MALIGNANT ARRHYTHMIAS: ECG IDENTIFICATION DR.SIVAKUMAR ARDHANARI MD @gmail.com.
60
MALIGNANT ARRHYTHMIAS: MALIGNANT ARRHYTHMIAS: ECG IDENTIFICATION ECG IDENTIFICATION DR.SIVAKUMAR ARDHANARI MD DR.SIVAKUMAR ARDHANARI MD www.anaesthesia.co.in [email protected]
-
Upload
quentin-oneal -
Category
Documents
-
view
216 -
download
1
Transcript of MALIGNANT ARRHYTHMIAS: ECG IDENTIFICATION DR.SIVAKUMAR ARDHANARI MD @gmail.com.

MALIGNANT ARRHYTHMIAS:MALIGNANT ARRHYTHMIAS:ECG IDENTIFICATIONECG IDENTIFICATION
DR.SIVAKUMAR ARDHANARI DR.SIVAKUMAR ARDHANARI MDMD
www.anaesthesia.co.in [email protected]


Normal sinus rhythmNormal sinus rhythm
Impulse formation beginning in the Impulse formation beginning in the sinus nodesinus node
At frequencies between 60 to 100 per At frequencies between 60 to 100 per minuteminute
P is always upright in I, II and aVF and P is always upright in I, II and aVF and inverted in aVRinverted in aVR
Though rhythm is regular, minor Though rhythm is regular, minor variation in PP interval exists & variation in PP interval exists & longest and shortest PP differ< 0.16 longest and shortest PP differ< 0.16 except in sinus arrhythmiaexcept in sinus arrhythmia

Normal sinus rhythmNormal sinus rhythm
Every P is followed by a QRS complexEvery P is followed by a QRS complex Every QRS is preceded by a P waveEvery QRS is preceded by a P wave P and its following QRS is separated P and its following QRS is separated
by fairly regular PR intervalby fairly regular PR interval TO BE VERY PRECISE P AND QRS ARE TO BE VERY PRECISE P AND QRS ARE
IN SIMPLE HARMONYIN SIMPLE HARMONY


NORMAL ECGNORMAL ECG
When the rhythm deviates from the When the rhythm deviates from the above said normalcy it is called above said normalcy it is called ARRHYTHMIAARRHYTHMIA
Broadly it is classified as brady and Broadly it is classified as brady and tachy arrhythmiatachy arrhythmia
Arrhythmogenesis may be due Arrhythmogenesis may be due various causesvarious causes


Some arrhythmias are considered Some arrhythmias are considered MALIGNANT MALIGNANT
Because if not properly and Because if not properly and immediately treated, it can be immediately treated, it can be LETHAL to the suffererLETHAL to the sufferer
This is important in understanding This is important in understanding the concept of SUDDEN CARDIAC the concept of SUDDEN CARDIAC DEATHDEATH
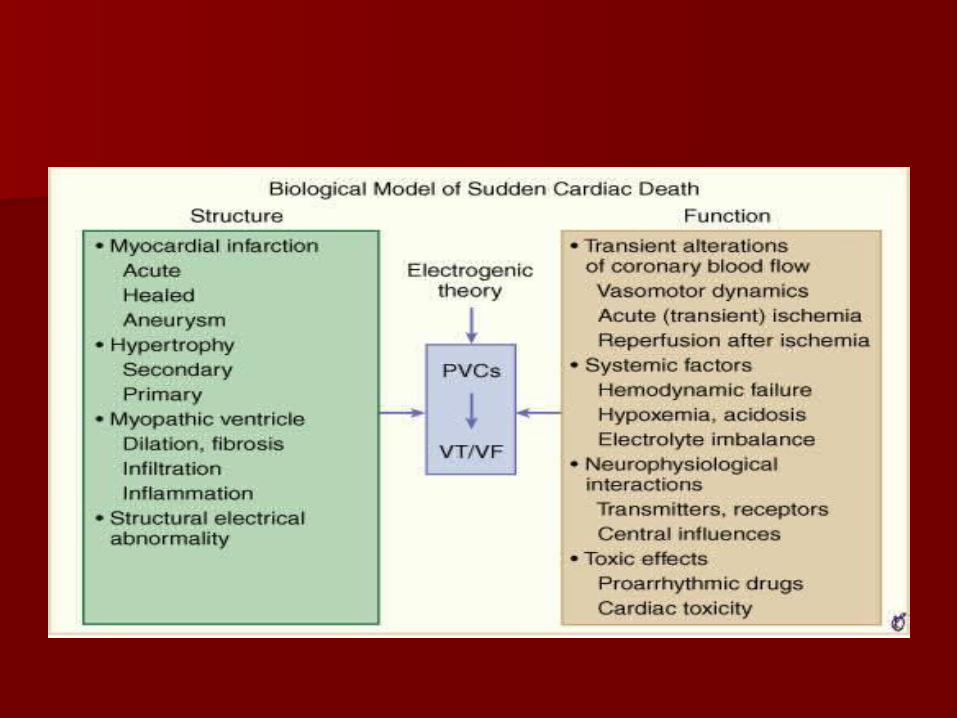

SUDDEN CARDIAC DEATHSUDDEN CARDIAC DEATH

Anatomy of the conduction Anatomy of the conduction systemsystem

Anatomy of the conduction Anatomy of the conduction systemsystem
Sinus node- Sinus node- – RCA (55-60%) RCA (55-60%) – left circumflex (40-45%)arteryleft circumflex (40-45%)artery
AV node-AV node-– RCA (85-90%) RCA (85-90%) – left circumflex (10-15%) arteryleft circumflex (10-15%) artery

ACUTE RVMI+IWMIACUTE RVMI+IWMI
Anatomy of conduction Anatomy of conduction systemsystem
The conduction system is densely The conduction system is densely innervated byinnervated by – Cholinergic fibers- parasympathetic Cholinergic fibers- parasympathetic – Adrenergic fibers- sympatheticAdrenergic fibers- sympathetic
This is important in understanding This is important in understanding – variability of cardiac function with variability of cardiac function with
autonomic influence autonomic influence – effect of parasympathetic stimulation in effect of parasympathetic stimulation in
terminating arrhythmiasterminating arrhythmias

BRADYARRHYTHMIASBRADYARRHYTHMIAS Sinus nodalSinus nodal
Sinus bradycardiaSinus bradycardia Sinus arrhythmiaSinus arrhythmia Sinus pause/arrestSinus pause/arrest Sinoatrial exit blockSinoatrial exit block Sick sinus syndromeSick sinus syndrome
AV nodal blocksAV nodal blocks First degreeFirst degree Second degree(MOBITZ type 1 and 2)Second degree(MOBITZ type 1 and 2) Complete heart blockComplete heart block

SINUS ARRESTSINUS ARREST

SICK SINUS SYNDROMESICK SINUS SYNDROME
ATRIO VENTRICULAR BLOCKATRIO VENTRICULAR BLOCK I degree I degree -conduction time prolonged: all impulses -conduction time prolonged: all impulses
are conductedare conducted
II degreeII degree -2 forms -2 forms
o Mobitz type I (WENCKEBACH)-Mobitz type I (WENCKEBACH)- progressive lengthening of progressive lengthening of conduction time until an impulse is failed to be conductedconduction time until an impulse is failed to be conducted
o Mobitz type II-Mobitz type II- occasional or repetitive sudden block in occasional or repetitive sudden block in conduction without prior measurable lengthening of conduction without prior measurable lengthening of conduction timeconduction time
Complete or III degreeComplete or III degree -no impulses are conducted -no impulses are conducted
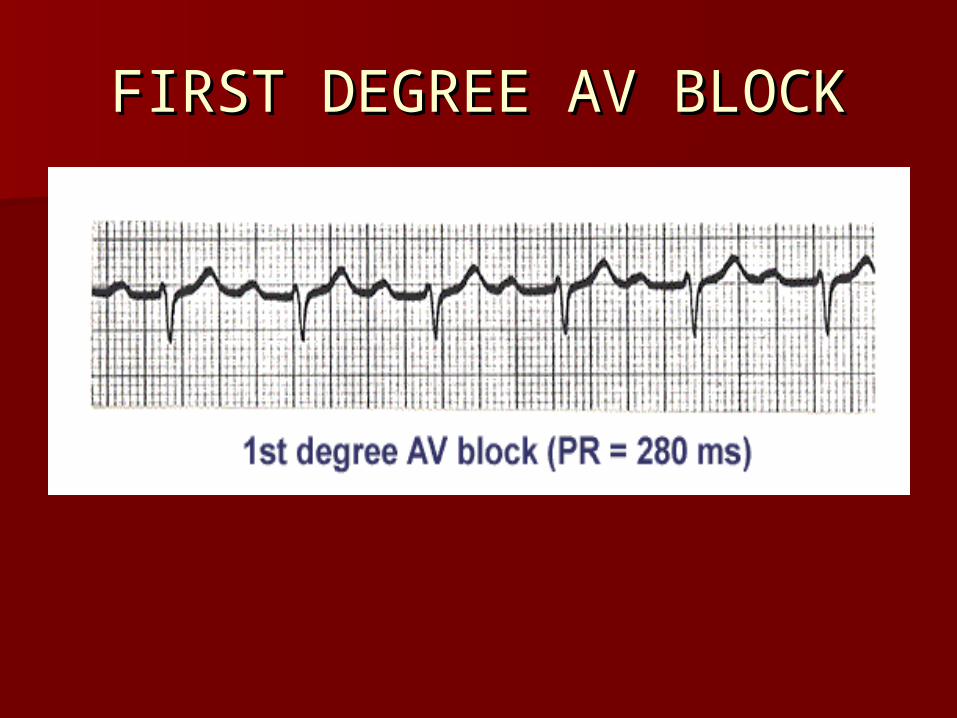
FIRST DEGREE AV BLOCKFIRST DEGREE AV BLOCK

FIRST DEGREE HBFIRST DEGREE HB
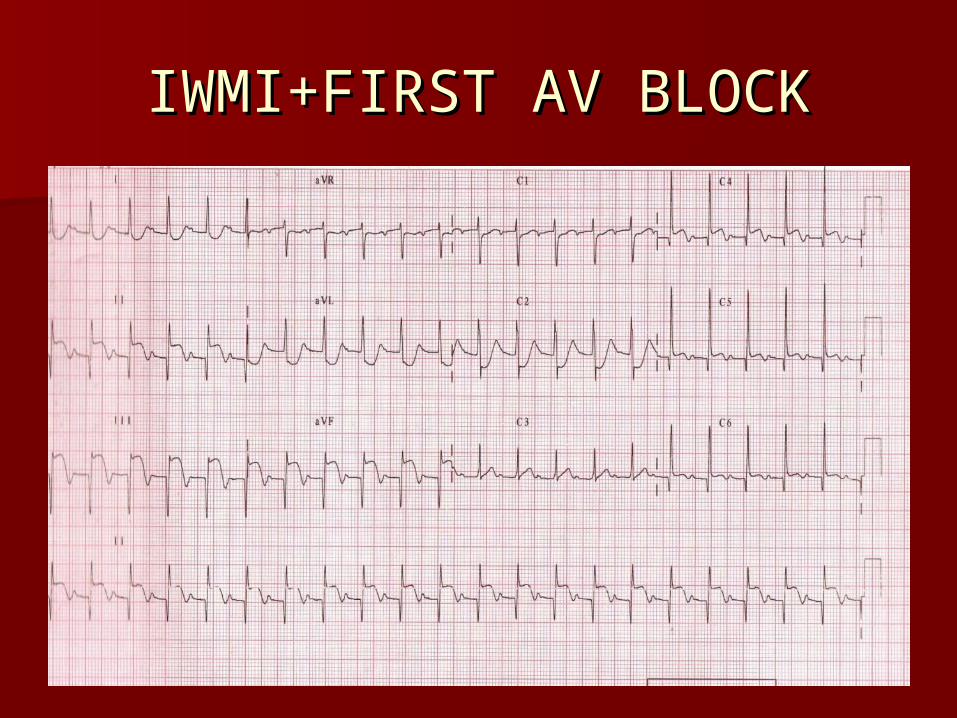
IWMI+FIRST AV BLOCKIWMI+FIRST AV BLOCK
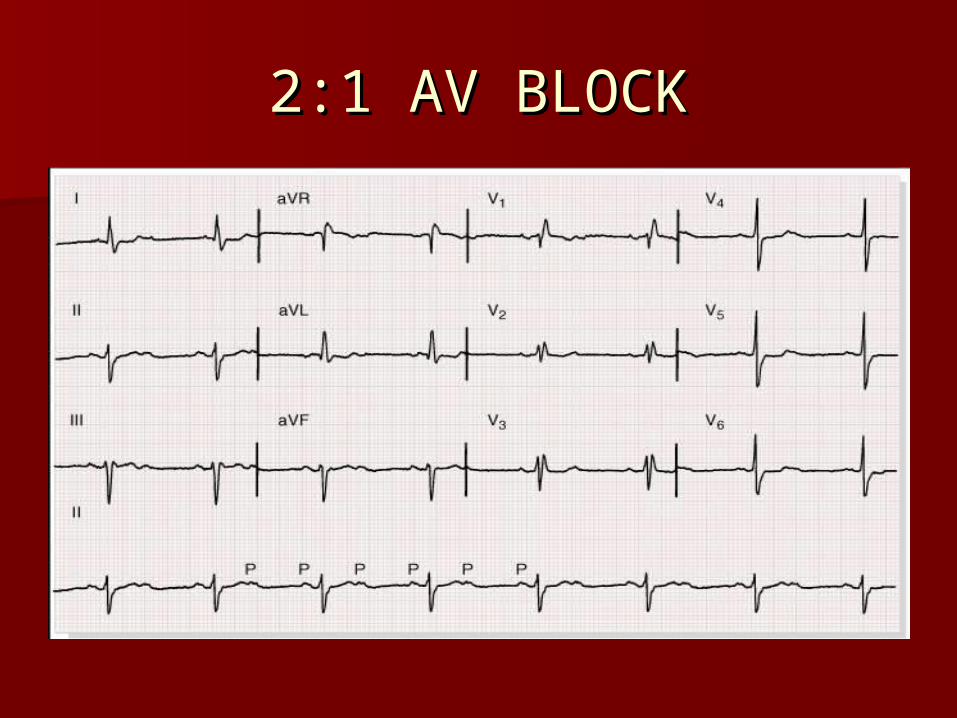
2:1 AV BLOCK2:1 AV BLOCK

COMPLETE AV BLOCKCOMPLETE AV BLOCK
Occurs when no atrial activity is Occurs when no atrial activity is conducted to the ventriclesconducted to the ventricles
So atria and ventricles are controlled So atria and ventricles are controlled by independent pacemakersby independent pacemakers
One type of complete AV dissociationOne type of complete AV dissociation Ventricular focus is usually just below Ventricular focus is usually just below
the site of blockthe site of block If focus near HIS bundle the rhythm If focus near HIS bundle the rhythm
is more stableis more stable
CHB can occur at various levelsCHB can occur at various levels– AV Node-usually congenital-40-60 AV Node-usually congenital-40-60
bpmbpm– Bundle of HISBundle of HIS– Purkinje sys-usually acquired-Purkinje sys-usually acquired-

COMP HEART BLOCKCOMP HEART BLOCK
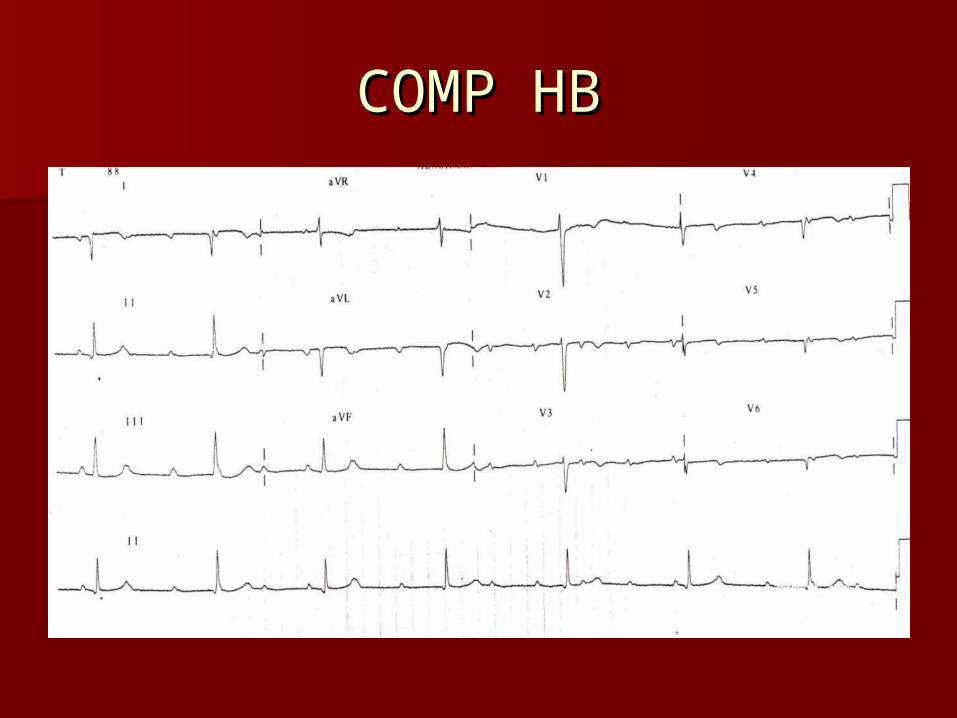
COMP HBCOMP HB

CHBCHB

CHBCHB
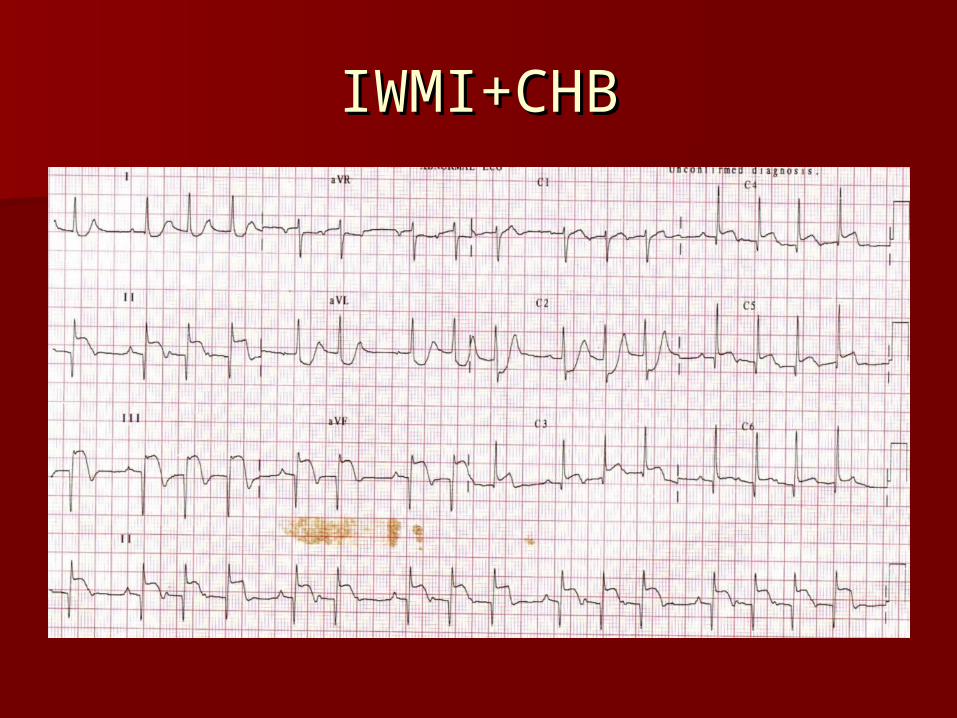
IWMI+CHBIWMI+CHB

APPROACH TO APPROACH TO TACHYCARDIATACHYCARDIA

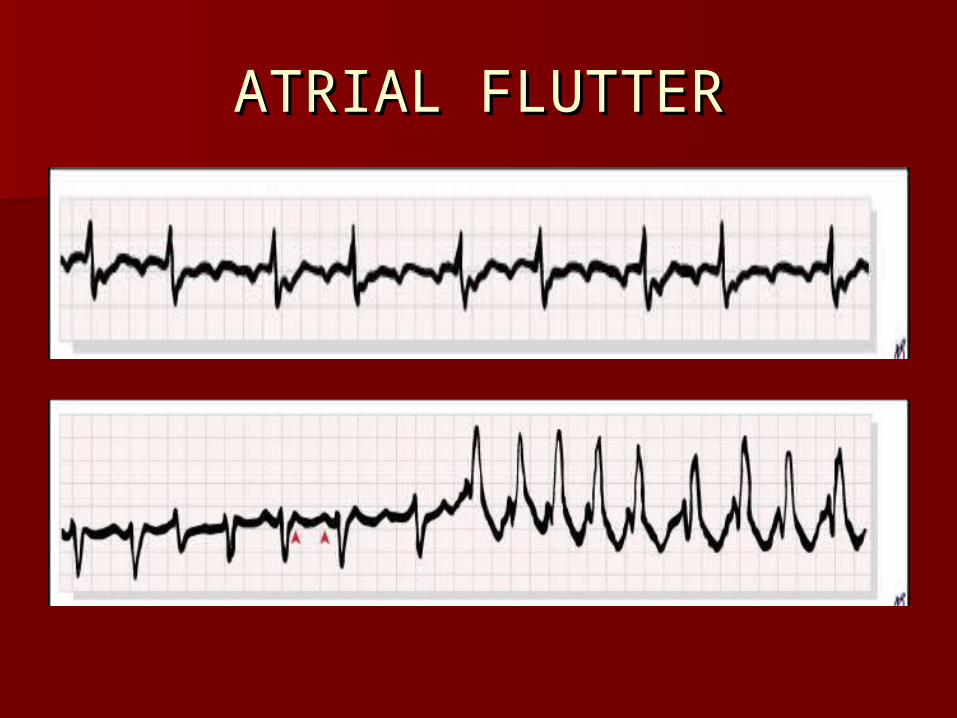
ATRIAL FLUTTERATRIAL FLUTTER
F waves: rapid regular undulationsF waves: rapid regular undulations
SAW TOOTH APPEARANCESAW TOOTH APPEARANCE Atrial rate:250-350 bpmAtrial rate:250-350 bpm Rate & regularity of ventricles: variable Rate & regularity of ventricles: variable
and depend on AV conduction and depend on AV conduction sequencesequence
QRS may be normal or abnormal as a QRS may be normal or abnormal as a result of preexisting intraventricular result of preexisting intraventricular conduction defect or aberrancyconduction defect or aberrancy

ATRIAL FLUTTERATRIAL FLUTTER
ATRIAL FLUTTERATRIAL FLUTTER

ATRIAL FLUTTERATRIAL FLUTTER


SVT VS VTSVT VS VT
Differentiating a VT from SVT can be Differentiating a VT from SVT can be difficult at timesdifficult at times
Golden rule in ER Golden rule in ER
ANY WIDE QRS TACHYCARDIA IS ANY WIDE QRS TACHYCARDIA IS VENTRICULAR TACHYCARDIA VENTRICULAR TACHYCARDIA UNTIL PROVED OTHERWISE UNTIL PROVED OTHERWISE ESP`LY WHEN THE PATIENT HAS ESP`LY WHEN THE PATIENT HAS A STRUCTURAL HEART DISEASEA STRUCTURAL HEART DISEASE

Diagnosis of VTDiagnosis of VT
Arises distal to the bifurcation of the Arises distal to the bifurcation of the HIS bundleHIS bundle
Diagnosis is by the occurrence of a Diagnosis is by the occurrence of a series of 3 or more consecutive, series of 3 or more consecutive, abnormally shaped PVCs whose abnormally shaped PVCs whose duration exceeds 120 ms, with ST-T duration exceeds 120 ms, with ST-T vector pointing opposite the major vector pointing opposite the major QRS deflectionQRS deflection

VENTRICULAR ECTOPICSVENTRICULAR ECTOPICS
RR can be exceedingly regular or can RR can be exceedingly regular or can varyvary
Atrial activity can be independent of Atrial activity can be independent of ventricular activity or can be ventricular activity or can be depolarized retrograde (VA depolarized retrograde (VA association)association)

Fusion beats and capture beats provide the Fusion beats and capture beats provide the maximum support for the diagnosis of VTmaximum support for the diagnosis of VT
FUSION BEATS-activation of ventricles from FUSION BEATS-activation of ventricles from 2 foci2 foci
CAPTURE BEATS- capture of the ventricle CAPTURE BEATS- capture of the ventricle by supraventricular rhythmwith normal by supraventricular rhythmwith normal confguration of the captured QRS at intrvl confguration of the captured QRS at intrvl shorter than tachycardia in question- shorter than tachycardia in question- indicates origin of impulse is indicates origin of impulse is supraventricularsupraventricular

FUSION AND CAPTURE FUSION AND CAPTURE BEATSBEATS

QRS contours can be QRS contours can be – Unchanging (MONOMORPHIC)Unchanging (MONOMORPHIC)– Vary randomly (POLY OR PLEOMORPHIC)Vary randomly (POLY OR PLEOMORPHIC)– Vary repetitively (TORSADES DE Vary repetitively (TORSADES DE
PONTES)PONTES)– Vary in alternative cplxs Vary in alternative cplxs
(BIDIRECTIONAL)(BIDIRECTIONAL)

MONOMORPHIC VTMONOMORPHIC VT

POLYMORPHIC VTPOLYMORPHIC VT

TORSADES DE POINTESTORSADES DE POINTES
TYPES OF VTTYPES OF VT
VT can beVT can be SUSTAINED- lasting longer than 30 SUSTAINED- lasting longer than 30
seconds or requiring termination due seconds or requiring termination due to hemodynamic collapseto hemodynamic collapse
NON SUSTAINED- stops NON SUSTAINED- stops spontaneously within 30 secondsspontaneously within 30 seconds

NON-SUSTAINED VTNON-SUSTAINED VT

SUSTAINED VTSUSTAINED VT

HYPER ACUTE EXT ALMIHYPER ACUTE EXT ALMI
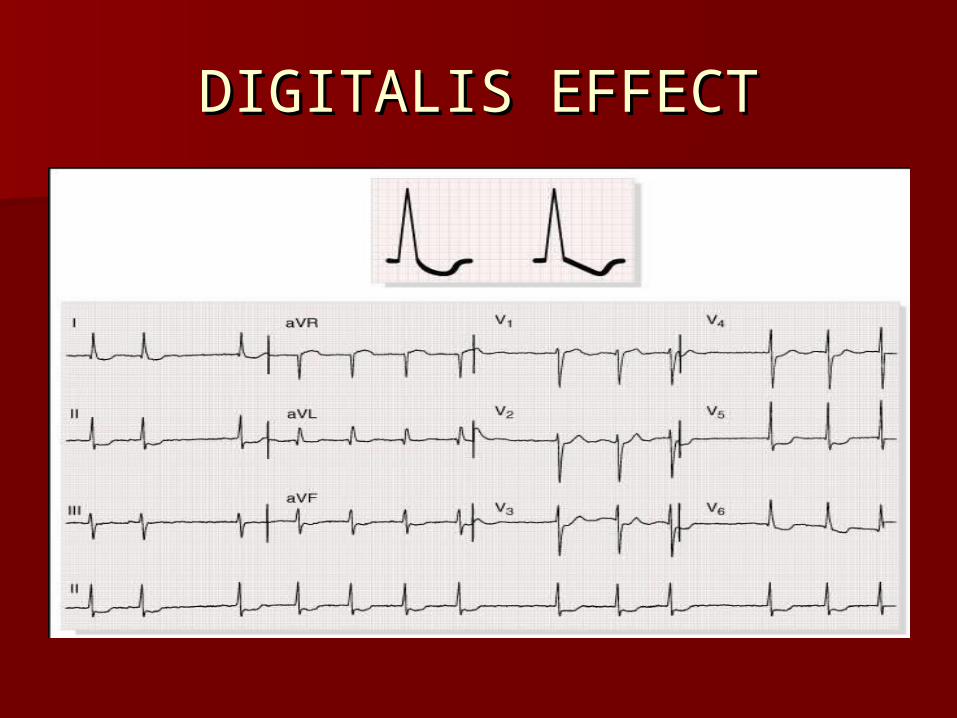
DIGITALIS EFFECTDIGITALIS EFFECT
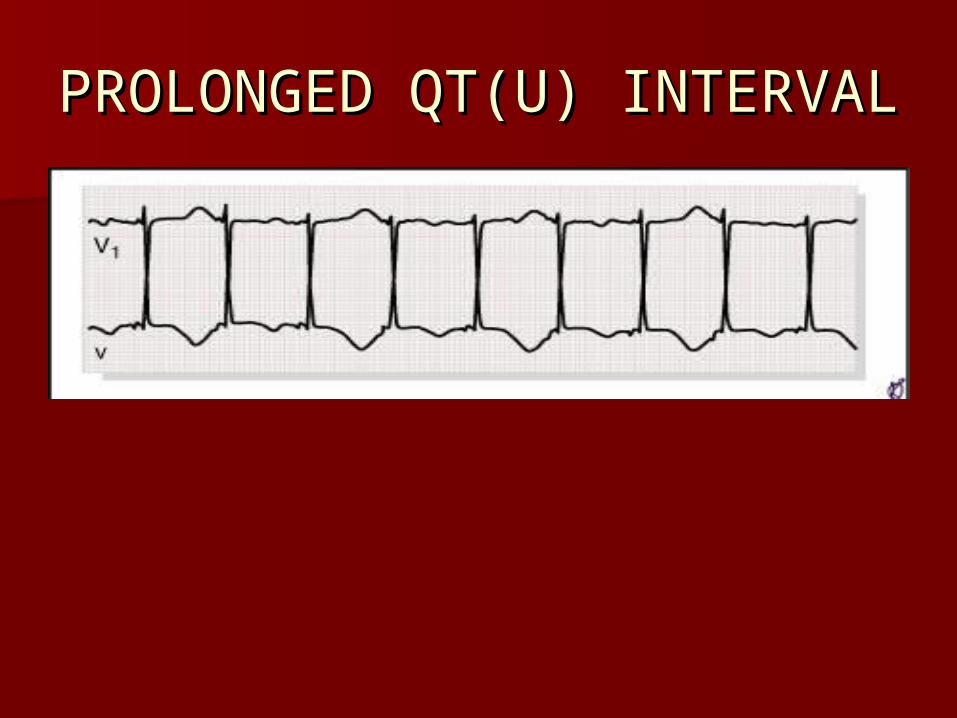
PROLONGED QT(U) PROLONGED QT(U) INTERVALINTERVAL

Ventricular flutter & Ventricular flutter & fibrillationfibrillation
Represent severe Represent severe derangement of heart beat derangement of heart beat that usually terminate fatally that usually terminate fatally within 3-5 mts if corrective within 3-5 mts if corrective measures are not undertaken measures are not undertaken promptly.promptly.

VENTRICULAR FLUTTERVENTRICULAR FLUTTER
Manifested as sine wave in Manifested as sine wave in appearanceappearance
Regular large oscillations occurring Regular large oscillations occurring at a rate of 150-300(usually 200)/minat a rate of 150-300(usually 200)/min

VENTRICULAR FLUTTERVENTRICULAR FLUTTER

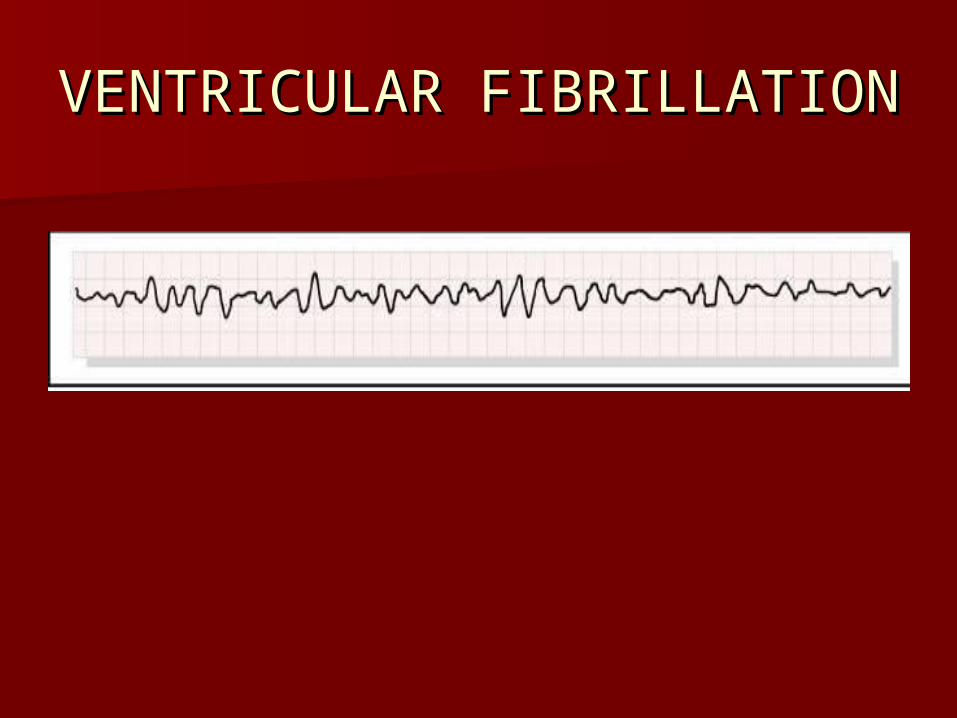
VENTRICULAR FIBRILLATIONVENTRICULAR FIBRILLATION
Irregular undulations of varying Irregular undulations of varying contour & amplitudecontour & amplitude
Distinct QRS, ST or T are absentDistinct QRS, ST or T are absent Fine amplitude fibrillatory waves Fine amplitude fibrillatory waves
(0.2mV) with prolonged VF: worse (0.2mV) with prolonged VF: worse prognosis: confused with asystoleprognosis: confused with asystole
VENTRICULAR FIBRILLATIONVENTRICULAR FIBRILLATION