Malnutrition - ACDIS Malnutrition PresentationFinalPDF.pdf · Malnutrition: Did you know... • 1...
22
Malnutrition By Litsa Georgakilas, RD LDN CNSC
Transcript of Malnutrition - ACDIS Malnutrition PresentationFinalPDF.pdf · Malnutrition: Did you know... • 1...

Malnutrition By Litsa Georgakilas, RD LDN CNSC

Overview
How is malnutrition defined?
Malnutrition diagnosis
ASPEN guidelines
Contacting a dietitian
Malnutrition: Did you know...
• 1 in 3 patients are malnourished on admission
• Patients diagnosed with malnutrition have a 3 times longer LOS
• Surgical patients with malnutrition have a 4 times higher risk of pressure ulcer
development
• The annual burden of disease-associated malnutrition across 8 diseases in the
U.S. is $156.7 billion
What is malnutrition? “An acute, subacute or chronic state of nutrition in which a combination of varying
degrees of overnutrition or undernutrition with or without inflammatory activity have led to a change in body composition and diminished function.”
– American Society of Parenteral Enteral Nutrition
Who is at risk?
Adults should be considered at risk if they have any of the following:
• Involuntary loss or gain within 6 months • Body mass index less than 18.5 kg/m2 or greater than 25 kg/m2 • Chronic disease • Increased metabolic requirements • Modified Diet • Inadequate nutrition intake, including not receiving food or nutrition products for
greater than 7 days
Malnutrition Diagnoses
● Involves:
○ Knowledge about the needs of
the population and individual
patient
○ Clinical judgement
○ Evidence-based practice
○ Nutrition standards
Malnutrition Etiologies
• Social/ Environmental Circumstances – Chronic starvation without
inflammation (access to food is limited, ex. Anorexia nervosa, physical conditions)
• Chronic Illness – mild- moderate inflammation for 3 months or longer (ex.
cancer, AIDS, COPD, celiac disease, CF, DM, chronic pancreatitis, sarcopenic
obesity)
• Acute Illness/ Injury - Moderate – severe inflammation for less than 3 months
(ex. infection, burns, trauma or pancreatitis, major surgery)
Diagnosis Criteria Weight loss: considers hydration status; weight change over time is represented as a percentage
of weight loss from baseline
Intake: RD obtains diet history and estimates energy needs; inadequate intake is represented as a
percentage of estimated need over time
Physical Assessment (FAT): loss of subcutaneous fat (i.e. triceps, fat overlying ribcage)
Physical Assessment (MUSCLE): loss of muscle (i.e. clavicles, shoulders, thigh)
Physical Assessment (FLUID): general or local fluid accumulation (i.e. extremities, ascites, or
vulvar/scrotal edema)
Functional Assessment: based on standards supplied by manufacturer of dynamometer
Diagnosis Criteria Weight loss
• Acute Illness- weight change estimated over 1 week, 1 month or 3 months
• Chronic Illness- weight change estimated over 1 month, 3 months, 6 months, 12 months
Intake
• Severe- Acute- </= 50% of estimated needs >/= 5 days
• Moderate- Acute- <75% of estimated needs > 7 days
• Severe- Chronic- </= 75% of estimated needs >/= 1 month
• Moderate- Severe- <75% of estimated needs >/= 1 month

Nutrition Focused Physical Exam
BIDMC approved abbreviation: NFPEx
• A head to toe examination to determine micronutrient deficiencies and fat, muscle
loss
Diagnosis Criteria Loss of subcutaneous fat
• Orbital, triceps, thoracic, lumbar, ribs, midaxillary line
Loss of lean muscle
• Temporalis muscle, clavicular and acromion bone, deltoid muscle, interosseous muscle, anterior
thigh, quadriceps, patellar region, gastrocnemius
Diagnosis criteria Edema & Ascites
• Weight loss may be masked by fluid retention
• Used as supportive evidence, but not necessarily r/t malnutrition
• Localized vs Generalized
• Scale +1 to +4
Mild: +1 (2mm)
Moderate: +2 (2-4mm)
Severe: +3 or greater (4-8mm)
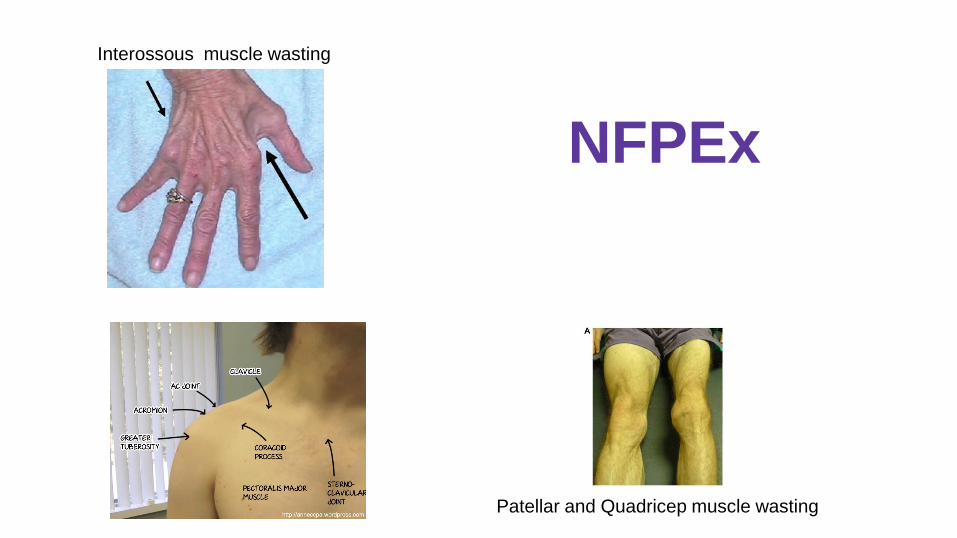
Interossous muscle wasting
Patellar and Quadricep muscle wasting
NFPEx
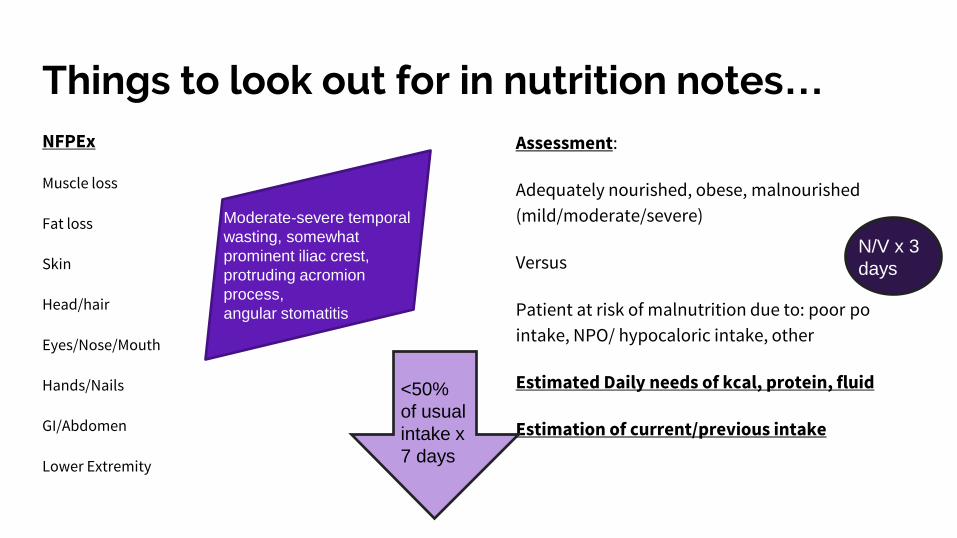
Things to look out for in nutrition notes… NFPEx
Muscle loss
Fat loss
Skin
Head/hair
Eyes/Nose/Mouth
Hands/Nails
GI/Abdomen
Lower Extremity
Assessment:
Adequately nourished, obese, malnourished
(mild/moderate/severe)
Versus
Patient at risk of malnutrition due to: poor po
intake, NPO/ hypocaloric intake, other
Estimated Daily needs of kcal, protein, fluid
Estimation of current/previous intake
Moderate-severe temporal
wasting, somewhat
prominent iliac crest,
protruding acromion
process,
angular stomatitis
<50%
of usual
intake x
7 days
N/V x 3
days
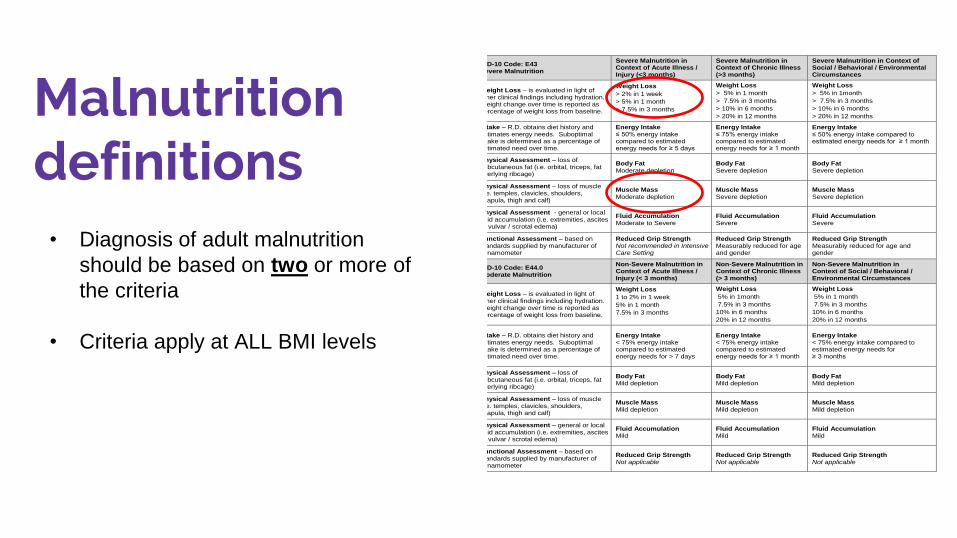
Malnutrition definitions
ICD-10 Code: E43 Severe Malnutrition
Severe Malnutrition in Context of Acute Illness / Injury (<3 months)
Severe Malnutrition in Context of Chronic Illness (>3 months)
Severe Malnutrition in Context of Social / Behavioral / Environmental Circumstances
Weight Loss – is evaluated in light of other clinical findings including hydration. Weight change over time is reported as percentage of weight loss from baseline.
Weight Loss
> 2% in 1 week
> 5% in 1 month
> 7.5% in 3 months
Weight Loss
> 5% in 1 month
> 7.5% in 3 months
> 10% in 6 months
> 20% in 12 months
Weight Loss
> 5% in 1month
> 7.5% in 3 months
> 10% in 6 months
> 20% in 12 months
Intake – R.D. obtains diet history and estimates energy needs. Suboptimal intake is determined as a percentage of estimated need over time.
Energy Intake ≤ 50% energy intake compared to estimated energy needs for ≥ 5 days
Energy Intake ≤ 75% energy intake compared to estimated energy needs for ≥ 1 month
Energy Intake ≤ 50% energy intake compared to estimated energy needs for ≥ 1 month
Physical Assessment – loss of subcutaneous fat (i.e. orbital, triceps, fat overlying ribcage)
Body Fat Moderate depletion
Body Fat Severe depletion
Body Fat Severe depletion
Physical Assessment – loss of muscle (i.e. temples, clavicles, shoulders, scapula, thigh and calf)
Muscle Mass Moderate depletion
Muscle Mass Severe depletion
Muscle Mass Severe depletion
Physical Assessment - general or local fluid accumulation (i.e. extremities, ascites or vulvar / scrotal edema)
Fluid Accumulation Moderate to Severe
Fluid Accumulation Severe
Fluid Accumulation Severe
Functional Assessment – based on standards supplied by manufacturer of dynamometer
Reduced Grip Strength Not recommended in Intensive Care Setting
Reduced Grip Strength Measurably reduced for age and gender
Reduced Grip Strength Measurably reduced for age and gender
ICD-10 Code: E44.0 Moderate Malnutrition
Non-Severe Malnutrition in Context of Acute Illness / Injury (< 3 months)
Non-Severe Malnutrition in Context of Chronic Illness (> 3 months)
Non-Severe Malnutrition in Context of Social / Behavioral / Environmental Circumstances
Weight Loss – is evaluated in light of other clinical findings including hydration. Weight change over time is reported as percentage of weight loss from baseline.
Weight Loss
1 to 2% in 1 week
5% in 1 month
7.5% in 3 months
Weight Loss
5% in 1month
7.5% in 3 months
10% in 6 months
20% in 12 months
Weight Loss
5% in 1 month
7.5% in 3 months
10% in 6 months
20% in 12 months
Intake – R.D. obtains diet history and estimates energy needs. Suboptimal intake is determined as a percentage of estimated need over time.
Energy Intake < 75% energy intake compared to estimated energy needs for > 7 days
Energy Intake < 75% energy intake compared to estimated energy needs for ≥ 1 month
Energy Intake < 75% energy intake compared to estimated energy needs for ≥ 3 months
Physical Assessment – loss of subcutaneous fat (i.e. orbital, triceps, fat overlying ribcage)
Body Fat Mild depletion
Body Fat Mild depletion
Body Fat Mild depletion
Physical Assessment – loss of muscle (i.e. temples, clavicles, shoulders, scapula, thigh and calf)
Muscle Mass Mild depletion
Muscle Mass Mild depletion
Muscle Mass Mild depletion
Physical Assessment – general or local fluid accumulation (i.e. extremities, ascites or vulvar / scrotal edema)
Fluid Accumulation Mild
Fluid Accumulation Mild
Fluid Accumulation Mild
Functional Assessment – based on standards supplied by manufacturer of dynamometer
Reduced Grip Strength Not applicable
Reduced Grip Strength Not applicable
Reduced Grip Strength Not applicable
• Diagnosis of adult malnutrition
should be based on two or more of
the criteria
• Criteria apply at ALL BMI levels
Case Study J.M. 72YO F who reports 6-7 months of decreased appetite r/t nausea. Consuming smaller breakfast, skipping L/D some days or having small bowl of soup, ½ sandwich.
59 in, Admit weight: 57 kg, UBW 70-72 kg
Dx: Pancreatic cyst (polycystic intraductal papillary mucinous neoplasia of the pancreas
PMhx: PE x 2, GERD, thyroid CA, anemia, pancreatitis
Labs: glucose 197 mg/dL, all other labs WNL
Diet order: NPO
No physical assessment performed
Abdomen WNL, NGT with no output
Coding
• Patient was seen POD1 from subtotal pancreatectomy and splenectomy
• Chronic -Severe malnutrition: 30 lb (19%) weight loss x 6- 7 months , <75% energy
intake >1 month r/t nausea
• Plan for diet advancement to low fat, starting diabetic oral supplements and
trending weights
When Should You Contact a Dietitian?
When a patient is suspected to have moderate or severe malnutrition
To confirm a diagnosis by verifying that at least 2 criteria have been met
To rule out other possible conditions
WRAP UP
• No universal definition of malnutrition
• Diagnosis requires anthropometric data, food/nutrient intake, laboratory data and a
complete NFPEx completed by an RD
• Malnutrition is associated with increased hospital costs, 1.5-5x higher rate of in
hospital death, 4x higher risk of developing pressure ulcer, and 2x longer hospital
stays
References http://journals.sagepub.com/doi/pdf/10.1177/0148607113512154
https://www.nutritioncaremanual.org/topic.cfm?ncm_category_id=11&lv1=144942&lv2=272214&ncm_toc_id=272214&ncm_headin
g=&
https://www.nutritioncaremanual.org/topic.cfm?ncm_category_id=11&lv1=144942&lv2=272215&ncm_toc_id=272215&ncm_headin
g=&
http://www.nutritioncare.org/malnutrition/
http://www.nutritioncare.org/Guidelines_and_Clinical_Resources/Toolkits/Malnutrition_Toolkit/
http://www.nutritioncare.org/uploadedImages/01_Site_Directory/Graphics_Directory/MAW/ASPEN%20Adult%20Care%20pathway_
Page_1.jpg?n=265
file:///C:/Users/Ashley%20St.%20Amand/Downloads/AMN%20FAQs%20November%202014_Final.pdf