
Managed Advocacy in Action
72
ABC for Health, Inc. Managed Advocacy in Action The Families MAP Blueprint
Transcript of Managed Advocacy in Action
ABC for Health, Inc.
ManagedAdvocacy inActionThe Families MAP Blueprint

ManagedAdvocacy in
Action
The Families MAP Blueprint
This project was supported through a grant from the Health Resources andServices Administration, U.S. Department of Health and Human Services.
ABC for Health, Inc.
Copyright © 2002 by ABC for Health, Inc. All rights are reserved. No part of this publication may be reproduced, in whole orin part, without the permission of ABC for Health, Inc., 1-608-261-6939.
ABC fABC fABC fABC fABC for Hor Hor Hor Hor Health,ealth,ealth,ealth,ealth, Inc Inc Inc Inc Inc.....152 W Johnson St, Ste 206Madison, WI 537031-608-261-69391-800-585-4222www.abcforhealth.org
This report was funded with a grant from the Maternal and Child Health Bureau, Health Resources and ServicesAdministration. It does not necessarily reflect the views of the Bureau, HRSA, or Department of Health andHuman Services.
About ABC for HealthABC (Advocacy and Benefits Counseling) for Health, Inc., is a nonprofit public interest law firm that provides free health benefitscounseling for families who have children with special health needs and legal services for low-income Wisconsin families havingproblems paying for health care. ABC gives information on available health care resources, helps families get benefits from privateinsurance and public financing programs, and helps resolve disputes with insurance companies, health care providers, andgovernment agencies.
Contents
Preface 5
Chapter OneBackground 7
Chapter Two
Managed Advocacy Project 13
Chapter Three
A Blueprint for Helping Familieswith Health Care Coverage 15
Chapter Four
Identifying Barriers in ManagedCare 19
Chapter Five
Families MAP and Health BenefitsCounseling: The Blueprint in Action 25
Chapter Six
Working with HealthWatchCommittees 35
Chapter Seven
Conclusion 45
Appendices
A: Wisconsin Services and Programs 47B: Intake Form 49

4 • Contents MANAGED ADVOCACY IN ACTION
C: Health Care Financing Resources 51D: HealthWatch Mission Statement 59E: Prior Authorization Insert 61F: HealthWatch Digest 63G: Medicaid/HMO Contract 65
Preface
Families Managed AdvocacyProject
Negotiating the complex system of health care cov-erage in this country is truly a bewildering task. Sadly,cost containment measures like prior authorizations,gatekeeper physicians and restricted networks posegreat challenges to obtaining needed care for chil-dren with special health care needs. And it is notjust HMOs that are restricting access to health carecoverage. Today, most care is delivered by managedcare plans that dominate the health insurance land-scape. As a result, new rules and new proceduresmay needlessly compound the stress and frustra-tion of patients and caregivers. Many families areconfused by the cost containment features of man-aged care and the payment systems that seem con-trary to the best interests of medically involvedchildren.
The Families Managed Advocacy Project (Fami-lies MAP) was one of thirteen projects funded na-tionally by the Maternal and Child Health Bureau toexamine and detail the impact of managed care ser-vices on children with special health needs (CSHN)and develop strategies to improve family satisfac-tion and involvement in the care received. In thisproject, partner agencies located in three differentparts of Wisconsin—Chippewa, Dane and Milwau-kee Counties—worked together to identify and com-pare differences in the barriers CSHN face inmanaged care. Strategies were developed for over-coming these coverage and access barriers throughpartnerships with families, medical providers, policymakers and representatives from managed care or-ganizations.
While many challenges remain in the processof developing a coordinated advocacy system forCSHN, Families MAP is a proven model that hasprovided parents with education, advocacy, support-ive services and, most importantly, a voice in policydevelopment that both helps managed care organi-zations to better serve children with special healthneeds and also promote the confidence of familiesthat their children are getting needed and appropri-ate care.
Families MAP agencies
As the lead agency for this project, and the host ofthe Dane County pilot site. ABC for Health is a non-profit public interest law firm based in Madison, Wis-consin, which is dedicated to ensuring health carecoverage for children and families, particularly chil-dren with special health needs. Our partners includedCommunity Advocates, a grass roots advocacy or-ganization working in urban Milwaukee on healthcare issues, and the Chippewa County Departmentof Public Health, the home of one of five RegionalCSHCN Centers in located in northern Wisconsin.All organizations in the project share a mission ofproviding information, advocacy tools and supportto CSHN. As such, our working relationship was en-riched by a common vision of a better system to servethe needs of children and families.
Because of the diversity of our communities andneeds, our goals were pursued, not in lockstep, butrather by following different pathways guided by com-munity concerns and priorities. Consequently, we

6 • Preface MANAGED ADVOCACY IN ACTION
believe that the Families MAP model can be adaptedand fine tuned to serve a variety of communitiesacross this country.
Using this guide
Managed Advocacy in Action reports on the devel-opment and operation of our Families MAP project,and also provides a flexible blueprint for the devel-opment and growth of managed advocacy programsin other communities. This report gives a brief back-ground on the families, programs and resourcesaround which Families MAP was developed, followedby chapters describing the health benefits counsel-ing model that provides the core philosophy behindthe client and committee work making up this project.Much of our work was guided by the critical involve-ment of parent advocates working with the projects.Input from families began with identification of sig-nificant care and coverage barriers. The strategiesand action steps developed to address these barri-ers are described in subsequent chapters.
This project was informed by nearly fifteen yearsof experience with health benefits counseling andworking with families that have children with specialhealth care needs. This managed advocacy modelalso relies heavily on the elements of the MedicalHome model (as defined by the American Associa-tion of Pediatrics) and the Maternal and ChildHealth’s Achieving and Measuring Success: A Na-tional Agenda for Children and Youth with SpecialHealth Care Needs and its objectives for ongoingand comprehensive health care for CSHN.
Is the Families MAP program appropriate foryour community? Certainly a better-coordinated ad-vocacy infrastructure and supportive services forparents is needed in Wisconsin. Families MAP pro-vides a framework for helping to build capacity withincommunities, to identify key stakeholders and to pro-vide a forum for issue identification and strategydevelopment to resolve barriers encountered byfamilies. And most importantly, a managed advocacyprogram can help us achieve our vision of a betterhealth care system that supports partnerships, ad-vocacy and a medical home for children with specialhealth care needs.
Background
Chapter One
The Families Managed Advocacy Project (FamiliesMAP), which involves health benefits counseling,coalition building, community education, and policyreform both inside and outside of managed care or-ganizations, is designed to enable families to accessthe most reliable and comprehensive health care fortheir children with special health needs.
These children with special health care needs(CSHCN) range in age from birth to 21 years of ageand have a long-term, chronic physical, developmen-tal, behavioral or emotional illness or condition. Theirillnesses or conditions:
� are severe enough to restrict growth, de-velopment or ability to engage in usual ac-tivities;
� have been or are likely to be present or per-sist for 12 months to lifelong; and
� are of sufficient complexity to require spe-cialized health care, psychological or edu-cational services of a type or amountbeyond that required generally by children.
Examples of their illnesses or conditions includecerebral palsy, leukemia, diabetes, autism, attention-deficit hyperactivity disorder and severe asthma.
Based on the above definition used by the Wis-consin Children with Special Health Care Needs Pro-gram, it is estimated that about fifteen to eighteenpercent, or about 274,000, Wisconsin children havespecial health care needs.
Their needs are as broad as their numbers. Un-like adults, children are susceptible to a multitude ofrare childhood disorders and a smaller set of com-mon ones—there are over two hundred chronic con-
ditions that are specific to children. Each of theseconditions brings with it a special set of care require-ments and family needs that require a unique re-sponse from the medical caregivers.
All children are dependent on adults for protec-tion, guidance and care. Children with special healthcare needs are no different except that the level ofthose needs are complex and require far greater timeand attention from parents and the rest of the family.The child with special health care needs often re-quires expansive medical services that cross the linebetween medical and home care including: primarycare, specialty treatment services, mental healthservices, prescription drugs, durable medical prod-ucts, nutritional services, community-based services,home nursing services and specialized day care.Clearly, the needs of children with special health careneeds are complex and multifaceted, necessitatingcomprehensive and coordinated health care ser-vices.
Family factors
There is no doubt that there are many challenges inraising a child with special health needs. From theday of birth or the onset of symptoms, the family hasto rely constantly on medical professionals and sup-port personnel to deliver the care their child needs.Like it or not, the family network must be expandedto include skilled and reliable caregivers, knowledge-able case managers, medical and educational per-sonnel. These individuals need to have direct access

8 • Background MANAGED ADVOCACY IN ACTION
to the child and, often, the home of the family. Whilemost families welcome supportive services, familyand individual privacy is frequently compromised.
Having a child with special health needs bringsmany other unique challenges to a family. A child’ssiblings might feel frustrated and left out, often long-ing for the attention that a child with special needsdemands. Stress in a household can increase tre-mendously, buoyed by the extra work, extra finan-cial requirements and extra emotional attention achild with special needs requires. In an ideal world,a child’s medical professionals and health care in-surance should support the family and their needs,not become an additional stressor in their lives. Theunfortunate reality is that frequently families need tobattle to get what their children need.
Additionally, Wisconsin’s geographic character-istics impact the health care and supportive servicesthat children with special needs might receive. Thosewho live in rural areas often have to drive long dis-tances to an appropriate primary care provider andeven longer distances for visits to specialists. Thera-peutic interventions might not be available to themat all, or in a reduced capacity, depending on skilland location of needed therapists. Those who live indensely populated urban areas, might be physicallyclose to appropriate providers, but might not havethe resources to access those providers. Particularlyfor families in poverty, lack of transportation options,time availability, lack of child care options, and thesheer number of medical appointments can be over-whelming. For these families, the inclusion of a medi-cal case manager, as in the medical home model,can be a virtual lifesaver for many families manag-ing their child’s health care.
What coverage programs areWisconsin families using?
Most CSHCN in Wisconsin are insured. Accordingto the Maternal and Child Health Title V 2002 BlockGrant Application, 77.9 percent of families with chil-dren with special health care needs surveyed indi-
cated that they had health insurance. Of that group,44 percent of families identified Medicaid or Bad-gerCare as their primary source of health insurance.Just three percent of families receiving care coordi-nation reported no insurance, but there is anothernineteen percent for who did not identify any primaryinsurance.
One of the most frustrating challenges for fami-lies was the overwhelming complexity of the cover-age choices and of the coverage options within careplans. In addition, many families were dealing withmore than one type of coverage or with frequentchanges in employer-sponsored plans. In our workwith almost 2,000 families to secure coverage andclarify covered services, programs fell into threebroad categories: 1) private health insurance plans,2) public coverage and services including Medicaid/BadgerCare and Birth to 3, and 3) educationally re-lated supports and therapies provided through localschool districts.
The families who sought assistance through theFamilies MAP health benefits counselors were typi-cally two-parent households, most with one or twochildren and incomes over 200 percent of the pov-erty level. Those with higher incomes typically hadprivate insurance and many also had Medicaid cov-erage through the Katie Beckett Program. Familieswith lower incomes often had SSI eligibility and there-fore Medicaid coverage for the child with specialneeds. Approximately eleven percent had no cover-age for the family.
The service needs families most often re-quested help with were advanced medical care (i.e.,surgery, cancer care, hospitalization due to complexcare needs), therapies (speech, physical, and occu-pational), mental health services, and prescriptionmedications. The coverage issues related to theseservices were typically benefit limitations (such asan insufficient number of therapy sessions covered),benefit exclusions (no coverage for mental health),denials of coverage as not medically necessary, andcosts not covered due to copays and deductibles.
MANAGED ADVOCACY IN ACTION Background • 9
Events triggering the requests for assistancewere often an application denial, both for Medicaidand private insurance; denial related to a specifictreatment need; and loss or imminent loss of cover-age due to job changes, divorce, the child’s transi-tion to adulthood, or changes in family circumstancesor the child’s health status that threatened eligibilityfor public programs. A pressing issue for many fami-lies stemming from these triggering events was theaccumulation of medical debt they didn’t know howto pay, or needing care for their child they couldn’tafford to get. Another issue that rises to the top formany families is quality and coordination of care (seeappendix A for a listing of Wisconsin Services andPrograms).
Managed care and the specialneeds child
In the past ten years, most health insurance planshave transitioned from fee-for-service to managedcare plans—including Medicaid. Fee-for-serviceplans, although often more costly, allow you to seeany physician, for any service, whenever you choose.You may have to meet a deductible or pay a co-pay-ment for those services, but in general the care youreceive is very flexible and therefore suits the needsof children with special health needs well.
Managed care plans are less costly but are alsoless flexible (see box below on Capitated Rates).Under a managed care organization (MCO), youmust get services from a specific group of provid-ers, with authorization by your primary care physi-cian, and must obtain a referral each time you needto see someone outside of the provider group. WithMedicaid’s transition from fee-for-service to managedcare, coverage for the many families who have chil-dren with special health needs has become morecomplicated.
There are several problems that stand in theway of children with special health needs receivingthe optimal care that they and their families can af-ford. The emphasis on cost-containment creates anenvironment in which primary and preventative careare emphasized—with a clear economic disincen-tive against offering complex treatments. This provesparticularly troublesome for children with specialhealth needs and their families. These families don’tjust take their child to the family practitioner like mostparents. They do have a primary health care pro-vider, but many also rely on an intricate web of spe-cialists, therapists, educational-related serviceproviders, social services officers, and a range ofother supportive professionals—most of whom re-main outside the managed care system. The realityof the child with special needs runs counter to theentire structure of managed care.
Capitated RatesManaged care organizations pay providers with what’s called a capitated rate. That means a doctor gets a setamount for seeing a set patient—whether she is a healthy 30 year old non-smoker or a 8 year old with spinabifida—and under most cases, the patient will primarily see that doctor and will have to obtain a referral to seeany other provider. An MCO does not differentiate between those with intensive needs and those with routinehealth care needs—all patients are the same when they walk in the door. This makes financial sense, but a sideeffect is that MCOs have an incentive to either (1) avoid enrolling the disadvantaged and medically complexchildren who have costly health care needs in order to save money for the extra time children with special healthneeds require or (2) place onerous restrictions on access to all but the most basic services so that it is difficult forchildren with special health needs to obtain more expensive services.
10 • Background MANAGED ADVOCACY IN ACTION
Looking toward the future: Incorporatingprinciples of the Medical Home model andHealthy People 2010As we look beyond the work of Families MAP, weneed to take environmental factors into consider-ation. The Maternal and Child Health Bureau at theUnited States Department of Health and Human Ser-vices and the American Association of Pediatricshave been taking a careful look at the ways in whichhealth care is delivered to and accessed by childrenwith special health care needs. As a result, severalconcepts are being implemented on a national ba-sis.
The first, the Medical Home model, was devel-oped by the American Academy of Pediatrics, in col-laboration with Family Voices, the Maternal and ChildHealth Bureau, the National Association of Children’sHospitals and Related Institutions, and Shriners Hos-pitals for Children. This model focuses on a partner-ship approach to delivering medical care and is firstand foremost family centered. There is a summaryof these important principles on the next page.
Healthy People 2010
The Medical Home principles have been incorpo-rated into Healthy People 2010, a joint effort led bythe Maternal and Child Health Bureau, the Ameri-can Academy of Pediatrics, Family Voices, andMarch of Dimes along with many other organizationsin the public and private sectors, to bring better healthcare to all people in the United States. Achieving Suc-cess for All Children and Youth with Special HealthCare Needs outlines the 10-year action plan that ad-dresses the objectives in Healthy People 2010 re-lated to the care of children and youth with specialhealth care needs. The six core objectives of Achiev-ing Success are:
� Families of children with special health careneeds will partner in decision making at alllevels and will be satisfied with the servicesthey receive;
� All children with special health care needswill receive coordinated ongoing compre-hensive care within a medical home;
� All families of children with special healthcare needs will have adequate private and/or public insurance to pay for the servicesthey need;
� All children will be screened early and con-tinuously for special health care needs;
� Community-based service systems will beorganized so families can use them easily;
� All youth with special health care needs willreceive the services necessary to maketransitions to all aspects of adult life, includ-ing adult health care, work, and indepen-dence. (source: National Center for MedicalHome Initiatives)
The Wisconsin Maternal and Child Health Pro-gram and its advisory committee is working to makesure that each child in the state has a medical anddental home by 2010. Additionally, this program isworking to incorporate the six core outcomes of the2010 plan in its programs as well.
As we leave Families MAP, we are excited aboutthe opportunities that exist in our state as work con-tinues to provide Wisconsin’s children with specialhealth needs and their families better health insur-ance coverage and more comprehensive servicesand care that they require. This blueprint for man-aged advocacy, when implemented, can provide agreat impetus for moving us down that road.

MANAGED ADVOCACY IN ACTION Background • 11
Medical Home PrinciplesThe medical home concept contains seven primaryelements. These are described below with a brief ex-planation of their meaning within the medical homecontext.Accessible: Accessibility is a multi-pronged compo-nent of the medical home:
Care in the Child’s Community: In order to be ac-cessible there have to be minimal requirements forobtaining care outside of local community. Addi-tionally, care should be given within a communityof other children.Physical Accessibility: This considers elementssuch as the geographical location, availability ofparking or public transportation and the accessibil-ity of buildings.Time Accessibility: Increased availability of ap-pointments, reduced waiting times at appointmentsand coordination of appointments with differentproviders (for multiple children if necessary) toavoid multiple trips to the facility.Medical Records Accessibility: All health recordsmust be made available to parents, other health careproviders, insurance programsInsurance Accessibility: Providers must accept alltypes of insurance private and public, assistancewith obtaining eligibility, filing claims and bring-ing appeals of denials, as well as accommodationas insurance programs change.
Coordinated: Care needs to be coordinated amongall those involved with the child, including the fam-ily, care giver to care giver, institution to institution,between care givers and payors, support, educationaland community-based services. Centralized informa-tion needs to be available to all of these entities aswell.Continuous: The medical home ideal states that careshould be continuous between providers, such as thePrimary Care Physician, other health care specialistsand health care institutions, as well as across the lifesituations and transitions of the child (Clinical, Home,School, Adulthood).Comprehensive: Comprehensive care includes carethat is available at all times, all degrees of intensity(preventive, primary, tertiary) and that insurance cov-erage is available and accepted for all levels of care.Culturally Effective: A family’s cultural backgroundmust be recognized, valued and respected, along withthe place of the child in these values.Family Centered: The family is always the principalcaregiver and the center of strength and support forthe child. Providers must support that role and giveunbiased and complete information to the family onan ongoing basis.Compassionate: The medical home concept includesexpressing and demonstrating concern for the well be-ing of the child and the family by everyone involvedin the child’s care.


Managed Advocacy Project
Chapter Two
What is managed advocacy? This simple questionis more difficult than it sounds due to the fact thatmanaged advocacy is more of a concept and a philo-sophical approach that can take on a different huedepending on the community where it is imple-mented. Having said that the definition is hard topin down and is, in fact, elusive and flexible, thereare some basic principles that form the broad out-line of the Managed Advocacy concept.
Managed Advocacy Defined
The Managed Advocacy Program is focused on athree-pronged approach:
1) advocating directly with families of CSHNto solve their health care access financingproblems;
2) organizing and educating parents ofCSHN, service providers and advocates tobecome active and involved participantswith managed care organizations on apolicy level; and
3) developing the information and advocacyinfrastructure to promote fundamental policychange and ongoing system responsive-ness in managed care organizations.
The vision of Families MAP was to improve thesystem of care for children with special health needsin managed care environments and create a sup-portive infrastructure where: 1) families fully under-stand their rights and options and can effectivelyadvocate on behalf of their children, 2) comprehen-
sive and accurate advocacy resources are availableto families in a timely manner, 3) systemic problemsaffecting children with special health needs are docu-mented and addressed in partnership with policymakers and managed care organizations and 4) par-ents are fully involved and confident in making deci-sions to place the care of their children in the handsof managed care organizations.
In order for the Families MAP to achieve its vi-sion, five goals would need to be met. Those include:1) maximizing insurance coverage for children withspecial health needs and promoting linkages to pri-mary and specialty care, 2) increase the coordina-tion and integration of services among managed careplans and other providers of services to children withspecial health needs, 3) expand family participationin managed care policy development, 4) developrecommendations to facilitate access to a medicalhome for children with special health needs and 5)improve family satisfaction in managed care.
Managed Advocacy by Design
Experience has shown that managed care systemsgenerate both worry and frustration for children withspecial health needs and their families. The contextwithin which these families care for their children issensitive and complicated. It includes not only theirprimary health care providers, but an intricate webof specialists, therapists, educationally-related ser-vices, social services, and other family support sys-tems – most of which remain outside the managedcare system. The transition to managed care for

14 • Managed Advocacy Project MANAGED ADVOCACY IN ACTION
these families can disrupt carefully nurtured networksof care and support, and exacerbate the difficultiesof navigating multiple systems of care and financ-ing. Moreover, the managed care system, organizedaround the axes of cost containment and primarypreventative medicine, is not very adept at respond-ing to the needs of children with chronic illnessesand disabilities. It is not uncommon for children withcomplex needs to require many different types ofservices, by multiple providers, who may or may notbe familiar with the child’s condition(s). The role ofthe health care advocate, which falls to the family orfamily support case manager, becomes a frustrat-ing, but essential task.
Families MAP was developed at a time whenmanaged care was developing rapidly across thestate of Wisconsin. Of course the expansion of asystem of care that did not necessarily fit well withinthe care needs of people with special needs, par-ticularly children, caused great concern for advo-cates, parents and providers. Indeed, it was thenotion of “direct cost containment” that stimulatedparents and advocates to action. These efforts haveled to the development of strategies to create sys-
tems that are supportive to families that need to navi-gate the complicated world of managed care.
The Families MAP Project was an important op-portunity to develop and test models of managedadvocacy for families and children with special healthneeds. As the dominant delivery system for healthcare in Wisconsin, managed care presents severechallenges to many families and their children. Ourchallenge was to design a system that would bothsupport the family and honor the central roll they playin a child’s life, but at the same time respond to anevolving health care system that was reacting to es-calating costs through restrictions in choice and limi-tations in service. As health care has become moresophisticated and integrated, the advocacy systemsthat were developed to help families through thatsystem have not kept pace. Families MAP, as dem-onstrated in Wisconsin, offers the potential to en-sure that families have access to accurate and timelyinformation and appropriate resources; to peer-to-peer parent support and, most importantly, to skilledand knowledgeable advocates and lawyers who un-derstand the system and who can help families ne-gotiate those systems.

A Blueprint for Helping Familieswith Health Care Coverage
Chapter Three
The design of Families MAP is based on severalsimple principles. Yet as in any good plan, simpleprinciples choreographed in harmony can create amodel of enduring quality and durability. Like a wellbuilt home, Families MAP stands on a solid founda-tion of health benefits counseling and legal services,the cornerstone is the active participation and thecontributions of life experience from parents. Thesturdy walls are held together by a strong collabora-tive network of key stakeholders working together tosolve difficult system and public policy issues relatedto coverage and access to care for families.
In order for the Families MAP model to fully func-tion the three major components of advocacy mustbe in place. Additionally, parent participation and keystakeholder collaboration should work together topromote positive change both for individual familiesand the larger systems of care and coverage forCSHN.
The Foundation
Direct services to clients are the essential elementof the Families MAP model. Although service pro-viders abound in the spectrum of needs that fami-lies and CSHN require, very few programs integratecommunity-based advocacy and legal resources onbehalf of clients. Health benefits counselors are prob-lem solvers in the area of health care payments. Theyare responsible for being familiar with as many healthcare payment options as they can, ranging from Med-icaid to the local Lion’s Club. What they don’t knowabout, they are responsible for having the investiga-
tive tools to find out. And when they know some-thing of a program, but not in enough detail to an-swer their client’s questions, they are responsiblefor having the persistence to get the answers or sup-port their clients in getting the answers. Persistence,investigative skills, and comprehensive detailedknowledge are the hallmarks of a health benefitscounselor, whether that counselor is a parent con-sultant, a benefits specialist in the health care facil-ity, or a benefits counselor in an community-basedadvocacy organization.
The services provided by benefits counselorsare broad, ranging from brief information and refer-ral to intensive formal advocacy. Some examples ofactivities counselors may engage in are:
� explaining the application process for Med-icaid;
� assisting with preparation of a Katie BeckettProgram application;
� providing counseling and intervention in as-set valuation for SSI applications;
� representing clients at HMO grievancehearings, Medicaid fair hearings, and SSIappeals hearings;
� locating financing resources for obscure orunusual health needs;
� negotiating with health care providers andcollectors over medical debt payment prob-lems;
� researching health insurance policy lan-guage to challenge inappropriate claim de-nials.

16 • A Blueprint for Helping Families MANAGED ADVOCACY IN ACTION
The Cornerstone: Parent involvement
To say the direct and active involvement of parentsin the planning, development and implementation ofFamilies MAP was crucial is an understatement. Par-ent leadership provided not only the passion and thelink to real world experiences but also helped to craftthe vision and build the structure of a new system ofadvocacy that merged with the established conceptsof care embedded in the Medical Home philosophy.
Families MAP endeavored to help families advo-cate for themselves by giving them the tools, informa-tion and advocacy advice to resolve difficult issues.Families MAP also honored the family’s role to decidetheir own priorities and approach to solving a givenproblem in the context of the needs of the entire family.Thus even if a parent asks a MAP counselor for helpregarding only one child with special needs, the cover-age needs of other children and the parents will beexamined. Throughout the process, families were notalone. Rather, in the background was a structure ofsupport from other parents and a link to accurate andtimely information that was buttressed by the force ofadvocacy and the law.
Parents and families had a direct link to otherparents. The parent advocates who worked as staffto the project and pilots provided an important linch-pin in bridging the gaps between Families MAP andother groups serving families. Parents engaged witha variety of advocacy and grassroots organizationsand were vocal members of committees and boardsengaged in policy discussions. More importantly theywere well connected to parent support groups andleadership training programs. Their dedication andcredibility gained through experiential kinship withother families was critical for the successful imple-mentation of Families MAP. Through frequent con-tacts at HealthWatch meetings with others involvedin helping families, parent advocates helped every-one reach a philosophic higher ground that wasbased on a mutual respect and a willingness to helpmeet a common goal: creating a better system forfamilies and children with special health needs.
The Walls: Key stakeholdercollaboration
The ability to build contacts and support in the com-munity of colleagues and bureaucrats (who may alsobe potential competitors and adversaries) is vital tothe development of a Families MAP model. ABC forHealth has approached this need in a variety of ways.We have worked with other advocacy groups in ourstate by inviting members of various advocacy groupsto join our statewide stakeholders committee; com-municating with advocacy groups through our train-ing programs, newsletters and publications;participating in and supporting other organizationsby serving as speakers and participants; making ap-propriate referrals to their agencies—and we haveparticipated actively in local HealthWatch commit-tees.
We have also learned through daily contactswith others involved in helping families in the healthcare system that there is an etiquette for dealing withhigh level bureaucrats and lower level staff, both onindividual cases and on broader policy reform issues,and that that etiquette must be based on a basicrespect for their willingness to help and recognitionof the validity and reasonableness of their perspec-tive.
Collaboration in implementing a Families MAPmodel works best when a clearly outlined and de-tailed plan of collaboration is developed; where jobresponsibilities were well-defined and the respec-tive responsibilities of each agency were understoodfrom the beginning. Good will and trust is decreasedif careful communication is lacking about such im-portant issues as the role of the health benefits coun-selor; the participation of parents within the network;the nature of the relationship between the partneragencies and the training and backup agency; thefinancing of positions; the responsibilities for fund-ing the position; payment for associated costs andongoing training. It is critically important to ensurethat there is a commitment of time and money toboth develop and maintain the key components ofthe Families MAP. Health care coverage is a rapidly

MANAGED ADVOCACY IN ACTION A Blueprint for Helping Families • 17
changing field, and without continual updating, thevalue and reliability of the counselor’s advice candeteriorate rapidly, and soon a credibility gapemerges as program staff lose their expertise on thecurrent health care coverage landscape.
Community educationSpreading the word. ABC for Health has found thata critical component of the Families MAP program isa variety of training and public education efforts.These activities are effective means of outreach, andprovide an efficient way to extend the informationand experience developed by the counselor andother project staff to a broader audience. Moreover,the necessity of communicating knowledge and strat-egies to an audience solidifies and hones theprogram’s expertise and health care financing knowl-edge. The project has provided intensive and ongo-ing workshops and trainings for parents andadvocates as well as health care provider staff andhealth professionals. Public education projects haveincluded consumer-friendly resource manuals andinformational brochures as well as web site informa-tion and other online materials. Project staff has alsobeen invited into university classrooms and healthpolicy forums to discuss the concept of health ben-
efits counseling and provide input on the future ofthe health care system. All of these activities buildvisibility in the community, while also providing sig-nificant, practical help for families and service pro-viders.
Policy reformMaking micro macro. A great strength of the healthbenefits counseling component of Families MAP isits ability to encompass both individual casework andpolicy level reform. The detailed and groundedknowledge gained through working with families asthey struggle with the system makes for a much richerand well thought out critique of the policies guidingthat system. One of the benefits of having a variedand community-based approach to health benefitscounseling is the keen insight into system failuresthat counselors develop. The legal backup compo-nent, working in concert with counselors, then pro-vides the expertise to translate individual casehistories into an advocacy strategy, whether throughHealthWatch committee work or policy positions orindividuals engaging in community organizing, oradvocacy within an administrative agency.

Identifying Barriers inManaged Care
Chapter Four
What problems do parentsexperience with managed care?
One of the first activities of the project was to iden-tify barriers to health coverage and care faced byfamilies. First we began by analyzing our experienceas health benefits counselors and attorneys in rep-resenting clients. ABC for Health developed healthbenefits counseling as a service to families thathelped us to identify, solve and organize around thehealth care financing and access issues negativelyaffecting families. Our direct knowledge gained inrepresenting families provided an important glimpseinto the struggles and barriers they encountered. Ad-vocating for others often begins with identifying theirproblems and concerns about getting needed ser-vices for their children and searching for ways to ad-dress them. Moreover, many of the complicationsthat families have when trying to navigate the healthcare system relate to figuring out how to pay for andaccess needed services. Offering services to assistfamilies in identifying their problems, sharing themand working together to solve them is the key ingre-dient of “advocacy” in managed advocacy program.
Next we assembled the key stakeholders in-volved in the care and treatment of CSHN. Theseincluded the parents, providers, managed care rep-resentatives, school health providers, as well as leg-islators and the media. By working with thesestakeholders we assembled an important cross sec-tion of issues that affected CSHN from a variety ofperspectives. Our first efforts were at HealthWatch,which were monthly meetings of the stakeholdersdescribed above to discuss systemic issues andstrategies for change. Subcommittees took action
on the needs and strategies identified at the Health-Watch meetings. More ideas came from participantsin training activities and events. The barriers facedby parents in an attempt to secure services or cov-erage for their CSHN are innumerable. The follow-ing are the major issues heard from families, clientsand service providers who participated in Health-Watch coalition meetings or attended communityeducation events.
Accurate and timely information on careand coverage options for CSHN is difficultto obtainMany families struggle finding services and fundingafter their child is born. Parents are overwhelmed bythe care needs of their child and are often confusedabout referrals or fail to get the right information aboutappropriate services at either the state or local level.In general, providers at all levels appear to lack for-mal mechanisms to link services so families can ben-efit maximally from money spent for their child’s care.Many health care providers, education staff, and so-cial service agencies in the community remain un-aware of the full array of current services availableto families.
The eligibility and application process forpublic health coverage programs iscomplicated and confusingThe eligibility and application process for Medicaid/BadgerCare is often confusing and misleading forfamilies. CSHN may fall into one or several differentcategories of recipients eligible for Medicaid, butthese categories are not self-explanatory in and of

20 • Identifying Barriers in Managed Care MANAGED ADVOCACY IN ACTION
themselves. In many cases, families self deny be-fore they see the income eligibility guidelines andassume they are not eligible. In fact, at least somemembers of their family may be eligible for cover-age. Even when families fill out and submit the ap-plication, they are often unable to determine fromthe long, complicated notices whether they are en-rolled or have been denied.
Choosing a Medicaid HMO is confusingOn top of the challenges that all families face duringthe application process for Medicaid, families withCSHN often must, if approved, make a decisionabout their provider network without adequate knowl-edge about which network would best serve theneeds of their child. This can happen because thechoice of managed care organizations (MCO) offeredto families is based on those that have not reachedtheir Medicaid enrollments caps. Often only one MCOis available to those that are eligible and if there isactually a choice between MCOs, families do not re-ceive adequate information about which servicesthey provide or what specialists are available.
Families struggle to obtain needed HMOplan information about services andprocessesFamilies may face obstacles obtaining and under-standing HMO plan information. Again, families needaccurate, timely and helpful information about itemssuch as notification requirements after emergencycare, the correct procedure for obtaining referrals,what providers are in their network, and what to dowhen network participants change. Families of CSHNmay need information about how HMOs treat a par-ticular condition or whether a specific drug is on theirHMOs formulary. Obtaining such information is of-ten challenging and families are often faced with longwaiting periods on the phone and vague and contra-dictory information when they contact their MCO forassistance.
Services are provided by a fragmentedsystem of providers and specialtypracticesParents of children with special health needs are frus-trated by fragmented services and poor access tospecialty practices necessary to meet their child’sneeds. Fragmentation occurs when there is no co-ordination between programs, providers, and com-munity resources. This lack of coordination ofnecessary services is broader than just in the child’sspecific medical provider in a clinic or hospital set-ting. It also occurs when parents work with socialworkers and discharge planners, expecting infor-mation and referral sources to resources that willhelp their child.
The following were identified by parents as bar-riers that affect providers and agencies and kept themfrom working together effectively:
� Lack of communication between agenciesand providers;
� Differing priorities and attitudes amongagencies and providers;
� Difficulty in updating information regardingother services of agencies;
� Lack of coordination between specialists orservices within the same agency
� General administrative demands, e.g.,changes in policies and large caseloads;
� Inadequate funding and staffing;
� Competition for funding; and
� Confidentiality requirements
Funding sources are fragmented and thisleads to confusion about coverageFor a parent of a child with special health needs,paying for the myriad of medical care needs, thera-pies, and durable medical equipment can be an over-whelming financial hardship. The complexity ofnavigating these systems increases dramatically

MANAGED ADVOCACY IN ACTION Identifying Barriers in Managed Care • 21
when parents must deal with coordinating benefitsbetween different insurance plans as well as publicbenefits program rules and regulations.
Therefore, many parents purchase a private in-surance plan and supplement the private insurancewith Medicaid coverage, usually through eligibility foreither Supplemental Security Income (SSI) disabil-ity eligibility, or through eligibility for the Katie BeckettMedicaid program. In some circumstances, if bothparents are working, there are coordination issuesbetween two private insurance plans and Medicaid.Each coverage plan is complicated in and of itself.Parents and children often end up being caught inthe middle between two or three entities all pointingfingers at the other in an attempt to get someoneelse to pay the bill, while in the meantime, the billsmount or the child is not getting needed services.
Access to other services and specialists iscontrolled by a primary care physicianwho often does not have an expertise inneeds of the childManaged care plans frequently require that a childhave a primary care physician (PCP) that makesreferrals to other services and specialists. Whatevertype of practitioner the PCP is, the reality is that thePCP manages both the care and the benefits, andessentially becomes a gatekeeper responsible fordeciding, in compliance with HMO financial formu-las, whether or not a referral to a specialist is appro-priate.
Parents are concerned that general practitio-ners and pediatricians do not have specialized knowl-edge to recognize and care for needs of their child;and because of that, are afraid of a missed diagno-sis.
In addition, HMOs set seemingly arbitrary rules(as opposed to set standards), and financial limita-tions (as opposed to health-care needs). The resultis that patients – and especially children with spe-cial health needs — do not receive needed or ap-propriate treatment. An HMO’s referral system affectsnot only the access to care by untimely decisions or
inappropriately denied referrals, but also the qualityof care if standards for referrals are made too re-strictive.
Lack of diagnosis-specific medicalinformation and resources for parentsParents are frustrated by their lack of knowledgeabout the complex medical diagnoses of their chil-dren. They are anxious to know everything they canabout their child’s conditions, treatments and learncoping strategies that will help them and their childmanage symptoms, monitor progress, be alert to sig-nificant changes, and have the latest possible infor-mation on treatments and care that will help theirchildren. They look to their primary care physiciansfor this type of support and information, but oftenfind that these doctors do not have the time to in-form themselves on the complex, diagnosis-specificinformation parents are looking for. This leaves par-ents to spend endless hours doing their own re-search.
Access to needed services for CSHN,particularly therapy services, ischallenging.In an effort to curb inappropriate utilization, andthereby control costs, health plans may establishcomplex prior approval procedures for many neededservices. This system of hoops and hurdles must benegotiated before access to necessary care will begranted. However, the process of receiving a priorauthorization for care, or appealing a denial of careto a grievance committee can seriously delay neededservices, sometimes irreparably. However, manychronic conditions CSHN have require ongoing spe-cialty care. Despite this, the use of standing refer-rals still is not available in most MCOs.
Lack of clarity about medically necessaryservices leads to frequent denialsThe term medically necessary services is sometimesused in both public and private coverage to denyservices, equipment and treatment for CSHN.

22 • Identifying Barriers in Managed Care MANAGED ADVOCACY IN ACTION
Oftentimes the definition used in state or privateplans is ill suited to meet the ongoing needs of CSHN.Services may be considered experimental in naturesimply because the third party payer does not haveaccess to available documentation or research out-comes that could justify a medical need. Conse-quently, obtaining referrals and approval for servicesis extremely challenging for families with CSHN. Inaddition, understanding the grievance procedure,coupled with gathering the needed proof to challengea denial based on medical necessity is both chal-lenging and complicated for families.
There is usually no health benefitscounselor working for the family to assistwith fragmented services and fundingMany families struggle while trying to negotiate a va-riety of services and programs, each with their ownset of rules. Families benefit from a health benefitscounselor who advocates only for the family and childand who would be helpful in negotiating these com-plex systems. Coordination problems are also exac-erbated for families who deal not only with multipleagencies, but also with multiple systems that caninclude long-term support programs, public schoolprograms, health care specialists, child protectiveservices, and others. Parents also report that whendealing with multiple medical specialists, therapists,and billing departments, they sometimes run intoproviders who do not understand the complexity offamilies’ needs.
Lack of support and planning help fortransitions makes creates additionalbarriers and challengesFamilies with CSHN face significant challenges inmaintaining continuity of care and funding for theirchild’s health care during life transitions such aschanging schools, summer break, and the transitionto adulthood or when transitioning from fee-for-ser-vice to managed care.
Loss or changes in coverage because ofchanges in plan or providerContinuity of health coverage is a common problemfor families who have insurance through their em-ployer, where the employer-sponsored coverage maychange from one plan to another every year. At anypoint during a person’s enrollment in an MCO theemployer may terminate the contract. This meansthat at any point a family with a CSHN may be forcedto switch providers and thus disrupt their child’s con-tinuity of care.
Finding qualified providers and paying forthemFor families in many parts of the state the shortageof dental and mental health providers who acceptMedicaid and understand the needs of CSHN hasreached a crisis level. Other services that providesupport to families, such as respite, day care and in-home nursing services can be anywhere from diffi-cult to impossible to find. In addition, in a true medicalhome, the variety of services a child with specialneeds requires will be offered in a minimal numberof settings. When services are fragmented, parentsare often forced to go to many different providers ina variety of locations to access care. This may in-clude accessing services such as therapies, specialtycare, assessments and evaluations, or specializeddurable medical equipment.
And when they can be located, parents still raninto difficulty finding a means to pay for them.
Grievance procedures are limited anddifficult to pursueFamilies often feel at a disadvantage when pursu-ing a grievance. Facing a managed care grievanceteam that includes legal staff, claims administratorsas well as medical consultants is intimidating. With-out help from a lawyer or advocate, families mayalso not be fully aware of their rights. Since attorney

MANAGED ADVOCACY IN ACTION Identifying Barriers in Managed Care • 23
fees are mostly nonexistent when challenging anMCO and fees to families may quickly exceed thecost of care, many families go it alone.
Using the MAP Blueprint
The next three chapters describe the activities usedin Families MAP to create solutions to these chal-lenges for the families in our project. First, healthbenefits counseling services were offered to any fam-ily of a child with special health needs with a healthcare financing problem—getting coverage, payingbills, or getting prior authorizations for services. Oncecontacted, benefits counselors worked directly withindividual families to address the immediate healthcare or coverage need the family was facing.
These families and others contacted throughnetworking with community agencies and providerswere invited to work with a group of interested par-ents, service providers and advocates in locallyformed HealthWatch committees. HealthWatch com-mittees identified local needs and goals that guidedthe development of each program. Activities includednetworking to solve locally based problems andstrengthen community resources; policy action; andcommunity training and educational resources.
There were successes and some frustrating dis-appoints that emerged when trying to address somany complex issues in a continually changing en-vironment. The impact of parent involvement in thisproject was enormous, and yet, the challenges toparent participation remained a constant concernwhether planning work schedules, meetings or com-munity workshops.

Families MAP and HealthBenefits CounselingThe Blueprint in Action
Families in crisis due to a health care coverage oraccess issue need a source of accurate and timelyinformation; they also need a reassuring voice anda steady hand to help guide them through an oftenemotional process of challenging an inappropriatecoverage denial or termination of benefits. For thefamilies participating in the Families MAP pilots thehealth benefits counselor served the role of advo-cate, friend and a link to legal resources and a vastarray of supportive resources.
Health benefits counseling provided the foun-dation of the individual advocacy piece of FamiliesMAP. Our counselors, parentadvocates and attorneys workedwith parents of children with spe-cial health needs to identify andresolve many problems withhealth care coverage or accessissues, including: connecting toinformation on public and privatehealth care financing programsand supportive services, gainingan understanding of their cover-age options that empoweredthem to make their own deci-sions; receiving application assistance for Medicaidprograms and advocacy assistance with grievancesand appeals, and taking actions that improved healthcare and avoided depletion of family resources.
Frequently families contact a health benefitscounselor during a crisis. Something has gone wrongor is simply too confusing or stressful to deal with orunderstand. The counselors role is to work with fami-lies to resolve immediate problems as they also
evaluate the health coverage needs of the wholefamily. By taking a proactive approach to workingwith a family, counselors can help prevent future cov-erage issues while at the same time empoweringthe family with information tools and resources. Thecounselor will also follow-up on unresolved issuesto ensure a potentially successful coverage strat-egy does not fail because of a missed deadline orincomplete form. On occasion, advocacy efforts riseto the level of legal intervention after administrativeappeals, or internal grievance procedures have beenexhausted. Access to legal services by an attorney
can provide the critical leverageneeded to nudge a recalcitrantthird party payor into action.Sometimes the mere shadow ofthe law can effect positivechange for families strugglingwith benefit denials or termina-tions. Other times a lawyer mayhave to intervene by filing suit.
Health benefits counselorsgain an important ground-levelview of the problems encoun-tered by families with children
with special health care needs in their communities.Moreover casework leads to the identification of sys-tem-wide barriers, specific managed care plan poli-cies, or geographic barriers that affect families intheir daily lives. For example, in Families MAP, onesuch issue was funding stream coordination betweenthe Medicaid program, the public schools and pri-vate insurance providers. A state representative whobecame active in Families MAP attended several lis-
Health Benefits Counseling ServicesDirect client services include: health ben-efits counseling to inform families of pos-sible eligibility for programs or services;consultation about patient’s rights and ob-ligations under their managed care plan; as-sistance with filing grievances and appeals;legal assistance with filing hearings, andconnections to support groups or other rel-evant organizations.
Chapter Five

26 • Families MAP and Health Benefits Counseling: The Blueprint in Action MANAGED ADVOCACY IN ACTION
tening sessions with parents. Based on their con-cerns, he launched an initiative to help develop abetter process to coordinate funding for families andchildren with special health care needs. This initia-tive also led to a workgroup on coordinated fundingto carry on this policy initiative.
Health Benefits Counseling:The process
Perhaps the most powerful and most compelling wayto describe the process of health benefits counsel-ing and Families MAP is through the stories of bravechildren and families served by the project. Yet thedetailed systems and structures developed as a partof the health benefits counseling process merit a dis-cussion and description to fully understand the pro-cess to get quickly to the details of the issueschallenging a family. Consequently the nitty grittyprocess of health Benefits counseling that followswill also be enlivened by examples that representthe casework of the health benefits counselors andattorneys
Family NeedsIn a perfect world, benefits counseling would be avail-able to all families 24/7. In our Families MAP reality,this was not possible. What we could do was striveto create systems that help families and CSHN atcritical times when parents feel they need counsel-ing help the most: at the birth of a baby, when afamily first learns of a diagnosis from a provider, orwhen a family finds that their health coverage oraccess to coverage has been terminated. No mat-ter the circumstance, a first priority for a health ben-efits counselor is getting connected to families whenand where the counseling services can be of thegreatest benefit. This in turn decreases stress onfamilies caused by worry about medical expenses,and starting or delaying needed treatment and thereal or long-term damage for children caused bythese missed opportunities.
Everything begins with getting the message toparents that they are not alone in trying to find as-sistance and answers to their questions. Health ben-efits counseling begins with quickly connectingfamilies with advocacy to find the care and cover-age solutions they seek. Connecting families to ben-efits counseling quickly is also important due to thelimited application time frames of public health cov-erage programs. Sadly, missed time lines meanmissed coverage opportunities for families. The vigi-lance of the counselor working with the family cansave not only dollars for the family but also the heart-break of massive bills and possible disruptions inrelationships with providers. In the end family stressis reduced and more care and attention can be fo-cused on the child.
Reaching out to parentsWord of mouth from parent to parent may be themost effective strategy for health benefits counse-lors to connect to parents. Word will spread quicklyif high quality services that get results are delivered.Through parent-to-parent support groups or otherparent-related associations, parent advocates arevery effective in talking with other families and shar-ing resources and valuable firsthand experience.Outreach to parent support groups can be achievedby sending written information describing servicesor attending meetings to talk to parents about healthbenefits counseling services.
In addition to parent groups, the counselorshould be well-networked with health care provid-ers, community agencies and advocates who workclosely with families and CSHN. Indeed an impor-tant strategy that health benefits counselors use toget connected to families is integrating with the ser-vice provider community. For example following upon an initial contact by a medical provider who maycall on behalf of the family or may contact the ben-efits counselor to see if a referral is appropriate.These technical assistance calls build relationshipsbetween agencies and provide an ongoing informa-

MANAGED ADVOCACY IN ACTION Families MAP and Health Benefits Counseling: The Blueprint in Action • 27
tion network that expands the effectiveness of anybenefits counseling efforts done by a single organi-zation.
All of these ways of forming connections involvedoing community outreach. Brochures, newspaperarticles, presentations to community groups, present-ing information at workshops and conferences allbuild connections and get the word out. If a counse-lor can’t do all of these things, the most importantplace to put effort is on building a strong connectionto the professional network in the community. Theother things will come.
The First Step: Intake interviewMost often, the first contact with a parent is a phonecall in which the benefits counselor collects informa-tion, first to analyze the coverage problem and de-termine if the issue falls within the scope of thecounselor’s services, or make a referral to other com-munity resources. Once the caller is determined tofalls within the health benefits counselors scope ofservices, an intake form is completed (see a sample
intake form in appendix B). The intake interview col-lects information that serves a number of purposes.It will be used to:
� determine the urgency of the problem—there is no way to overstate the importanceof a timely response when offering finan-cial counseling services and the need toidentify immediate sources of care and cov-erage pending the review of a denial.
� determine what the caller is asking - in afamily crisis, the caller may not always beable to clearly say what they want. Theymay simply state that they have no healthinsurance for their CSHCN, or cannot payfor a needed service.
� determine if the family has private or publichealth care coverage
� determine financial and non-financial eligi-bility for either purchasing a private insur-ance plan or applying for public programs(as illustrated in the case study below)
Case Study—Financial and non-financialeligibilityAngela and Kevin are married and have onechild with special health care needs due to agenetically inherited condition. Angela is now 5months pregnant with their second child, andthe pregnancy is considered high risk due tothe genetic factors that affected her first child.Kevin was recently laid off from his job of fiveyears, but fortunately was only out of work fora month before finding a new job. Kevin signedup for insurance at his new job, but was toldthat there was no coverage for Angela’s preg-nancy because it was pre-existing condition.Angela then checked into Medicaid HealthyStart as a coverage option, but found out thatKevin’s income was too high for her to qualifywithout first paying a several thousand dollardeductible.
Referral Sources for Families MAPService providers with mission related to health care
Health care providersCSHCN Program or Regional CentersBirth to 3 agenciesKatie Beckett ProgramCounty public health departmentsFamily Support Program
County human and social service departmentsNonprofit organizations
Community-based service agenciesAssociations or disease-related organizationsInformation and referral agencies
Community ContactsParent support groupsSchools, CESA, Head StartFriends and family

28 • Families MAP and Health Benefits Counseling: The Blueprint in Action MANAGED ADVOCACY IN ACTION
Angela knows Rose, the parent consultant inChippewa Falls, because she attends Health-Watch meetings and a parent group in her areato help her and Kevin find support and resourcesin coping with their son’s disabilities. Angelatalks to Rose at one of the meetings about herconcern in finding health insurance to pay forher prenatal care and the birth of her baby. Rosetells Angela that she will look into some optionsfor her. Later that day, Rose makes a call to theHealth Benefits Counselor she works with todiscuss Angela’s concerns.
The first thing that Rose is told is that there isa federal law called the Health Insurance Port-ability and Accountability Act (HIPAA) that pro-tects people from being rejected coverage dueto a pre-existing condition under these circum-stances (this law does not allow pregnancy tobe considered a pre-existing condition). HIPAAapplied to Angela because she was moving fromone group insurance plan to another without a63-day gap in coverage. The Health BenefitsCounselor did an intake with Angela and re-ferred this case to the supervising attorney toaddress with Kevin’s employer.
� determine if a grievance or appeal needsto be filed and the deadline for doing so
� determine what documentation needs to becollected from the caller to proceed withevaluating the case – for example, if thecaller has received a denial for a requestedservice, ask for a copy of that denial
� determine if other parties need to be con-tacted and a release of information needsto be signed
� explain what a health benefits counselorcan and cannot do – define the scope ofassistance and do not raise expectationsabove what can be offered
Gather documentation and evaluate issueAfter completing the intake the counselor will gatherrelevant documentation to evaluate and assess theidentified case issue. There are times when, afterinitial investigation, the issue might look somewhatdifferent from what the family initially described. Forexample. A family calls and tells the counselor thatthey have a denial of services and an unpaid bill asa result. They may be calling looking for representa-tion in the grievance process or to find out if otherfunding sources might cover those costs. Upon re-viewing the insurance policy, the counselor identi-fies that the service is clearly not covered and thatthe family may end up being financially responsiblefor service their child has already received. Althoughthis may not be the answer the parents were initiallylooking for, once the confusion is cleared up, manytimes parents are happy to have a better understand-ing of their coverage options.
Medicaid noticesNotices a family receives after applying for Medic-aid coverage should be reviewed by a health ben-efits counselor both for accuracy and to make surethe family or child receives the most beneficial cov-erage available to them. If a family receives a denialof eligibility, that denial should be assessed to de-termine the reason for the denial and to make sureall information used in the calculation of eligibilitywas correct. For example, if a family is denied eligi-bility for Medicaid due to excess income, the noticeshould be checked to make sure a Medicaid De-ductible was calculated as in the case example be-low.
Case Study—Medicaid Deductible
Katie and Sam are married and have two chil-dren, Emma age 6 and Josh age 2. Josh is achild with special health care needs. They haveinsurance through Sam’s employer, but thereis a $500 calendar year deductible per familymember and co-payments ranging from $15.00
MANAGED ADVOCACY IN ACTION Families MAP and Health Benefits Counseling: The Blueprint in Action • 29
to $50.00 for all medical services. The out-of-pocket costs, especially for Josh, are runningin the thousands each year. Katie and Sam arelooking for some help with these costs. Sammakes $35,000 per year and the income guide-lines for Medicaid eligibility for Josh to get cov-erage under the Healthy Start Medicaid programis $33,485 (year 2002), so Katie and Sam as-sumed there were no coverage options avail-able to them.
While talking to a Health Benefits Counselorabout their medical costs, Katie is told about“wrap around coverage” and the Medicaid De-ductible feature. This is when a family enrollsin Medicaid as a way to help meet out-of-pocketmedical costs even though the family alreadyhas a private insurance plan. This is especiallyhelpful for a family with a CSHCN where theregenerally are more doctor appointments,therapy visits, and prescriptions to buy. TheMedicaid Deductible feature allows the familyto use the outstanding medical debt and healthinsurance premiums they currently pay to offset their income that is above the Medicaid in-come guidelines. With a Medicaid deductiblemet, Josh can have Medicaid Healthy Start payfor all of his medical care that is not covered bySam’s private health plan.
After assessing the case with the family andusually after consulting a supervising attorney, thehealth benefits counselor should appeal a denial thatappears incorrect. The same process will also holdtrue for other types of denials, such as denial of cov-erage under a private insurance plan, a request forprior authorization for a type of medical treatment,durable medical equipment such as a wheelchair orwalker, or for therapy services.
Key Counseling Elements
Health benefits counselors (HBC)The benefits counseling process has many twistsand turns, with new directions to be explored all thetime. Counselors work with families to handle prob-lems from identification through to a legal referral.In broad strokes their responsibilities include:
� Conducting outreach to identify families ofCSHN
� Provides counseling and assistance to chil-dren with special needs who are not cov-ered and have inadequate coverage.
� Investigate terminations and denials of cov-erage for services and equipment
� Provides counseling and assistance fami-lies dissatisfied with their treatment by amanaged care organization, assists withproblem resolution including filing of com-plaints and grievance procedures.
� Serves as an independent advocate on be-half of enrollees in the resolution of dis-putes. Monitors and enforces compliancewith contracts and regulations at both anindividual case level and systemic level.
� Disseminates information and providescounseling regarding state managed careand insurance laws
� Collect information from HMOs as well asmaintains detailed and categorized recordsof the services it provides. Include clientdemographics, number and types of prob-lems and requests for assistance, sourceof referrals to the program, success of ad-vocacy work, time spent on specific pro-grams or inquiries, and program costs.

30 • Families MAP and Health Benefits Counseling: The Blueprint in Action MANAGED ADVOCACY IN ACTION
Parent advocatesFamilies MAP was enriched by having a parent ad-vocate working in each of the pilot projects. Thesesettings gave the project experience with the differ-ences in challenges faced by rural and urban fami-lies. Projects were set up in a Public HealthDepartment housing the Regional CSHN Center andin two community-based organizations—a large con-sumer advocacy organization and in a nonprofit lawfirm. Counseling, training and technical support ser-vices were provided to parents by an experiencedhealth benefits counselor and attorney located in thenonprofit law firm.
Parent advocates combined the real life expe-rience of raising a child with special health care needswith the experiential kinship that is offered to par-ents they assist. Many parent advocates have ex-perienced the hard knocks of problems accessingand paying for expensive and ongoing care for theirchildren. They have experienced hassles with insur-ance companies and denials for requests for ser-vices. These are parents of CSHCN who want touse their life experience to help other parents avoidtheir frustrations and disappointments, and who wantto improve the system for their own child and par-ents and children coming down the road. Parentadvocates are also in a critical pipeline of new infor-mation and can learn new skills to help them in theirown personal situation.
In this project, parent advocates worked parttime in the community in which they live and accessservices for their own children. A flexible, part-timeschedule allows a parent of a child with special needsthe ability to take care of the many needs their de-manding personal life requires, yet allows them tonetwork and grow in knowledge and abilities as aparent in the CSHN community. Parent advocatesreport that they felt rewarded in their ability to helpother parents and a renewed optimism in dealingwith their own life stressors.
Parent advocates played an important roll in theFamilies MAP project in accomplishing some of thegoals mentioned in the health benefits counselingsection. These key players in the project were in their
communities doing outreach to other parents andconnecting those parents to services on a daily ba-sis. The parent advocate ran local support groups,arranged local training events and brought in speak-ers for other parents who were having difficulty ac-cessing or financing health care services for theirCSHCN. The parent advocate also worked closelyone-on-one with each parent they came in contactwith to provide individual counseling and referral toother needed resources. Counseling services pro-vided by parent coordinators included counselingfamilies on their coverage options from a variety offinancing resources, helping them with eligibility strat-egies and the application process, helping to resolvecoordination of benefits problems between privateHMO coverage and Medicaid, and dealing with de-nials of referral and therapy requests.
Technical support on complicated case issuesand questions was provided to the parent advocatesby the health benefits counselor and the project at-torney. The parent advocate was able to call withquestions and get guidance on how to proceed witha case, or if it was appropriate to refer the case tothe counselor for staffing with an attorney if it lookedlike a representation or legal issue faced the familythe parent advocate was working with. Some casesremained with the parent advocate, and some caseswere moved to other resources for case resolution.
Legal servicesThe importance of a link to legal services for a healthbenefits counselor or a parent advocate should notbe underestimated. The law has the potential to bethe great equalizer between the enormous powerand leverage possessed by large insurers or gov-ernment agencies. More importantly the mere pres-ence of lawyers working with your program is not anindication that all interactions with other organiza-tions will be adversarial and confrontational. Whatit will mean is that the discussions, negotiations andstrategies developed will be done within the shadowof the law. Indeed the presence of a lawyer canhave a stabilizing effect on the process of resolving

MANAGED ADVOCACY IN ACTION Families MAP and Health Benefits Counseling: The Blueprint in Action • 31
a payment or eligibility dispute for a family. In factmost disputes (over 99%) for families were resolvedwithout going to court.
The link to legal services that are part of a Man-aged Advocacy Program must be affordable for fami-lies. Many families are too poor to hire privatecounsel, but even if they could afford it, they wouldhave a hard time finding a private lawyer willing totake a case involving a health insurance claim dis-pute or medical debt. We typically found that fami-lies with medical debt can find counsel to assist inbankruptcy proceedings more easily than they canlocate an attorney to provide the legal counsel andrepresentation on health care coverage issues thatMAP provided. Consumer health care coverage lawis a specialization rarely practiced by attorneys work-ing in consumer bankruptcy or poverty law, perhapsbecause the interface of state and federal rules gov-erning eligibility and billing of public programs is com-plex, and because many cases involve relativelysmall sums of money and statutory attorney feesare not generally available Additionally, those whoqualify financially for a Legal Services Corporationattorney might not obtain assistance for a case in-volving private health coverage because few if anyLegal Services or Volunteer Lawyer programs offercounsel in private pay or mixed private and publiccoverage program disputes.
As a part of Families MAP legal services wereprovided for Families and CSHN on the followingissues: private health insurance disputes and deni-als of coverage based on preexisting conditionclauses, medical necessity, and usual and custom-ary costs, in both state regulated and federally regu-lated ERISA plans; COBRA continuation andconversion; denials of service from HMOs in bothprivate and MA/HMO plans; health insurance mar-keting; eligibility for or access to services under child-hood disability programs such as SSI and the KatieBeckett Program; and multiple private and publichealth financing streams for a single insured.
� consultation and advice by telephone or inperson;
� case investigation (fact finding and gather-ing financial, medical or insurance informa-tion or documents);
� referrals to the private bar, pro bono attor-neys, and other agencies;
� negotiations with insurance companies,HMOs, collection agencies and health careproviders;
� filing complaints with the Commissioner ofInsurance and monitoring actions taken bythe Commissioner to ensure proper redressfor clients;
� representation at administrative hearings,before the State Claims Board, in state andfederal court; and
� appellate review.
Families are also less able to withstand themedical debt that arises when insurance claims orMedicaid benefits are denied. The target populationsfor ABC’s legal services have ongoing medical billsthat rapidly become credit (and legal) problems.Chronic illness, very expensive health insurance andmedical expenses not covered by their policies areall obstacles to needed health care. Families areespecially vulnerable to serious credit problems as-sociated with catastrophic illness. Furthermore, manyfamilies already struggling with the psychosocialneeds of a seriously ill family member may accumu-late unnecessary medical debt due to coordinationof benefit problems. They are frequently harassedfor payment by unscrupulous collection agencies thatviolate state and federal law.
Using Casework to Create Changein Families MAP
Providing legal services allowed the lawyers withFamilies MAP to identify and frame many of the largerissues and frustration faced by families in a legalcontext. Not only did the attorneys use the law andthe experience of past court battles and decision to

32 • Families MAP and Health Benefits Counseling: The Blueprint in Action MANAGED ADVOCACY IN ACTION
help assert the rights of families, they also kept aneye to the future to the new legal and advocacy path-ways that needed to be created to address emerg-ing health care coverage and access concern forfamilies. As with health benefits counseling, the in-dividual casework conducted by lawyers was animportant vehicle for education and system change.
Case Study—Home care denial
Sally Smith, a single parent, has a 6-year-oldmedically involved daughter named Emma.Emma has a neurological disorder that requiresprivate duty nursing services 24 hours a day.Sally has two other children, an older son, John,who is 14 and starting his first year of highschool and Tim, a 3-year-old who recently wasdiagnosed with Attention Deficit Disorder. Sallyhas taken care of Emma at home since shewas released from the Neonatal Intensive CareUnit when she was about three months old. Re-cently, Sally received a notice from the statethat private duty nursing hours would be re-duced from 24 hours a day to 16 hours a day.The rationale for the reduction in nursing hourswas that Sally, as a parent, is required to pro-vide certain cares to her child and is availableto provide cares. Sally has learned many of theprocedures and services required by Emma,since there are times when there may be ashortage of nurses or a nurse fails to show upfor a shift. Although Sally is capable of provid-ing the services, she is not comfortable sinceshe is not trained as a nurse, nor does she havethe time to take over a nursing shift since sheneeds to work full-time as well as meet theneeds of her other children. Sally contacted theattorney at an advocacy organization who in-tervened and filed a suit in court claiming thatthe State had developed no criteria to identifysituations where parents should be required toprovide these types of care for their children,nor did the State define circumstance in whichthe other care needs of family members as well
as needs of the mother are taken into consid-eration. The court reversed the State’s decisionand the judge indicated that the State was, inessence, punishing the mother for being a goodmother and learning to provide the cares, butthen expecting her to take over the role of atrained nurse. Twenty-four hour care was rein-stated for Emma.
This example demonstrates how active and in-volved parents can get caught and penalized by theState’s drive for cost containment. The state is in-terested in curbing redundant or not medically nec-essary expenses. As they examine costs to cut,high-ticket items like private duty nursing are closelyscrutinized. Here the state crossed the line whenthey failed to look at the situation from a family cen-tered perspective. By failing to account for themother’s other activities and other children, the stateput forward an argument that was seeminglygrounded in common sense. Parents have a re-sponsibility to care for the needs if their children.But the state failed to look at the circumstances ofthis family and this mother to make an appropriateand legal determination of the care need of a medi-cally fragile child. The law helped to play a correct-ing influence on over zealous state determinationsand this decision was useful to advocates and fami-lies across the state.
Private insurers are also very interested in cut-ting unnecessary and what they consider to be ex-perimental or duplicative costs. The drive to cut costsfrom private insurance can boarder on fraud or badfaith, particulrly when some unscrupulous compa-nies use an illegitimate contract term to deny ben-efits. Phantom clauses can be inserted into policiesthat have little or no meaning. Like a scarecrow inthe field, what might look scary at first blush, is actu-ally harmless.

MANAGED ADVOCACY IN ACTION Families MAP and Health Benefits Counseling: The Blueprint in Action • 33
Case Study—Phantom clause
Tom and Rita Jorgenson have a 15-year-old sonnamed Isaac. Isaac was recently diagnosedwith a brainstem tumor that could not be oper-ated on. The family sought the care of a spe-cialist who had developed an innovative therapyto treat brainstem tumors The treatments thathad undergone Food and Drug Administrationtrials. The insurance company however, deniedcare for Isaac as not being covered due to itbeing experimental. The policy contained aclause that indicated any treatment or servicethat was not medically approved by the Ameri-can Medical Association would not be coveredunder the terms of the policy. The family con-tacted an attorney to review the denial, con-tacted the AMA, and discovered that the AMAis not in the position to approve or disprovecertain types of therapy—experimental or non-experimental treatments. The attorney receivedan affidavit from the general counsel at the AMAconfirming the position of the AMA and for-warded it to the insurance company to challengethe denial. After alerting the insurance companyof the fraudulent nature of the clause in theirpolicy, the matter was settled and the treatmentswere paid for by the insurance company.
The important lesson from the above exampleis that sometimes there may be language in an in-surance policy that is meaningless or makes nosense. In situations like this, a family should care-fully review the policy and contact an attorney if theyfind language that they don’t understand or that maybe placed in the policy only to deceive or confusethe policyholder.
Combining the ingredientsBenefits counseling combines the work of the healthbenefits counselor, parent advocate and staff attor-ney. The common element of all three positions isadvocacy on behalf of families. They are all advo-
cates, each with a unique set of skills or life experi-ence that when combine becomes a powerful forcefor families seeking health care coverage or access.
A benefits counseling program can find a homein many different places. Anyone who is interestedin advocating for others, specifically in the area ofhealth care financing and navigation can provide cli-ent services that serve to address these issues.
In a provider organization it could be a seniorstaff member of a financial services department, asocial worker, a discharge planner, or the personwho manages the charity care program. In a non-profit it could be anyone willing to become an experton health care financing and access issues
Good locations certainly include clinics andhospitals, public health departments, nonprofit ad-vocacy agencies serving health and social needs,and public interest law firms.
Getting startedWhether you are one person or there are a group ofpeople that have identified the health care accessand financing problems facing families that havechildren with special needs, you or that group ofpeople have the capacity to do something about it. Itmay mean taking time out of your day to work onthose issues with families, it may mean trying to in-tegrate this type of advocacy into your job descrip-tion.
Turn a problem into an advocacy issue. De-velop an issue that is important to you. Find otherswith similar concerns and learn everything you can.
Share hard-to-find information with otherparents and/or professionals. Some information re-lated to CSHN is hard to find or difficult to locate.The first step in becoming an effective advocate canbe putting together or learning about existing re-source lists. Developing personal relationships withCSHN staff, county agency, etc., will lay the ground-work for an organizational meeting to discuss sharedgoals.
Becoming a skilled health advocate largely de-pends on practice. It requires the willingness to learnas you go by taking on new cases and searching for

34 • Families MAP and Health Benefits Counseling: The Blueprint in Action MANAGED ADVOCACY IN ACTION
solutions, and eventually becoming skilled andknowledgeable about health care coverage, access,policy and advocacy.
There are many tools and resources a Healthadvocate will use to increase his or her ability to serveclients. In Wisconsin, HBC’s attended trainings spe-cific to health care financing programs sponsoredby the State Department of Health and Family Ser-vices. Federally funded legal service offices also puton trainings once a year on a variety of topics, in-cluding childhood disability programs under the So-cial Security Administration. Training programs fromother statewide and local community organizationson related health care coverage or health care re-lated programs were attended whenever the oppor-tunity presented itself.
Key tools for the advocate to have on hand areprogram and policy manuals and handbooks thatdescribe program rules and state regulations thatapply to health coverage and eligibility rules. In Wis-consin a HBC has a subscription to the MedicaidHandbook and receives the periodic updates thatkeep the handbook current with program rules. Wis-consin also puts out regular Operations Memos withupdates, clarifications, and changes to programrules. It is a valuable tool to keep current on upcom-ing MA Handbook and policy changes. Other valu-able resources every HBC has include the WisconsinAdministrative Code and Wisconsin State Statutes.Internet access is very important to be able to searchwebsites for information about government pro-grams, community based programs and state re-sources, and other electronic manuals for specificprogram information and rules related to CSHCN(e.g. Katie Beckett program, Healthcheck (EPSDT)program, Birth to 3, Medicaid Provider Handbook).Developing a resource with frequently used contactsand resources is an invaluable tool for any benefitscounselor to have (see appendix for a list of HealthCare Financing Resources).
The Final Steps
After you have identified your community needs andassembled the key components of a health benefitscounseling program you may want the answer to thethreshold question of how to fund a program. Clearlyhealth benefits counseling programs should befunded as a necessary service for families by thestate or Federal government. A similar program forseniors is funded statewide in Wisconsin throughState funds and Federal Older American Act funds.For Families, The Family Opportunity act holds prom-ise for advocacy resources. Other resources to tapinto include Medicaid administrative resources or out-reach dollars. Other funding may include case man-agement or care coordination benefits availablethrough EPSDT in your state. Finally, providers whohave a vested interest in getting medical servicespaid for may be willing to institute a program of healthbenefits counseling at their facility. That said theservice can be shown to more than pay for itself in aprovider setting. Our work has shown that a $10 in-vestment has the capacity to generate over $100 inthird party reimbursement after the first encounterwhen health benefits counseling is provided to aMCH population. This service has also been shownto be a great customer service as well as contribut-ing to better provider staff morale.
Our work in developing a families MAP programdocuments the compelling need to help familiesthrough the blizzard of red tape they encounter asthey seek care and service for their children. Healthbenefits counseling programs can provide just thehelp that a family needs. Now is the time for policymakers and agency leaders to step up to the plateto support the deliver of comprehensive health ben-efits counseling services that include support for bothparent advocates and links to legal services
Working with HealthWatchCommittees
Chapter Six
Concept of Health Watch
Everyday, in communities across Wisconsin, caringpeople strive to offer guidance, support and servicesto families who have children with special healthneeds who are struggling with the challenges of mul-tiple service needs and coverage programs. Parents,Birth to 3 coordinators, public health nurses, eco-nomic support workers, health care providers, schoolnurses and counselors, advocates, lawyers, andclergy – all are important stakeholders who help fami-lies wind their way through the health care coverageand financing maze.
However, many of the challenges that confrontfamilies and their children with special health needscannot be resolved by individuals working in isola-tion or even within a single agency or provider orga-nization. Only by coming together to identifyproblems and community resources can we reallyaddress system based barriers. Working together,people in communities across the state are able tocreate change. One way of pursuing systems changeis the development of HealthWatch committees.
The greatest strength of these coalitions is theirdiversity of voices and the ability of group membersto identify problems in their day-to-day interactionswith families. Coalitions such as these are a testa-ment to the power of local associations to find cre-ative solutions for local and statewide problems.
HealthWatch is an organizational effort intendedto stimulate development of sustainable local com-mittees focused on health care access and financ-ing issues for children with special health needs. AHealthWatch committee works to:
� Create a local forum for networking to re-solve local service issues and problems
� Identify systemic issues for policy change
� Provide community education events andresources
The HealthWatch concept first had its start in1989 when a diverse group of health care providers,representatives of community based organizationsand government policy makers met in Milwaukee todiscuss local, systemic issues that they encounteredthrough their work. In response to these local con-cerns, they organized a HealthWatch coalition. TheHealthWatch concept evolved as these individualslearned that by meeting regularly to advocate forfamilies in need of care, with a particular emphasison Medicaid managed care problems, they couldeffectively work together to resolve many of theseissues. The Milwaukee committee proved to be sucha successful model for collaborative issue spottingand problem solving that ABC for Health created asimilar committee in Dane County in 1996.
HealthWatch and Families MAP
Through Families MAP, ABC for Health worked tocreate CSHN focused HealthWatch subcommitteesin Milwaukee, Dane County and rural ChippewaCounty in 1998. Each of these pilot sites focused

36 • Working with HealthWatch Committees MANAGED ADVOCACY IN ACTION
their discussions on the specific barriers that fami-lies who have children with special health needs facein managed care. In Chippewa County, where noformal HealthWatch committee had existed previ-ously, a new committee was organized which had aspecific focus on children with special health needs.
During the years of 1999 through 2001,Wisconsin’s Title V Maternal and Child Health pro-gram and local public health departments conducteda variety of surveys of families who have childrenwith special health needs. These surveys furthersupported the compelling issues that were being dis-cussed in the HealthWatch committees. Two enor-mous barriers facing families were access to careand adequate information about services and re-sources. Parents specifically identified a need for amore coordinated system of identifying health re-sources and supports for their children and their fami-lies. And, as families’ needs were identified, it wasrecognized that there was no formal mechanism todocument and capture these needs statewide. Ad-ditionally, a systematic way of developing strategiesand action plans to address these identified concernsneeded to be formulated.
Each of the pilot sites was charged with form-ing a committee that would focus on identifying prob-lems and strategize solutions regarding health carecoverage and access for families of CSHN. Pilotshad wide latitude in the development of these com-mittees. Due to the unique demographics and otherfactors in each of the pilot locations, each Health-Watch committee developed quite differently fromone another and faced distinct challenges.
What follows is a synopsis of the HealthWatchdevelopment in each pilot site. Their unique charac-teristics are highlighted and reflect the fact thatHealthWatch committees adapt well to the particu-lar characteristics of their communities. You will learnmore about how these committees were formed,what the singular factors were in each location, thevarying evolutions of these committees and the les-sons that were learned at each site.
Experience by location
MilwaukeeAccording to 2000 census data, Milwaukee is a cityof nearly a million people. Twenty five percent areidentified as African American and 8.8 percent asLatino. Children are numbered at 27,626 and anestimated 20,426 families with children in the house-hold are living beneath the poverty level.
Community Advocates (CA) was the home forthe Milwaukee pilot project. CA is a 25-year-old com-munity-based organization whose mission is to workwith low income and destitute persons and familiesto gain and ensure access to programs and services.This mission is accomplished by staff and volunteersproviding self-advocacy, representation, gap-filling,and system advocacy services to all persons in need.CA also specializes in coalition building. Employeeswork out in the community with many other agen-cies and understand the needs of families. CA is con-veniently located in the middle of Milwaukee whereover the last 25 years they have earned a widespreadreputation for helping families get what they need. Aparent advocate was identified to staff the CSHNHealthWatch subcommittee.
Getting startedSince Milwaukee County had an existing, broad-based HealthWatch committee before Families MAP,the Milwaukee parent advocate called upon about60 current HealthWatch members to participate inthe CSHN subcommittee. These participants in-cluded representatives from four major MedicaidHMOs, parents/grandparents of CSHN, representa-tives of the Latino Health Organization, HmongAmerican Friendship society, the Black Health Coa-lition, W2 Job Centers, the Medicaid enrollment con-tractor, specialty hospitals and rehabilitation facilitiesserving CSHCN, Milwaukee Public Schools, childcare providers, assembly and state senate repre-sentatives, and other health care advocates.

MANAGED ADVOCACY IN ACTION Working with HealthWatch Committees • 37
Of the seventeen major ideas generated by theinitial meeting, the top three were the fragmentednature of state services, insufficient provision ofhealth care for families of children with disabilitiesand a need for more advocacy for families with spe-cial needs children with all levels of government. Ofthose three, fragmentation of services was priori-tized as the most profound problem: families—eventhose eminently eligible for services—were unsureof who to talk to and where to go. Even when theydid get to the right place, there were often waitinglists for receiving benefits. Compounding matterswere the large number of low-income families inMilwaukee coupled with county workers not fullyunderstanding eligibility criteria for families applyingfor state and federal health coverage programs.
Building capacityThe process of building the local HealthWatch sub-committee in a large urban county like Milwaukeewas fraught at time with fits and starts. The issuesthe subcommittee addressed at times strayed fromthe core issues of health care coverage and accessin managed care for CSHN. At times, attempts torefocus the mission of the committee caused dropsin participation and continuity of membership. Atother times, Milwaukee encountered difficulty inmaintaining the initial committee participants due to“turf” issues between the numerous provider agen-cies, and an atmosphere of protectiveness over cli-ents and families. This lead to a lack of informationsharing and few referrals for benefits counselingearly in the project. Ultimately a core group of sub-committee members emerged to refocus the agendaand make significant contributions in the form ofunique trainings and models of consumer participa-tion on managed care organization committees.
ActivitiesMilwaukee provided trainings on a variety of pro-grams, including Medicaid and BadgerCare, KatieBeckett eligibility, SSI, prior authorizations, commu-
nity resources, prescription drugs, the Medical Homemodel, a training on managed care and CSHN froma provider/parent, and a parent panel sensitivity train-ing for W2 workers. They were also involved in anorientation for committee members on the rules andlaws pertaining to their rights within certain programsand how to navigate through the system.
There were also opportunities for HealthWatchgroups to collaborate on advocacy issues. In fact,during a time period when budget cuts threatenedhealth coverage programs in Wisconsin, Dane andMilwaukee counties sent a joint letter to the Gover-nor supporting a proposal to allocate more fundingto BadgerCare. Later, during intense budget debates,the governor took Medicaid “off the table.”
Another issue involved the widespread practiceof balance billing Medicaid recipients for services.The coalitions sent a letter alerting the AttorneyGeneral and the Medicaid program about the wide-spread practice of illegal billing of Medicaid recipi-ents. The Division of Health Care Financing lateradopted new procedures to alert recipients of theirrights. These examples helped to demonstrate thepower of a collective and amplified voice of theHealthWatch model.
Lessons learnedPeople identified—even to the point of getting some-what off-track—everything that they felt negativelyaffected children with disabilities. With the numer-ous barriers that existed for Milwaukee’s low-incomepopulation, often single parent families; it was diffi-cult to reign in discussion to only those problemsrelated to managed care.
As mentioned earlier, many of the families thatworked with Community Advocates had more thanone major challenge to address. Not only did thesefamilies have children with special needs to get healthcare for, but they were also dealing with employ-ment, childcare, transportation and other issues. Thecombination of these challenges made it difficult tokeep some families at the table. The Milwaukee com-
38 • Working with HealthWatch Committees MANAGED ADVOCACY IN ACTION
mittee also realized firsthand how working with par-ents comes second to their taking care of their chil-dren when they become seriously ill.
For more information on the Milwaukee Health-Watch, contact Ken Germanson at Community Advo-cates, (414) 449-4767 or at [email protected].
Dane CountyDane County is home to Madison, the state’s capitolcity. The entire county has little less than half thepopulation of Milwaukee, at 410,719, and 51 per-cent of the population of the county resides in Madi-son. 106,531 of the total county population arechildren. Four percent of the residents are identifiedas African American, with 3.5 percent Asian and 3.4percent Latino. An estimated 3,611 families with chil-dren were under the poverty level.
Getting StartedDane County’s HealthWatch has been in existencesince 1996. Like Milwaukee, their focus is broaderthan just children with special needs (see appendixD for the mission statement for the South CentralWisconsin HealthWatch). However, also like Milwau-kee, the children with special needs subcommitteewas formed with participation of HealthWatch mem-bers.
An initial kickoff event was organized, at whichparticipants (ranging from state senate representa-tives to parents to HMO representatives to Depart-ment of Health and Family Service staff members)brainstormed a laundry list of issues they saw asbarriers facing families of CSHN in managed care.From this list, five basic task forces were formed—Internal Communication and Supportive Services,Uncovered Benefits, Prior Authorization and Refer-rals, Network of Providers, and Funding StreamCoordination
Building CapacityIn the beginning, meetings were held after work
hours to discuss the issues identified and brainstormsolutions to them. It didn’t take long to realize that
even though committee members cared about theissues, parents especially are very busy people, andmany were not able to participate regularly after workand school hours.
It also soon became apparent that when meet-ings were coupled with a training on a topic that couldactually assist parents and advocates in their day-to-day lives or work, participants were much morelikely to attend. Over time, meetings to discuss is-sues became less frequent and trainings on issuescommittee members identified took more promi-nence. These trainings became an integral part ofthe Families MAP community education program.
ActivitiesAs was just mentioned, Dane County provided sev-eral training events for local committee members.These topics included:
� Social Security and Disability
� Advocating with Your Provider
� Mental Health Laws
� Managed Care Contracts
� HMO Panel on Grievance Procedures andServices for CSHCN
� Prior Authorization Forum
� Getting Therapies Approved
� Managed Care Rights and Responsibilities
� Review of the Medicaid Contract
� Health Insurance Checkup
� Alternative Therapies
� Cultural Competency
In addition, a quarterly newsletter was sentstatewide, and included topics such as:
· Transitions
· Prior Authorization Basics (see Prior Authorization insert, appendix E)
· Parent Advocacy
· Methods for getting things covered

MANAGED ADVOCACY IN ACTION Working with HealthWatch Committees • 39
· Mental Health
· Medical Home
· Consumer Health Care Financing Updates
· State budget and local issues
Lessons learnedIt was difficult for this committee to take a countywidefocus. Since Madison is the geographic hub of thecounty, and since state legislators and other officialshave offices in Madison, there always seemed to bean overrepresentation of Madisonians at DaneCounty events. We found, however, that taking goodmeeting minutes, and posting these and agendason our web site, as well as highlighting training in-formation in a newsletter which was distributedwidely, were good techniques for informing thosewho were not able to attend meetings (see appen-dix F for a digest of some HealthWatch minutes).And hosting meetings over an extended lunch hourseemed to increase regular participation of commit-tee members.
For more information on the Dane CountyHealthWatch Committee, contact Bobby Peterson,ABC for Health, 608-261-6939 or email [email protected]
ChippewaChippewa County is located in rural northwesternWisconsin, about 90 miles east of St. Paul, Minne-sota. It has approximately 1/17 the population sizeof Milwaukee county, and 1/8 that of Dane, with55,195 people, 16,000 of which are children. Twopercent of the residents identified as African Ameri-can, 9% as Asian and 5% as Latino.
Getting StartedUnlike Milwaukee and Dane counties, ChippewaCounty did not have an existing HealthWatch com-mittee from which to form a CSHN-focused sub-com-mittee. Due to their more rural location and smaller
number of potential committee members, they de-termined it was best to have one HealthWatch com-mittee with an emphasis on CSHN.
At one of the first meetings, the sub-groupseach identified four main issues to work on. Findingthe issues in common, they found speakers for eachof the issues.
They were initially unsure whom to invite to themeetings. Getting all of the agencies together (in-cluding parents of CSHN, nurses, county social ser-vices and Medicaid enrollment staff, HMOrepresentatives, private health care providers andvendors, school parent facilitators, Head Start andKatie Beckett Program staff, health care access ad-vocates, and members of the faith community) wasmuch needed in that community. After the initialmeeting, a series of smaller forums were held whichattracted many of these people.
Building CapacityThe Chippewa committee determined that havingonly professional speakers wasn’t the best idea. Atmeetings, they would ask participants to voice anyissues that they were concerned about and who theywanted to hear from at particular meetings. Theybegan to incorporate parent stories as well. TheCommittee became very participant driven, as op-posed to chairperson driven.
ActivitiesBeing in a more rural location, the Chippewa com-mittee found that mental health access issues werethe biggest barrier. Responding to this, the Chippewacommittee formed a special sub committee to focusattention on the issue and develop community strat-egies to address the identified problems. They helda public forum on mental health issues, a seminaron the role of the HMO advocate, and a training onBadgerCare. Prior authorizations, SSI basics and ap-plication process, Social Security determination pro-cess were other training topics addressed.

40 • Working with HealthWatch Committees MANAGED ADVOCACY IN ACTION
Lessons learnedMembers of the committee worked hard to form posi-tive relationships with other agencies, particularlythose workers in economic support.
The committee invited people from variouschurches to participate, although only one represen-tative responded. Other organizations heard aboutHealthWatch from committee members. HMOs inparticular were very receptive. For them it was dualpurpose, they could both and give sort of “inside”information about the workings of a managed careplan. One benefit was that these representativescould often be approached right after the meetingby a number of concerned people. This informal net-working and problem solving can be one of the mostvaluable aspects of a HealthWatch committee.
For more information about the ChippewaCounty HealthWatch, contact Rose Marsh atChippewa County Department of Public Health at715-726-7908.
Funding Resources for HealthWatchCommittees
One of the biggest challenges in developing any newprogram is identifying a funding source. Developinga HealthWatch committee is no different. Althoughwe can point to less family stress, greater access tocare, better coordination of services and links to amedical home that offers less expensive care in thelong-run, it may be difficult to quantify short-termsavings to a healthcare system that is chronicallyshort of resources. Nevertheless, there are oppor-tunities to help initiate a HealthWatch committee inyour community with some resourcefulness, somecooperative community stakeholders, and supportfrom the state and federal Medicaid programs (seethe CSHN HealthWatch Toolkit on this Families MAPPublications CD for resources on starting a localHealthWatch).
Funding may be available from the state, TitleV program or from your county Medicaid office. Inaddition, you may have a local community founda-
tion that is interested in supporting collaborative ac-tivities to help build local infrastructure and support-ive services. The HealthWatch committee of FamiliesMAP fits this criterion nicely. Another opportunity maybe to use local dollars as match to help secure fed-eral Medicaid reimbursement. These resources maycome from outreach or part of the administrativedollars that go to support Medicaid programs. Byfostering local communication, problem solving andstrategies, this system can be improved to help thecost effective delivery of healthcare and supportiveservices that are embedded in the managed advo-cacy concept.
Local health departments have a very impor-tant role in assuring the health care access needsof their respective communities. There may be ex-isting meetings that a managed advocacy programagenda could be added onto to help focus on theneeds of families and children with special healthneeds. A good place to start may be by contactingyour local county health department director or evena member of your local county board to see if theycan help get a local HealthWatch coalition started.Forming the local coalition may be the importantstarting point to get the other attendant services de-veloped.
As you establish a HealthWatch committee inyour community, be sure to identify the high priorityareas that families need assistance with. These highprofile issues will help not only gather momentumand enthusiasm for your work, but will also gain theattention of funders as community priorities that arein need of local support. Keep building and strength-ening your local coalition to help ensure that youhave the broadest range of support and allies. Getletters of support and help communicate the needsof your community to make sure that your managedadvocacy program is well funded and serving theneeds of your community.

MANAGED ADVOCACY IN ACTION Working with HealthWatch Committees • 41
HealthWatch Committees andSystemic Policy Change Activities
The goals of the HealthWatch committees was notonly to educate parents, advocates and providers,but to facilitate communication among groups af-fected by managed care programs, identify areas ofconcern regarding access to health care services,participate in problem solving strategies and offerpolicy changes to make the managed care systemmore responsive to the needs of families of CSHN.The Committees worked to identify problems andattempt to collaborate with coalition members tosolve problems on a local level. The HealthWatchcommittees that were developed during FamiliesMAP planted the seeds for a larger movement on astatewide basis.
One of the strong points of the HealthWatchcommittees is that problems and issues were identi-fied from real life experiences. The committee mem-bers were able to participate in developing specificpolicy recommendations. Partnerships were devel-oped as parents and advocates worked along withpolicy makers as equal members on the Health-Watch committees. And, committee members wereinformed of existing mechanisms for officially pro-posing policy changes and were connected to otherrelated statewide advocacy initiatives.
A major activity the HealthWatch committeesgot involved in was drafting proposed changes tothe Medicaid contract between the state and MCOs.For a complete description of how to influence themanaged care contract in your state see appendixG, HMO/Medicaid Contract.
Hosting Events for PolicymakersAn important outcome of the HealthWatch commit-tees is to influence public policy. Therefore, localcoalitions should identify strategies to engage pub-lic policy leaders. There are a variety of ways to helpeducate public policy leaders. For example, busylegislators may not have time to attend specificHealthWatch meetings or events, but a staff repre-sentative from their office could become a regular
participant and important liaison to the legislator. Onestrategy to involve political leaders is to give theman opportunity to speak at your meeting or on a topicthat is important to them. As part of the process,there could be questions and answers that will pro-vide an opportunity for issues and concerns of theHealthWatch committee to be introduced and de-bated.
There are several important logistical consid-erations that need to be taken into account whenplanning to host a public policy event. For example,it may be a good idea to conduct an event near oreven at the State Capitol. This way, busy legislatorscan avoid losing precious time in travel. Anotherpossibility is to find when the legislators are in thehome district and schedule an event around theirvisit. Many legislators want to hear what the issuesare from local constituents and this can provide agood opportunity to provide important dialogue onissues of concern that the committee has identified.
Identifying the correct legislator to involve inyour work is also an important consideration. Obvi-ously, working with Families with Children with Spe-cial Health Care needs members of the Health orChildren and Families committee may be appropri-ate legislators to target. If your HealthWatch com-mittee is planning a broader town hall agenda for agroup of legislators and policymakers, make surethat your panel gets good information ahead of timeabout types of issues that will be addressed, howthe question and answer format will be developed.For example, at some forums the questions fromthe audience were submitted in advance to a mod-erator to avoid the chance that legislators might beembarrassed or sidetracked on other issues thatwere not germane to the issues and concerns of theHealthWatch committee. Setting up an appropriatestructure that gives the legislator a chance to air theirissues as well as to field important questions canhelp to establish credibility and trust with your Health-Watch coalition.
Remember, legislators are not the onlypolicymakers. Your coalition should also work to en-gage representatives from key agencies like the

42 • Working with HealthWatch Committees MANAGED ADVOCACY IN ACTION
State Medicaid Bureau, the Children with SpecialHealth Care Needs Program, Public Health offices,as well as major stakeholder from the provider andspecial education community. In summary, hostingpublic policy events can be a major way for advanc-ing the agenda developed by HealthWatch commit-tees. Only through open debate and dialogue andengaging the key decision makers will meaningfulchange occur in your community. By developing stra-tegic links to key policymakers, your HealthWatchgroup will not only grow stronger, but you will attractmore members as you advance an agenda for chil-dren with special health care needs in your commu-nity.
HealthWatch Committees andCommunity Education
A critical component of Families MAP was creatinga variety of training and public education opportuni-ties. Such activities are effective means of outreach,networking and providing an efficient way to extendthe information and case experience of health ben-efits counselors to a broader audience.
There are many ways to share your message.This depends on available resources and those ofthe HealthWatch committee. Some effective meansfor sharing information with other professionals andfamilies that Families MAP used are:
� Public events
� Trainings and public forums
� Presentations at local community meetings,professional meetings, workshops, andexhibits at health fairs.
� Information resources, including brochures,newsletters, publications, resource lists andagency website.
Public EventsFamilies MAP pilots created a variety of informationand training events for parents and providers basedon locally identified priorities. Topics offered includedtraining for health care provider staff and health pro-fessionals, parents and staff from community agen-cies who work with CSHN families. In addition,presentations at conferences and workshops weredone for families and the general public.
Topics were chosen as parents, providers andadvocates in the community identified barriers fami-lies were facing in getting health care. Speakers werefound with knowledge and expertise in those spe-cific topic areas. For example, parents said that theyhad difficulty in communicating with their child’s phy-sician. The project was fortunate to find a physicianin the community who was also a parent of a childwith special needs. This parent/doctor did a presen-tation on his perspective of being both a parent try-ing to communicate with his child’s doctor, and beingthe doctor on the other side with his patient and try-ing to effectively communicate with the families heworked with.
Another topic that Families MAP held trainingsessions on was the prior authorization process fortherapies. Again, a therapist who works with CSHNwas identified and agreed to make multiple presen-tations to both parent groups and other therapistson better ways to address their frustrations and con-cerns with the prior authorization process. At onetraining, the prior authorization review staff from theState of Wisconsin did a joint presentation with thistherapist on what helped prior authorization requestsbe approved and move through the evaluation pro-cess more quickly.
In relation to funding stream coordination, a fo-rum was held in which a legislator came to hear whatparents, providers, and school staff had to tell him inregards to the difficulty of getting the Medicaid pro-gram to pay for therapies outside of the school envi-ronment. This topic ended up being addressed atan additional training session as the legislator re-

MANAGED ADVOCACY IN ACTION Working with HealthWatch Committees • 43
quested the opportunity to learn more about thisproblem and how it could be remedied on a system-wide basis.
Once topics were chosen, and speakers hadbeen secured, it was necessary to publicize theevents and reach as large an audience as possible.Parents were not always able to attend events, sotopics were often covered in meetings and with fol-low-up fact sheets, website minutes and in newslet-ters.
PublicationsTo reach a larger audience, public education projectssuch as consumer-friendly resource manuals andbooklets and informational brochures were used. Allof these activities built visibility in the community whilealso providing significant, practical help for families.
The website made a number of the resourcesmore widely available, including the MAP Report, theproject newsletter, and a series of fact sheets onfinancing resources for families. A larger publication,The Health Insurance Guidebook, was published asa pdf included on this Families MAP CD, which made
linking to numerous other web resources a possibil-ity. A limited number of copies were also printed forfamilies who did not have easy computer access.
All community education projects tied back tothe health benefits counseling and policy efforts ofFamilies MAP.
Conclusion
HealthWatch coalitions are a vital part of an overallstrategy of managed advocacy. The coalitions notonly help to zero in on the public policy concernsrelating to coverage for CSHN and families but theyalso work to greatly amplify the issues. More impor-tantly community collaborations can result in strate-gic alliances that help inform the public andpolicymakers about health issues concerning kidsand families. Finally, the friendships you make aspart of a community coalition like HealthWatch areendearing. Don’t be surprised if the representativeof a managed care organization or a county workerthat you once viewed with suspicion or even angersoon becomes an important colleague…and maybeeven a friend.


Conclusion
Managed advocacy was conceived during a time ofrapid change in the health care delivery systems inWisconsin. Those changes continue today and willcontinue tomorrow as we as a society grapple withskyrocketing costs and the implications of restrict-ing individual choices about health care services. Assuch Managed Advocacy and the processes de-scribed in this monograph are continuing to evolve.In response to the changing environment of healthcare delivery, new structures of advocacy and sup-portive services for parents will need to continuallybe developed and fine-tuned. However, we believe,the framework of Managed advocacy in Action willprovide a flexible blueprint for years to come as oursystems of care and coverage for CSHCN evolve.
Now that you have reviewed the process andseen the blueprint of a Managed Advocacy Plan inAction you might be ready to take the next stepstoward building a program in your community. Whatare the next steps? Begin to ask the questions inyour community to see if the mood is right for theestablishment of Managed Advocacy. Rememberthat the model is designed to be collaborative andnot adversarial. There will be pitfalls along the way
and you may be greeted with suspicion and looks ofpuzzlement. Broken fences may need to be mendedas you assemble key stakeholders and parents. Theinclusion of advocates and lawyers working withparents was not meant to be provocative, but ratherwas an attempt t level the playing field between fami-lies and the large bureaucracies and institutions serv-ing them. On an equal plateau, families, advocatesand providers all working toward a common goal:improving the systems of care and coverage forChildren with special health care needs.
The development of a managed advocacy pro-gram is not a simple proposition. In fact assemblingthe pieces to build a program will take hard work,creativity and most of all passion. However onceyou begin the process it may be impossible to turnback the clock. Moreover, the combination of advo-cacy, parent involvement and links to key commu-nity stakeholders can have a catalytic effect in yourcommunity to promote significant and lasting changeto the attitudes and philosophy of the providers andthe bureaucracies that are established to help andsupport families and CSHN.
Chapter Seven


Wisconsin Services andPrograms
Appendix A
Wisconsin Public Coverage andServices
Wisconsin Medicaid ProgramsWisconsin families eligible for Medicaid coveragemust, whenever possible, enroll in one of the Medic-aid HMOs currently serving the state. Enrollmentoptions vary with zip code, ranging from a singleHMO in an area up to three from which to choose.Exemptions allow those children with an SSI disabilitydetermination to opt out of an HMO, and choose fee-for-service coverage.
A fee-for-service Medicaid card allows moreflexibility in seeking care from a wide range of phy-sicians and providers, as long as those providersaccept Medicaid. This flexibility is especially impor-tant for CSHCN who may need to see a variety ofspecialists to treat their specific diagnosis.
Wisconsin provides comprehensive coveragefor all but one of its Medicaid programs (Healthy StartPresumptive Eligibility for pregnant women). Thestate has also chosen to allow families and childrento become Medicaid eligible through optional Med-icaid programs such as the Medical Assistance De-ductible program and the Family Fiscal Unit (FFU).These two strategies were very helpful to CSHCNfamilies who had large medical expenses or wereseeking coverage for one specific person in thehousehold. The Medicaid deductible allows familieswith excess income to use their outstanding medi-cal debt to offset their income that is above the eligi-bility guidelines for Medicaid. The FFU allow thecalculation of individual eligibility if a person in theapplicant family meets specific program criteria.
BadgerCare: This is Wisconsin’s SCHIP program.It provides low-cost or free family Medicaid cover-age to low- to moderate-income families with chil-dren under age nineteen who do not have accessto, or coverage by, a private health insurance plan.The income guidelines are 185% FPL. BadgerCarecovers children under the age of nineteen and thenatural, adoptive, or step- parent(s) who reside withthem. It does not cover non-legally responsible rela-tive caregivers such as grandparents, aunts anduncles, etc.
Healthy Start: Pregnant women, infants, and chil-dren under the age of six are eligible for HealthyStart. An applicant’s family income must be under185% of the federal poverty level (FPL).
Healthy Start OBRA: For children ages six to nine-teen the income eligibility guidelines are 100 % FPL,much lower than for Healthy Start or BadgerCare.
Katie Beckett: Allows certain children with long termdisabilities or complex medical needs, living at homewith their families, to receive a Wisconsin Medicaidcard. Children under age nineteen who are not eli-gible for other Medicaid programs because the in-come or assets of their parents are too high, may beeligible for Medicaid through the Katie Beckett Pro-gram if they are determined to be disabled by So-cial Security standards; require a level of care athome that is typically provided in a hospital or nurs-ing facility; can be provided safe and appropriatecare in the family home; as an individual, do not have
48 • Wisconsin Services and Programs MANAGED ADVOCACY IN ACTION
income that exceeds program guidelines, or assetsin excess of $2000; do not incur a cost of care athome to the Medicaid Program that exceeds the costMA would pay if the child were in an institution.
CIP IA/CIP IB/ CIP II/COP W: To enable personswho might enter nursing homes, intermediate carefacilities, or the state centers for the developmen-tally disabled to live at home or in a variety of com-munity settings such as group homes.
Community Options Program (COP): This pro-gram enables persons who live at home or in anycommunity setting, such as a group home, readyaccess to generic community resources. Flexiblefunding to meet a variety of needs such as respite,adaptive home modifications, vehicle transportationmodifications, etc.
CSHCN Program (MCH Title V Block Grant pro-gram): Manages five regional centers and Wiscon-sin First Step Hotline. The regional centers werelaunced in 2000 to provide information, referral andfollow-up services to families that have children withchronic illnesses or physical disabilities. They pro-mote parent-to-parent support networks and localprovider networking for service coordination.
Birth to 3: For parents with a child under three yearsof age who are concerned about the way their babyis developing, this program offers early interventionservices; information and referral; development of aplan of services; assistance to find funding for ser-vices. This program coordinates developmental,health, and social services within the local commu-nity in a comprehensive fashion that recognizes theimportance of parents, family and friends in a youngchild’s life. Families transition out of Birth to 3 whentheir child turns four and becomes eligible for evalu-ation for school district services.
Family Support Program: To provide support to thefamily to enable the family to care for a severely dis-abled child at home. Support includes the services
of a Family Support Program Coordinator who canhelp families identify and obtain needed services andresources and link families together, and funding (upto $3,000 per year) to purchase goods and servicesnot available through other programs.
Health Insurance Risk Sharing Plan: State spon-sored pool that provides insurance coverage to high-risk persons with chronic or disabling conditions whodo not qualify for Medical Assistance or Social Se-curity disability, and who cannot purchase coveragethrough any other alternative insurance plan.
Supplement Security Income(SSI): A cash assis-tance program that is run by the Social Security Ad-ministration for children who are disabled and forwhom their household income is low enough toqualify for the monthly cash benefit. A child who re-ceives an SSI check, automatically is eligible forMedical Assistance coverage.
Managed Care Plans in Wisconsin
There are 21 health maintenance organizations op-erating in Wisconsin, thirteen of which provide man-aged care services through Medicaid HMO contractswith the state. See appendix G for information onparticipating in a review of the state Medicaid HMOcontract.
Local School Districts Services
School districts offer a variety of services for CSHCN.However, the number and type of service varies de-pending on the size of the school district. Examplesof some services available through the school arecomprehensive education needs assessment (IEP),physical therapy, occupational therapy, speechtherapy, and tutoring. These services are bases oneducational needs and goal, not community needs.
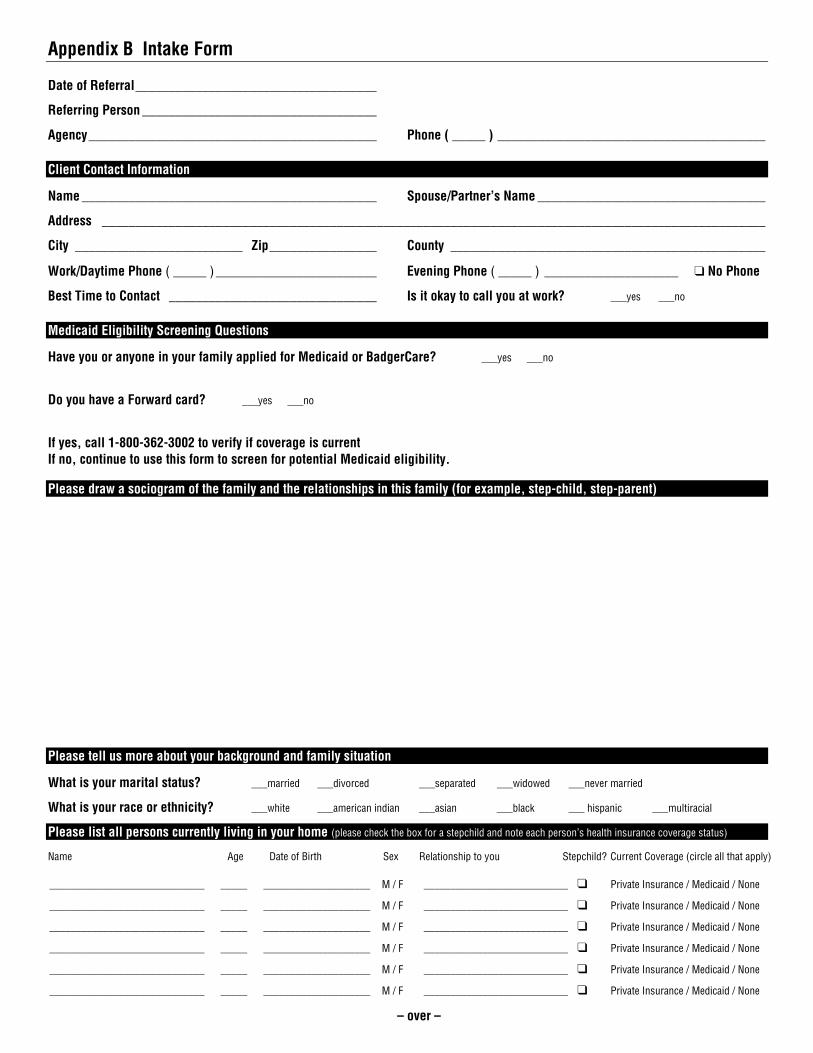
Appendix B Intake Form
Date of Referral____________________________________
Referring Person ___________________________________
Agency___________________________________________ Phone ( _____ ) ________________________________________
Client Contact Information
Name ____________________________________________ Spouse/Partner’s Name __________________________________
Address ___________________________________________________________________________________________________
City _________________________ Zip________________ County _______________________________________________
Work/Daytime Phone ( _____ ) ________________________ Evening Phone ( _____ ) ____________________ ❑ No Phone
Best Time to Contact _______________________________ Is it okay to call you at work? ___yes ___no
Medicaid Eligibility Screening Questions
Have you or anyone in your family applied for Medicaid or BadgerCare? ___yes ___no Do you have a Forward card? ___yes ___no If yes, call 1-800-362-3002 to verify if coverage is current If no, continue to use this form to screen for potential Medicaid eligibility. Please draw a sociogram of the family and the relationships in this family (for example, step-child, step-parent) Please tell us more about your background and family situation
What is your marital status? ___married ___divorced ___separated ___widowed ___never married
What is your race or ethnicity? ___white ___american indian ___asian ___black ___ hispanic ___multiracial
Please list all persons currently living in your home (please check the box for a stepchild and note each person’s health insurance coverage status)
Name Age Date of Birth Sex Relationship to you Stepchild? Current Coverage (circle all that apply)
_____________________________ _____ ____________________ M / F ___________________________ ❑ Private Insurance / Medicaid / None
_____________________________ _____ ____________________ M / F ___________________________ ❑ Private Insurance / Medicaid / None
_____________________________ _____ ____________________ M / F ___________________________ ❑ Private Insurance / Medicaid / None
_____________________________ _____ ____________________ M / F ___________________________ ❑ Private Insurance / Medicaid / None
_____________________________ _____ ____________________ M / F ___________________________ ❑ Private Insurance / Medicaid / None
_____________________________ _____ ____________________ M / F ___________________________ ❑ Private Insurance / Medicaid / None
– over –
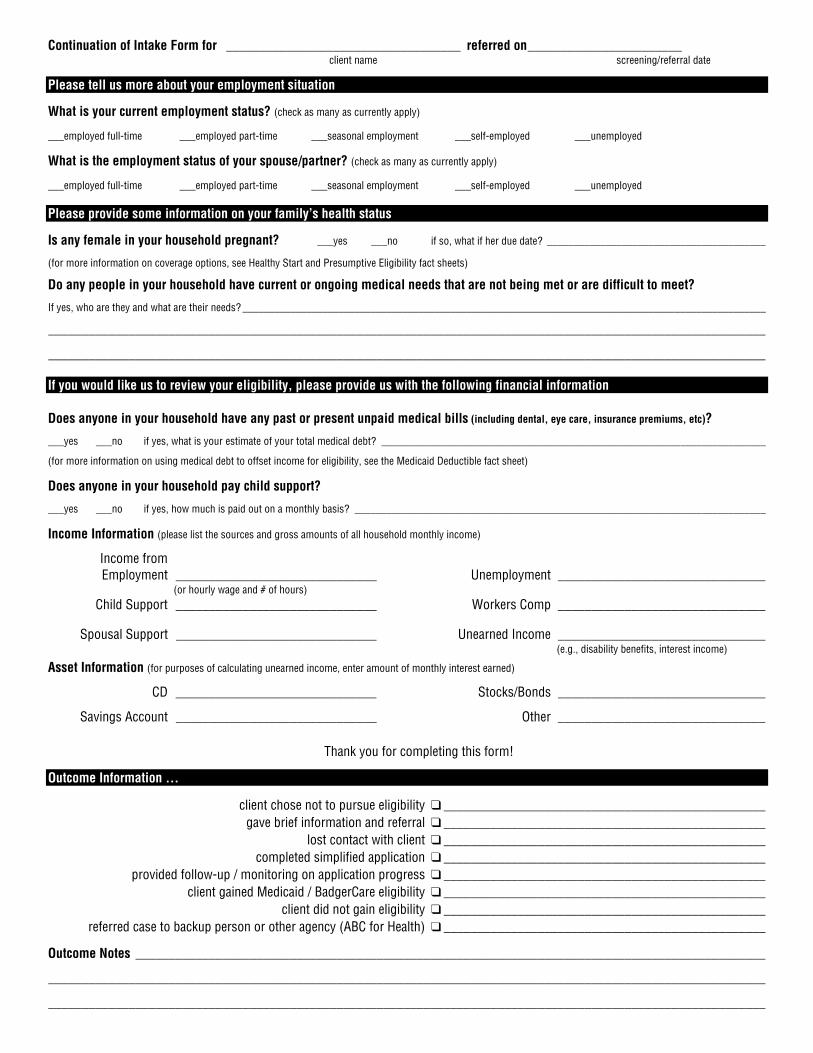
Continuation of Intake Form for ___________________________________ referred on_______________________ client name screening/referral date
Please tell us more about your employment situation
What is your current employment status? (check as many as currently apply)
___employed full-time ___employed part-time ___seasonal employment ___self-employed ___unemployed
What is the employment status of your spouse/partner? (check as many as currently apply)
___employed full-time ___employed part-time ___seasonal employment ___self-employed ___unemployed Please provide some information on your family’s health status
Is any female in your household pregnant? ___yes ___no if so, what if her due date? _________________________________________
(for more information on coverage options, see Healthy Start and Presumptive Eligibility fact sheets)
Do any people in your household have current or ongoing medical needs that are not being met or are difficult to meet?
If yes, who are they and what are their needs? __________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
If you would like us to review your eligibility, please provide us with the following financial information Does anyone in your household have any past or present unpaid medical bills (including dental, eye care, insurance premiums, etc)?
___yes ___no if yes, what is your estimate of your total medical debt? ________________________________________________________________________
(for more information on using medical debt to offset income for eligibility, see the Medicaid Deductible fact sheet)
Does anyone in your household pay child support?
___yes ___no if yes, how much is paid out on a monthly basis? _____________________________________________________________________________
Income Information (please list the sources and gross amounts of all household monthly income)
Income from Employment ______________________________ (or hourly wage and # of hours) Child Support ______________________________ Spousal Support ______________________________
Unemployment _______________________________ Workers Comp _______________________________ Unearned Income _______________________________ (e.g., disability benefits, interest income)
Asset Information (for purposes of calculating unearned income, enter amount of monthly interest earned)
CD ______________________________ Stocks/Bonds _______________________________
Savings Account ______________________________ Other _______________________________
Thank you for completing this form!
Outcome Information …
client chose not to pursue eligibility ❑ ________________________________________________ gave brief information and referral ❑ ________________________________________________ lost contact with client ❑ ________________________________________________ completed simplified application ❑ ________________________________________________ provided follow-up / monitoring on application progress ❑ ________________________________________________ client gained Medicaid / BadgerCare eligibility ❑ ________________________________________________ client did not gain eligibility ❑ ________________________________________________ referred case to backup person or other agency (ABC for Health) ❑ ________________________________________________
Outcome Notes ______________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Health Care FinancingResources
ABC for HealthDescription: statewide benefits counseling and legalservices for families with children who are having problemsfinancing health careContact Info: 1-800-585-4222 or 608-261-6939 [email protected] Address: http://www.abcforhealth.org
Adoption AssistanceDescription: financial support and health insurance for pre-adopted children with special needsContact Info: adoption agency or 608-266-0690
AIDS/HIV+ Drug Reimbursement ProgramDescription: pharmaceuticals for people with AIDSContact Info: [email protected] Address: http://www.dhfs.state.wi.us/aids-hiv/Re-sources/Overviews/AIDS_HIV_drug_reim.htm
AIDS/HIV+ Health Insurance AssistanceDescription: health insurance premiums paid for peoplewith AIDSContact Info: 1-800-991-5532 [email protected]
Web Address: http://www.dhfs.state.wi.us/aids-hiv/Re-sources/Overviews/AIDS_HIV_hlth_ins.htm
Air Life LineDescription: air transport in private planesContact Info: [email protected] Address: http://www.airlifeline.org
American Legion Temporary FinancialAssistanceDescription: financial funding for healthcare, rent, and anyother of children of legion members needsContact Info: 1-800-322-0838; [email protected] Web Address: http://www.legion.org/membership/memdisc2.htm
BadgerCareDescription: state sponsored low cost health insurance forfamilies with childrenContact Info: county social servicesrecipient services: 1-800-362-3002Web Address: http://www.dhfs.state.wi.us/badgercare/index.htm
Betaseron FoundationDescription: makes betaseron available to MS patientsContact Info: 1-800-948-5777Web Address: http://www.betaseronfoundation.org
Birth to 3Description: a variety of services for children with specialhealth care needs under age 3Contact Info: [email protected] Address: http://www.dhfs.state.wi.us/bdds/b3.htm
Birth to Three DirectoryDescription: directory of county contactsWeb Address: http://www.dhfs.state.wi.us/bdds/b3dir/b3dir.htm
Appendix C

52 • Health Care Financing Resources MANAGED ADVOCACY IN ACTION
Bureau for the BlindDescription: independent living servicesContact Info: 1-888-879-0017 or 608-266-3109Web Address: http://www.dhfs.state.wi.us/aboutDHFS/DSL/Guide/DSLbureaus.htm
Bureau for the Deaf and Hard of HearingDescription: independent living servicesContact Info: 1-800-947-6644Web Address: http://www.dhfs.state.wi.us/aboutDHFS/DSL/Guide/DSLbureaus.htm
Car Insurance - MedicalDescription: auto insurance policy
Center for Independent LivingDescription: adaptive aids and equipmentContact Info: 1-800-690-6665
Child Care Payment AssistanceDescription: payment of child care for low-incomeworking parentsContact Info: county social services
Children’s Craniofacial AssociationDescription: travel costs associated with surgery; adultsincludedContact Info: 1-800-535-3643Web Address: http://www.ccakids.com
Children’s Miracle NetworkDescription: assistive devices on a case-by-case basisContact Info: 1-800-428-5000Web Address: http://www.cmnwi.org
Chronic Disease ProgramDescription: financial funding for kidney disease, cysticfibrosis, and hemophilia needsContact Info: 608-221-3701
Church FundsContact Info: your church
College Health InsuranceContact Info: your college
Community Action AgencyDescription: limited housing modernization and rentassistanceContact Info: 608-244-4422
Community Health Centers DirectoryDescription: medical services on a sliding fee scaleContact Info: 608-277-7477Web Address: http://www.bphc.hrsa.gov/databases/fqhchttp://www.wphca.org/org.htmlhttp://www.wphca.org/affiliate.html
Community Options Program (COP)Description: a variety of services for persons withdisabilitiesContact Info: check statewide directoriesWeb Address: http://www.dhfs.state.wi.us/LTC_COP/cop.htm
Community Options Program DirectoryDescription: directory of county and tribal contactsWeb Address: http://www.dhfs.state.wi.us/LTC_COP/contacts.htm
Comparison Shop for Health Care CostsDescription: substantial cost differences do existContact Info: provider’s office
County Social / Human ServicesDescription: directory of county social / human servicesofficesContact Info: county social servicesWeb Address: http://www.dhfs.state.wi.us/Medicaid1/contacts/medcontact2.htm
Crime Victims Compensation ProgramDescription: payment of crime-related required servicesnot covered by insuranceContact Info: [email protected] Address: http://www.doj.state.wi.us/cvs/programs/cvc.asp
Cystic Fibrosis CenterDescription: general information and referral to localhealth care centers for care and financingContact Info: 1-800-344-4823;608-263-8555
MANAGED ADVOCACY IN ACTION Health Care Financing Resources • 53
Disabled Children’s Relief FundDescription: provides grants for assistive devices andrehabilitative servicesContact Info: 516-377-1605Web Address: http://www.dcrf.com
Division of Supportive LivingDescription: a variety of independent living servicesContact Info: 608-266-5383Web Address: http://www.dhfs.state.wi.us/aboutDHFS/DSL/dsl.htm
Division of Vocational RehabilitationDescription: a variety of employment-related healthservicesContact Info: 608-243-5600Web Address: http://www.dwd.state.wi.us/dvr
Early Intervention (Birth to Three)Description: a variety of services for children with specialneeds under age 3Contact Info: [email protected] Address: http://www.dhfs.state.wi.us/bdds/b3.htm
Earned Income Tax CreditContact Info: 608-266-8100 or tax preparerElder Law CenterDescription: benefits counseling and legal assistance forthe elderly on a broad range of issues, including healthcareContact Info: 608-224-0660 or 1-800-366-2990
Energy AssistanceDescription: cash toward heating billsContact Info: county social services
Family Health Center Insurance PlanDescription: sliding fee scale health insurance throughMarshfield Clinic for residents of certain counties inCentral WisconsinContact Info: 1-800-942-5420
Family Support ProgramDescription: a variety of services for children with specialneedsContact Info: county social serviceWeb Address: http://www.dhfs.state.wi.us/bdds/fsp.htm
First Star BankDescription: a variety of itemsContact Info: 608-257-3764; 1-800-538-0838
Food StampsDescription: vouchers for groceriesContact Info: county social services
Foster ChildrenDescription: health insurance for children in foster careContact Info: county social services
General assistance or General Relief-MedicalDescription: limited medical care and other servicesContact Info: county social services
Health Insurance Risk Sharing Plan (HIRSP)Description: high risk health insuranceContact Info: 1-800-828-4777; 608-221-4551Web Address: http://www.dhfs.state.wi.us/hirsp
HealthCheckDescription: sealants and orthodontia servicesContact Info: local clinic / public health; 1-800-722-2295
HealthCheck Other ServicesDescription: Medicaid non-covered servicesContact Info: local clinic / public health
Healthy StartDescription: health insurance for pregnant women andchildren under 6Contact Info: county social services; 1-800-722-2295Web Address: http://www.dhfs.state.wi.us/medicaid1/recpubs/factsheets/healthy_start.htm
Hear NowDescription: hearing aids and cochlear implantsContact Info: 1-800-648-HEAR
54 • Health Care Financing Resources MANAGED ADVOCACY IN ACTION
HIKEDescription: hearing needs for children and schoolsContact Info: 608-847-4194; 262-896-0643
Hill Burton HospitalsDescription: hospitalizationContact Info: 1-800-638-0742
Homestead Tax CreditDescription: low income singles and families renters andhomeowners tax refundContact Info: 608-266-8641Web Address: http://www.dor.state.wi.us/ra/hmst02.html
Hospital Charity CareDescription: hospitalizationContact Info: Local hospital
Indigent Drug ProgramsDescription: certain drugs free through pharmaceuticalcompaniesContact Info: 1-800-PMA-INFOWeb Address: http://www.edhayes.com/indigent.html
JudicareDescription: legal services agency for Northern Wiscon-sinContact Info: 1-800-472-1638 or [email protected] Address: http://www.judicare.org
Katie Beckett ProgramDescription: health insurance for disabled children underage 19 living at homeContact Info: 608-266-3236Web Address: http://www.dhfs.state.wi.us/bdds/kbp.htm
Knights of ColumbusDescription: offers long-term insurance for nursinghomes and home healthcare for Knights of ColumbusmembersContact Info: local Catholic churchWeb Address: http://www.kofc.org
Knights Templar Eye FoundationDescription: vision needsContact Info: [email protected] Address: http://www.knightstemplar.org/ktef
Knights Templar Hearing FoundationDescription: hearing needsContact Info: 414-965-2200; 1-800-242-2307
Legal Action of WisconsinDescription: legal services agency with offices inKenosha, Madison and MilwaukeeContact Info: [email protected] Address: http://www.legalaction.org
Legal Services of Northeastern WisconsinDescription: legal services agency with offices in GreenBay, Oshkosh and SheboyganContact Info: 920-432-4645 or 1-800-236-1127Web Address: http://www.lsnew.org
Lion’s ClubDescription: vision and hearing needsContact Info: local clubWeb Address: http://www.lionsclub.org
Local service groupsDescription: assistance on case by case basisContact Info: local community
Locks of LoveDescription: free wigs for childrenContact Info: [email protected] Address: http://www.locksoflove.com
Low Income Rental HousingContact Info: 1-800-334-6873 or 608-267-9077
Lutheran Bishops FundDescription: assistance on case by case basisContact Info: local Lutheran pastor
Lutheran Social ServicesDescription: counseling on a sliding fee scale
MANAGED ADVOCACY IN ACTION Health Care Financing Resources • 55
Contact Info: 414-281-4400Web Address: http://www.lsswis.org
Magic FoundationDescription: funding for growth hormones, educationContact Info: 1-800-362-4423; [email protected] Address: http://www.magicfoundation.org
MedicaidDescription: health Insurance for low-income familieswith childrenContact Info: 1-800-362-3002Web Address: http://www.dhfs.state.wi.us/medicaid/index.htm
Medically NeedyDescription: health insurance for disabled or blindchildren and adults, adults over age 65 or for childrenage 6 to 19Contact Info: County social services
MedicareDescription: federally sponsored health insurance forblind or disabled adults over 18, or adults over age 65Contact Info: Social Security office or 1-800-MEDICAREWeb Address: http://www.medicare.gov
Miracle Ear Children’s FoundationDescription: hearing aids for school-age childrenContact Info: 1-800-234-5422Web Address: http://www.miracle-ear.com/services/children_request.asp
Miracle Flights for KidsDescription: volunteer pilots fly children to hospitalsContact Info: 1-800-359-1711; [email protected] Address: http://www.miracleflights.com
Muscular Dystrophy AssociationDescription: services related to muscular dystrophyContact Info: 414-453-7600Web Address: http://www.mdausa.org
National Children’s Cancer SocietyDescription: transportation, housing, and assistance on acase-by-case basisContact Info: 1-800-532-6459Web Address: http://www.children-cancer.org
National Easter Seal SocietyDescription: camps, equipment,etcContact Info: 608-277-8288; [email protected] Address: http://www.wi-easterseals.org
National Eye Care ProjectDescription: eye care for people age 65+ (eyeglasses notincluded)Contact Info: 1-800-222-3937
National Patient Air Transport HelplineDescription: free or reduced rates for air travelContact Info: 1-800-296-1217Web Address: http://www.patienttravel.org
New Eyes for the NeedyDescription: eyeglasses onlyContact Info: 973-376-4903
Office for the BlindDescription: independent living servicesContact Info: 608-243-5656
Office of the Deaf and Hard of HearingDescription: independent living servicesContact Info: 608-243-5625
Parent’s Health Insurance for Post-Secondary StudentsContact Info: parent’s policy
Patient Advocate FoundationDescription: advocacy and legal referralContact Info: 1-800-532-5274
Planned ParenthoodDescription: male and female reproductive healthservices, education, sliding fee scaleContact Info: [email protected]
56 • Health Care Financing Resources MANAGED ADVOCACY IN ACTION
Web Address: http://www.plannedparenthood.com
Presumptive EligibilityDescription: immediate health insurance for pregnantwomenContact Info: local public health agency
Public Health AgencyDescription: home health care, mammograms, papsmears, immunizations, birth control, STD testingContact Info: Local Public Health DepartmentWeb Address: http://www.dhfs.state.wi.us/DPH_Ops/LHDL.HTM
Qualified Medicare Beneficiary ProgramDescription: Medicaid coverage for Medicare premiumsand copaysContact Info: county social service
Red CrossDescription: services for hemophilia and other bleedingdisorders and disaster reliefContact Info: 1-800-261-4182 or local [email protected] Address: http://www.redcross.org
Ronald McDonald HouseDescription: housing for parents of hospitalized childrenwith serious illnessesContact Info: 608-232-4660; 630-623-7048Web Address: http://www.rmhc.com
Salvation ArmyDescription: assistance on case by case basisContact Info: 1-800-378-7272 or local chapter; 608-256-2321Web Address: http://www.salvationarmy.org
School SystemDescription: therapy and educational necessities forstudents with special needsContact Info: Local school system
See AmericaDescription: provides assistance for eye surgeries andexamsContact Info: 1-800-208-6733
Web Address: http://www.seeintl.org/america.html
Short Term Disability InsuranceDescription: private insurance/policy through employer
Shriners HospitalsDescription: medical services for children with orthopedicproblems, burn injuries, or cleft palateContact Info: 1-888-293-2832Web Address: http://www.shrinershq.org/Hospitals
Sister Kinney InstituteDescription: rehabilitative services and therapyContact Info: 612-863-4457
Social Security Disability IncomeDescription: monthly income for disabled adultsContact Info: Social Security officeWeb Address: http://www.ssa.gov/disability/
Supplemental Security IncomeDescription: health insurance and cash payment fordisabled or blind children and adults, or adults over 65Contact Info: Social Security office; [email protected] Address: http://www.dhfs.state.wi.us/ssi/
Starkey Hearing FoundationDescription: hearing aidsContact Info: 1-800-328-8602Web Address: http://www.starkey.com/about/about5_foundation.html
Telecommunications Equipment PurchaseProgram (TEPP)Description: specialized telephone access equipmentContact Info: 608-231-3305
Tribal Health CentersDescription: available services dependent on each tribeContact Info: tribal health centerWeb Address: http://www.dhfs.state.wi.us/dph_ops/lhdl.htm#Tribal
MANAGED ADVOCACY IN ACTION Health Care Financing Resources • 57
Unified Services BoardDescription: services related to mental health, develop-mental disabilities, and substance abuseContact Info: county social services
United Cerebral Palsy of West CentralWisconsinDescription: lending library of equipment used in physicaltherapy, neuro-developmental clinic, and financialassistanceContact Info: 1-888-845-5775; [email protected] Address: http://www.ucpa.org/main.cfm/156
Veterans Health BenefitsDescription: various health care programs for veteransand their familiesContact Info: local county veterans service office or 608-266-1311; 1-800-947-8387Web Address: http://dva.state.wi.us/benefits.asp
Viatical SettlementsDescription: sale of life insurance policy for cash, call theOffice of the Commissioner of Insurance to get names ofcompanies licensed to do business in WisconsinContact Info: 1-800-236-8517
Vision USA (available in limited months)Description: eye exam and glassesContact Info: 1-800-678-5357Web Address: http://www.aoa.org/visionusa.index.asp
Waisman Center Genetics ClinicDescription: genetics-related servicesContact Info: [email protected] Address: http://www.waisman.wisc.edu
Western Wisconsin Legal ServicesDescription: legal services agencyContact Info: 608-785-2809 or [email protected]
WIC ProgramDescription: food and infant formulaContact Info: [email protected] Address: http://www.dhfs.state.wi.us/wic
WisconscareDescription: low cost health insurance in certain countiesContact Info: 608-221-3815Web Address: http://www.safetyweb.org/publications/factsheets/ir-wiscc.htm
Wisconsin Coalition for AdvocacyDescription: protection and advocacy for persons withdevelopmental or physical disabilities and people withmental illnessContact Info: 1-800-928-8778Web Address: http://www.w-c-a.org
Wisconsin Coalition of Independent LivingCentersDescription: adaptive aids and equipmentContact Info: 1-800-690-6665 or [email protected]
Wisconsin Council for the BlindDescription: rehabilitation, canes, and loansContact Info: 1-800-783-5213 or [email protected] Address: http://www.wcblind.org
Wisconsin Women’s Cancer ControlProjectDescription: mammograms, pap smears, exams, andtestsContact Info: 1-800-422-6237
Wisconsin’s Well-Woman Health ScreeningProgramDescription: breast and cervical cancer, diabetes,depression, heart disease, osteoporosis, etc.Contact Info: 1-800-397-7094Web Address: http://www.nci.nih.gov

58 • Health Care Financing Resources MANAGED ADVOCACY IN ACTION
WisTECHDescription: assistive technology for daily livingContact Info: 608-266-9303Web Address: http://www.wistechstate.wi.us
Worker’s Compensation BureauDescription: work-related injuriesContact Info: 608-267-1365Web Address: http://www.dwd.state.wi.us/wc
World Life FoundationDescription: air travelContact Info: 1-800-289-5433

HealthWatch Mission forSouth Central Wisconsin
Appendix D
Description of HW in Dane countyThe HealthWatch committee was developed to ad-vocate for and with low-income families in Wiscon-sin on issues relating to access and quality of healthcare services with a particular emphasis on Medic-aid managed care.
Although the mission has been revised since it wasfirst created, HealthWatch Dane County’s mission isto advocate for underserved populations on issuesrelating to access and quality of health care servicesand coverage, with particular emphasis on peopleenrolled in Medicaid and BadgerCare.
The goal is to improve the delivery of quality healthcare services to people with low incomes. To accom-plish this goal, HealthWatch will facilitate communi-cation among groups affected by managed careprograms, identify areas of concern regarding ac-cess to health care services, and participate in prob-lem solving strategies and offer policy changes.
Goals and objectives of the group include:1. Advocate on health care issues to state,
county and local agencies and managedcare organizations.
¨ Develop contract recommendations to theState. (Managed care, and enrollment.
¨ Analyze and interpret information from theState and HMOs, regarding utilization data,audits, contract evaluations, reimbursementfigures and health goals.
¨ Monitor, analyze and respond to ongoingpolicies and practices of HMOs, certifiedMedicaid and other providers.
¨ Monitor, analyze and respond to ongoingstate initiatives involving health care.
2. Monitor, develop and promote strategiesto resolve issues arising from the impactof welfare reform upon the access to qual-ity health care coverage for low-incomefamilies, with specific attention to the fol-lowing:
¨ Eligibility and access.
¨ Expansion of safety net programs to coverthose who will become uninsured.
¨ Support the development of a monitoringor evaluation system to assess the impactof welfare reform.
¨ Support the development of a statewidenetwork of advocacy for access to qualityhealth care for low-income families.
¨ Provide input to the State administrativerule-making process on health care issues.
¨ Link with other HealthWatch groupsaround the state for a more unified voiceon shared issues
3. Increase membership, participation and in-volvement of interested organizations, in-cluding Family Medicaid/BadgerCareenrollees in HealthWatch, specifically to:
¨ Develop additional resources to achieveHealthWatch goals.
60 • HealthWatch Mission for South Central Wiscosnin MANAGED ADVOCACY IN ACTION
¨ Conduct outreach to culturally diverse popu-lations and organizations.
¨ Conduct outreach to FAMILY MEDICAID/BADGERCARE enrollees and organiza-tions that serve such persons.
¨ Promote opportunities for consumer in-volvement in HealthWatch actions and de-cision-making.
¨ Build partnerships with other committeesand organizations that share the Health-Watch mission.
4. Support innovative strategies to provide ad-vocacy and services to FAMILY MEDICAID/BADGERCARE enrollees toward a goal of“benefits management” through health ben-efits counseling
5. Promote the education of health care pro-fessionals about health care reforms tak-ing place at both the state and federallevels.
HealthWatch activities include, but are not lim-ited to, advocacy with the managed care industry,recipient and provider education, supporting and pro-moting the role of local health departments in moni-toring and assuring access to care for people andinfluencing the development of policy. The goal is toimprove the delivery of health care services to low-income families and individuals. HealthWatch willfacilitate communication among groups affected byMedicaid managed care programs, identify areas ofconcern regarding access to health care services,and participate in problem solving strategies and of-fer policy changes.
HealthWatch provides an important forum forconsumers and advocates to vocalize their concernsrelated to managed care and more importantly ad-vocate for positive change.

Prior Authorization BasicsAppendix E
Spring 2002
Problems with PAs
As many families and advocates havediscovered, the Prior Authorization (PA)process for getting medically necessarytherapies approved is both cumbersomeand complicated. This is particularly diffi-cult for parents working with school- andcommunity-based services, privateinsurance and Medicaid.
While a child has a right to receive bothschool therapies and medically necessarycommunity therapies, there is often aconflict over who should pay. Problems canbe avoided by creating a PA request that iscarefully coordinated with the Individual-ized Education Program (IEP). A child canbe functional in school and not in a homeenvironment. As a result, the IEP teamshould clearly explain that the requestedPA service is medically necessary for non-education needs.
Putting a PA Together
PA requests are prepared by the provideroffering the services. Each request includestwo attachments that are reviewed by EDSconsultants: the Prior Authorization TherapyAttachment (PA/TA) and a copy of theIndividualized Education Plan (IEP) forschool-aged children or the IndividualizedFamily Support Plan (IFSP) for children notyet in school.
The PA/TA and IEP/IFSP are usedtogether to review the recipient’s medicaland therapy histories to determine if therequested PA is appropriate. If the recipi-
ent is receiving other services (such ashome health services, in-home autism pro-gram services or has access to or usesadaptive equipment), information aboutthose services should be included in the PArequest.
PA Therapy Attachment
The PA/TA contains information such as thetotal number of sessions required andnumber of times per day/week. The PA/TAalso includes pertinent medical andpersonal history, including the recipient’sdiagnosis and date of onset of thediagnosis, the recipient’s occupational andeducation status, living situation, durablemedical equipment used, and recentchanges in his/her condition.
The TA also is used to report therecipient’s therapy history, which includescurrent therapies, previous therapies, andthe objectives of the therapy. It furtherdescribes the progress of previoustherapies in measurable and functionalterms since treatment was initiated or lastauthorized.
PA/TA vs. IEP
A PA may be denied if the requestedtherapy is also listed in the IEP/IFSP as itmay be considered duplicative. The TA isthe place where supplementary and re-lated information can be described tostrengthen the recipient’s case for theequipment or services. IEPs often don’t pro-vide specific information that could be com-pared to what is requested in the PA. Pro-viders need to describe why the requestedtherapy is medically necessary and how itwill result in a functional outcome differentfrom that of the school therapy.
New PA/TA Form
Wisconsin Medicaid has introduced arevised PA/TA that providers have beenrequired to use since January 2002.Revisions to the form were made to helpproviders identify required elements andgive suggestions about the clinical detailsneeded in the request. For more informa-tion and copies of the new form, see theshaded box.
If Your Prior Authorization IsDenied
If the PA is denied, the recipient or therecipient’s family or legal guardian willreceive a form letter stating the servicesrequested, the action taken and codes forany modified or denied services. The letteralso contains an explanation of how toinitiate the appeal process, which isoverseen by the Division of Hearing andAppeals (DHA). The appeal must be filedwithin 45 days or families will lose their rightto appeal. Families who wish to haveassistance in preparing for the hearing,may request a postponement of their firsthearing date, while they are seeking coun-sel.
Reduction or Modification
If a PA request is approved with a reduc-tion in the duration of the request, it is con-sidered an approved PA. If the frequencyof the service is reduced (i.e., therapy wasrequested for 3x/week but changed by thereviewing consultant to 1x/week), it isconsidered a modification. The recipientor the recipient’s family will be notified oftheir right to appeal modified and deniedPA decisions.
ABC for Health152 W Johnson St Ste 206Madison WI 53703-2213tel 608.261.6939fax 608.261.6938email [email protected] www.abcforhealth.org
The insert includes information from Families MAP meeting minutes and FMAP trainings on Prior Authorizationoffered over the lastyear. Presentors included Lynn Steffes, from the WCDD and Barbara Evans from the Division of Health Care Financing. The meetingminutes can be viewed on the ABC for Health website at www.abcforhealth.org.

ABC for Health Prior Authorization Basics Winter 2001
Improvements to the Process
PAs for things such as medications, ortho-pedic shoes, etc., can now be done overthe phone. Also providers have been ableto fax PAs since November 2000. Whensubmitted, the entire PA will be reviewedfor any clerical errors and then returned forcorrections, so that providers need to makeonly one set of clerical revisions. When thePA is resubmitted, if the necessary clericalinformation has been corrected, the PA willbe forwarded to the clinical consultant forreview. If the clinical documentation isincomplete, all additional clinical informa-tion needed will be identified before beingreturned to the provider.
All documentation needs to be clearand detailed to provide reviewers withample information that services are appro-priate and necessary. Many cases aremade more difficult because of inadequatedocumentation of progress made by CSHN.Certainly this type of “front end” effort canhelp avoid many difficulties and problemslater on down the road. Even with gooddocumentation there are still several areasthat can cause frustration for parents.
Role of the Parents
In a March 2002 presentation, Lynn Steffes,a pediatric physical therapist, explainedthat in the PA process, the therapist tries tocapture functional and measurable infor-mation. It is critical that families considerthemselves partners in therapy, both in as-sisting children at home and in initiating thePA. Parents can begin, by making sure theirchild is diagnosed early. Parents are some-times reluctant to label their child with adiagnosis, but getting an accurate diagno-
sis may help to get services covered. (Formore about working successfully with atherapist, contact Lynn at stefbiz.wi.rr.com.)
Most children receive therapy only a fewtimes a week. Therefore, therapists workwith parents on maintaining the skills athome. However, a line needs to be drawnbetween reinforcing therapy lessons athome and asking the parents to be a thera-pist. The therapist should find out from thefamily what outcomes they desire for theirchild, as they will most likely be more aptto work with their child on attaining thosegoals at home. Also if a family membercannot assist with therapy homework dueto things such as caring for other childrenin the home or work reasons, this can benoted in the PA to potentially insure thetherapy hours outside of the home.
Role of the Therapist
The role of the therapist is to listen and in-terpret the challenges the family is havingand educate them to help them navigatethe system. Historically, providers havetried to assist and even insulate familiesfrom the process by telling them that theywould take care of the prior authorizationand follow-up. Rather, providers, families,members, advocates and the doctor mustall be empowered and involved. Therapistsneed to try and optimize care, not maxi-mize it.
More Is Not Always Better
Therapists should look at any treatmentplan to determine whether or not the childactually needs a specific service. Provid-ers should also look at past reports beforeevaluating a child. There are cases where
the length of treatment may be too longfor the child to handle or where moretherapy will not yield additional benefits, butwill keep the child from going about theirlife for another three or more hours a week.
Reduction of Requested Services
On the other hand, when EDS or DHCFreduces the frequency or duration oftherapy, the therapist may not be able toaccomplish the original goals in the shortertime period. When PAs are returned it takessome weeks to catchup, leaving the thera-pist and child with very few weeks of ap-proved therapy. If a subsequent PA is thenrequested, it may be denied because noprogress had been shown from the previ-ous PA.
This insert can be used as a tool to helpparents better understand how to write andeffective PA. However, it only scratches thesurface of the information available forparents about the PA process. For addi-tional information about PAs, refer to theshaded box below.
We deliver to your desktop!To subscribe to the weekly email version of the Updatesend a blank email to [email protected]
ADDITIONAL RESOURCES
DAWN Resources on Prior Authorizationdawninfo.org/advocacy/issues/medicaid.cfm
Medicaid Therapy Serviceswww.dhfs.state.wi.us/medicaid1/recpubs/child_index.htm
New Prior Authorization TherapyAttachment Form and Instructions
www.dhfs.state.wi.us/medicaid/updates/2001/2001-37.htm
Department of Public InstructionParent Page: www.dpi.state.wi.us/dpi/dlsea/een/hmparents.html
IEP: www.dpi.state.wi.us/dpi/dlsea/een/sbiep.html
HealthWatch Digest
Appendix F
A sample digest of selected HealthWatch reportsfrom the minutes of the Dane County HealthWatchCommittee
Inappropriate Billing of Medicaid Recipi-entsBobby is concerned that when Medicaid recipientsare told it’s illegal for a recipient to be billed by aprovider, they throw the bills away without notifyinganyone. This can create serious problems if thematter if referred to collections or judgment is en-tered against family. These third party billing issuesare easier to untangle if they can be dealt with rightaway. Bobby would like to see families facing thisissue referred to Amy Jones at the Justice Depart-ment (200.3444), Mullin Williams at the US Attor-neys Office (608.264.2222) or ABC for Health. Pamsuggested that people working with Medicaid recipi-ents remind the consumer to immediately contactsomeone if a provider bills them.
Families MAP and the HMO ContractThe next Families MAP meeting on July 17th will fo-cus looking at contract issues and how it affects chil-dren with special health care needs. Because FMAPis working to promote a partnership between MCOs,parents and advocates, recommendations at thatmeeting will need to be made on a consensus ba-sis. The southern forum is July 11th and will alsofocus on the HMO contract. ABC will let the FMAPparticipants know so they can participate.
Job LossesIts important to keep families facing a lay-off con-nected to health care coverage. Matt Olson at ABCincluded a list of the plant closings announced byDWD in the Weekly Update. ABC is consideringsending letters to plant personnel around the stateto inform them about BadgerCare eligibility.
COBRAJim, from Dane County Economic Support, addedthat it is important for people to realize that COBRAis not the only health insurance option for peopleleaving or losing a job. People have 60 days to de-cide whether or not to opt for COBRA. Paul alsopointed out that confusion over when insurance froma previous job ends can result in families losing Bad-gerCare.
HMO PanelThe HMO panel discussion on 8/3, sponsored byFamilies MAP was a forum to bring the HMOs andconsumers together to get questions answered andcreate some understanding, and was a success.ABC may suggest that the Statewide Coalition andthe pilots use a similar format and hold other forums.Minutes are being put together and will be sent outshortly.
CSHCN Report

64 • HealthWatch Digest MANAGED ADVOCACY IN ACTION
Barbara reported about the prior authorization fo-rum concerning the denial of therapy services forCSHCN. The forum included Rep. Mark Miller whois interested in learning more about the subject inhopes of bringing it to the legislature for a solution.The forum was timed in conjunction with the legisla-tive audit bureau.
Bobby reported that ABC would like to have a smallermeeting with Miller to discuss some of the strate-gies that have been developed by the stakeholders.Barbara also reported that the State legislature hasa special committee on developmental disabilitiesthat is looking at the waiting list issues.
OutreachBarbara explained that she is working on outreachfor FMAP. She is working to get more parents ofCSHCN informed about the work of FMAP and hookthem up with our agency and the committee. She isalso learning about managed health care issues that
families are dealing with. If anyone is working witha parent organization or parent of a CSHCN thathas any managed health care issues please referthem to Barbara.
Regional CSHCN CentersThere was a discussion concerning the regionalhealth care centers. The state has funded 5 regionalcenters to work directly with the counties (probablylocal and county health departments) to coordinateservices for CSHCN and to provide supportive ser-vices to the county. The Waisman Center is he re-gional center for the southern region (including DaneCounty). A list of the CSHCN centers will be postedon the ABC website at www.abcforhealth.org. If youwould like a copy, contact Michele at 261-6939 ext.200. Barbara will contact Amy from Waisman to givea presentation on the services that are available inthis region.
HMO/Medicaid Contract
Each state has a contract between the single stateMedicaid agency and the health maintenance orga-nizations (HMOs) that serve the state’s Medicaidpopulation. The contract is an important documentbecause it governs how Medicaid clients are treated,who will pay, what services the clients will receive,what rights the clients have and how those rightsare enforced.
In addition to being a valuable advocacy tool,your state’s HMO/Medicaid contract is a vehicle formaking changes to the system. The contract mustbe renewed periodically (typically every two years).This is a great time to bring issues to the attention ofstate administrators and collectively develop recom-mendations to resolve problems in the state’s Med-icaid managed care system. The procedure forrenewing the contract will vary from state to state.Federal regulators look for evidence that the statesolicited community level input into the state con-tract. Some states may actively solicit public partici-pation in the process; others may attempt to do thingsbehind closed doors. However the state chooses togo about revising the terms of its contract, keep inmind that the process is a matter of public recordand that your advocacy network is entitled to access.If you feel you being shut out of the process youmay want to contact your regional CMS administra-tor to complain. Or if you find that the state does notopenly solicit public commentary on the contract re-newal, remember that other avenues—the media,friendly legislators, or letter campaigns, for example—are available to make your voice heard.
Getting input from your networkYour advocacy network’s input into the contract pro-cess is especially important for at least two reasons.First, two parties, the state and the HMOs, leavingthe Medicaid population out of the loop, sign theHMO/Medicaid contract. Your advocacy group canspeak as and on behalf of Medicaid clients, thus in-jecting a missing piece into the contract renewal.Second, if your advocacy group is composed of rep-resentatives of all sectors of the medical world—patients, providers, advocates, etc.—you have atyour disposal a powerful pool of knowledge aboutthe realities of the health care system. Together,you can possess both an intimate understanding ofwhat works and what doesn’t work as well as theperspectives needed to come up with innovativesolutions. If, additionally, you can reach consensuson recommendations for changes to the contract,the suggestions you submit will have the added cloutof a group of people who use and work in the sys-tem. Moreover the state may actually appreciate youradvocacy efforts as it provides an important coun-terweight in often difficult negotiations with politicallypowerful managed care entities.
With respect to the contract renewal cycle spe-cifically, your network will need to find out when thecurrent state HMO/Medicaid contract expires andwhether and how public input on the upcoming con-tract will be taken. To get this information, your groupshould contact the single state Medicaid agency. Ispecific? Once you know when and how to makeyour recommendations, you can begin planning astrategy for compiling the suggestions.
Appendix G

66 • HMO/Medicaid Contract MANAGED ADVOCACY IN ACTION
Establishing proceduresIt is also important for your group to think about andcome to agreement in advance on what the group’sprocedure will be for submitting contract change sug-gestions. This will help to avoid headaches and sur-prises down the line.
As your advocacy group may well find, how-ever, the contract on paper often differs substantiallyfrom how HMOs, providers and Medicaid clients in-teract on a day-to-day basis. An essential part ofyour contract review, therefore, should be an effortto draw on the practical experiences of people us-ing, working in, or operating the Medicaid managedcare system. Finally, there are some national re-sources that can be very helpful to your group’sanalysis of your existing contract. The Center forHealth Services Research and Policy at GeorgeWashington University publishes a periodic compara-tive review of state Medicaid managed care con-tracts. The same Center has also published “SamplePurchasing Specifications”—essentially a modelcontract—for state Medicaid managed care pro-grams. These two documents can help you to iden-tify some of the strengths and weaknesses of yourcontract and give you ideas about alternative con-tract provisions. Both publications are available viathe Center’s website at: Center’s website at:). Check.Select “Contract Studies” or “Sample PurchasingSpecifications” from the sidebar to find the managedcare contracts.
Additionally, new federal legislation may haveimpacts on state Medicaid managed care contracts.The best source for this information is FamiliesUSA,which can be contacted via the web at: http://www.familiesusa.org. Select “Managed Care” fromthe Issues sidebar.
Out of this review, you should be able to gathera rather substantial set of comments, ideas and sug-gestions for changes. For organizational purposes,it may be useful to you to divide the feedback youhave received into four groups:
� Eligibility and enrollment issues. Including:Outreach, mandatory enrollment,reenrollment, disenrollment, assignment ofprimary care physicians, continuity of care,barriers to client comprehension, etc.
� Benefits, coverage, services and access is-sues. Including: Emergency and urgentcare, special health care needs includingCSHCN, provider incentives, ‘medical ne-cessity’ determinations, discriminationagainst Medicaid clients, etc.
� Payment and billing issues. Including:Avoiding billing Medicaid clients, third partyliability, addressing low Medicaid cap rate,etc.
� Grievances and appeals issues. Including:Internal and external Medicaid patient ad-vocates, notice of right to appeal, sanctions,etc.
The next step is to convert the comments, ideasand suggestions you have gathered into a viablecontract change suggestions. If your state has aspecific system for receiving public input, be sure atthis point that the recommendations you are draft-ing fit whatever format the state requires. In somecases, submitting a comment alone may be suffi-cient. In other cases, you may have to include spe-cific citations from the existing contract. This is atricky step that you may want to delegate to a loneindividual or try to tackle in groups.
If, your state does not have an established pro-cedure for submitting recommendations for contractchanges, you will still need to synthesize your groups’thoughts and ideas on the existing contract into aformat (bullet points or a talking paper, for example)that can serve as the platform for your public rela-tions campaign.
Building consensusOnce your group has a set of draft contract changesuggestions, your next task is to build consensusaround them. A clear explanatory statement detail-
MANAGED ADVOCACY IN ACTION HMO/Medicaid Contract • 67
ing the group’s procedure for making commentsshould accompany drafts. The same individual orgroups that wrote the drafts of your group’s contractchange suggestions will then need to incorporate thecomments received from the group to produce a fi-nalized set of contract change suggestions.
Distribute the finalized versions to all membersof your group. At this point, your group will need asystem by which each member can indicate that theyeither approve or reject the individual contractchange suggestions. The two most obvious ways todo this are either by inclusion or by default. Usingthe inclusion method, members respond to the final-ized suggestions by indicating whether or not theywill sign on. Under the default method, the groupsecretary or chair can indicate that she intends tosubmit the finalized contract change suggestions bya specified date unless any member of the groupindicates their objection.
Submitting your resultsAs the next to last step, you must submit your sug-gestions to the state. If there is a formal process forthis, then making your submission should be rela-tively straightforward, however, depending on howimportant the changes are to your group, you mightwant to consider some kind of public relations eventto coincide with the submission in order to draw ex-tra attention to your idea and put additional pres-sure on the state to accept it. If your state has noformal process for public input in the contract renewalprocess, you will need to be more creative aboutyour method for submission. It’s possible that youcan piggyback off of a sympathetic legislator or oth-
erwise make your suggestions known through themedia and lobbying. You might also wish to con-sider a campaign to open the Medicaid managedcare contract renewal process to greater public in-put and access.
Finally, your group will need to follow-up andmonitor the contract renewal process. This is espe-cially important whether your group decides to sub-mit contract change suggestions or not. Even ifnobody else weighs in on the new contract, the stateand the HMOs will since they are the contractingparties. Both the HMOs and the state have incen-tives to reduce costs and they may use the contractrenewal to pursue these interests in ways that aredetrimental to the provision of quality service to Med-icaid clients.
Your advocacy network is in an excellent posi-tion to evaluate any changes that either the state orthe HMOs propose. To do so, however, your groupmust keep a close watch on the development of thenew contract. You should be able to obtain drafts ofthe new contract before it is signed, appealing topublic records laws if necessary. In the event thatyour analysis reveals major and detrimental changesto the contract, you may want to prepare some formof response, through lobbying or public relationsstrategies, to prevent the offending piece of the newcontract draft from being incorporated into the finalversion.
This last piece of the process should not belooked upon as an afterthought. Your advocacy net-work should consider defending the strengths of thecurrent contract just as important as the effort to findremedies for the contract’s weaknesses.



ABC for Health152 West Johnson Street, Suite 206Madison, Wisconsin 53703-2213tel 608.261.6939 800.585.4222fax 608.261.6938web www.abcforthealth.org


















