
Improving the Health of Canadians: Exploring Positive Mental Health

Making a Difference in the
Health of Canadians: CIHI's
Health Data and Information
Breakfast with the Chiefs
March 22, 2006
Glenda Yeates, President and CEO

Vision
• CIHI improves the health of Canadians and
strengthens their health system by:
developing, integrating and disseminating timely and
relevant health and health services information, and
by facilitating informed discussion and evidenced-
based decision-making

Our Mandate
• To serve as a national coordination mechanism for healthinformation in Canada
• To provide accurate and timely information that is requiredfor:
Sound health policy
Effective management of health caresystem
Public awareness of healthdeterminants
• Through the work carried out by the Canadian PopulationHealth Initiative (CPHI), CIHI aims to:
Foster a better understanding of factors that affect the healthof individuals and communities; and
Contribute to developing policies that reduce inequities andimprove the health and well being of Canadians

Governance
• 16-member Board, proportionally constituted to:
Create a balance among health sectors and regions
of Canada
Link F/P/T governments with non-government health
related groups
Provide strategic guidance to CIHI and Health
Statistics Division of Statistics Canada
Advise the Conference of Deputy Ministers of Health.

Toronto
OttawaVictoria
Edmonton
Our OfficesOver 500 employees across Cana
Regional offices in Western Canaand in Montreal
To be opening an office in theAtlantic region
Montreal

From Vision to Action

Premier Source of Information –Collaboration is key
• CIHI facilitates the collaboration of many different
groups of stakeholders, who collectively join to
form Canada’s health information infrastructure.
Statistics Canada
Ministries ofHealth
RegionalHealthAuthorities
Health facilities
Public andPrivate SectorOrganizations
ProfessionalAssociations
Advocates
Researchers

Who we serve –Our Target Audiences
• Policy-makers
• Health System Managers
• Members of the Public

Where we have made progress
• More Databases
• More analyses
• Timeliness
• Data Quality

Data Holdings - 1994
• Health ServicesDAD
Hospital Morbidity
Hospital Mental Health
Therapeutic Abortions
Organ Registry (CORR)
Trauma Registry (OTR)
• Health Professionals
Physician
– NPDB
– SMDB
Nursing
– RNDB
Health Personnel
• Health Expenditures
Provincial, regional,
and local (CMDB)
National (NHEX)
International (OECD)

Data Holdings - 2005Health Services
Discharge Abstract Database (DAD)Hospital MorbidityAmbulatory Care (NACRS)Hospital Mental HealthTherapeutic AbortionsOrgan Registry (CORR)Trauma Registry (NTR/OTR)Joint Replacement Registry (CJRR)Continuing Care (CCRS)Rehabilitation (NRS)Ontario Mental Health ReportingSystem (OMHRS)Medical Imaging Technology (MIT)
UNDER DEVELOPMENT
Home Care Reporting SystemPharmaceutical (NPDUIS)Medication Incident Reporting(CMIRPS)
Health Professionals
Physician
– NPDB, SMDB
Nursing
– RNDB, LPNDB
– RPNDB
Health Personnel
Five new HHR databasesunder development e.g.Pharmacists and O.T.
Health Expenditures
Provincial, regional, andlocal (CMDB)
National (NHEX)
International (OECD)

Publications
2000-2001:
• Total number of analytical reports released = 18
• CIHI released it first Annual Health Care in
Canada Report.
2005-2006:
• Total number of analytical reports
planned/released = 48
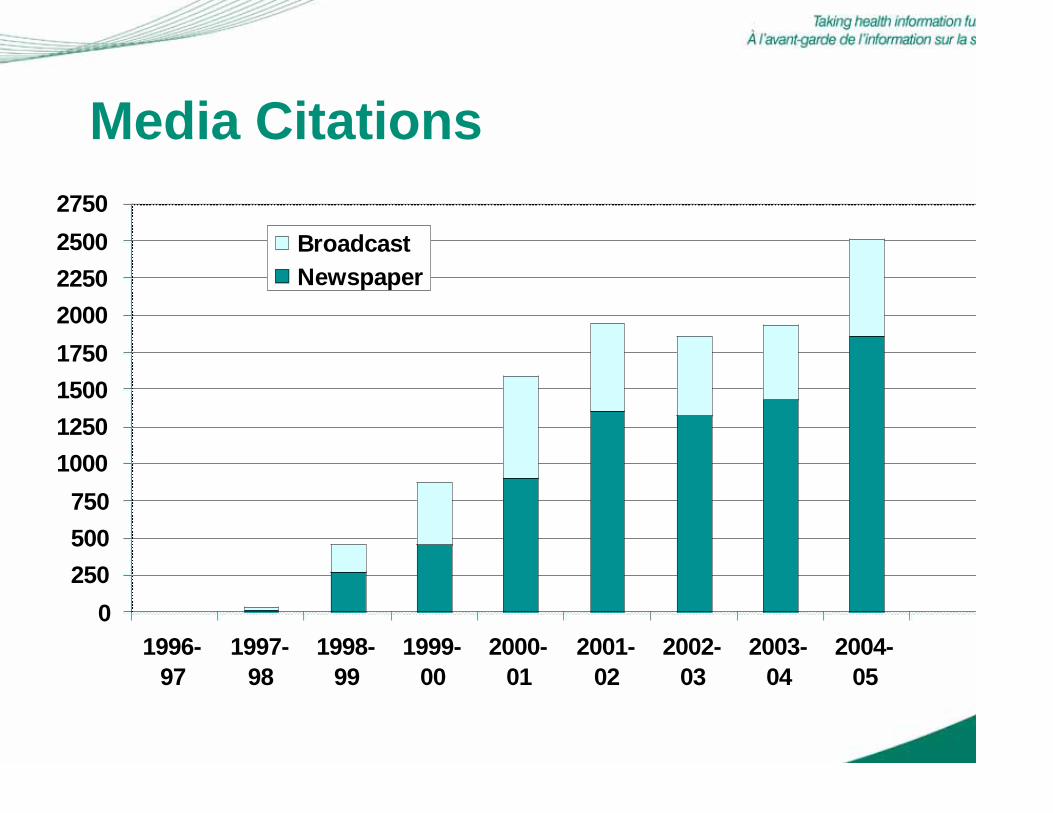
Media Citations
0
250
500
750
1000
1250
1500
1750
2000
2250
2500
2750
1996-
97
1997-
98
1998-
99
1999-
00
2000-
01
2001-
02
2002-
03
2003-
04
2004-
05
Broadcast
Newspaper

Journal Citations
0
20
40
60
80
100
120
2000-01 2002-03 2003-04 2004-05

Supporting Policy-makers
• Support for Income
Testing (e.g. in Fair
Pharmacare Program)
Inter-provincial
comparison data
presented in Health
Care in Canada used to
plan changes related to
the structure of
Pharmacare

Supporting Health Care Management
• Ministry of Health and RHA Performance
Agreements
Data based on CIHI data standards are used to
populate performance agreements between the MOH
and the RHAs
• Reference Based Drug Pricing in BC
CIHI data were used to evaluate the use of Reference
Drug Program (RDP). The evaluation indicated that
the use of RDP did not negatively affect health and
saved money

Looking Forward
• Enhanced analytical products
• Continued database development
• Increased emphasis on data quality
• New tools for better access to information
• Regional connections

Enhanced Analytical Products
• Access to care/Wait times
• Quality/Outcomes of health services
• Health Human Resources
• Population Health activities
• Costs/expenditures

New Indicator Development
• Safer Healthcare Now!
• Hospital Standardized Mortality Rates
(HSMR)
• Primary Health Care Indicators

Continued Database Development
• Drug Utilization Database
• Medication Incident Reporting
• Health Human Resources
• Focus on adding new jurisdictions to
existing databases e.g.
Ambulatory Care/E.R.
Home Care Reporting System

Addressing Data Quality
• Timeliness
• Data Quality Strategy including
re-abstraction studies
• Data Quality Progress Reports to
Deputy Ministers of Health

CIHI’s Evolving External Electronic Data Access& Analytical Sophistication
QuickStats (2002)
eReports (2001)
CIHI Portal (2005)
Public View
Aggregate, Static Repor for Health Care
Stakeholders
Detailed, ad hoc reportfor authorized
Health Care Stakeholde

Portal Features
• Secure access to pan-Canadian CIHI data
• Powerful web-based analytical tools
• Custom facility comparisons
• Patient de-identified analysis
• Standardized templates
• Peer collaboration
• User-specific e-Learning


On Quality and Outcomes-Health Care in Canada
• This report was
released in June 2005
and focused on
volumes and
outcomes

Low VolumesWhat Are The Odds?

Mortality by Hospital Volume Quintile:Abdominal Aortic Aneurysm Repair
3.0% 3.0%
2.2%2.4%
1.8%
0%
1%
2%
3%
4%
Lowest HighestHospital Volume
Ad
jus
ted
30
-Da
y I
n-H
os
pit
al
Mo
rta
lity

On Access to Care/Wait timesWaiting for Health Care in Canada
• Waiting for Health Care in
Canada: What We Know
and What We Don’t Know
is the first report of this
kind
• Released on March 7,
2006

Leading Reasons Cited forAccess Problems Differ
• Routine/on-going care
Difficulties getting an appointment
• Pap smear/mammography
Didn’t think it was necessary
• Specialist care for new health problem & selected
non-emergency tests (MRI, CT, angio)
Waited too long for an appointment
• Non-emergency surgery
Waited too long

What Type of Care you Need
next day (day after admission)Hip Fracture
Months(with knees > hips)
Joint Replacement
a few monthsCataract
days to weeksCardiac
Median WaitType of Surgery

Waits for Angioplasty or BypassSurgery Following a New Heart Attac
Waited 137days or lesWaited 23 days or less90% of patients
Waited 18 days or lesWaited 4 days or lessMedian
Waited 6 days or lesWaited 0 days10% of patients
CABGAngioplasty

Medical Imaging in Canada, 2005
• Third annual report
• Information on
supply, distribution,
utilization, costs
and personnel
• New this year was
the information on
utilization

Number of MRI Exams per 1,000 Population, byJurisdiction and Canada, 2003–2004 and 2004–2005
0
1 0
2 0
3 0
4 0
5 0
6 0
N.L. P.E.I. N.B. Que. Ont. Man. Sask. Alta. B.C. Can.
2003–2004 2004–2005

Average Number of MRI and CT Exams per 1,000Population, Per Scanner, US, England & Canada, 2004-2005
7,745
--
5,298
CT
87.3
43.0
172.5
CT MRIMRI
4,66625.5Canada
3,51319.0England
3,41283.2United States
Exams per ScannerExams per 1,000population
Country

Number of MRI Scanners in Hospitals and Free-Standing Imaging Facilities, Canada, 1998 to2005.
38
69
115119 121
130
2 4 715 19
25 27 28
148
46
0
20
40
60
80
100
120
140
160
1998 1999 2000 2001 2002 2003 2004 2005
Year
Nu
mb
er o
f M
RI S
can
ners
Hospitals
Free Standing

Facility-Based Continuing Care in
Canada
• Report is being
released today
• First report that sheds
some light on a sector
of the health care
system that until now,
we have known very
little about.

Five Most Common DiseaseCategories/Diagnoses on Admission,Residential Continuing Care
19%Psychiatric/Mood
34%Endocrine/Metabolic/Nutritional
40%Musculoskeletal
65%Heart/Circulation
77%Neurological
% of residents with MDSAssessments
DiseaseCategories/Diagnoses

On Health Human ResourcesGeographic Distribution of Physicians
in Canada
• Report co-authored byRoger Pitblado and RayPong, Centre for Rural andNorthern Health Research,Laurentian University
• 1999 report described thedistribution of Canada’sphysicians in 1991 and1996
• New in this report is anexamination of the types ofservices family doctorsprovide in urban and ruralsettings

Urban-Rural Distribution of Family Physicianand Specialist Physicians, Canada, 2004
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Rural 16.0% 2.4%
Urban 84.0% 97.6%
Family Physicians Specialist Physicians
N t C iti ith f th 10 000 l d fi d “ l”

Percent of Large City and Small Town FamilyPhysicians Who Provide Various Types ofHealth Care Service, Canada, 2004
8.5%
12.1%
19.5%
15.3%
32.9%
40.4%
41.8%
73.9%
0% 20% 40% 60% 80% 100%
Delivering Babies
Hospitalist Care
Cancer Care &
Oncology
Emergency
Medicine
Large City Small Town
Note: “Large cities” are cities with one mill ion or more people “Small towns” have populations of less than 10 000 where

Average Distance to Physicians forResidents of Large Cities and Small Towns,Canada, 2004
2.1
2.5
3.2
0.7
91.9
103.3
100.5
10.5
0 20 40 60 80 100 120
Psychiatrist
Pediatrician
OB/GYN
Family Physician
Kilometers
Large Cities Small Towns
Note: “Large cities” are cities with one mill ion or more people “Small towns” have populations of less than 10 000 where

Number of Physicians Moving Abroad andReturning From Abroad, Canada, 1969-2004
0
100
200
300
400
500
600
700
800
900
1969
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
Moved Abroad Returned From Abroad
Source: Southam Medical Database CIHI

On Population HealthImproving the Health of Canadians:
Promoting Healthy Weights
• Focus: how where welive, learn, work and playcan make it easier – orharder – to make choicesthat promote healthyweights.
• Reviews research andpresents analyses
• Reviews relevantprograms and policies
• Presents information onthe Canadian public’sviews on options topromote healthy weights

Adults Living in the Urban Core ReportLower BMIs (< 25)
Source: CPHI analyses of CCHS 2.2 (2004) and Census 2001, Custom Tabulation.
* Significantly different from Urban Core p < 05
52%45%* 45%* 44%* 46%* 43%*
0%
25%
50%
75%
100%
Urban
Core
Urban
Fringe
Urban
Area
Outside
CMA/CA
Secondary
Urban
Core
Rural
Fringe
Rural Area
Outside
CMA/CA

Physical Inactivity and Income(% Adults age 18+)
Source: CPHI analyses of CCHS 2.2 (2004), Custom Tabulation.
66%* 67%* 64%*58%*
50%
0%
25%
50%
75%
100%
Q1
(Lowest)
Q2 Q3 Q4 Q5
(Highest)

On Costs and ExpendituresExploring the 70/30 Split: How Canada's
Health Care System Is Financed
• Today, about 70% oftotal Canadian healthexpenditures comes fromthe public purse. Theremainder (about 30%)comes from privatesources.
• This report, which wasreleased in September2005 looks at trends infinancing and atvariations in this 70/30split across provinces
d t it i

Total Health Expenditure Per Capita, 15 SelectedCountries, 2003
684
705
1,535
1,960
2,031
2,450
2,669
2,967
3,088
3,204
3,534
4,976
5,041
5,635
$0 $1,000 $2,000 $3,000 $4,000 $5,000 $6,000
Hungary (e)
South Korea
Spain
Australia (a)
United Kingdom (a)
Japan (e)
CANADA (e)
France (e)
Netherlands
Germany
Denmark
Norway (e)
Switzerland (e)
United States
$ Per Capita ($US Exchange Rate)
Source: OECD Health Data 2005
OECD Average - $2349

Total Health Expenditure as a Percent of GDP, 15Selected Countries, 2003
5.6%
6.2%
7.7%
7.7%
7.9%
8.4%
9.3%
9.8%
9.9%
10.1%
10.3%
11.1%
11.5%
15.0%
9.0%
0.0% 3.0% 6.0% 9.0% 12.0% 15.0% 18.0%
Korea
Mexico
Spain
United Kingdom (a)
Japan (e)
Hungary (e)
Denmark
Australia (a)
Netherlands
CANADA (e)
France (e)
Norway (e)
Germany
Switzerland (e)
United States
OECD Average – 8.7%
Source: OECD Health Data 2005

Sources of Health Spendingin Canada 2003
14%
12%
3%
70%
Public Out-of-Pocket
Private Insurance All Other Private Funds

Public Spending in 2003
0
10
20
30
40
50
60
70
80
90
100
Hospitals Physicians Drugs Dental
France
Germany
Canada
Percentage of Services Covered by Public Funds
Source: OECD Health Data 2005

Per Capita Health Spending
$291$2,214$2,903France
$312$2,343$2,996Germany
$793$2,503$5,635U.S.
$448$2,098$3,001Canada
Out-of-pocket spendingcapita (in U.S.$)
Public-sector health spendingper capita (in U.S.$)
Health spending percapita (in U.S.$)
Note: All numbers represent 2003 data unless otherwise noted. Spending percapita was converted to U.S. dollars using purchasing power parities for GDP.
Source: Health at a Glance—OECD Indicators 2005.

Where we need your help
• Identifying priority information needs
• Timeliness of our data
reliance on providers to supply timely data
• Data Quality
Support with our data quality strategies

The Road Ahead. . .


















