Making Laparoscopic Myomectomy Safe - thetrocar.com · Making Laparoscopic Myomectomy Safe...
11
Making Laparoscopic Myomectomy Safe Laparoscopic myomectomy has provided minimal invasive alternative to laparotomy for subserous and intramural myomas 1,2 . It is no longer a subject of debate 2,3 Though opinion may differ in cases of large & multiple myomas among the endoscopist 2 . Number of instruments & various angles of insertion to approach surgical site are limited & therefore myomas may be technically difficult to remove laparoscopically but with experience , sound knowledge of suturing & acquiring greater skill over a period of time one can overcome these technical difficulties 4 . It is always wise to start with smaller,singular & subserous than deep intramural or multiple myomas. As experience increases the exclusion criteria relaxes considerably & one proceeds for more complicated cases. The comfort level expands. More one does, more number of patients he/she will be able to count as good candidates as one becomes adapt at managing large &/or multiple myomas. It is important for surgeon to know that safety of patient is more important than type of surgery (laparoscopic or open) 5 . Hence before proceeding for laparoscopic surgery it is mandatory for the surgeon to ask himself/herself – ‘Is it possible for me to give the best of the result by laparoscopy in this patient with my setup and experience?’ and then proceed accordingly Pre-operative Requisites : A thorough ultrasonographic evaluation of pelvis for location, size & number of myomas is a must 6,7 . In laparoscopic surgery tactile sensation is lacking. In cases of large & multiple myomas it is better to have a limited MRI of pelvis done as surgeon can decide pre- operatively his incision sites, number of incisions , how many myomas can be removed via one incision & relation of myomas with uterine cavity. Though after putting a laparoscope one needs to re-evaluate his/her own pre-operative decisions. Head of Department, Dept. of Obstetrics and Gynecology Chief, IVF and Endoscopy Centre,Ruby Hall Clinic, Pune Elected Board Member, ISGE (2013-2017) Executive Board Member, IAGE Librarian , ISAR Founder Secretary Maharashtra Chapter, ISAR Co-Chairperson Research Committee of ISAR FOGSI Infertility Committee Chairperson ( 2011-2013 ) Reviewer, Fertility and Sterility Reviewer, Journal of Human Reproductive Sciences. Dr. Sunita Tandulwadkar MD, FICS, FICOG
Transcript of Making Laparoscopic Myomectomy Safe - thetrocar.com · Making Laparoscopic Myomectomy Safe...

Making Laparoscopic Myomectomy Safe
Laparoscopic myomectomy has provided minimal invasive alternative to laparotomy
for subserous and intramural myomas1,2
. It is no longer a subject of debate2,3
Though opinion
may differ in cases of large & multiple myomas among the endoscopist
2. Number of
instruments & various angles of insertion to approach surgical site are limited & therefore
myomas may be technically difficult to remove laparoscopically but with experience , sound
knowledge of suturing & acquiring greater skill over a period of time one can overcome these
technical difficulties4.
It is always wise to start with smaller,singular & subserous than deep intramural or
multiple myomas. As experience increases the exclusion criteria relaxes considerably & one
proceeds for more complicated cases. The comfort level expands. More one does, more
number of patients he/she will be able to count as good candidates as one becomes adapt at
managing large &/or multiple myomas. It is important for surgeon to know that safety of
patient is more important than type of surgery (laparoscopic or open)5. Hence before
proceeding for laparoscopic surgery it is mandatory for the surgeon to ask himself/herself –
‘Is it possible for me to give the best of the result by laparoscopy in this patient with
my setup and experience?’ and then proceed accordingly
Pre-operative Requisites :
A thorough ultrasonographic evaluation of pelvis for location, size & number of
myomas is a must 6,7
. In laparoscopic surgery tactile sensation is lacking. In cases of large &
multiple myomas it is better to have a limited MRI of pelvis done as surgeon can decide pre-
operatively his incision sites, number of incisions , how many myomas can be removed via
one incision & relation of myomas with uterine cavity. Though after putting a laparoscope
one needs to re-evaluate his/her own pre-operative decisions.
Head of Department, Dept. of Obstetrics and Gynecology
Chief, IVF and Endoscopy Centre,Ruby Hall Clinic, Pune
Elected Board Member, ISGE (2013-2017)
Executive Board Member, IAGE
Librarian , ISAR
Founder Secretary Maharashtra Chapter, ISAR
Co-Chairperson Research Committee of ISAR
FOGSI Infertility Committee Chairperson ( 2011-2013 )
Reviewer, Fertility and Sterility
Reviewer, Journal of Human Reproductive Sciences.
Dr. Sunita Tandulwadkar MD, FICS, FICOG

It is advised to perform hysteroscopy in all cases of multiple myomas before
proceeding for laparoscopic myomectomy 8 as smaller submucosal myomas can be missed
out in presence of large & multiple myomas.
Practical tips of myomectomy
Thorough preoperative preparation can improve his/her intraoperative performance.
The following aspects should be well planned in mind by the surgeon well before the start of
surgery:
Trocar entry
Inspection and assessment of the myoma(s).
Direction of the incision
Energy source to be used
Enucleation technique
Closure of the myoma bed
Extraction
Adhesion prevention
1a. 1b.
1c. 1d. 1e.
Fig 1 a-e: Preoperative imaging is essential to know the size, number,
location and relation of the myomas to each other and to the cavity.

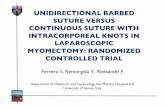
Trocar Entry: Port Placement
Port placement depends upon size of myoma, its location and total number of myomas
4. It is always wise to shift upwards towards upper abdomen as the size of myoma increases,
so as to ensure a good panaromic view.
Ancillary ports have to be taken in such a way that one can reach to the myoma
without making acute angles with each other. If necessary apart from 3 ancillary ports one
can add on more ports especially in cases of large and multiple myomas as these myomas
with different location can be approached through different ancillary ports.
The port of a telescope should always be at least 5-6 cm above the upper margin of
myoma to have good field of vision. 300 telescope helps tremendously to reach difficult site
myomas.Fig.2 a,b,c
Epigastric port
Palmer’s point
Primary port-supraumbilical
Ipsilateral secondary upper
port
Ipsilateral secondary lower
port
Epigastric port
Contralateral secondary
upper port
Contralateral secondary
lower port
Fig. 2a.Routine placement upto 14 wks Fig. 2b.Veress needle at Palmer’s point
Fig.2c For larger myomas
shift upwards

Procedure 9-
Placement of primary and secondary trocars depends upon the size and
site of myomas.
After primary port entry, reanalysis of size and site of myoma is done and
then accordingly sites of secondary ports are decided.
Relation of myomas with the uterus and fallopian tube should be
carefully assessed
Examination of the pelvic cavity is also performed to ascertain relation of
the fibroids to other pelvic structures. (Fig 3a,b)
Vasopressin 1 in 100 dilution is injected into myomas at 3 to 4 sites to
minimize bleeding (action will remain only for 20-30 min).
Careful planning of incision is done: The incision should be taken
carefully to avoid any cornual damage. In case of multiple myomas one
should optimize the incision so as to remove many myomas from a single
incision, as far as possible.
Incision can be taken with a scissors, monopolar hook, harmonic scalpel
or Enseal vessel sealing device Fig. 4 a,b,c
Fig. 4a Incision with monopolar hook
Fig. 3a,b Insepction of myoma and examination of pelvic cavity

Most preferred incision is transverse incision, as it will cut fewer vessels.
Incision should be of sufficient depth, so that capsule of myoma is
visualized.
With 2 non-traumatic forceps, cut edges are pulled apart so as to expose
capsule of myoma well and make space for myoma screw insertion.
Once the myoma screw is inserted, myoma is pulled outward and upward
keeping counter traction on uterus downward with 2 Allis forceps applied
on the anterior lip the cervix.
If one is in the right plane, myoma is usually extracted easily and there is
minimal bleeding.
Position of myoma screw is changed from time to time so that traction is
applied next to cleavage line.
For a larger myoma, 10 mm myoma screw helps in better extraction &
hence shortens operative time.
Usually the base of myoma will have large feeding vessels, which should
be cauterized and cut. ( Cuatery more on myoma than on myoma bed )
Only active bleeders of the bed are cauterized which can be easily
identified by underwater inspection.
Undue cautery should be avoided, as it will give defective healing.
Myoma after removal is parked at right paracolic gutter.
Fig. 4b Incision with Harmonic scalpel
Fig. 4c Incision with Enseal vessel sealing device

Closure of uterine flap-
Reconstruction of myoma bed can be performed with Vicryl no. 1 suture or barbed
suture (see table 1) / V loop (table no2)
Whether single or multiple layer closure is individual’s decision-but the ultimate aim
is to obliterate the dead space completely so as to avoid hematoma formation, which
is another cause of weakening of scar.
Start from one angle, first stitch is placed beyond angle either with intra-corporeal or
extra-corporeal suture and then rest of defect is closed by taking deep continuous
locking sutures and the end suture should be again beyond the angle of opposite side.
If it is a single layer closure, ensure that stitches are deep enough to obliterate the
dead space.
Studies have shown that three-layer closure with first layer, as endometrial layer
doesn’t compromise pregnancy or pregnancy outcome.
Fig. 5a Placement of suture beyond the angle
Fig. 5b Continuous locking sutures Fig. 5c Baseball sutures

Strengthening of myoma scar :
Laparoscopic myomectomy has received many controversies & debates for the
obvious reason that strength of myomectomy scar gets tested in subsequent pregnancies &
rupture of uterus can sometime lead to maternal morbidity & mortality apart from fetal
mortality
To prevent the weakening of a scar one has to take care of following triad.
A) One can think of avoiding hematoma formation by –
1.Using excellent energy source for incision & extraction of myoma so that vessels get sealed
before cutting.
2. Remaining in right plane hence less bleeding
3. Excellent closure – Barbed / V Lock / vicryl no 1 ( Obliterate the dead space )
B) Avoiding tissue necrosis –
1. Cauterisation of myoma bed for sealing of vessels should be avoided unless it has a large
bleeder.
2. Compression of myoma bed by assistant till surgeon gets in suture material will help to
seal smaller veins and cappilaries
Tissue Necrosis Hematoma
Infection Weakening of scar
Fig 6. Compression rather than cauterization of the myoma
bed to achieve hemostasis

3.Immediate and excellent suturing will also achieve hemostasis.
Needless to say good sterile precautions, shorter duration of surgery, avoidance of hematoma
formation will avoid infections.
Extraction of myoma-
Myomas are extracted by electronic morcellation. Fig. 5 a, b, c Smaller
myomas can be extracted by colpotomy.
A meticulous lavage is given and hemostasis is checked.
End result should be a clean pelvis.
To keep a drain in the postoperative period is again an individual’s
choice.
In difficult situations-
Pedunculated myomas with a broad base-
Instead of transverse incision, circular incision should be taken at the
base of myoma in a circumferential manner.
With myoma screw, myoma is pulled up and enucleated after
cauterizing base of the pedicle.
( Again ensure no cauterization un uterus)
Adhesion prevention:
Studies have shown that long term complications of adhesion formation can be prevented by
use of absorbable adhesion barriers such as Interceed™.
Other measures that can be taken by the surgeon to avoid adhesions are ensuring proper
hemostasis, thorough lavage of the pelvic cavity after the operation and early post-operative
mobilization.
!!
Fig 5a. Extraction of myoma
Fig. 5c Morcellated pieces of myoma
Fig 5b. Morcellation in process

Tips
In case of multiple myomas where the shape of the uterus is distorted, round ligament
helps in identification.
As far as possible, incision should be taken anteriorly than on posterior wall. Self pre-
operation USG always helps to enhance surgical performance on table especially in
cases of multiple myomas. One can decide the number of myomas that can be taken
out through a single incision. There is no tactile sensation in laparoscopy so small
myomas hidden under large myomas, if known beforehand, can be removed
successfully.
We don’t advocate use of pre-op GnRH analogues to reduce the size of myoma.
Traction on uterus downwards with Allis forceps applied to anterior lip of cervix and
upward counter traction on myoma with myoma screw, next to cleavage line will
facilitate extraction.
Myomas up to 5-6 cm can be delivered with colpotomy.
Proper serosal approximation, hemostasis, clean pelvis at the end, early mobilization
will help in prevention of postoperative adhesions.
Instillation of vasopressin, speedy surgery, skillful and rapid suturing, good knot tying
techniques will help to minimize bleeding.
Determination of surgeon , his/her operative skills, willingness to learn and use newer
modalities of energy sources & suture materials, learning with his/her own mistakes will
make an excellent laparoscopic surgeon.
It is important for every surgeon to ask himself/herself at the end of the day, whether I
would have done the same case in better way? And if yes what way? Adopt that technique
or mind for the next case & needless to say he/she becomes better, faster & safer day by
day.
Fig. 7: Use of Interceed™ adhesion
barrier ; also note clean pelvis

References:
1. Laparoscopic Myomectomy : A Current View – Jean Bernard Dubuisson, Chapron C,
Arnaud Fauconnier Et Al, Human Reproduction Update 2000, Vol 6, No 6, Pp 588-594
2. Endoscopic Management Of Uterine Fibroids. : Agdi M, Tulandi T., Best Pract Res
Clin Obstet Gynaecol. 2008 Aug;22(4):707-16. Epub 2008 Mar 6.
3. Pregnancy Outcomes after Laparoscopic Myomectomy with Ultrasonic Energy and
Laparoscopic Suturing of the Endometrial Cavity: Nelson H et al, The Journal of the
American Association of Gynecologic Laparoscopists; Volume 8, Issue 1, February
2001, Pages 129-136
4. Treatment Of Myomas By Laparoscopic And Laparotomic Myomectomy And
Laparoscopic Hysterectomy : L. Mettler, T. Schollmeyer, E. Lehmann, Willenbrock, J.
Dowaji And A. Zavala, Informa Healthcare, Minimally Invasive Therapy And Allied
Technologies, 2004, Vol. 13, No. 1 , Pages 58-64
5. Factors Influencing Laparoconversions During The Learning Curve Of Laparoscopic
Myomectomy : H. Marret, M. Chevillot, B. Giraudeau, K. Lalitha, Acta Obstetricia Et
Gynecologica Scandinavica, March 2006, Volume 85, Issue 3, Pages 324–329,
Limitations of Laparoscopic Myomectomy:
The size
Number & positions of myomas
Whether future fertility is desired
The experience of surgeon especially mastery over endosuturing
How big is big? & How many are too many?
The answer varies from surgeon to surgeon depending upon which part of learning curve
he/she is on. It is a relative term but -
The easiest myomas to remove are those that are subserous than deep intramural & anterior
& fundal than posterior & isthmic.

6. Nezhat's Operative Gynecologic Laparoscopy And Hysteroscopy Camran Nezhat,
Farr R. Nezhat, Ceana Nezhat, Page 155, 316 – 322
7. Uterine Leiomyoma (Fibroid) Imaging: Hilip Thomason, Director Of Diagnostic
Radiology, Department Of Radiology, Beverly Hospital Contributor Information And
Disclosures Emedicine WebMD Updated: May 6, 2008
8. Laparoscopic Myomectomy: Feasibility And Safety—A Retrospective Study Of 762
Cases : P. G. Paul, Aby Koshy And Tony Thomas, Gynecological Surgery, 2006,
Volume 3, , 97-102
9. Endoscopy Simplified : Practical Tips By Experts – Dr. Sunita Tandulwadkar, Jaypee
Publication, 2008
10. The Power Of The Barbed Suture : Michael S. Kluska, Plastic Surgery Practice, Jan 2010
11. Motion Study – Comparison Of Wound Closure Time Using Conventional Techniques And Knotless, Self Anchoring Surgical Sutures In Ex-Vivo Porcine Model For Single Layer Closure
With Barbed Devices Vs. Double Layer Closure With Traditional Suture . Royal College Of
Surgeons, London, UK; Covidien, 2010
12. Time Study - V-Loc™ 180 Absorbable Wound Closure Device, Robert T. Grant, MD,
Msc, FACS, New York-Presbyterian Hospital, Argent Global Services, 2010
13. Utilization Of A Porcine Model To Demonstrate The Efficacy Of An Absorbable Barbed
Suture For Dermal Closure, UTSW, S. Brown, 2010