
Malignant Bone Neplasms
77
-
Upload
waiting488 -
Category
Documents
-
view
214 -
download
0
Transcript of Malignant Bone Neplasms
8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 1/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 2/77
Osteosarcoma is a malignancy of mesenchymal cells that have the ability to produce osteiod or immature bone .
Excluding hematopoietic neoplasms, osteosarcoma is the most
common malignancy to originate within the bone.
Two forms -Osteoblastic or sclerosing type and osteolytic type.
Majority having intramedullary origin but a small number may
be juxtacortical.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 3/77
Occurs chiefly in young persons,
majority between the age 10 and
25 years.
Males affected more frequently than females.
Predominant site -long bones
chiefly the femur and tibia,
In older patients the axial skeleton and flat bones are
involved most frequently,.
8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 4/77
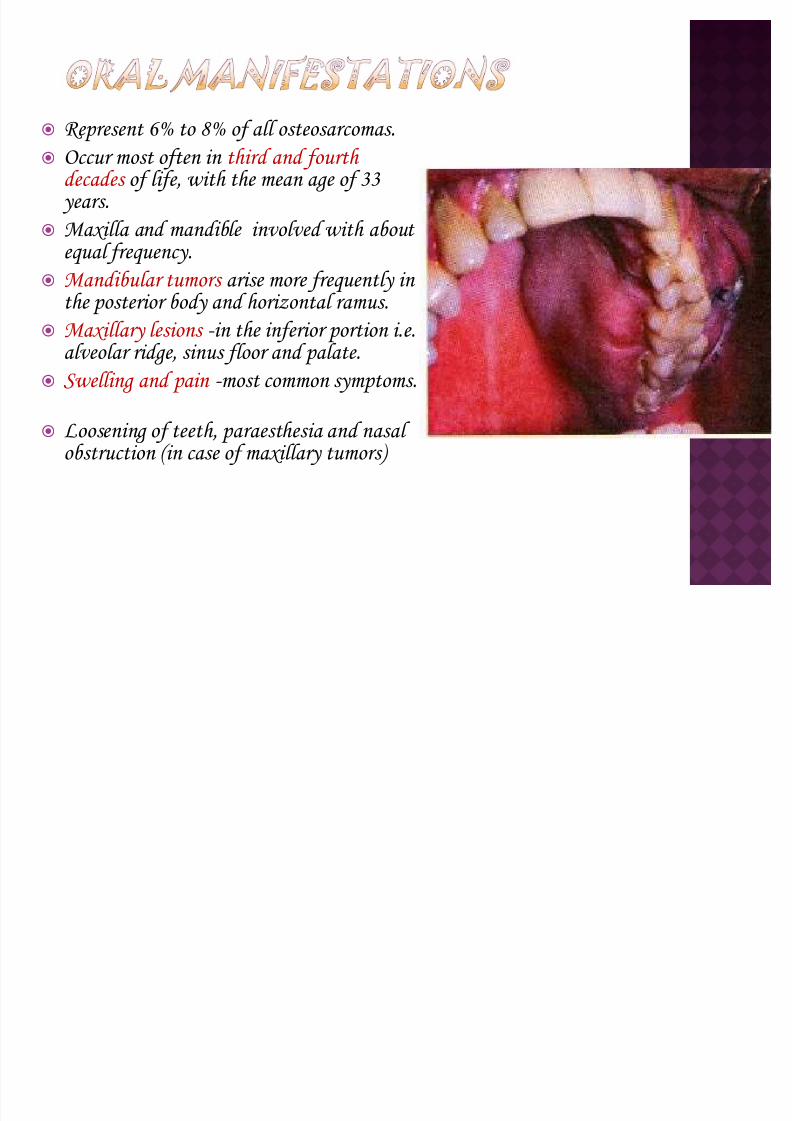
R epresent 6% to 8% of all osteosarcomas. Occur most often in third and fourth
decades of life, with the mean age of 33 years.
Maxilla and mandible involved with about equal frequency.
Mandibular tumors arise more frequently in the posterior body and horizontal ramus.
Maxillary lesions -in the inferior portion i.e.alveolar ridge, sinus floor and palate.
Swelling and pain -most common symptoms.
Loosening of teeth, paraesthesia and nasal obstruction (in case of maxillary tumors)

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 5/77
Periapical, occlusal and panoramic
radiographs can be taken.
SCLE R OSING TYPE:
Excessive bone production.
In some cases, irregular spicules or
trabeculae of new bone may be seen radiating outwards on the
periphery of the lesion, producing
the so called " SUN- RA Y"
appearance .

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 6/77
OSTEOLYTIC TYPE:
Destructive one, producing an irregular radiolucency and
demonstrating both expansion of
cortical plates and destruction.
A n important early radiographic
change- symmetric widening of the
periodontal ligament space around a
tooth or several teeth due to result of
tumor infiltration along the
periodontal ligament space:

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 7/77
If the internal structure is minimal or absent- fibrosarcoma or
metastatic carcinoma If osseous structure is visible - chondrosarcoma
If speculated periosteal new bone is present - prostate and breast
metastases
Benign tumors such as ossifying fibroma and benign conditions
such as fibrous dysplasia may mimic osteosarcoma; however these
conditions are usually better demarcated and have a more
uniform internal structure

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 8/77
8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 9/77
The treatment of osteosarcomas must be radical if there is to be
hope of curing the patient.
Treatment is by early mandibulectomy or maxillectomy together with wide excision of any soft-tissue extensions of the tumors.
May be combined with radiotherapy and/or chemotherapy .
The prognosis depends mainly on the extent of the tumor at
operation and The 5-year survival rate may range from 40% for
tumors less than 5cm in diameter to zero for tumors over 15cm.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 10/77
Originates adjacent to the cortex of the bone, initially grow
outward from the surface not involveing the underlying
medullary cavity.
The P AR SOTE A L type is a lobulated nodule attached to the
cortex by a short stalk. There is no elevation of the periosteum
and no peripheral periosteal reaction. It is a low-grade
sarcoma having a small risk of recurrence and metastasis.
The PE R IOSTE A L type is a sessile lesion that arises within
the cortex and elevates the over lying periosteum often, the
leading edge of the tumor mass perforates the surface of the
periosteum and extends into surrounding soft tissue.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 11/77
Characterized by the formation of cartilage , but not bone, by
the tumor cells.
Comprising about 10% of all primary tumors of skeleton but
rarely involving the jaws.
A bout half as common as osteosarcoma and about twice as common as Ewing's Sarcoma.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 12/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 13/77
A rise ore frequently in the axilla.
A painless ass or s elling.
ay be associated ith separation or loosening of teeth.
axillary tu ors ay cause nasal obstruction, congestion,
epistaxis, photophobia, or visual loss.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 14/77
Consists of a radiolucent process with poorly defined borders.
The radiolucent area often contains scattered and variable amounts of radiopaque foci, which are caused by calcification or ossification of the
cartilage matrix.
Penetration of the cortex can result in a sunburst pattern.
R oot resorption or symmetric widening of the periodontal ligament space of the teeth
They may grow in a lobular pattern with minimal or no foci of
calcification, appearing as a multilocular radiolucency.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 15/77
Ill-defined radiolucent lesion of posterior mandible
containing radiopaque foci

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 16/77
Osteosarcoma -radiographically indistinguishable.
A lthough the typical calcifications of chondrosarcoma
may be absent from osteosarcoma.
Fibrous dysplasia - the radiopaque portion is abnormal
bone and not calcification.
Periphery of fibrous dysplasia is better defined and its
margin from adjacent teeth differs from that of
chondrosarcoma.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 17/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 18/77
Grade II Chondrosarcoma
Moderately sized nuclei and increased cellularity, particularly
about the periphery of lobules. Low mitotic rate.
Grade III Chondrosarcoma
Highly cellular and may show a prominent spindle cell
proliferation.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 19/77
Prognosis related to the size, location and grade of the lesion.
The most effective treatment -radical surgical excision.
R adiation and chemotherapy -less effective and primarily used
for unrespectable high-grade chondrosarcoma.
Local recurrence leads to death by direct extension of the tumor into vital structures of head and neck.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 20/77
A lso called as 'Endothelial Myeloma' or ' R ound cell Sarcoma'.
Composed of small undifferentiated round cells of uncertain
histogensis.
6% to 8% of all primary malignant bone tumors
Third most common osseous neoplasm after osteosarcoma and chondrosarcoma.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 21/77
Second decade of life.
Slight male predominance
The long bones, pelvis and ribs are
affected most frequently.
Pain, often associated with
swelling -most common symptom.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 22/77
Intermittent pain varying from dull to severe.
Fever, leukocytosis and an elevated ES R .
Facial neuralgia and lip paraesthesia
Soft tissue mass overlying the affected area of bone.
More common in the mandible than the maxilla.
Paraesthesia and loosening of teeth.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 23/77
Irregular lytic bone destruction with ill-defined margins.
Cortical destruction or expansion may or may not be present.
´ onion-skin" appearance the film.
Thickened cortex infiltrated by the tumor.
Osteophyte formation

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 24/77
O steo yelitis ay share so e of the radiographic features of
ing·s sarco a; ho ever osteo yelitis is likely to have
de onstrable sequestration present ithin confines of the lesion,
hereas ing·s sarco a does not.
In case of eosinophilic granulo a of the ja , la inar periosteal
reaction is present in this condition, not in ing·s sarco a.
he other central pri ary alignancies of bone such as
osteosarco a, chondrosarco a and fibrosarco a

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 25/77
Composed of solid sheets or mass of small round cells with very little
stroma.
Small and round cells with little
cytoplasm and relatively large round or ovoid nuclei..
Broad sheets of small round cells
with well-defined nuclear outlines
and ill-defined cytoplasmic borders. Tiny vascular channels
A bsence of multinucleated giant
cells.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 26/77
Combined surgery, radiotherapy and multi drug chemotherapy.
Because of the risk of post radiation sarcomas, sometimes
radiation is not recommended.
It frequently metastasizes to the lungs, liver, lymph nodes and other bones.
The anatomical location of the tumor is a critical factor in
prognosis.
Pelvic lesions are associated with poorest diagnosis. Distal lesions have a better prognosis than those in a proximal location.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 27/77
Most common form of cancer involving the bone.
Carcinoma of lung, breast, prostate, thyroid and kidney give rise
to majority of gnathic metastasis.
Metastatic spread of a carcinoma to jaws usually occurs by
haematogenous route.
Sarcomas arising in soft tissues and other bones may metastasize
to the jaws, but this is very rare.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 28/77
Most patients are older,
The vertebrae, ribs, pelvis and skull -most frequent sites for
metastasis.
The jaws - uncommon sites for metastasis.
Metastasis to maxilla uncommon
Pain, swelling, loosening of teeth, a mass or paraesthesia.
Metastasis to the mandible with involvement of the inferior alveolar nerve producing NUMB-CHIN SYND R OME having
unexplained loss of sensation in the lower lip .

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 29/77
In some instances, the patient may be completely
asymptomatic and the diagnosis occurs only after
radiographic examination.
A n osseous metastasis may occur in a non-healing
extraction site from which the tooth was recently removed
because of complaints of local pain or significant mobility.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 30/77
A ppear as radiolucent defects.
May be well-circumscribed resembling a cyst, but more often is
ill defined with a " MOTH-E A TEN" appearance.
Widening of periodontal ligament.
Some carcinomas, particularly from the prostate and breast,
may stimulate new bone formation in the metastatic site,
resulting in radiopaque or mixed radiolucent and radiopaque
lesion

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 31/77
Panoramic radiograph showing destruction of alveolar bone surrounding the roots of Mandibular 2 nd
molar.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 32/77
Multiple myeloma- border is usually better defined than in
metastatic disease.
Periapical inflammatory lesion -periodontal ligament space widening from inflammatory lesion is centered about the
apex of root. In contrast the malignant tumor causes
irregular widening which may extend up the side of the root.
Squamous cell carcinoma - differentiated by clinical
examination.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 33/77
V arying microscopic appearance
In some instances, the
metastasis tumor is well
differentiated and closely resembles a colcannon of a
specific site, such as kidney,
colon or thyroid.
However, metastatic
carcinomas are poorly
differentiated

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 34/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 35/77
Uncommon malignancy of plasma cell origin that often
appears to have a multicentric origin within bone.
Neoplasm of bone that originates from cells of the bone
marrow which bear a remarkable to plasma cells.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 36/77
Disease of adults, with men being affected slightly more often than women.
Median age at diagnosis -between 60 and 80years
Twice as frequently in blacks as whites.
Bone pain is the most characteristic presenting symptom.
Fever may be present as a result of neutropenia with increased
susceptibility to infection.
Metastatic calcification may involve the soft tissues.R enal failure

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 37/77
Mandible is more frequently involved than the maxilla. The ramous angle and molar region of mandible -most frequent
sites of the lesion.
Sites classically affected include the oral mucosa, particularly
tongue. The tongue may show diffuse enlargement and firmness or may
have more of a nodular appearance.
Pain, swelling, and expansion of the jaw, numbness and mobility of tooth.
In addition, extra osseous lesions occur which may resemble gingival enlargements
Extension of the disease to other sites, outside the skeleton such as to lymph nodes, skin and viscera also occurs.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 38/77
Numerous sharply punched out areas.
May vary in size from a few
millimeters to a centimeter or more in diameter, but there is usually no
peripheral bone reaction.
Diffuse distribution lesions of bone
may also occur.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 39/77
Metastatic carcinoma ² knowledge of prior malignancy may help to differentiate from multiple myeloma.
Osteomyelitis ² a visible cause for it usually exists. A dditionally,
osteomyelitis causes sclerosis in adjacent bone, where multiple
myeloma does not. Simple bone cysts ²usually corticated in part and characteristically
interdigitate between the roots of the teeth in a much younger
population.
Metabolic diseases such as thalassemia, gaucher,s disease ² ruled out on the basis of medical history.
8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 40/77
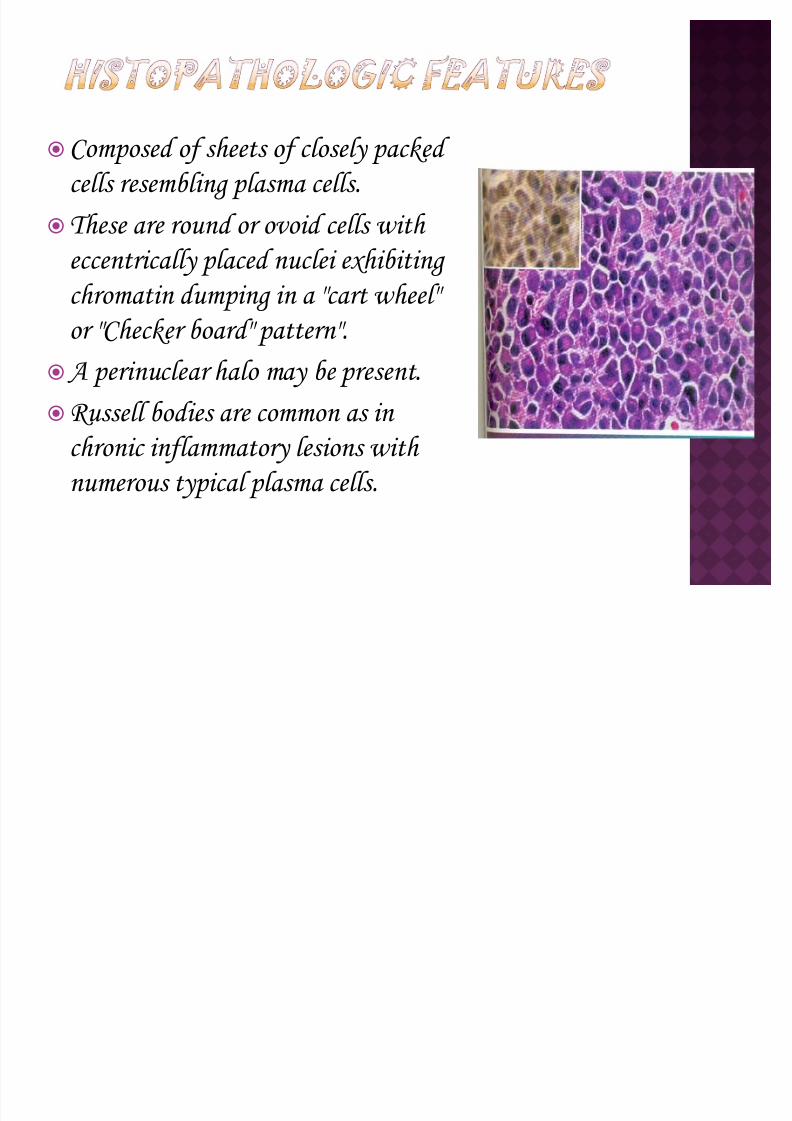
Composed of sheets of closely packed cells resembling plasma cells.
These are round or ovoid cells with
eccentrically placed nuclei exhibiting
chromatin dumping in a "cart wheel"
or "Checker board" pattern".
A perinuclear halo may be present.
R ussell bodies are common as in chronic inflammatory lesions with
numerous typical plasma cells.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 41/77
Chemotherapy -treatment of choice.
R adiation therapy also used, often in combination with
chemotherapy.
Unfortunately, the prognosis is poor, with the median
survival time being two to three years.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 42/77
A lso called Histiocytosis X, Eosinophilic granuloma, Langerhans
cell Granuloma.
It includes a spectrum of clinicopathologic disorders characterized
by proliferation of histiocyte-like cells that are accompanied by varying numbers of eosinophils, lymphocytes, plasma cells and
multinucleated giant cells.
The distinctive histiocyte-like cells present in this lesion are called
Langerhans cells and the condition as Langerhans cells Histiocytosis.
Langerhans cells are dendritic mononuclear cells normally found in
the epidermis, lymph nodes and bone marrow.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 43/77
Primarily occurs in older children and young adults.
Male to female ratio is 2:1
The clinicopathologic spectrum includes the following.
Monostotic or polyostotic eosinophilic granuloma of bone- Solitary or multiple bone lesions without visceral
involvement.
Chronic Disseminated Histiocytosis- A disease involving bone, skin and viscera (Hand-
Schuller Christian disease). A cute Disseminated Histiocytosis:- A disease with prominent cutaneous, visceral and
bone marrow involvement occurring mainly in infants. (Letterer-Siwe disease).
l ll h l h l

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 44/77
Clinically, the lesion may present no physical signs or
symptoms and may be found only upon on incidental
radiographic examination of bones of the head or other areas.
On the other hand, there may be local pain, swelling and tenderness.
The lesion may occur in the jaw and overlying soft tissues of
mouth.
A lthough the skull and mandible are common sites of involvement the femur, humerus, ribs and other bones may
also be affected.
General malaise and fever.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 45/77
The lesions are destructive and are well demarcated, roughly
round or oval in shape.
The area destroyed is replaced by soft tissue, the composition of
which varies, depending upon the stage at which the lesion is
examined.
The tissue of early lesion is soft and brown and, since there is
no necrosis, is not friable.
Later the lesion becomes fibrous and the grayish.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 46/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 47/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 48/77
Periodontal disease ² the epicenter of bone destruction in LCH is approximately in the midroot region. In contrast the bone
destruction in periodontal disease starts at the alveolar crest
and extends apically down the root surface.
Squamous cell carcinoma ² the borders of LCH lesion are typically well defined.
Simple bone cysts ² the alveolar crest is maintained in simple
bone cysts and a partial cortex may be present.
Solitary intraosseous lesions ² differentiated by well defined borders and the periosteal reaction seen in Histiocytosis.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 49/77
Diffuse infiltration of large, pale- staining mono-nuclear cells that resemble histiocyte.
Indistinct cytoplasmic borders
and rounded or indented vesicular nuclei.
V arying numbers of eosinophils are typically interspersed among the histiocyte-like cells.
Plasma cells, lymphocytes and multinucleated giant cells are often seen, and areas of necrosis and hemorrhage may be present.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 50/77
A ccessible bone lesions, such as those in the maxilla and
mandible -treated by curettage.
Low doses of radiation -for less accessible bone lesion
Intralesional injection with corticosteroids in case of
localized bone lesions.
The Prognosis for bone lesions in the absence of
significant visceral involvement is generally good.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 51/77
A lso called as Epidermoid carcinoma .
Most common oral malignancy which may be defined as a
malignant tumor arising from surface epithelium.
Characterized initially by invasion of malignant epithelial cells
into the underlying connective tissue with subsequent spread into
deeper soft tissues, adjacent bone, local regional lymph nodes and ultimately to distant sites such as the lung, liver and skeleton.
8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 52/77
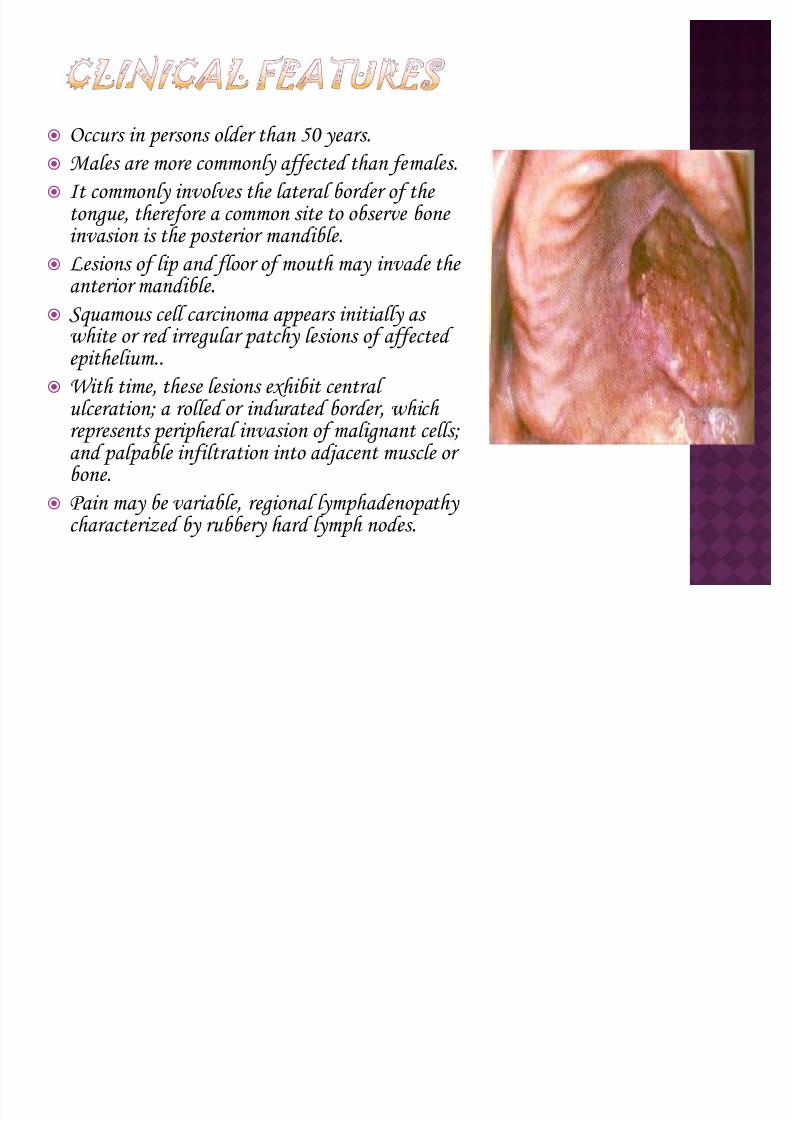
Occurs in persons older than 50 years. Males are more commonly affected than females.
It commonly involves the lateral border of the tongue, therefore a common site to observe bone invasion is the posterior mandible.
Lesions of lip and floor of mouth may invade the
anterior mandible. Squamous cell carcinoma appears initially as
white or red irregular patchy lesions of affected epithelium..
With time, these lesions exhibit central ulceration; a rolled or indurated border, which represents peripheral invasion of malignant cells; and palpable infiltration into adjacent muscle or bone.
Pain may be variable, regional lymphadenopathy characterized by rubbery hard lymph nodes.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 53/77
Other clinical features include a soft tissue mass,
paraesthesia, anesthesia, dysesthesia, pain, foul smell,
trismus, grossly loosened teeth or hemorrhage.
Large lesions can obstruct the airway, Eustachian tube or
the nasopharynx.
Patients often report a significant weight loss and feel unwell

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 54/77
Squamous cell carcinoma may erode into underlying bone from any direction, producing a radiolucency that is polymorphous and
irregular in outline.
If bone involvement is extensive the periphery appears to have finger like extension preceding a zone of osseous destruction.
Sclerosis in underlying osseous structures may be seen in
association with erosions from surface carcinomas.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 55/77
Evidence of invasion of bone around teeth may first
appear as widening of periodontal ligament space with loss of adjacent lamina dura.
Teeth may appear to float in a mass of radiolucent soft
tissue.
Destruction of adjacent normal cortical boundaries such
as the floor of the nose, maxillary sinus or Buccal or
lingual Mandibular plate may occur.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 56/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 57/77
It is characterized by invasive islands and cords of malignant squamous epithelial cells.
Invasion is represented by irregular extension of lesional epithelium through the basement
membrane and into subepithelial connective tissue.
Individual squamous cells and sheets or islands of cells appear as individual entities within connective tissue. They may extend deeply into underlying adipose tissue, muscle
or bone. The lesional cells generally show abundant
eosinophilic cytoplasm with large, often darkly staining nuclei and increased nuclear- to-cytoplasmic ratio.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 58/77
Combination of surgery and radiation therapy. The choice of treatment depends upon the protocol of the treating
centre and the location and severity of the tumor.
Generally, if an adequate margin of normal tissue can be obtained,surgery is the usual treatment, followed by radiation treatment.
A n alternative is to use radiation as the primary treatment followed by surgical salvage.
Currently, chemotherapy is used as an adjunct to either radiation or surgical treatment.
The prognosis for survival depends upon tumor stage. The 5-year disease free survival rate for intraoral carcinoma is 76% if metastasis has not occurred at the time of diagnosis (stage1 and II), 41% when cervical nodes are involved (stageIII) and 9% when metastasis below clavicle is present.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 59/77
A lso called Primary intraosseous carcinoma, intra alveolar
carcinoma or central mandibular carcinoma.
Primary intraosseous carcinoma is a squamous cell carcinoma arising within the jaw that has no original
connection with the surface epithelium of oral mucosa.
It is presumed to arise from intraosseous remnants of the odontogenic epithelium.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 60/77
These neoplasms are rare and may remain silent until they have reached a fairly large state.
It mainly occurs in fourth to eighth decades of life and more
common in males.
The mandible is far more commonly involved than maxilla.Posterior region are involved more frequently than anterior
region.
A s the lesion is associated with remnants of dental lamina, it
originates only in tooth bearing parts of jaw. The surface epithelium is invariably normal in appearance.
Pain, pathologic fracture, and sensory nerve abnormalities such
as lip paraesthesia and lymphadenopathy

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 61/77
The periphery of majority of lesions is ill- defined, although some may be well defined.
They are most often rounded or irregular in shape and have a border that demonstrates osseous destruction and varying degrees of extension
at periphery. The degree of raggedness of the border may reflect the aggressiveness of
lesion.
The internal structure is wholly radiolucent with no evidence of bone production and very little residual bone left within the centre of the lesion.
These lesions are capable of causing destruction of antral or nasal floors, loss of cortical outline of the mandibular canal and effacement of the lamina dura. R oot resorption is unusual.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 62/77
If the lesions are not aggressive and have a smooth border
and radiolucent area they may be mistaken for Periapical
cysts and granuloma.
If the lesions are not centered about the apex of a tooth,
then it is difficult to differentiate from odontogenic cysts
and tumors.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 63/77
It is characterized by invasive islands and cords of
malignant squamous epithelial cells.
The lesional cells generally show abundant eosinophilic cytoplasm with large, often darkly staining nuclei and
increased nuclear-to-cytoplasmic ratio.
V arying degree of cellular and nuclear pleomorphism is seen. Keratin pearls may be produced into lesional cells.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 64/77
Generally, these tumors are excised with their surrounding
osseous structure in an en-bloc resection.
R adiation and chemotherapy can be used as adjunctive
therapies.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 65/77
A lso called as Epidermoid cell carcinoma or ex odontogenic
cyst.
This condition may arise from inflammatory, Periapical,
residual, dentigerous and odontogenic keratocysts.
Histologically, the lining squamous epithelium of the cyst gives rise to the malignant neoplasm.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 66/77
This tumor may occur anywhere an odontogenic cyst is found,namely, tooth-bearing portions of the jaws.
Most cases occur in the mandible, with a few cases reported in
the anterior maxilla.
The most common presenting sign or symptom associated with condition is pain. The pain may be characterized as dull and of
several months duration.
Swelling is occasionally reported.
Pathologic fracture may occur, as may fistula formation and regional lymphadenopathy.
If the upper jaw is involved, sinus pain or swelling may be
present

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 67/77
A s the lesion arises from a cyst, the shape is often round or ovoid.
If it is a small lesion in the cyst wall, the periphery may be mostly
well defined and even corticated. A s the malignant tissue
progressively replaces cyst lining, the smooth border is lost or becomes ill-defined.
The advanced lesion has an ill-defined, infiltrative periphery that
lacks any cortication.
It is capable of thinning and destroying the lamina dura of adjacent teeth or adjacent cortical boundaries such as inferior border of jaw or
floor of the nose.
It may result in complete destruction of the alveolar process.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 68/77
If a dental cyst is infected, it may loose its corticated
boundary and appear ragged and identical to a malignant
lesion arising in a preexisting cyst. However inflamed
cysts usually show a reactive Periapical sclerosis, this is
not normally present in a cyst which has undergone
malignant transformation..

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 69/77
It is characterized by invasive islands and cords of
malignant squamous epithelial cells.
The lesional cells generally show abundant eosinophilic
cytoplasm with large, often darkly staining nuclei and
increased nuclear-to-cytoplasmic ratio.
V arying degree of cellular and nuclear pleomorphism is
seen. Keratin pearls may be produced into lesional cells.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 70/77
Generally, these tumors are excised with their surrounding
osseous structure in an en-bloc resection.
R adiation and chemotherapy may be used as adjunctive
therapies.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 71/77
Melanoma is a malignant lesion of melanocytic origin that
arises from a benign melanocytic lesion or de novo.
The mucosal melanoma tends to appear at higher stage and is more aggressive.
Melanoma usually affects parotid gland, usually as a
metastatic deposit from scalp, conjuctival or paranasal tumor.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 72/77
Sixth or seventh decade of life.Males are commonly affected than females.
Four of every five oral melanomas are found on the hard palate
or maxillary alveolus.
A n oral lesion typically begins as a brown to black macule with irregular borders.
The macule extends laterally, and a lobulated, exophytic mass
develops once the vertical growth is initiated.
Ulceration may develop early, but many lesions are dark,
lobulated, exophytic masses without ulceration at the time of
diagnosis.
Pain is not a common feature except in ulcerated lesion

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 73/77

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 74/77
The tumor consists of radiolucency with ill-defined
margins.
There is lytic bone destruction.
The borders are irregular giving it a characteristic
´MOTH-E A TEN µ appearance.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 75/77
A malgam tattoo
Oral melanoticmacule
Melanocytic hyperplasia Focal hemosiderin deposit
Local patch of melanoplakia

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 76/77
Melanomas consist of neoplastic
melanocytes often surrounded by clear
halo, both within the epithelium and
invading deeper tissues.
These cells are round to spindle shaped
and typically speckled or intensely
pigmented with melanin.
In the early stages of the neoplasm,
atypical melanocytes are seen scattered
singly among basal epithelial cells or
nests within basal cell layer.
In later stages malignant melanocytes
are seen invading the connective tissue.

8/8/2019 Malignant Bone Neplasms
http://slidepdf.com/reader/full/malignant-bone-neplasms 77/77
Surgical excision is the only curative treatment.
For small early tumors, surgical margins of 1 cm are necessary to achieve control. However, for larger and deeply invasive tumors, wide surgical excision is
recommended. It may metastasize to regional lymph nodes, so surgical
excision of regional lymph nodes is recommended.
R adiation therapy has no significant impact; however
chemotherapy and immunotherapy can be used as an adjunct.
The prognosis is extremely poor. Young patients have a better survival than older ones.


















