Management of early rectal carcinoma Joint Hospital Surgical Grand Round Jeren Lim United Christian...
34
Management of early Management of early rectal carcinoma rectal carcinoma Joint Hospital Surgical Grand Round Jeren Lim United Christian Hospital
-
Upload
scott-oneal -
Category
Documents
-
view
214 -
download
1
Transcript of Management of early rectal carcinoma Joint Hospital Surgical Grand Round Jeren Lim United Christian...

Management of early rectal Management of early rectal carcinomacarcinoma
Joint Hospital Surgical Grand Round
Jeren LimUnited Christian Hospital

Early rectal carcinomaEarly rectal carcinomaAdenocarcinoma
invaded into, but not beyond the submucosa
T1N0M0 tumour3 – 8.6% of all
resected rectal carcinomas
Tytherleigh et al, Br J Surg 2008; 95: 409-423
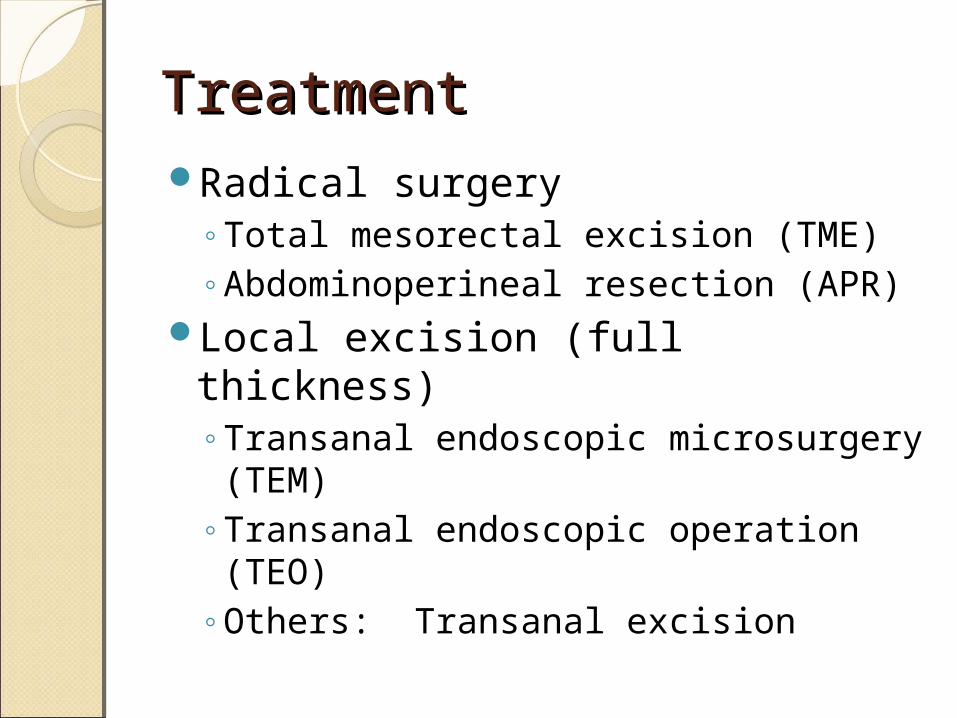
TreatmentTreatmentRadical surgery
◦Total mesorectal excision (TME)◦Abdominoperineal resection (APR)
Local excision (full thickness)◦Transanal endoscopic microsurgery
(TEM)◦Transanal endoscopic operation
(TEO)◦Others: Transanal excision

TEMTEMFull thickness excision1cm resection marginTumours at 6-15cm from anal
verge
Sharma et al, Surg Oncol 2003; 12: 51-61
Karita et al, Gastrointest Endosc 1991; 37: 128-132

TEM advantages vs radical TEM advantages vs radical surgerysurgeryLess major postoperative
complications (RR 0.16, P<0.0001)
Lower perioperative mortality (RR 0.15, P=0.03)
Avoids need for stoma (RR 0.11, P<0.00001)
Kidane et al, Dis Colon Rectum 2015; 58: 122-140

TEM advantages vs radical TEM advantages vs radical surgerysurgeryLower blood loss (P<0.001)Shorter operative time (103 vs
149mins, P<0.05)Shorter hospital stay (5.7 vs 15.4
days, P<0.0001)
Kunitake et al, Perm J 2012; 16: 45-50

TEOTEOModification of TEMHigh definition 2D TFT monitorStandard universal laparoscopic
instruments

TEO vs TEMTEO vs TEMLess steep learning curveRelatively shorter surgical timeLower overall costs (€2031 vs
€2603, P=0.003)
Nieuwenhuis et al, Surg Endosc 2009; 23: 80-86Serra-Aracil et al, World J Gastroenterol 2014; 20: 11538-11545

QuestionQuestionHow effective is local excision in
terms of oncological control?

Local excision vs radical Local excision vs radical surgerysurgeryA nationwide cohort studyNational Cancer Database of
American College of SurgeonsT1 rectal cancersHigher 5-year local recurrence
rate (12.5% vs 6.9%, P<0.003)Lower 5-year disease specific
survival rate (93.2% vs 97.2%, P=0.004) You et al, Ann Surg 2007; 245:
726-733

TEM vs radical surgeryTEM vs radical surgerySystemic review and meta-
analysisCompared oncological controlT1N0M0 rectal adenocarcinoma1 randomized controlled trial and
12 observational studies2855 patients
Kidane et al, Dis Colon Rectum 2015; 58: 122-140

TEM vs radical surgeryTEM vs radical surgery5-year local recurrence
Kidane et al, Dis Colon Rectum 2015; 58: 122-140

TEM vs radical surgeryTEM vs radical surgery5-year overall survival
Kidane et al, Dis Colon Rectum 2015; 58: 122-140

QuestionQuestionHow to select the suitable
patients for local excision?

Management controversyManagement controversyLocal excision does not remove
the mesorectum and regional LNProblem of predicting the N
(nodal) staging in T1 tumours
Tytherleigh et al, Br J Surg 2008; 95: 409-423

Lymph node metastasisLymph node metastasisT1 tumours: 0-12%T2 tumours: 12-28%T3 tumours: 36-79%
Chang et al, J Surg Educ 2008; 65(1): 67-72

Preoperative locoregional Preoperative locoregional stagingstagingEndorectal ultrasound (ERUS)
◦T-staging accuracy: 69-97%◦N-staging accuracy: 61-80%
Klessen et al, Eur Radiol 2007; 17: 379-389

Preoperative locoregional Preoperative locoregional stagingstagingMagnetic resonance imaging
(MRI)◦T-staging accuracy: 67-86%◦N-staging accuracy: 57-85%
Klessen et al, Eur Radiol 2007; 17: 379-389

Preoperative locoregional Preoperative locoregional stagingstagingDifficult for MRI to differentiate
between T1 and T2 tumours.ERUS is more valuable for T-
stagingCombination of ERUS and MRI is
useful for N-staging
Mulla et al, Indian J Radiol Imaging 2010; 20: 118-121Muthusamy et al, Clin Cancer Res 2007; 13: 6877-6884

Preoperative stagingPreoperative stagingNo imaging modality can
completely rule out mesorectal nodal involvement
Thus pathological examination after local excision is necessary
Categorize T1 tumours into low or high risk
Iafrate et al, Radiographics 2006; 26: 701-714
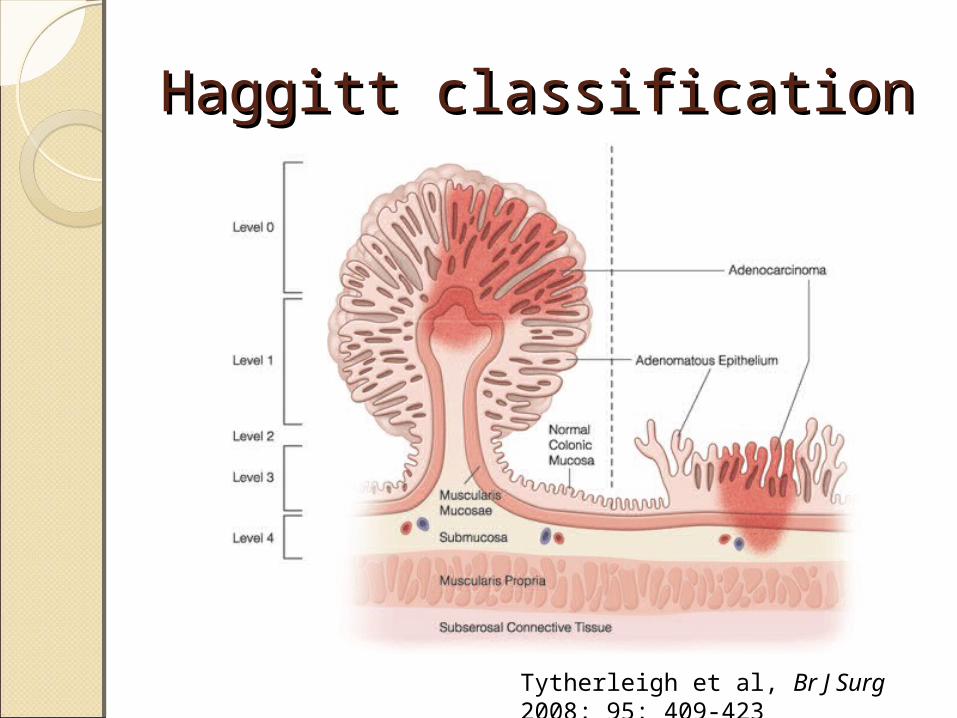
Haggitt classificationHaggitt classification
Tytherleigh et al, Br J Surg 2008; 95: 409-423

Kikuchi classificationKikuchi classification
Kikuchi et al, Dis Colon Rectum 1995; 38: 1286-1295
0-3.2%
8-11%
12-25%
Lymph node metastasis

Histopathological features of Histopathological features of T1 tumoursT1 tumours
Low risk High risk
Differentiation Well, moderate Poor
Haggitt level 1-3 -
Kikuchi level Sm1, +/- Sm2 Sm3, +/- Sm2
Lymphatic or vascular invasion
No Yes
Resection margin involvement
No Yes
Tytherleigh et al, Br J Surg 2008; 95: 409-423

Low risk vs high riskLow risk vs high riskLong term results from the
Memorial Sloan-Kettering Cancer Center
Paty et al, Ann Surg 2002; 236: 522-529
Disease specific survival

Immediate salvage Immediate salvage surgerysurgeryHigh risk T1 tumoursNo compromise in outcome when
performed immediately after local excision
30-day mortality (P=0.49)Local recurrence (P=0.49)Distant metastasis (P=0.61)
Levic et al, Tech Coloproctol 2013; 17: 397-403

Local recurrenceLocal recurrenceSalvage surgeryOutcomes are inferior to those
who initially received radical surgery
Only 59% were disease free at a mean follow-up of 39 months after salvage surgery
Friel et al, Dis Colon Rectum 2002; 45: 875-879

QuestionQuestionIs there a role for adjuvant
therapy?
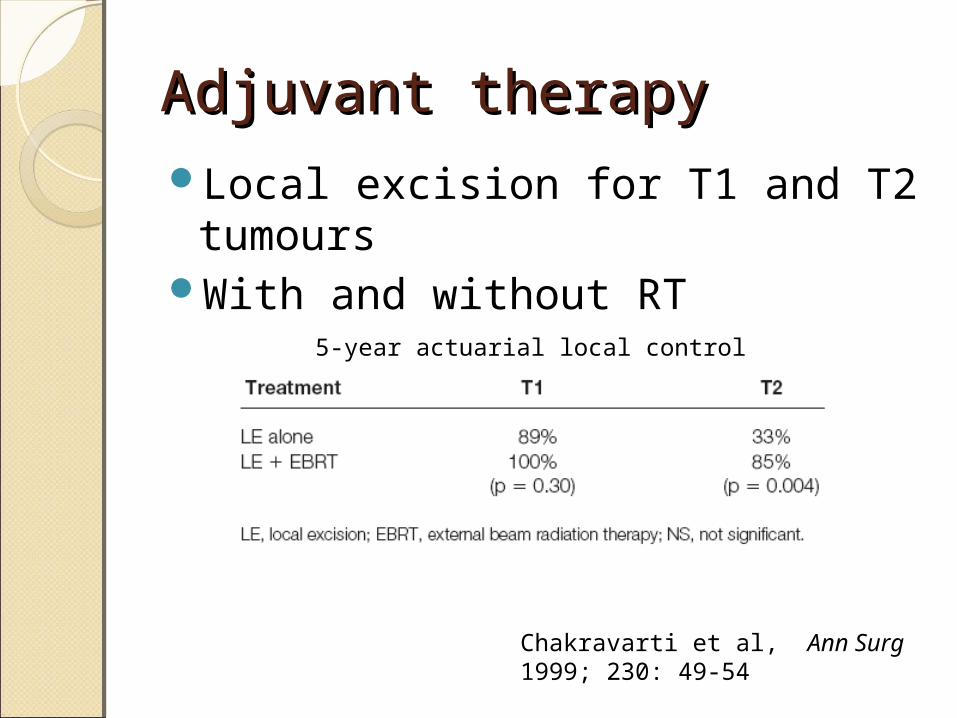
Adjuvant therapyAdjuvant therapyLocal excision for T1 and T2
tumoursWith and without RT
Chakravarti et al, Ann Surg 1999; 230: 49-54
5-year actuarial local control
Adjuvant therapyAdjuvant therapyLocal excision + RT +
chemotherapyT1 and T2 cancers5-year local control rates
increased from 81% to 96%Not significant (P=0.15)
Chakravarti et al, Ann Surg 1999; 230: 49-54

Adjuvant therapyAdjuvant therapySystemic review of 11 studiesLocal excision with chemoRT in
T1 and T2 cancersLocal recurrence 10%Overall survival 75%Disease specific survival 89%
Ung et al, Colorectal Dis 2014; 16: 502-515

NCCN guidelines 2015NCCN guidelines 2015Early rectal carcinoma
High risk pT1, NX T2, NX
Low risk pT1, NX
ERUS, MRI
cT1, N0(Size <3cm, <30% bowel circumference, mobile)
Local excision
Salvage surgery
Surveillance

ConclusionConclusionTEM has a comparable overall
survival rate to radical surgery in T1N0M0 rectal cancers
Higher local recurrence ratePatient selection is importantImaging and histopathological
features help to predict lymph node metastases

ConclusionConclusionFull thickness local excision by
TEM / TEO is suitable for low risk T1 rectal carcinomas
Immediate salvage surgery recommended if high risk features present
Adjuvant therapy showed no significant benefit in T1 cancers

Thank youThank you