound was down to 0.6 x 0.2 x 0.025 cm.Complete wound closure was reported by thenursing team on 04/24/06 with final evaluationand discharge on 05/05/06. (Figure 4)
Figure 2: Initial Assessment
Figure 3: After two weeks of topical treatmentwith silver sulfate mesh dressing
Figure 4: Wound closure confirmed at final visit
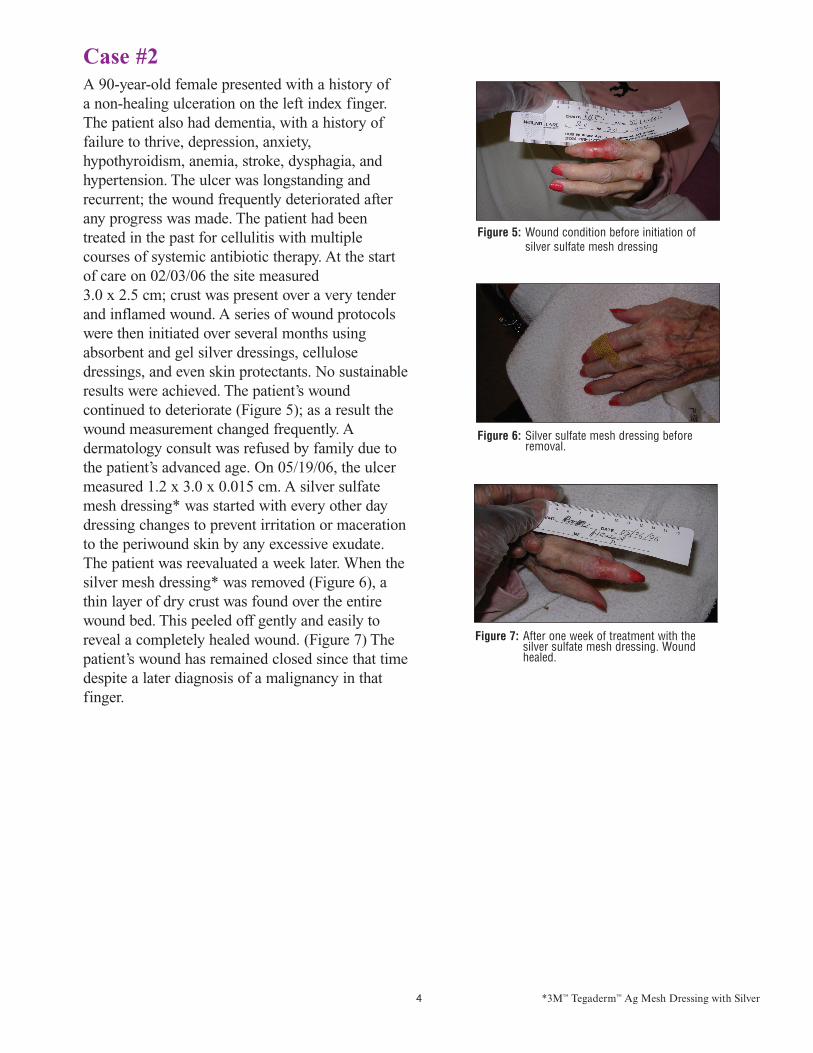
Case #2A 90-year-old female presented with a history of a non-healing ulceration on the left index finger.The patient also had dementia, with a history offailure to thrive, depression, anxiety,hypothyroidism, anemia, stroke, dysphagia, andhypertension. The ulcer was longstanding andrecurrent; the wound frequently deteriorated afterany progress was made. The patient had beentreated in the past for cellulitis with multiplecourses of systemic antibiotic therapy. At the startof care on 02/03/06 the site measured 3.0 x 2.5 cm; crust was present over a very tenderand inflamed wound. A series of wound protocolswere then initiated over several months usingabsorbent and gel silver dressings, cellulosedressings, and even skin protectants. No sustainableresults were achieved. The patient’s woundcontinued to deteriorate (Figure 5); as a result thewound measurement changed frequently. Adermatology consult was refused by family due tothe patient’s advanced age. On 05/19/06, the ulcermeasured 1.2 x 3.0 x 0.015 cm. A silver sulfatemesh dressing* was started with every other daydressing changes to prevent irritation or macerationto the periwound skin by any excessive exudate.The patient was reevaluated a week later. When thesilver mesh dressing* was removed (Figure 6), athin layer of dry crust was found over the entirewound bed. This peeled off gently and easily toreveal a completely healed wound. (Figure 7) Thepatient’s wound has remained closed since that timedespite a later diagnosis of a malignancy in thatfinger.
Figure 5: Wound condition before initiation of silver sulfate mesh dressing
Figure 6: Silver sulfate mesh dressing before removal.
Figure 7: After one week of treatment with thesilver sulfate mesh dressing. Woundhealed.
7010053.qxd 1/4/07 2:09 PM Page 2
Management of Recalcitrant Ulcers with 3M™ Tegaderm™ Ag MeshDressing with Silver*Salome Agbim ND, CNS, APRN, BCTH Wound Consultants Aurora, Colorado
BackgroundNumerous dressings delivering ionic silver areavailable for wound care. These dressings differ inprimary material and construction, silver content,silver type, moisture management properties,versatility and ease of use.
Ability to kill or control microbes is of primaryimportance to clinicians caring for patients withrecalcitrant wounds. To achieve an antimicrobialbarrier effect, a dressing must contain a form ofsilver that readily releases soluble ionic silverwhen exposed to moisture. The greater thesolubility of the dressing’s silver compound, themore readily ionic silver can be generated.
The dressing must release enough silver to killmicrobes commonly seen in chronic wounds, e.g.S. aureus and Pseudomonas(1). Delivery ofexcessive silver is undesirable and has been shownto interfere with healing(2) and cause skin staining!
The dressing’s material and the method ofincorporating a silver compound also impactseffectiveness. Pad or fibrous dressings withembedded silver must first absorb moisture. Thesilver then must dissolve and diffuse to the surfaceof that material before being available to controlbacteria. This may impair ability of the material toprovide rapid reduction of microbes. A silvercompound on the surface of a material such asmesh or fiber, results in more silver available toreadily dissolve and generate ionic silver when itcomes into contact with moisture. Faster microbialkill will typically occur when a more water solubletype of silver is incorporated on the dressingsurface.
Versatility of the material is also important toclinicians. The ability to cut the dressing and use itin a variety of wounds is desirable. Conformability
allows packing into cavities, areas of underminingor tunnels commonly encountered in pressureulcers and open surgical wounds.
A dressing that can be moistened with normalsaline (readily available in most care settings) ismore convenient than one that requires sterilewater.
A new silver dressing* has recently beenintroduced. In vitro testing with conventionalassays(3) has demonstrated rapid and sustainedeffectiveness of the dressing against a wide rangeof microbes. Composed of 100% cotton non-woven gauze, it is porous and coated with silversulfate, a form of silver that is readily soluble.(Figure 1) A material familiar to clinicians, thesoft cotton gauze mesh may be moistened withnormal saline, sterile water or a liquid hydrogel.Alternatively, it may be applied dry to heavilydraining wounds where exudate can be sufficientto dissolve the silver sulfate. It can be cut to fit thewound or fluffed and used as a wound fillermaking it useful for wounds with varying depthand undermining.
This poster illustrates use of the new silver meshdressing* in two patients with recalcitrant woundsthat had failed to improve with multiple topicaltreatments including alternative silver dressings.
Figure 1: Silver sulfate mesh dressing*
2 *3M™ Tegaderm™ Ag Mesh Dressing with Silver 3 *3M™ Tegaderm™ Ag Mesh Dressing with Silver 4 *3M™ Tegaderm™ Ag Mesh Dressing with Silver
Case #1A 79-year-old female presented with a chronicvenous stasis ulceration to the right medial malleolus. Past medical history included chronicvenous insufficiency with persistent bilateral lowerextremity edema and blanche atrophy, obesity, andsedentary life style. Ulceration had started morethan two years ago after the patient noted a minorskin breakdown on a small area on her right medial malleolar area. At the start of care on05/20/05 the ulcer measured 1.5 x1.8 cm. Slough,copious exudate, and periwound inflammationwere noted. The wound was exceedingly painful.A series of treatments had been attemptedincluding compression, sharp and enzymaticdebridement, nanocrystalline silver andbiocellulose dressings, small intestinal submucosawound matrix graft, and serial silver nitratecautery with essentially no progress.
Attempts were also made to improve circulation to the site by using monochromatic infrared photo-thermal energy therapy but that wasdiscontinued due to lack of wound progress after weeks of therapy.
Diagnostic tests ruled out the presence of anyosteomylitis and tissue pathology. At this point(03-07-06) the patient was faced with the prospectof spending the rest of her life with an open, non-healing 1.9 x 1.3 x 0.1 cm wound. The goal ofcare was to keep the wound from becominginfected by using a silver antimicrobial geldressing while controlling edema with dailyapplication of compression stockings. A shortcourse of monochromatic infrared photo-thermalenergy was again resumed to promote circulationto the site.
On 03/20/06 a silver sulfate mesh dressing*became available for use on the patient, and withthe patient’s consent, was started immediately.Ulcer measured 1.9 (l) x 1.0 x 0.05 cm withmoderate serous exudate, open edges withirregular margins, and periwound erythema andedema. (Figure 2) Daily application of a
compression stocking was maintained. Thedressing was changed three times a week due tohigh exudate load. After two weeks of repeatapplication with the silver sulfate mesh dressing*,the patient’s ulcer now measured 1.0 x 0.3 x 0.025cm (04/03/06) with significant decrease in exudateand periwound erythema. (Figure 3) By 04/17/06the wound was down to 0.6 x 0.2 x 0.025 cm.Complete wound closure was reported by thenursing team on 04/24/06 with final evaluationand discharge on 05/05/06. (Figure 4)
Figure 2: Initial Assessment
Figure 3: After two weeks of topical treatmentwith silver sulfate mesh dressing
Figure 4: Wound closure confirmed at final visit
Case #2A 90-year-old female presented with a history of a non-healing ulceration on the left index finger.The patient also had dementia, with a history offailure to thrive, depression, anxiety,hypothyroidism, anemia, stroke, dysphagia, andhypertension. The ulcer was longstanding andrecurrent; the wound frequently deteriorated afterany progress was made. The patient had beentreated in the past for cellulitis with multiplecourses of systemic antibiotic therapy. At the startof care on 02/03/06 the site measured 3.0 x 2.5 cm; crust was present over a very tenderand inflamed wound. A series of wound protocolswere then initiated over several months usingabsorbent and gel silver dressings, cellulosedressings, and even skin protectants. No sustainableresults were achieved. The patient’s woundcontinued to deteriorate (Figure 5); as a result thewound measurement changed frequently. Adermatology consult was refused by family due tothe patient’s advanced age. On 05/19/06, the ulcermeasured 1.2 x 3.0 x 0.015 cm. A silver sulfatemesh dressing* was started with every other daydressing changes to prevent irritation or macerationto the periwound skin by any excessive exudate.The patient was reevaluated a week later. When thesilver mesh dressing* was removed (Figure 6), athin layer of dry crust was found over the entirewound bed. This peeled off gently and easily toreveal a completely healed wound. (Figure 7) Thepatient’s wound has remained closed since that timedespite a later diagnosis of a malignancy in thatfinger.
Figure 5: Wound condition before initiation of silver sulfate mesh dressing
Figure 6: Silver sulfate mesh dressing before removal.
Figure 7: After one week of treatment with thesilver sulfate mesh dressing. Woundhealed.
7010053.qxd 1/4/07 2:09 PM Page 2
Management of Recalcitrant Ulcers with 3M™ Tegaderm™ Ag MeshDressing with Silver*Salome Agbim ND, CNS, APRN, BCTH Wound Consultants Aurora, Colorado
BackgroundNumerous dressings delivering ionic silver areavailable for wound care. These dressings differ inprimary material and construction, silver content,silver type, moisture management properties,versatility and ease of use.
Ability to kill or control microbes is of primaryimportance to clinicians caring for patients withrecalcitrant wounds. To achieve an antimicrobialbarrier effect, a dressing must contain a form ofsilver that readily releases soluble ionic silverwhen exposed to moisture. The greater thesolubility of the dressing’s silver compound, themore readily ionic silver can be generated.
The dressing must release enough silver to killmicrobes commonly seen in chronic wounds, e.g.S. aureus and Pseudomonas(1). Delivery ofexcessive silver is undesirable and has been shownto interfere with healing(2) and cause skin staining!
The dressing’s material and the method ofincorporating a silver compound also impactseffectiveness. Pad or fibrous dressings withembedded silver must first absorb moisture. Thesilver then must dissolve and diffuse to the surfaceof that material before being available to controlbacteria. This may impair ability of the material toprovide rapid reduction of microbes. A silvercompound on the surface of a material such asmesh or fiber, results in more silver available toreadily dissolve and generate ionic silver when itcomes into contact with moisture. Faster microbialkill will typically occur when a more water solubletype of silver is incorporated on the dressingsurface.
Versatility of the material is also important toclinicians. The ability to cut the dressing and use itin a variety of wounds is desirable. Conformability
allows packing into cavities, areas of underminingor tunnels commonly encountered in pressureulcers and open surgical wounds.
A dressing that can be moistened with normalsaline (readily available in most care settings) ismore convenient than one that requires sterilewater.
A new silver dressing* has recently beenintroduced. In vitro testing with conventionalassays(3) has demonstrated rapid and sustainedeffectiveness of the dressing against a wide rangeof microbes. Composed of 100% cotton non-woven gauze, it is porous and coated with silversulfate, a form of silver that is readily soluble.(Figure 1) A material familiar to clinicians, thesoft cotton gauze mesh may be moistened withnormal saline, sterile water or a liquid hydrogel.Alternatively, it may be applied dry to heavilydraining wounds where exudate can be sufficientto dissolve the silver sulfate. It can be cut to fit thewound or fluffed and used as a wound fillermaking it useful for wounds with varying depthand undermining.
This poster illustrates use of the new silver meshdressing* in two patients with recalcitrant woundsthat had failed to improve with multiple topicaltreatments including alternative silver dressings.
Figure 1: Silver sulfate mesh dressing*
2 *3M™ Tegaderm™ Ag Mesh Dressing with Silver 3 *3M™ Tegaderm™ Ag Mesh Dressing with Silver 4 *3M™ Tegaderm™ Ag Mesh Dressing with Silver
Case #1A 79-year-old female presented with a chronicvenous stasis ulceration to the right medial malleolus. Past medical history included chronicvenous insufficiency with persistent bilateral lowerextremity edema and blanche atrophy, obesity, andsedentary life style. Ulceration had started morethan two years ago after the patient noted a minorskin breakdown on a small area on her right medial malleolar area. At the start of care on05/20/05 the ulcer measured 1.5 x1.8 cm. Slough,copious exudate, and periwound inflammationwere noted. The wound was exceedingly painful.A series of treatments had been attemptedincluding compression, sharp and enzymaticdebridement, nanocrystalline silver andbiocellulose dressings, small intestinal submucosawound matrix graft, and serial silver nitratecautery with essentially no progress.
Attempts were also made to improve circulation to the site by using monochromatic infrared photo-thermal energy therapy but that wasdiscontinued due to lack of wound progress after weeks of therapy.
Diagnostic tests ruled out the presence of anyosteomylitis and tissue pathology. At this point(03-07-06) the patient was faced with the prospectof spending the rest of her life with an open, non-healing 1.9 x 1.3 x 0.1 cm wound. The goal ofcare was to keep the wound from becominginfected by using a silver antimicrobial geldressing while controlling edema with dailyapplication of compression stockings. A shortcourse of monochromatic infrared photo-thermalenergy was again resumed to promote circulationto the site.
On 03/20/06 a silver sulfate mesh dressing*became available for use on the patient, and withthe patient’s consent, was started immediately.Ulcer measured 1.9 (l) x 1.0 x 0.05 cm withmoderate serous exudate, open edges withirregular margins, and periwound erythema andedema. (Figure 2) Daily application of a
compression stocking was maintained. Thedressing was changed three times a week due tohigh exudate load. After two weeks of repeatapplication with the silver sulfate mesh dressing*,the patient’s ulcer now measured 1.0 x 0.3 x 0.025cm (04/03/06) with significant decrease in exudateand periwound erythema. (Figure 3) By 04/17/06the wound was down to 0.6 x 0.2 x 0.025 cm.Complete wound closure was reported by thenursing team on 04/24/06 with final evaluationand discharge on 05/05/06. (Figure 4)
Figure 2: Initial Assessment
Figure 3: After two weeks of topical treatmentwith silver sulfate mesh dressing
Figure 4: Wound closure confirmed at final visit
Case #2A 90-year-old female presented with a history of a non-healing ulceration on the left index finger.The patient also had dementia, with a history offailure to thrive, depression, anxiety,hypothyroidism, anemia, stroke, dysphagia, andhypertension. The ulcer was longstanding andrecurrent; the wound frequently deteriorated afterany progress was made. The patient had beentreated in the past for cellulitis with multiplecourses of systemic antibiotic therapy. At the startof care on 02/03/06 the site measured 3.0 x 2.5 cm; crust was present over a very tenderand inflamed wound. A series of wound protocolswere then initiated over several months usingabsorbent and gel silver dressings, cellulosedressings, and even skin protectants. No sustainableresults were achieved. The patient’s woundcontinued to deteriorate (Figure 5); as a result thewound measurement changed frequently. Adermatology consult was refused by family due tothe patient’s advanced age. On 05/19/06, the ulcermeasured 1.2 x 3.0 x 0.015 cm. A silver sulfatemesh dressing* was started with every other daydressing changes to prevent irritation or macerationto the periwound skin by any excessive exudate.The patient was reevaluated a week later. When thesilver mesh dressing* was removed (Figure 6), athin layer of dry crust was found over the entirewound bed. This peeled off gently and easily toreveal a completely healed wound. (Figure 7) Thepatient’s wound has remained closed since that timedespite a later diagnosis of a malignancy in thatfinger.
Figure 5: Wound condition before initiation of silver sulfate mesh dressing
Figure 6: Silver sulfate mesh dressing before removal.
Figure 7: After one week of treatment with thesilver sulfate mesh dressing. Woundhealed.
7010053.qxd 1/4/07 2:09 PM Page 2

Management of RecalcitrantUlcers with 3M™ Tegaderm™
Ag Mesh Dressing with Silver*bySalome Agbim ND, CNS, APRN, BCTH Wound Consultants Aurora, Colorado
1. White, RJ. et al. Topical Antimicrobials in the Control of Wound Bioburden. Ostomy Wound Management. 2006; 52 (8): 26-48.
2. Innes, ME. et al. the use of silver coated dressings on donor site wounds: a prospective, controlled matched pair study. Burns. 2001; 27 (6): 621-7.
3. Baxter, KA. et al. In vitro Assessment of the Microbidical Activity of3M™ Tegaderm™Ag Mesh Dressing with Silver Using a Short-term Time Kill Procedure. 3M 2006.
4. Burrell, RE. A Scientific Perspective on the Use of Topical Silver Preparations. Ostomy Wound Management. 2003, 5A: 19-24.
5. Fleck, CA, Paustian, C. The Use of Silver Containing Dressings: TheNew “Silver Bullet” in Wound Management? ECPN. July/August 2003; 22-25.
6. Ovington, L. The Truth About Silver. Ostomy Wound Management. 2004; 50 (9A): 1S-16S.
7. Harding, K. Non-healing wounds: recalcitrant, chronic, or not understood? OstomyWound Management. 2000; 46 (1-A Supplement):4S-7S.
References and Selected Bibliography
3M and Tegaderm are trademarks of 3M.Printed in U.S.A.© 3M 2006 All Rights Reserved.70-2009-7535-0
3
Health Care 3M Canada3M Center, Building 275-4W-02 Post Office Box 5757St. Paul, MN 55144-1000 London, Ontario N6A 4T1 USA Canada1 800 228 3957 1 800 563 2921www.3M.com/healthcare Please Recycle
ConclusionUse of this silver sulfate mesh dressing* led torapid closure of two chronic wounds thus ending acycle of expensive wound protocols and allowingpatients to regain their quality of life and dignity
once again. This easy-to-use dressing led to rapidand permanent closure of difficult wounds notachieved with a variety of other treatmentsincluding alternative silver dressings.
5 *3M™ Tegaderm™ Ag Mesh Dressing with Silver
7010053.qxd 1/4/07 2:09 PM Page 1

Management of RecalcitrantUlcers with 3M™ Tegaderm™
Ag Mesh Dressing with Silver*bySalome Agbim ND, CNS, APRN, BCTH Wound Consultants Aurora, Colorado
1. White, RJ. et al. Topical Antimicrobials in the Control of Wound Bioburden. Ostomy Wound Management. 2006; 52 (8): 26-48.
2. Innes, ME. et al. the use of silver coated dressings on donor site wounds: a prospective, controlled matched pair study. Burns. 2001; 27 (6): 621-7.
3. Baxter, KA. et al. In vitro Assessment of the Microbidical Activity of3M™ Tegaderm™Ag Mesh Dressing with Silver Using a Short-term Time Kill Procedure. 3M 2006.
4. Burrell, RE. A Scientific Perspective on the Use of Topical Silver Preparations. Ostomy Wound Management. 2003, 5A: 19-24.
5. Fleck, CA, Paustian, C. The Use of Silver Containing Dressings: TheNew “Silver Bullet” in Wound Management? ECPN. July/August 2003; 22-25.
6. Ovington, L. The Truth About Silver. Ostomy Wound Management. 2004; 50 (9A): 1S-16S.
7. Harding, K. Non-healing wounds: recalcitrant, chronic, or not understood? OstomyWound Management. 2000; 46 (1-A Supplement):4S-7S.
References and Selected Bibliography
3M and Tegaderm are trademarks of 3M.Printed in U.S.A.© 3M 2006 All Rights Reserved.70-2009-7535-0
3
Health Care 3M Canada3M Center, Building 275-4W-02 Post Office Box 5757St. Paul, MN 55144-1000 London, Ontario N6A 4T1 USA Canada1 800 228 3957 1 800 563 2921www.3M.com/healthcare Please Recycle
ConclusionUse of this silver sulfate mesh dressing* led torapid closure of two chronic wounds thus ending acycle of expensive wound protocols and allowingpatients to regain their quality of life and dignity
once again. This easy-to-use dressing led to rapidand permanent closure of difficult wounds notachieved with a variety of other treatmentsincluding alternative silver dressings.
5 *3M™ Tegaderm™ Ag Mesh Dressing with Silver
7010053.qxd 1/4/07 2:09 PM Page 1