Management Conference Young woman with several episodes of hematemesis Raika Jamali MD Digestive...
83
Management Conference Young woman with several episodes of hematemesis Raika Jamali MD Digestive Disease Research Center Tehran University of Medical Sciences
-
Upload
allen-charles -
Category
Documents
-
view
213 -
download
0
Transcript of Management Conference Young woman with several episodes of hematemesis Raika Jamali MD Digestive...

Management Conference
Young woman with several episodes of hematemesis
Raika Jamali MDDigestive Disease Research Center
Tehran University of Medical Sciences

• 19 year old girl with hematemesis admitted for evaluation of UGI bleeding.
• There were Hx of hematemesis 2 months ago and also 1 year ago with several episodes in early childhood( 2 years old).
• There was no history of epistaxies, hematuria and siezure.

• The endoscopic diagnosis was vascular malformation( hemangioma?) in distal esophagus .
• Although the recent endoscopy in our hospital showed 2 rows of G1 and 2 rows of G2 distal esophageal varices and also gastric fundal varices with snake skin appearance.

Physical examination• There was orthostatic hypotension and
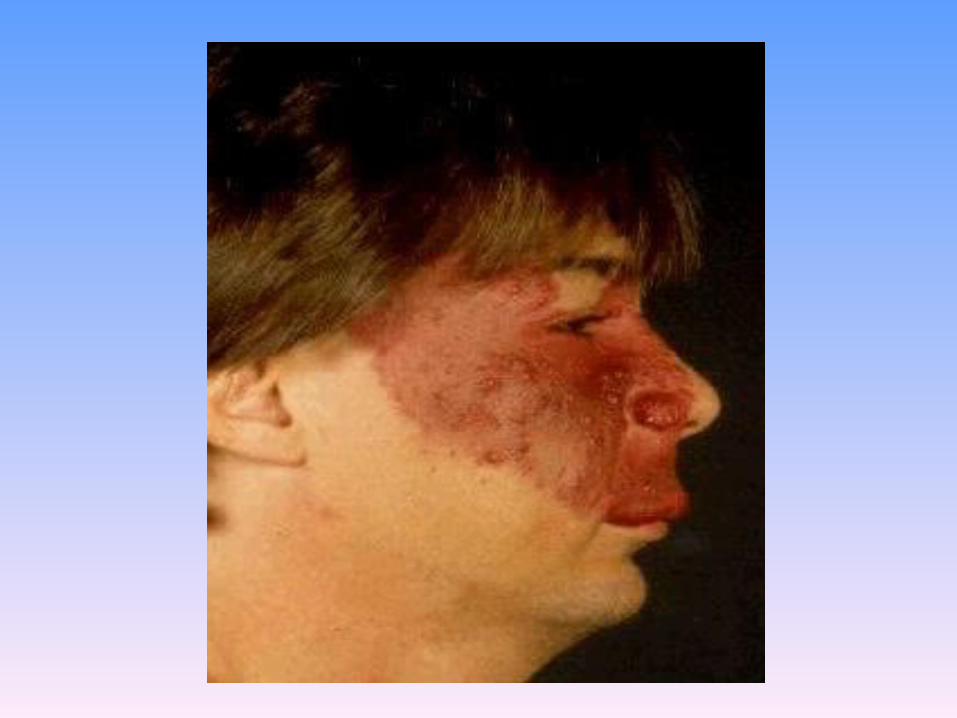
tachycardia on admission.• There were cutaneus hemangiomas on right
side of the face and also on the dorsum of the right leg & thigh.
• The conjunctiva was anemic.• Heart & lung were NL.• The abdomen was normal. No collateral in
abdominal inspection. • No hepatosplenomegaly. No shifting dullness.

LAB DATA• WBC=8700
• DIFF=NL
• RBC=3640000
• Hb=9.7
• MCV=78
• MCHC=26
• PLT=293000

• AST=12 BUN=20
• ALT=14 Cr=0.7
• ALP=130 Na=141
• BILI TOTAL=3.2 K=4
• BILI DIRECT=0.6 FBS=90
• PT=12.6 (INR=1.1)
• PTT=26
• SERUM ALBUMIN=4.6
• SERUM PROTEIN=5.8
• SERUM IRON=58
• TIBC=380
• HBs Ag=negative
• HBs Ab=negative
• HBc Ag=negative
• HCV Ab=negative

ABDOMINAL SONOGRAPHY
• Liver had normal echotexture and span.
• Portal vein=9 mm
• Spleen, biliary tree, gall bladder were NL.
• No ascitis.

COLER DOPLER SONOGRAPHY
• Hepatic veins( right, left and middle) were patent with normal flow.
• Portal and splenic veins were patient with hepatopethal flow.
• There was no sign of collateral formation.

Abdominal CT Angiography
• Liver, spleen, stomach, biliary system, and gall bladder were NL.
• No ascitis
• Hepatic veins, portal and splenic veins were NL.
• There was no collateral formation.
• Arterial system were NL.

Endosonography
• There was varices in distal Esophagus, stomach & duodenum were NL.

Colonoscopy
• Anus, rectum, sigmoid, descending, transverse ,ascending and cecum were NL.

Dermatology consult• The patient is a case of “ Nevic Port
Wine syndrome, segmental sub type”.
• This syndrome is associated with multiple nevics as hemangiomas & varices in visceral organs like, meningium, eye and GI tract.

Ophthalmologic consult
• The anterior chamber, viterous and retina was normal.
• There was no hemangioma.
Neurologic consult The neurologic exam was normal .

UGI Endoscopy

Date:1385/6/11 • Esophagus:
Crico-pharyngeus , upper third and middle third were normal. 2 rows of Grade 1 and 2 rows of Grade 2 varices with red sign were found in lower third. ____________________________Stomach:Antrum and pre-pyloric area were normal. Snake skin appearance was seen in fundus and body. Stomach varices were observed in fundus and without stigmata of bleeding. ____________________________Duodenum:Bulb and 2nd part were normal.
• Recommendation:E.V.L.
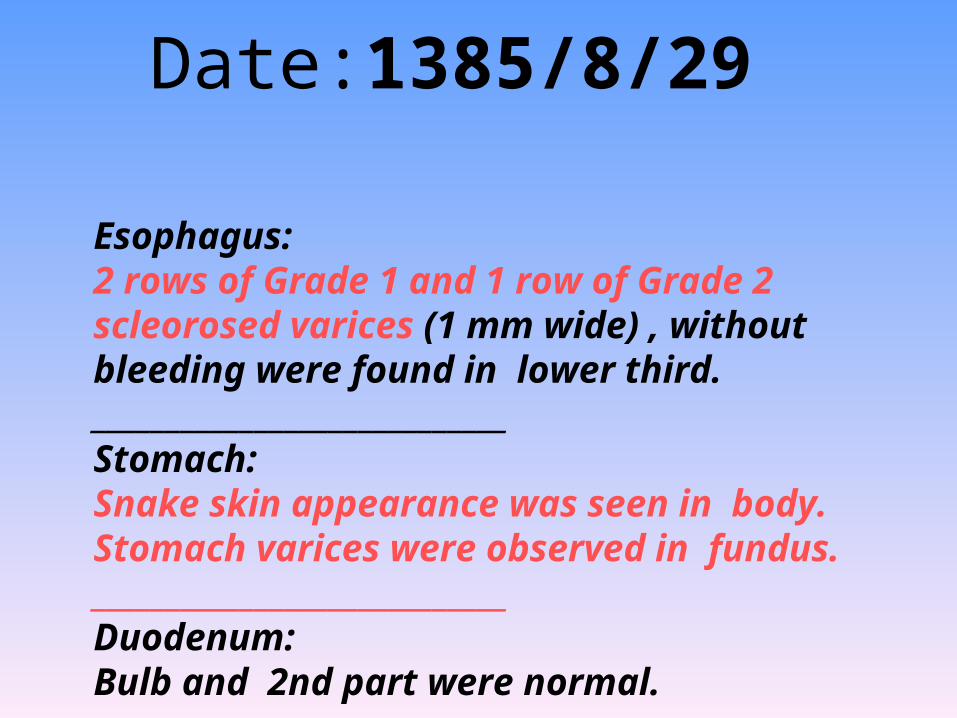
Date:1385/8/29
Esophagus:2 rows of Grade 1 and 1 row of Grade 2 scleorosed varices (1 mm wide) , without bleeding were found in lower third. ____________________________Stomach:Snake skin appearance was seen in body. Stomach varices were observed in fundus. ____________________________Duodenum:Bulb and 2nd part were normal.

Port wine stain or nevus flammeus
• The port wine stain is a cavernous hemangioma consisting of dilated blood vessels.
• It is associated with the Sturge-Weber syndrome.
• This lesion is congenital and usually covers the eye and nearby facial skin, typically in the distribution of a branch of the trigeminal nerve .

• It does not blanch with pressure.
• It may be associated with ocular and leptomeningeal vascular hamartomas as well as glaucoma and retinal detachment.
• Argon laser therapy has been somewhat successful at removing these lesions .


Sturge-Weber syndrome• rare congenital vascular disorder
• affects capillary size blood vessels.
• It is not a heritable disorder.
• recurrence is unlikely.
• somatic mutations in fetal ectodermal tissues that cause inappropriate control or maturation of capillary blood vessel formation.

CLINICAL FEATURES
• characterized by a facial angioma (port-wine stain)
• leptomeningeal angioma .
• Ocular
• and neurologic abnormalities.

Cutaneous manifestations
• port-wine stain is the most common type of vascular malformation, occurring in 0.3 percent of newborn infants. However, only a small proportion of children with port-wine stains have SWS.
• In SWS, the port-wine stain typically is present on the forehead and upper eyelid, primarily in the distribution of the first or second division of the trigeminal nerve .

• The distribution of the cutaneous angioma influences the risk of an associated leptomeningeal angioma.
• Leptomeningeal angioma occurs in approximately 90 percent of cases when the port-wine stain involves both the upper and lower eyelids, compared to 10 percent when only one eyelid is affected.

• The skin lesion usually is obvious at birth. However, its appearance changes with age and its size increases as the patient grows.
• In the newborn, the lesion is flat and usually light pink in color.
• It typically darkens with age to a deep red, port-wine appearance, and vascular ectasias develop .

• The vascular ectasias produce nodularity and superficial blebbing, which lead to overgrowth of the underlying soft tissues and sometimes the bone.

Vascular lesions
and
congenital nevi

VASCULAR LESIONS
• There are two general categories of vascular lesions:
• 1) benign vascular neoplasms
2)vascular malformations.
• Benign vascular neoplasms, such as hemangiomas, are characterized by proliferation of endothelial cells, while vascular malformations have normal endothelial turnover.

Hemangiomas
• Hemangiomas, which are also called infantile hemangiomas are the most common benign tumors of infancy.
• They occur in up to 10 percent of infants, generally within the first few weeks of life.

Vascular malformations
• Vascular malformations are anomalies of morphogenesis and are always congenital.
• Unlike neoplasms, endothelial turnover is normal.
• They are categorized as capillary, venous, arterial, lymphatic, or combined groups .
• or as low-flow (capillary, venous, lymphatic, or combination) and high-flow (arterial, arteriovenous) lesions.

• Vascular malformations are always present at birth but often are clinically subtle.
• They become more apparent over time as they slowly expand in proportion to the infant's overall growth.
• There is progressive ectasia secondary to changes in blood or lymphatic flow, pressure associated with trauma, or hormonal changes such as at puberty.

Port wine stains
• Port wine stains (PWS), which are capillary malformations,
• are uncommon (0.1 to 0.3 percent of newborns)
• low flow malformations that can occur anywhere on the body

• The lesions are pink or red patches that are unilateral in 85 percent of cases .
• They enlarge proportionally to the child's growth and persist in approximately 40 to 60 percent of affected patients.
• While most PWS are isolated anomalies, they may be associated with developmental defects.

Sturge-Weber syndrome
• is a rare congenital but not hereditary vascular disorder characterized by a facial capillary malformation and an associated leptomeningeal vascular malformation. These malformations may be associated with specific ocular (predominantly glaucoma) and neurologic abnormalities, including seizures, hemiparesis, mental retardation, and behavior problems.

Klippel-Trenaunay syndrome
• is an extensive PWS with underlying venous and/or lymphatic malformations involving an extremity.
• Increased angiogenesis is a mechanism for these lesions, and mutations in the gene for an angiogenic factor (VG5Q) that result in increased transcription or activity have been identified in some patients with this disorder .
• VG5Q is expressed in blood vessels, is secreted during vessel formation, and promotes endothelial cell proliferation.

Hepatic vascular anomalies in infancy: a
twenty-seven-year experience.
• SO - J Pediatr 1996 Sep;129(3):346-54.

• Infantile hemangioma and arteriovenous malformation (AVM) of the liver have a similar presentation but a different natural history.
• Pharmacologic treatment is used for symptomatic multiple liver hemangiomas.
• Embolization allows interim control of heart failure.
• A decreased mortality rate after interferon alfa-2a therapy is encouraging.
• We recommend combined embolization and surgical resection for hepatic AVM and for solitary symptomatic hemangioma, if drug therapy fails.

An unusual cause of upper gastrointestinal
haemorrhage
Gut 2005;54:343
Clinical presentation• A 59 year old man presented with melena.
• He had a history of iron deficiency anaemia for the past five years that required oral iron supplements intermittently.
• Previous oesophagogastroduodenoscopy and colonoscopy were negative.
• Physical examination disclosed bluish vascular lesions on the upper trunk and undersurface of the tongue .
• The patient underwent capsule endoscopy which showed a single active bleeding vascular lesion of the small bowel .
• The patient then proceeded to a segmental resection of the involved gut.
• Histological examination of the removed lesion disclosed cavernous haemangiomas compatible with blue rubber bleb nevus syndrome (BBRBNS).

BRBNS• is characterised by haemangiomas in
the skin, gastrointestinal tract, and other viscera.
• The most common mode of presentation of BRBNS is gastrointestinal bleeding.

• Lesions are most commonly found in the small intestine and distal large bowel and are typically discrete mucosal nodules with a central bluish nipple, although they may be flat, macular, or polypoid.
• BRBNS may affect several successive generations by autosomal dominant inheritance caused by a mutation on chromosome 9p.

Association of solitary, segmental hemangiomas of
the skin with visceral hemangiomatosis
• Arch Dermatol. 2004 May;140(5):591-6.

• Multiple hemangiomas of the skin have traditionally been recognized as a clue to potential visceral hemangiomas.
• Recently, hemangiomas have been recognized to have subcategories, localized and segmental, which correlate with risk of complications.

• segmental hemangiomas of the skin have a higher risk of being life- or function-threatening and having associated structural anomalies such as those that occur in PHACE (posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities) syndrome .

The most common site of internal organ involvement was:
• liver (20 cases [43%]),
• gastrointestinal tract (16 [34%]),
• brain (16 [34%]),
• mediastinum (9 [19%]),
• lung (7 [15%]).
• pancreas, spleen, bones, or kidneys(<6%).

• Death during infancy, most commonly because of gastrointestinal involvement or congestive heart failure secondary to liver involvement.

ESOPHAGEAL VARICEAL BLEEDING CAUSED BY
HYPOPLASIA OF THE PORTAL VEIN IN A PATIENT WITH THE
KLIPPEL-TRENAUNAY SYNDROME
• American Journal of GastroenterologyVolume 93 Issue 2 Page 275 - February 1998

• The case of a patient affected by Klippel-Trenaunay syndrome presenting with esophageal variceal bleeding caused by hypoplasia of the vena porta is reported.
• Hemostasis was achieved by performing a proximal spleno-renal shunt.
• We suggest the likely association of this mesodermal development abnormality and vascular disorders of the portal vein.

INTRODUCTION
• Klippel-Trenaunay syndrome (KTS) is a rare congenital disorder characterized by cutaneous hemangiomata, venous abnormalities, and bony and soft tissue hypertrophy .
• Malformations of deep veins, including hypoplasia of the vena cava, have been reported .
• Gastrointestinal hemorrhage, basically from colonic vascular malformations, has been described in a few patients with KTS.
• However, no cases of upper gastrointestinal bleeding have been reported.

CASE REPORT
• A 20-year-old Caucasian man was admitted to our unit for two episodes of hematemesis associated with tachycardia (108 bpm) and systemic hypotension (80/50 mm Hg).
• At the age of 6 years old, he was diagnosed with having KTS because of the presence of severe diffuse varicose veins in the right thigh and multiple perianal and genital vascular ectasia

• his physical examination revealed generalized pallor.
• Neither hepatosplenomegaly nor cutaneous stigmata of chronic liver disease were observed.
• Emergency endoscopic examination revealed the presence of three esophageal varices with red signs and active bleeding in one of them.

• Sonography showed a normal liver and mild splenomegaly, with a patent portal vein with a diameter of 10 mm with hepatopetal flow.
• Doppler register of the portal vein was reduced without echo-graphic signs of thrombosis.
• Angiographic examination revealed a marked hypoplasia of the portal vein.

• Hemodynamic studies showed a normal wedge hepatic venous pressure.
• Diagnosis of prehepatic portal hypertension caused by portal vein hypoplasia in a patient with KTS was made.
• The patient was discharged asymptomatically under treatment with propranolol.

• One month later, the patient was readmitted because of hematemesis and melena.
• On admission, there were no signs of hypovolemia.
• A new endoscopic examination showed a large esophageal varix with a fibrin clot as a unique source of bleeding.
• Hemostasis was achieved in 24 h with somatostatin infusion.
• Then, a proximal spleno-renal shunt was performed

Vascular lesions of the stomach
• Journal of Gastroenterology and HepatologyVolume 17 Issue 5 Page 621 - May 2002

angiodysplasia
&
telangiectasia

Angiodysplasia
isolated mucosal vascular ectasias
• low-grade obstruction of submucosal veins followed by proliferation of dilated and deformed superficial vessels and the development of small arteriovenous fistulas.

Telangiectasia
• lesions that occur in more generalized disorders such as hereditary hemorrhagic telangiectasia (Osler–Weber–Rendu disease), vasculitis and scleroderma.

Other vascular lesions
• gastric antral vascular ectasia, hemangiomas,
• angiosarcomas,
• Dieulafoy lesions
• multiple hemangioma syndromes such as the blue rubber bleb nevus syndrome.

• Angiodysplastic lesions are found in the stomach or duodenum in 1–2% of upper gastrointestinal endoscopies.
• account for upper gastrointestinal bleeding in 1–4% of patients.
• lesions are:
• flat or slightly raised,
• bright red,
• 2–10 mm
• 'fernlike' margins.

Angiodysplasia of stomach

• the red area appears to be composed of small blood vessels while the lesion is surrounded by a pale area or halo.

gastric telangiectasia
Endoscopic treatment
• neodynium YAG lasers,
• argon plasma coagulation,
• heater probes,
• band ligation
• injection sclerotherapy.

Cavernous transformation of the portal vein associated to multiorgan developmental
abnormalities
• Volume 24 Issue 1 Page 80 - February 2004

• We describe here a case of association of prehepatic portal hypertension, due to cavernous transformation of the portal vein, with right pulmonary hypoplasia, cardiac dextroposition, and right renal ectopia.

• In the pediatric age group portal vein thrombosis is a common cause of prehepatic portal hypertension, and is idiopathic in more than half of the cases.
• When present in children, cavernous transformation of the portal vein is frequently associated to congenital anomalies.

• Among these abnormalities the most frequent are atrial septal defects or malformations of the biliary tract or of the inferior vena cava.
•

Gastric hemangioma: An unusual cause of upper gastrointestinal bleed
• Indian journal of gastroenterology• Year : 2004 | Volume : 23 | Issue : 3 | Page : 113-114

• We report a 36-year-old lady who presented with hematemesis.
• Emergency endoscopy showed a polypoidal lesion in the gastric fundus that appeared like a varix.
• Since histacryl glue was not available and an attempt at using heater probe proved unsuccessful, balloon tamponade using a Linton tube was resorted to plan angiography.

Celiac angiogram confirmed this to be a hemangioma located in the fundus.
• This was managed by arterial embolization.

Blue Rubber Bleb Nevus Syndrome: A Clinical
Spectrum with Correlation Between Cutaneous and
Gastrointestinal Manifestations
• Journal of Gastroenterology and HepatologyVolume 18 Issue 8 Page 1000 - August 2003

• Blue rubber bleb nevus syndrome characterized by distinctive cutaneous and gastrointestinal cavernous hemangiomas.
• Patients usually present with iron deficiency anemia from occult gastrointestinal bleeding.

There are three important conclusions that can be drawn
• First, there appeared to be a correlation between the number of cutaneous hemangiomas and visceral hemangiomas.

• Second, the outcome is poorer for those with extensive involvement of the viscera, with more extensive resection needed and a high re-operation rate for recurrent bleeding.
• Finally, for patients with limited involvement of the gastrointestinal tract, definitive surgery can potentially provide long-term remission of gastrointestinal bleeding.