MANAGEMENT OF CERVICAL INTRAEPITHELIAL NEOPLASIA. DR OMOLO THE CLINIC GROUP.
39
MANAGEMENT OF CERVICAL INTRAEPITHELIAL NEOPLASIA . DR OMOLO THE CLINIC GROUP
-
Upload
stewart-young -
Category
Documents
-
view
229 -
download
0
Transcript of MANAGEMENT OF CERVICAL INTRAEPITHELIAL NEOPLASIA. DR OMOLO THE CLINIC GROUP.

MANAGEMENT OF CERVICAL INTRAEPITHELIAL NEOPLASIA
.
DR OMOLOTHE CLINIC GROUP

NCD Report May 2015
A total of 183 cancer related deaths occurred in Swaziland as reported by the national prevention and control of non-communicable diseases programme annual report 2014

I screened a total of 75 ladies who presented in my practice, the youngest being 20 years and oldest 76 years. 54 ladies had normal results and 21 abnormal results, thus 22.6% of ladies required additional evaluation.

The results were categorized as: 54 normal;1 ASCUS;1 AGCUS; 2 LSIL; 2 LSIL-HSIL;13 HSIL; 2 carcinoma

74 ladies accepted to be tested for HIV;52 ladies were HIV negative(69.3%);22 ladies tested HIV positive(29.3%) and 1 lady declined to be tested(0.01%)

Lesions in the background of HIV: 1 lady with normal findings declined screening; among 52 who were HIV negative 8(15.3%) had abnormal smear results; among 22 who were HIV positive 13 (59%) had abnormal results. Being HIV makes the lady 4 times likely to have abnormal CIN.

CIN
CIN ₌ Cervical intraepithelial neoplasia, is the term now used to encompass all epithelial abnormalities of the cervix. These abnormalities are confined to the epithelium and are regarded as preinvasive lesions.
In average cervical preinvasive lesions precedes cervical cancer by 15.6 years (range 3-20 years).CIN is asymptomatic.

Screening
Being asymptomatic, CIN are identified through screening. The standard screening test is cervical cytology. Eitheri) Papanicolaou (Pap) smear Ii) Liquid based cytology,(thin layer preparation of cervical specimen) is a modification of pap smear.Cervical cytology selects those women who should have further evaluation and ≈ 7-10% of women who are screened require additional evaluation.
Terminology for reporting cervical cytology is standardized by the Bathesda system.Lesions are broadly divided into two subgroups: 1)Mild atypical cellular changes in the lower third of the epithelium referred to as low-grade cervical intraepithelial neoplasia(CIN1= ASCUS, Atypical squamous cell cannot exclude high grade squamous intraepithelial lesion, LSIL)2)Moderate and severe atypical cellular changes confined to the basal two thirds and full thickness of the epithelium referred to as high-grade cervical intraepithelial neoplasia (CIN II–III/CIS)

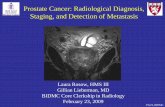
Diagrammatic illustration of CIN

Screening guidelines
a)With cytology (Pap smear or LBC) every 2 years between ages 21-29 years, then cytology every 3 years between ages 30-65 years provided that the last 3 reports are normal.
b) With cytology & HPV-DNA typing every 3 years after 30 years, discontinue between 65-70 years in negative screened women in the last 10 years.
c) More frequent screening is advised in high risk group e.g. those with HIV; those who are immunosuppressed-transplant patients or those on prolonged steroids and those who have been treated for CIN II, CIN III, or cervical cancer.

Role of human papillomavirus
Sexual activity has been consistently implicated as the dominant risk factor for occurrence of cervical cancer. These lesions are almost non-existent in women who have not had any sexual relationships.
And the major factor causing these lesions is the infection with the human papilloma virus .
HPVI association is so strong that most other behavioural, sexual and socioeconomic co-variables are all dependent upon HPV infection and do not hold up as independent risk factors.

12
Normal epithelium
Basement membrane
Basal (stem)cells
Parabasalcells
Squamous layer
Mature squamous
layer
Infected epithelium
Cervical canal
HPV infects basal layer of cervical epithelium
HPV lifecycle in the cervix is confined to the epithelium
Adapted from Frazer IH. Nat Rev Immunol 2004; 4:46–54.
Virus particles are assembled and virus released
Virus uses host cell to replicate viral DNA and express virally encoded proteins
Note that this diagram depicts infection of the squamous epithelium not columnar epithelium.

Sequelae of acute infection
Once the epithelium is infected. 3 clinical scenarios may result :1) Latent infection without any manifestations, what is seen in over
90% of infected women2) Active infection where HPV undergoes vegetative replication, but is
not integrated into the host cell genome (will results in low grade lesions)
3) Neoplastic transformation in which HPV integrates into the human genome (results in HSIL and cancer). 2 major factors i) Infection with high risk HPV subtypes(16,18,31,33,35,45,59) and ii) Persistence factors such as smoking, sexual exposure and immunosuppression as predisposing factors to neoplastic transformation.

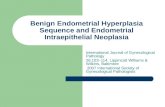
Natural history of CIN(cervical carcinogenesis)
REGRESS HSIL/CIS CA
ASCUS IN 24 MONTHS 68% 7.3% 0.25%
LOSIL IN 24 MONTHS 47% 21% 0.15%
HSIL IN 24 MONTHS 35% 1.44%
LOSIL IN 20 YEARS 60% 10% 1%
HSIL IN 20 YEARS 33% 12%

Burd EM. Clin Microbiol Rev 2003; 16:1–17; Solomon D, et al. JAMA 2002; 287:2114–2119.
Low-grade squamous intraepithelial lesion (ASCUS/LSIL)
High-grade squamous intraepithelial lesion (HSIL)
Invasivecarcinoma
Time YearsMonths
Normal epithelium
HPV infectionkoilocytosis
CIN1 CIN2 CIN3
Regression
* With increasing probability of viral DNA integration.CIN = cervical intraepithelial neoplasia; ASCUS = atypical squamous cells of undetermined significance.
Progression*
HPV cervical disease: cervical carcinogenesis (Progression & regression)

II Treatment
Given the natural history of CIN, the goal of treatment is to prevent possible progression to invasive cancer while avoiding overtreatment of lesions that are likely to regress

Diagnosis
Being asymptomatic, screening is our only option of making a diagnosis .Cytology(pap smear & LBC) (remains an art - as many as 30% of new cases of cervical cancer each year are the result of false-negative test results).To improve accuracy of screening ,it is best, where available to combine HPV DNA testing with cytology for ladies above 30 years

Colposcopy
As an adjunctive technique to cytologyColposcope is designed to study the genital epithelium. It allows the entire cervix to be carefully examined at low power, with emphasis on the details of the transformation zone. Findings sought for include:-Keratosis(represents HPV infection, chronic trauma or scarring)-Acetowhite (represent higher nuclear/cytoplasm ratio-more distinct in CIN)-Borders(sharper & smoother of Acetowhite lesions are seen in HSIL)-Surface contour(uneven contours seen with warts,cauliflower,nodular or ulcer with cancer)-Color-Lugol’s uptake(neoplastic cells lack glycogen hence do not turn brown)-Vascular pattern(neoplastic epithelium produces angiogenic factors VEGF which results in neovascularisation).-inflammation (when present make exam difficult and must be treated before colposcopy)

CIN1
Cytology• Mild dysplasia• Changes to shape and size of cells• Changes to size and appearance of cell
nuclei• Koilocytosis
Appearance on colposcopy• Acetowhite reaction
– More transient – Mild translucent acetowhite
• Margins– Feathered, flocculated and geographic– Indistinct– Irregular
• Surface contours flat• No abnormal vessels• Reduced iodine uptake, light yellow
Normal, healthy cervix1
1. Image used with permission from Professor Achim Schneider. 2. Image used with permission from Dr Alejandro Ortiz de la Peña.
Cervix with CIN1
Mild aceto-white epithelium2

CIN2
Cytology• Moderate dysplasia• More abnormal nuclei, especially
in immature cells
Appearance on colposcopy• Acetowhite reaction
– Dull, oyster-white colour• Surface contour
– Flat or raised • Margins
– Straight• Vascular pattern
– Mosaic – Punctation
• Iodine uptake– Reduced, bright yellow
Cervix with CIN2
Image used with permission from Professor Muhieddine Seoud.
Moderate aceto- white epithelium

CIN3
Cytology• Severe dysplasia• Severe nuclear abnormality in immature basal
cells• Keratinization or cornification may be present at
surface or in isolated cells inside epithelium
Appearance on colposcopy• Acetowhite reaction
– Dull, denser white, not shiny– Remains for longer time
• Surface contour– Flat or raised
• Margins– Sharp and distinct– Internal margins possibly present with LSIL
• Vascular pattern– Coarse punctation and or mosaic– Wide intercapillary distance
• Iodine uptake– Rejects iodine
Cervix with CIN3
Image used with permission from Dr Alejandro Ortiz de la Peña.
A dense opaque acetowhite area with coarse mosaics

Treatment overview techniques
• Treatment decisions are based upon diagnostic results from histologic examination, preferably colposcopically directed biopsies where available.

Low grade lesions(HPV &CIN 1)
These have a high spontaneous remission rate and that most lesions will regress within a 2-year follow-up period. Options for the management include i) Conservative treatment by ablation or ii) Close follow-up without treatment (observation, expectant management) by
surveillance Pap smears every 4–6 months or HPV testing at 12 months for 2 years then every 6 months if low-grade changes persist.
Women can return to regular screening only if consecutive normal Pap smear results are obtained. If the lesion progresses during the surveillance period it should be treated. Treatment is only recommended: • If CIN 1 persists for >24 months• For an occasional anxious patient who may elect to be treated to relieve her
anxiety.• In a patient at very high risk for loss to follow-up.

High grade lesions /(CIN 2, 3; CIS)
These patients require treatment. Ablative techniques are only appropriate when invasive cancer has been excluded .1. If the lesion is small, the entire lesion is well-visualized, and there is no endocervical disease, then cryotherapy can be used for the management of high-grade lesions. Cryotherapy is not recommended for large, complex high-grade lesions. 2.Large lesions are treated with:i) The LEEP procedure (widely available and easy). The main advantage of the LEEP is that there is a histologic specimen for evaluation. Two disadvantages for it’s use, include the removal of excessive amounts of tissue and the danger of overtreatment.ii) CO2 laser vaporization(if available) allows greater precision in the destruction of abnormal tissues. It’s main advantage is in the treatment of lesions wide on the transformation zone and in situations in which the treatment of cervical dysplasia is concurrent with laser treatment of dysplastic lesions of the vagina and vulva.

High grade lesions /(CIN 2, 3; CIS)
Excisional therapy(cervical conization): is recommended for women with cytological findings potentially associated with high-grade lesions. These allow further histologic study. Cervical conization (also known as cone biopsy) refers to the excision of a cone shaped portion of the cervix surrounding the endocervical canal and including the entire transformation zone.Techniques for cervical conization include cold-knife conization, laser conization, and the use of the LEEP as cone. In general, either ablative or excisional treatments of CIN are successful.

Hysterectomy
Hysterectomy is not the treatment of choice But valid indications include:1. When conization specimen margins are positive for HSIL,(completed childbearing and expected poor compliance with follow-up). Though, the treatment of choice is close clinical follow-up or, in select cases, reexcision to exclude an invasive cancer instead of hysterectomy. Hysterectomy should generally be reserved for those in whom a repeat excisional procedure is not technically feasible or where the cervix and vagina are scarred in a way that severely compromises the reliability of cervical cytology and close clinical follow-up.2. Presence of coexistent gynaecologic conditions requiring hysterectomy such as symptomatic uterine fibroids3. Patient request and persistent or recurrent HSIL.

III Preinvasive cervical lesions in HIV -setting• In 1993, the CDC designated high grade lesions as conditions defining a
stage of early symptomatic HIV infection and invasive cervical carcinoma as an AIDS defining condition.
• The incidence of CIN is 4-5 times higher among HIV-infected compared to HIV-negative women. And the risk of cervical cancer among HIV-infected women is 5-7 fold the risk in the HIV-negative women.
• HIV infected women especially those with low CD4 counts have the highest prevalence of HPV infection,habor high risk HPV types and are at high risk for persistence of cervical HPV infection

How then do one manage CIN in these setting:
The appropriate management of CIN, timing and method of follow up is still unfortunately largely unknown. Guiding data is not available and therefore close follow up is essential.
This is study item for one to look into in order to design treatment of CIN for this category.

Low grade lesions
Understanding the natural history of such lesions in HIV infected women is necessary in order to determine the treatment approach. No satisfactory data exist and therefore same recommendation of expectant management of women with biopsy confirmed CIN1 and satisfactory colposcopy. The use of HAART has been associated with increased rates of regression and decreased rates of recurrence in HIV infected women. Based on this, HIV infected women using HAART with low viral loads and stable CD4 levels may be managed similar to non-HIV infected women.

High grade lesions
Excision and ablation are both accepted treatment modalities for HIV infected women with satisfactory colposcopic examinations.
If colposcopy is not available or not satisfactory, then ablative treatment is unacceptable because histopathological examination of the nonvisualized tissue is required to exclude the presence of occult cancer. A diagnostic and therapeutic excisional procedure is performed in these cases. Excision is also recommended for patients with recurrent disease after ablation.
The success rate of these modalities in HIV-negative women is over 90% but is lower in HIV-infected women. Persistence and recurrent disease is also more common. One factor that contributes to the poorer treatment outcome is incomplete excision or ablation of CIN. The margin status of the tissue specimens is critical.

Medical therapy
Because of the results of standard excisional therapy are not better as compared to those in HIV-negative women, use of primary or adjuvant medical therapy to improve treatment outcomes has been investigated.• Topical –fluorouracil (5-FU) is an effective prophylactic agent for
immunosuppressed women with CIN. 6 months of topical application of 2g of 5% cream biweekly is recommended as adjunctive therapy to excision/ ablation procedures for high grade lesions
• HAART- is associated with regression of CIN. It lends support to the recommendation that CIN is a relative indication for HAART.

Follow-up
HIV-infected women with CIN should be advised that recurrence is more frequent than in the general population.
Cancer can also develop rapidly in HIV infected women (3.2 vs. 15.7 years). Therefore, these women require close monitoring after treatment. Hysterectomy is an option for recurrent CIN in women not desirous of fertility.
The recommendation is monitor with both cervical cytology, colposcopy, with liberal use of biopsy, at least 3 month intervals for an indefinite period of time.

Surveillance
Surveillance after treatment should be designed to identify women with treatment failures as well as those in whom recurrent CIN develops. 1. Persistence of a lesion (incomplete treatment or recurrent CIN)seen in 1–
20% of cases). 2. Factors associated with persistent or recurrent disease include age older
than 40 years, glandular involvement, large lesions, and positive treatment margins, HIV coinfection.
3. Serial repeat Pap smears performed at 3–6month intervals for several years will identify persistent or recurrent CIN.
The use of HPV testing is particularly attractive in post treatment follow up. The majority of women with recurrent CIN have persistent positive high-risk HPV tests while recurrence is rare in the face of negative follow-up HPV testing.

Surveillance
When several consecutive smears are within normal limits and/or a repeat high-risk HPV test is negative for persistent infection, the patient can return to regular screening.If recurrent dysplasia is noted on follow-up Pap, the patient should undergo repeat colposcopy. Recurrent dysplasia documented by directed biopsy should be treated with • cold-knife conization or LEEP conization. • In cases in which invasive carcinoma has been excluded and fertility is not
desired, hysterectomy can be considered. Care should be taken to evaluate for vaginal involvement in these recurrent cases, because failure to treat concomitant vaginal dysplasia may result in persistently abnormal smears.

Treatment complications
Cryotherapy, CO2 laser therapy, and LEEP excision all have excellent success rates, each is associated with some risk of complication.Cryotherapy has the lowest rates of bleeding and infection but has higher failure rates when treating large lesionsBoth laser and LEEP may be associated with bleeding, but complication rates are low. Post treatment bleeding occurs in 2–7% of LEEP procedures, with bleeding significant enough to result in hospitalization in only 1–2%.Long-term morbidity of these procedures is minimal.i) Scarring severe enough to result in unsatisfactory colposcopic examination occurs in 1.3% to 9% of patients undergoing LEEP and 1.3–3.8% have cervical stenosis after the procedure. The risk of cervical stenosis and its resulting hydro-hematometra is much higher in women who have a LEEP that extends 1.5 cm or more into the endocervical canal and in women who have had previous ablative therapy.

Treatment complications
Ablative techniques such as cryotherapy or CO2 laser for treatment of dysplasia have less impact on future fertility than surgical conization. Several studies have addressed the impact of LEEP procedures on subsequent pregnancy outcome with favourable results. • Two case–control studies showed that compared with controls, patients
with a history of a cervical LEEP procedure had no higher rate of prematurity or cesarean delivery.
Impact on fertility is more difficult to obtain, but no clear association between decreased fertility and LEEP procedures has been demonstrated. In general, excision depth should be limited to less than 7–10 mm in patients desiring to preserve fertility, and repeat excisions should be performed with caution, and for good reason, in young patients.

Our duty/ role
Sex the all important risk factor is rampant in the human race. And CIN exists, more so amongst the HIV positive population. CIN is asymptomatic and therefore we should look for it when an opportunity presents itself, remember the screening guidelines and enquire with your client and recommend screening if it is due.The burden for us in the fight against cervical cancer mainly is in prevention. We are completely helpless when it comes to treating cervical cancer. We should advocate for • screening as a secondary preventive method and • HPV vaccination to prevent HPVI and with it, the development of CIN and • attempt to instill good morals amongst the at risk groups.Vaccination have almost eradicated over 27 infections.I leave you with the disease human race have benefited from vaccines.

To date, vaccines have been used very successfully to prevent 27 major diseases
Anthrax
Cholera
Diphtheria
Haemophilus influenzae type b
Hepatitis A
Hepatitis B
Influenza
Japanese encephalitis
Measles
Meningococcal
Mumps
Pertussis
Pneumococcal
Polio
Rabies
Rubella
Smallpox and vaccinia
Tetanus
Tick-borne encephalitis
Tuberculosis
Typhoid Varicella
Yellow fever
Human papillomavirus
Benefits of vaccination

END
THANK YOU.

![(Endometrial Intraepithelial Neoplasia): Improved Criteria ... · Endometrial intraepithelial neoplasia [EIN] EIN Reproducibility UsubutumA et al Modern Pathol25: 877-884, 2012. Questionaire,](https://static.fdocuments.net/doc/165x107/6053ec04465f250d537d95f4/endometrial-intraepithelial-neoplasia-improved-criteria-endometrial-intraepithelial.jpg)