MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE · 3 MANAGEMENT OF CHRONIC OBSTRUCTIVE...
8
Academy of Medicine Malaysia Malaysian Thoracic Society Ministry of Health Malaysia QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE [2 nd Edition]
Transcript of MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE · 3 MANAGEMENT OF CHRONIC OBSTRUCTIVE...

Academy of Medicine Malaysia Malaysian Thoracic SocietyMinistry of Health Malaysia
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
MANAGEMENT OFCHRONIC OBSTRUCTIVE PULMONARY DISEASE
[2nd Edition]

2
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERS
Diagnosis and Assessment of COPDA diagnosis of COPD should be considered in any individual with symptoms of chronic cough, sputum production or dyspnoea and a history of exposure to risk factors for the disease, especially cigarette smoking.
The diagnosis should be confirmed by spirometry showing a post-bronchodilator FEV1/
FVC ratio of less than 70%.
COPD severity should be assessed based on the severity of spirometric abnormality, symptoms, exercise capacity, complications and the presence of co-morbidities.
Table 1: Classification of COPD Severity Based on Spirometric Impairment and Symptoms
COPD stage Severity
Classification by post-bronchodilator spirometric values
Classification by symptoms and disability
I Mild FEV1/FVC < 0.70FEV1 > 80% predicted
Shortness of breath when hurrying on the level or walking up a slight hill (MMRC 1)
II Moderate FEV1/FVC < 0.7050% < FEV1 < 80% predicted
Walks slower than people of the same age on the level because of breathlessness; or stops for breath after walking about 100 m or after a few minutes at own pace on the level (MMRC 2 to 3)
III Severe FEV1/FVC < 0.7030% < FEV1 < 50% predicted
Too breathless to leave the house or breathless when dressing or undressing (MMRC 4)
IV Very severe
FEV1/FVC < 0.70FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure
Presence of chronic respiratory failure or clinical signs of right heart failure
*Should there be disagreement between FEV1 and symptoms, follow symptoms
3
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERS
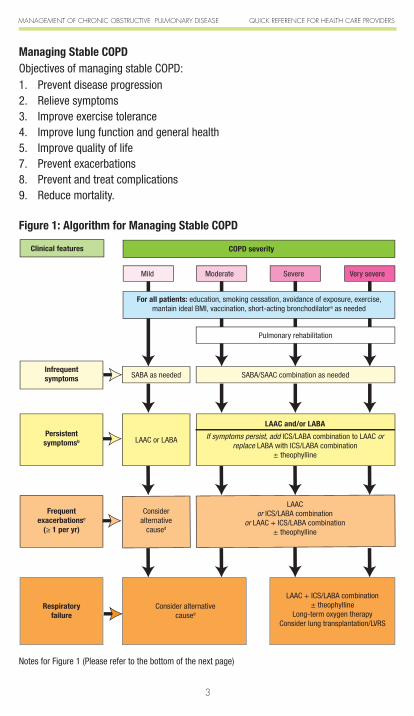
Managing Stable COPDObjectives of managing stable COPD:1. Prevent disease progression2. Relieve symptoms3. Improve exercise tolerance4. Improve lung function and general health5. Improve quality of life7. Prevent exacerbations8. Prevent and treat complications9. Reduce mortality.
Figure 1: Algorithm for Managing Stable COPD
COPD severity
Pulmonary rehabilitation
Clinical features
Infrequentsymptoms SABA/SAAC combination as needed
Mild
SABA as needed
Persistentsymptomsb LAAC or LABA
Moderate Severe Very severe
For all patients: education, smoking cessation, avoidance of exposure, exercise, mantain ideal BMI, vaccination, short-acting bronchodilatora as needed
LAAC and/or LABA
If symptoms persist, add ICS/LABA combination to LAAC or replace LABA with ICS/LABA combination
± theophylline
Frequentexacerbationsc
(≥ 1 per yr)
Consideralternative
caused
LAAC or ICS/LABA combination
or LAAC + ICS/LABA combination± theophylline
Respiratoryfailure
Consider alternativecaused
LAAC + ICS/LABA combination± theophylline
Long-term oxygen therapy Consider lung transplantation/LVRS
Notes for Figure 1 (Please refer to the bottom of the next page)

4
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERS
Figure 2: Algorithm for Managing Stable COPD in Resource-Limited Settings
COPD severity
Pulmonary rehabilitation
Clinical feature
Infrequentsymptoms SABA/SAAC combination as needed
Mild
SABA as needed
Persistentsymptomsb
SABA/SAACcombination
regularly
Moderate Severe Very severe
For all patients: education, smoking cessation, avoidance of exposure, exercise, maintain ideal BMI, vaccination, short-acting bronchodilatora as needed
Frequentexacerbationsc
(≥ 1 per yr)
Consideralternative
caused
SABA/SAAC combination regularly + ICS + theophylline
(Consider referring to a tertiary centre to obtain long-acting bronchodilators)
Respiratory failureConsider alternative
caused
SABA/SAAC combination regularly + ICS + theophylline
Long-term oxygen therapy Consider lung transplantation/LVRS
SABA/SAAC combination regularly
If symptoms persist, add theophylline and/or ICS
Clinical features
Notes:1. SABA – Short-acting β2 agonist; SAAC – Short-acting anticholinergic; LAAC – Long-acting anticholinergic;
LABA – Long-acting β2 agonist; ICS – Inhaled corticosteroid; LVRS – lung volume reduction surgery
2. ICS dose per day should be at least 500 µg of fluticasone or 800 µg of budesonide
a. All COPD patients, irrespective of disease severity, should be prescribed SABA or SABA/SAAC combination (Berodual®/Combivent®) as needed. SABA has a more rapid onset of bronchodilatation than SAAC.
b. Defined as need for rescue bronchodilators more than twice a week.
c. Frequent exacerbation is defined as one or more episodes of COPD exacerbation requiring systemic corticosteroids ± antibiotics and/or hospitalisation over the past one year
d. Consider alternative causes - it is less common for patients with mild COPD to have frequent exacerbations; similarly, respiratory failure is uncommon in patients with mild to moderate COPD severity. Hence, in such patients, an alternative cause should be explored even if the COPD diagnosis is firmly established.

5
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERS
Table 2: Evidence-based Interventions in Stable COPD
Intervention Outcome Level of evidence*
Smoking cessation FEV1 decline, mortality I
Influenza vaccination COPD exacerbations, all-cause mortality (in patients aged ≥ 65 years during influenza season)
II-1
Pneumococcal vaccination community-acquired pneumonia II-2
Inhaled short-acting β2-agonists
post-bronchodilator FEV1,
dyspnoeaI
Inhaled long-acting β2-agonists
post-bronchodilator FEV1, symptoms,
QoL, COPD exacerbationsI
Inhaled short-acting anticholinergic
post-bronchodilator FEV1, dyspnoea I
Inhaled long-acting anticholinergic (tiotropium)
post-bronchodilator FEV1, symptoms,
exercise tolerance, QoL, COPD exacerbations, mortality
I
Inhaled corticosteroids FEV1, QoL, COPD exacerbations I
Inhaled long-acting β2-agonist and
inhaled corticosteroid combination [Seretide Accuhaler (salmeterol 50 µg/fluticasone 500 µg) twice daily, and Symbicort Turbuhaler (budesonide/formoterol 320/9 µg) twice daily]
post-bronchodilator FEV1, QoL,
COPD exacerbationsI
Oral theophylline Small FEV1, symptoms II-1
Long-term oxygen therapy mortality
(in patients with respiratory failure)I
Pulmonary rehabilitation
dyspnoea, exercise capacity, QoL, anxiety and depression associated
with COPD
I
number of hospitalisations and days in hospital
II-1
peripheral muscle strength II-2
Lung volume reduction surgery FEV
1, exercise tolerance, QoL,
mortalityI
* Refer to Table 4↓ : reduces, ↑ : increases or improves, QoL : quality of life

6
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERS
Managing Acute Exacerbations of COPDObjectives of managing exacerbations of COPD: • Relievesymptomsandairflowobstruction• Maintainadequateoxygenation• Treatanyco-morbidconditionsthatmaycontributetotherespiratorydeterioration• Treatanyprecipitatingfactorsuchasinfection
Table 3: Evidence-based Interventions in Acute Exacerbations of COPD
Intervention Outcome Level of evidence*
Inhaled short-acting β2-agonists FEV
1, dyspnoea I
Inhaled short-acting anticholinergic FEV1, dyspnoea I
Intravenous aminophylline FEV1, dyspnoea II-1
Systemic corticosteroids FEV1, shorten recovery time,
hypoxaemia I
Antibiotics
short-term mortality, treatment failure, sputum purulence(in patients with purulent sputum and increased dyspnoea or increased sputum volume, and in patients requiring ventilatory support)
II-1
Supplemental oxygen hypoxaemia III
Non-invasive ventilation intubation, mortality, length of hospital stay (in acute respiratory failure) I
* Refer to Table 4↓ : reduces, ↑ : increases or improves
Table 4: US / Canadian Preventive Services Task Force Level of Evidence Scale
I Evidence obtained from at least one properly randomized controlled trial
II - 1 Evidence obtained from well-designed controlled trials without randomization
II - 2 Evidence obtained from well-designed cohort or case-control analytic studies, preferably from more than one center or research group
II - 3 Evidence obtained from multiple time series with or without intervention. Dramatic results in uncontrolled experiments (such as the results of the introduction of penicillin treatment in the 1940s) could also be regarded as this type of evidence
III Opinions of respected authorities, based on clinical experience; descriptive studies and case reports; or reports of expert committees

7
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERSFi
gure
3: A
lgor
ithm
for M
anag
ing
Acut
e Ex
acer
batio
ns o
f COP
D: H
ome
Man
agem
ent
Patie
nt wi
th AE
COPD
None
• Inh
aled s
hort-
actin
g bron
chod
ilator
(SAB
A +
SAAC
) from
pMDI
via a
spac
er de
vice o
r ne
bulis
er de
pend
ing on
seve
rity
Good
resp
onse
toini
tial tr
eatm
ent
• Di
scha
rge w
ith fo
llow-
up •
Chec
k inh
aler te
chniq
ue •
Arran
ge ap
propri
ate in
vesti
gatio
ns if
this i
s a
new
prese
ntatio
n •
Refer
to sp
ecial
ist if
nece
ssary
Home
Man
agem
ent
• Inc
rease
dose
and f
reque
ncy o
f inha
led sh
ort-ac
ting b
ronch
odila
tor (S
ABA +
SAA
C) fro
m pM
DI•
Oral
predn
isolon
e 30-4
0 mg d
aily f
or 7-1
4 day
s (if t
here
is sig
nifica
nt dy
spno
ea or
base
line F
EV1 <
50%
predic
ted)
• Or
al an
tibiot
ics if
patie
nt ha
s 2 ou
t of 3
cardi
nal s
ympto
ms (ie
, puru
lent s
putum
, incre
ased
sputu
m vo
lume,
increa
sed d
yspn
oea)
Obta
in rel
evan
t hist
ory: U
nderl
ying C
OPD
seve
rity (if
know
n), co
-morb
iditie
s, pre
sent
treatm
ent re
gimen
Hosp
ital a
sses
smen
t or a
dmiss
ion in
dicate
d
Admi
nister
initia
l trea
tmen
t: •
Inhale
d sho
rt-ac
ting b
ronch
odila
tors
(SAB
A + S
AAC)
from
pMDI
via a
sp
acer
devic
e or n
ebuli
ser
• Or
al pre
dniso
lone (
or int
raven
ous
hydro
cortis
one i
f pati
ent u
nable
to
swall
ow or
vomi
ts)•
Start
initia
l dos
e of a
ntibio
tics
(if ap
propri
ate)
• Su
pplem
ental
oxyg
en th
erapy
(pr
eferab
ly via
Ventu
ri mas
k) if
Sp
O 2 < 90
%, ai
m for
SpO
2 90-93
%
Refer
to ne
arest
hosp
ital
or
patie
nt’s u
sual
hosp
ital
Failu
re to
impro
ve
Indica
tions
for h
ospit
al as
sess
ment
or ad
miss
ion:
• Ma
rked i
ncrea
se in
inten
sity o
f sym
ptoms
such
as
sudd
en de
velop
ment
of dy
spno
ea•
Unde
rlying
seve
re CO
PD•
Deve
lopme
nt of
new
phys
ical s
igns e
.g., c
yano
sis,
perip
heral
oede
ma•
Haem
odyn
amic
instab
ility
• Re
duce
d aler
tness
• Fa
ilure
of ex
acerb
ation
to re
spon
d to i
nitial
med
ical
mana
geme
nt •
Signif
icant
co-m
orbidi
ties
• Ne
wly o
ccurr
ing ca
rdiac
arrhy
thmias
• Ol
der a
ge•
Insuff
icien
t hom
e sup
port
Any i
ndica
tion f
or ho
spita
l ass
essm
ent o
r adm
ission
?

8
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE QUICK REFERENCE FOR HEALTH CARE PROVIDERSFi
gure
4: A
lgor
ithm
for M
anag
ing
Acut
e Ex
acer
batio
ns o
f COP
D: H
ospi
tal M
anag
emen
t
Patie
nt w
ith A
ECOP
D
Good
resp
onse
• Di
scha
rge
with
follo
w-up
• Ch
eck i
nhale
r tec
hniqu
e •
Refe
r to
spec
ialist
if th
is is
a ne
w pr
esen
tatio
n
Hom
e M
anag
emen
t•
Incr
ease
dos
e an
d fre
quen
cy o
f inha
led
shor
t-acti
ng b
ronc
hodil
ator
(SAB
A +
SAAC
) fro
m
pMDI
• Or
al pr
ednis
olone
30-
40 m
g da
ily fo
r 7-1
4 da
ys•
Ensu
re a
dequ
ate
supp
ly of
ora
l ant
ibiot
ics if
starte
d
Failu
re to
impr
ove
Hosp
ital M
anag
emen
t•
Cont
rolle
d su
pplem
enta
l oxy
gen
ther
apy t
o m
ainta
in Pa
O 2 > 8
kPa
or
Sp
O 2 > 9
0% w
ithou
t wor
senin
g hy
perc
apnia
or p
recip
itatin
g ac
idosis
•
Inha
led sh
ort-a
cting
bro
ncho
dilat
ors f
rom
pM
DI vi
a a
spac
er d
evice
or
nebu
liser
• Co
nside
r int
rave
nous
am
inoph
ylline
if ina
dequ
ate
resp
onse
to in
haled
sh
ort-a
cting
bro
ncho
dilat
ors
• Sy
stem
ic co
rtico
stero
ids fo
r 7-1
4 da
ys•
Antib
iotics
(if a
ppro
priat
e)•
Mon
itor f
luid
balan
ce a
nd n
utrit
ion•
Cons
ider s
ubcu
tane
ous h
epar
in•
Clos
ely m
onito
r con
dition
of t
he p
atien
t•
Cons
ider i
nvas
ive o
r non
-inva
sive
vent
ilatio
n
Indi
catio
ns fo
r hos
pita
l adm
issi
on:
• M
arke
d inc
reas
e in
inten
sity o
f sym
ptom
s su
ch a
s sud
den
deve
lopm
ent o
f dy
spno
ea•
Unde
rlying
seve
re C
OPD
• De
velop
men
t of n
ew p
hysic
al sig
ns e
.g.,
cyan
osis,
per
ipher
al oe
dem
a•
Haem
odyn
amic
insta
bility
• Re
duce
d ale
rtnes
s•
Failu
re o
f exa
cerb
ation
to re
spon
d to
ini
tial m
edica
l man
agem
ent
• Si
gnific
ant c
o-m
orbid
ities
• Ne
wly o
ccur
ring
card
iac a
rrhyth
mias
• Ol
der a
ge•
Insu
fficien
t hom
e su
ppor
t
• Ob
tain
relev
ant h
istor
y: Cu
rrent
sym
ptom
s, re
cent
trea
tmen
t fro
m o
ther
doc
tors
, COP
D se
verit
y, pr
eviou
s epis
odes
(A
ECOP
D/ho
spita
l adm
ission
/ICU
adm
ission
/inva
sive
or n
on-in
vasiv
e ve
ntila
tion)
• Ex
amine
for d
ange
r sign
s: Re
spira
tory
dist
ress
, tac
hyar
rhyth
mia,
cyan
osis,
hea
rt fa
ilure
, exh
austi
on.
• Ar
rang
e ap
prop
riate
inve
stiga
tions
: ABG
(not
e th
e Fi
O 2), F
BC, B
USEC
r, LF
T, blo
od g
lucos
e, C
XR, E
CG, s
putu
m C
&S
Adm
inis
ter i
nitia
l tre
atm
ent:
• Co
ntro
lled
oxyg
en th
erap
y if S
pO2 <
90%
, aim
for S
pO2 9
0-93
%•
Inha
led sh
ort-a
cting
bro
ncho
dilat
ors (
SABA
+ S
AAC)
from
pM
DI vi
a a
spac
er d
evice
or n
ebuli
ser
• Or
al pr
ednis
olone
(int
rave
nous
hyd
roco
rtiso
ne if
patie
nt u
nable
to sw
allow
or v
omits
)•
Star
t ant
ibiot
ics if
patie
nt h
as 2
out
of 3
card
inal s
ympt
oms (
i.e, p
urule
nt sp
utum
, incr
ease
d sp
utum
volum
e, in
crea
sed
dysp
noea
)
No in
dicat
ion fo
r hos
pital
adm
ission
Adm
it to
hosp
ital