
Major Trauma A standard approach - Ballarat Health...
96
Major Trauma A standard approach Steve Costa Ballarat Health Services Emergency Medicine Training Hub
Transcript of Major Trauma A standard approach - Ballarat Health...

Major Trauma
A standard approach
Steve Costa
Ballarat Health Services
Emergency Medicine Training Hub

Learning objectives
To understand the Victorian State Trauma System and the role of Ballarat Health Services in that system.
To be familiar with BHS protocols for trauma including trauma teams
Management of suspected cervical spine injuries
Pre reading
Hughes T & Cruickshank J. Adult Emergency Medicine at a Glance. Chichester, West Sussex, UK : John Wiley & Sons, 2011. Chapter 8 Trauma; primary survey. Chapter 9 Trauma; secondary survey. Chapter 10 Major head and neck injury. Chapter 11 Minor head & neck injury
Refer to ED lecture series and self directed workbooks

Other learning resources
http://www.health.vic.gov.au/trauma/links.htm
http://www.health.vic.gov.au/trauma/triage.htm
Relevant guidelines for Ballarat Health Services
Trauma – General Approach BHS Intranet Link
http://webapps/airapps/Services/au/org/bhs/govdoc/HTMLViewer.php?id=-31766~intranet-search
Trauma Team Activation BHS Intranet Link
http://webapps/airapps/Services/au/org/bhs/govdoc/HTMLViewer.php?id=-32235~intranet-search
Cervical spine BHS Intranet Link
http://webapps/airapps/Services/au/org/bhs/govdoc/HTMLViewer.php?id=-32499~intranet-search
All available via http://bhsnet/gov-doc-search

Introduction
Trauma leading cause death 1-40yo
Peak age 15-30
Cost in A$ 11 billion
Up to 40% trauma deaths preventable
Improvements largely due to social education Seat belts
Speed limits
Drink driving
Helmets
For each death estimated to be 10 serious non-fatal injuries

Essence of Trauma Care
Right patient to the right resources as soon
as possible
Achieved by:
Integrated system - ‘Trauma Network’
Seniority or experience of providers
Decision Pathways and education
Trauma Network
Ministerial Taskforce on Trauma and
Emergency Services - 1997
ROTES report (Trauma deficiencies) – 1999
Victoria State Trauma Network – 2000 Two adult and one paediatric hospital as major trauma services (MTS)
Statewide system organisation and management of trauma response
Trauma triage and transfer protocols
Enhanced retrieval and transfer services (ARV)
Education and training
Research, service and technology developments
Quality management.

http://www.ambulance.vic.gov.au/

Results
80 per cent of all major trauma patients are
treated at a MTS
a reduction in mortality rates with fewer than
expected deaths according to international
benchmarks
positive trends in preventable deaths
reduced length of stay in hospitals.

Introduction
Medical management has shown far less improvement
Standardisation of approach has helped improve outcomes
Concept of “Golden Hour”
50% deaths <1/24 due to major vessel, CNS, spinal injury
benefit from prevention
30% deaths patients major truncal injuries causing respiratory &
circulatory compromise
benefit from prevention and timely intervention
20% die from sepsis, organ failure etc.
benefit from prevention, timely intervention and possibly from integrated
approach to recovery

Phases of care
Pre-hospital
Triage
Primary survey
Secondary survey
Disposition

Prehospital
Very little evidence to support major interventions in
the field
Oxygenation
Immobilisation cervical spine
Ventilation (unproven)
Fluids (unproven)
Lights and sirens (increases mortality and
community risk)

Triage to trauma centre
http://docs.health.vic.gov.au/

Triage to trauma centre
Associations with increased risk of death
Demographics
Age <5 >55
Know chronic cardiac/respiratory disease
Vital signs
BP <90
HR >124/min
RR <12 or >24
GCS < 13
O2 sats <90%
Trauma score >14 (not assessable prospectively)

Triage to trauma centre
Injuries
Penetrating injury to chest, abdomen, head,
neck or groin
Significant injuries to two or more body
regions
Severe injury to head, neck or trunk
Two or more proximal long bone fractures or
pelvis
Limb amputations (incl. partial or compound)
Burns >20% or involving face or airway

Triage to trauma centre
Mechanism
High speed >60 kph (>30kmh cyclists)*
Fall > 3m*
Struck on head by falling object >3m*
Ejection from vehicle*
Explosion*
Prolonged extrication
Pedestrian vs vehicle
And
>55 y.o. OR
Pregnant OR
Significant co-morbidity

Trauma reception
Prior warning
Prepare
Staff
Area
Paramedical services

Trauma teams
Team leader Overview
Resus
Assessment Communication
Internal & external
Airway team
Assess and secure airway
Control cervical spine
Ventilation
NGT
Procedure team
IV access & bloods
IDC
ICC
Scribe
Scout
Radiographers
• Assessment
• primary
• secondary surveys

Handover
Patient should transferred to trauma trolley prior to hand over
Parallel processing Team listens in ‘silent’ handover OR if pt unstable
Airway and procedure teams commence assessment
And
leader receives handover
Assume the worst & protect against unforeseen injuries do not focus on obvious injuries – protocol of ATLS

Primary survey
Airway & cervical spine
Assess & secure airway
Patency
Look, listen, feel
Jaw trust (no chin lift as cervical spine uncleared)
Oropharyngeal airway, nasopharyngeal airway?
RSI
Maintain cervical protection until spine cleared
In-line immobilization
Consider NGT

Primary survey
Ventilation/Breathing
Oxygen is the most important drug in the trauma room
Ensure adequate ventilation
Assess adequacy
Exclude pneumothorax, haemothorax
Bag/mask, ETT if required to maintain ventilation
Aim for normocarbia
CXR
Intervention may precede investigation if required

Primary survey
Circulation
Assess adequacy & effect of blood loss
Conscious state
Pallor
Capillary return
BP
HR
visual estimation of blood loss unreliable
FAST scan – ‘rule in’ test

Primary survey
Circulation
Control haemorrhage
pressure dressings
Tourniquets
Haemostatic dressings
Splinting
Thoracotomy (Cardiac manoeuvres/Aortic compression)
Theatre

Primary survey
Haemorrhage classification
Class Loss BP HR RR CR UFR CS
Class I <15% N N/+ N N/+ N N
Class 2 <30% N + + + anx
Class 3 <40% ++ ++ ++ leth
Class 4 >40% +/- +/- ++
coma

Primary survey
Circulation Access 2x >16G peripheral IV’s
Fluids initially crystalloid 20mlkg (repeat if required) warmed
Crystalloid vs colloid (no proven benefit)
Blood O negative Class III/IV haemorrhage
Continuing need for crystalloid
Consider need for clotting factors and plateletes ‘1:1:1’
Hypotensive resuscitation

Primary survey
Disability
Level of consciousness
AVPU
ALERT
VOICE
PAIN
UNCONSCIOUS
GCS – E4M6V5
Pupil response
Don’t ever forget the glucose

Primary survey
Exposure
Remove
Clothes
Jewellery
Avoid hypothermia

Primary survey
Monitoring
ECG, BP, SaO2, GCS +/- ventilator obs
Analgesia
Radiology
CXR, Cx spine, AP pelvis
IDC traditionally part of 1° survey but usually
done later

Secondary survey
AMPLE history
Allergy
Medications
Past history
Last food
Event

Secondary survey
Head to toe examination – ‘all over and all
holes’
Look, feel, move, listen
Log roll
PR examination
Consider
Tetanus toxoid
Antibiotic prophylaxis

Review
Constantly reassess and review
Any change repeat 1° survey
After any corrective procedure repeat 1°
survey
Disposition
Parallel thinking from before patients arrival
Direct to appropriate services
Definitive care made aware of patient
Discharge with appropriate support

Questions?

Summary
You are all part of a trauma network
Education saves lives
Reassess, reassess, and reassess again
(and intervene if required of course . . .)

Thankyou
Go and get coffee
See you in 20mins

Major Trauma
Practical and Scenarios
Ballarat Health Services
Emergency Medicine Training Hub

Fitting a cervical collar

Young man diving from a
pier…


http://www.rch.org.au/clinicalguide/guideline_index/Cervical_Spine_Injury/

Fingers between jaw and
trapezius
http://www.rch.org.au/clinicalguide/guideline_index/Cervical_Spine_Injury/
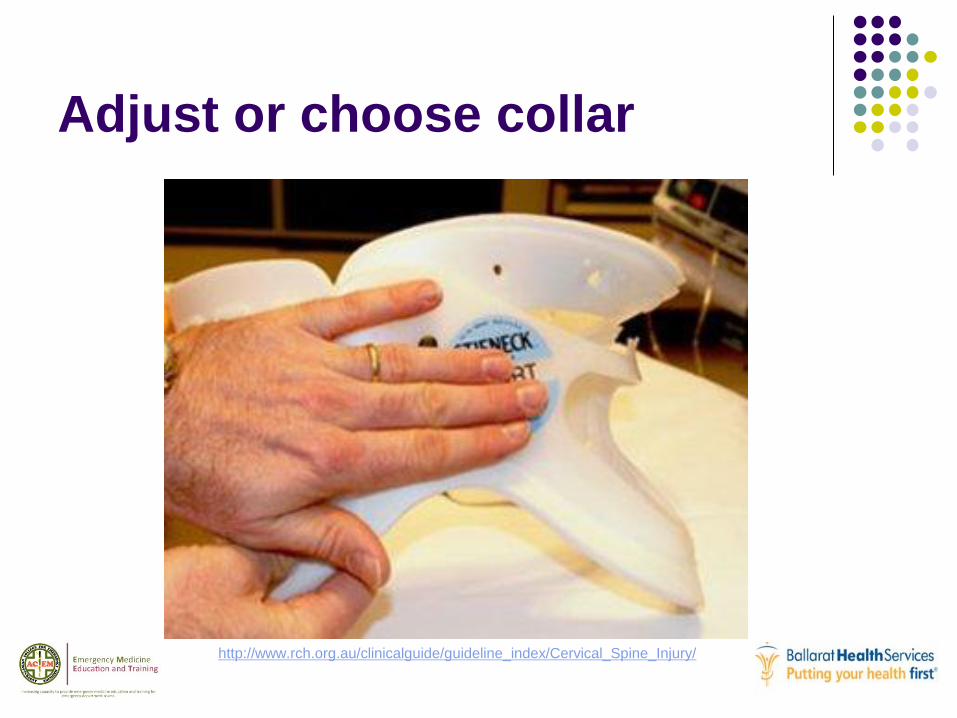
Adjust or choose collar
http://www.rch.org.au/clinicalguide/guideline_index/Cervical_Spine_Injury/

Apply!
http://www.rch.org.au/clinicalguide/guideline_index/Cervical_Spine_Injury/

Your turn!

Primary Survey
A – Talk to the patient first!
B – Listen for air and blood
C – Cyanosis, CRT, HR, BP
D – GCS, Spinal and Limb assessment, BSL
E – Full exposure and environmental control

Trauma Scenario 1
You receive a phone call from the ambulance
service. They have a 27 yr old male involved
in a MCA, he is conscious alert, the car has
rolled he has been ejected from the vehicle.
He has a probable # femur and compound
# tib/fib
How are you going to prepare?

Trauma preparation
Trauma call
personnel
trauma team
radiology
pathology
department
equipment

Trauma Scenario 1 Arrival
history as above
patient conscious, alert,
orientated
HR145 BP100/50 RR30
complaining of severe pain in
R leg
Deformity upper leg and
obvious compound R tib/fib
What is your approach? http://lifeinthefastlane.com/ortho-library/open-fractures/

Trauma Scenario 1
Primary survey
Airway intact
Breathing decreased air entry L hemi-thorax
What else would you look for?

Assessment of pneumothorax
Tension pneumothorax
RR30
BP100/50
HR145
tracheal deviation
decreased chest movement
venous engorgement
What are you going to do now?

Management tension
pneumothorax
Needle decompression
Then ICC
CXR
re-check ABC

Trauma Scenario 1
Once AB stable
re-check C continued hypotension N saline
bolus
D
E
rest of trauma series radiology
analgesia femoral N block + iv analgesia
Prepare for ankle reduction
head to toe examination – secondary survey

Questions?
next case . . .

Trauma Scenario 2

Trauma Scenario 2
A patient presents following a MVA, the other
driver was killed, she left the scene and
brought herself to hospital. She is
complaining of abdominal discomfort and
back pain.
What is you approach?

Approach to trauma
• Primary survey
• AcBC
• CXR, C-Spine, Pelvis XRs
• Secondary survey
• head to toe
• include log roll (if not already done)
• IDC
• NGT

Primary survey
primary survey
Airway normal
Cervical collar applied and immobilised
Breathing RR35, otherwise normal
Circulation HR140 BP100/45
Describe your subsequent management
Hypotensive trauma
Resuscitate circulation

Hypotensive trauma
Resuscitate circulation
Analgesia

Hypotensive trauma
Resuscitate circulation
Analgesia
Exposure of abdomen in 1° survey
marked seat belt bruising over mid/lower
abdomen
abdomen tender generalised guarding
log roll
Thoraco-lumbar junction tender with bruising
PR NAD

Hypotensive Abdominal
trauma
Surgical registrar review asks for:
CXR
Lateral lumbar spine
what other injuries are likely?
what further investigations do you require?
What does the patient need?

Reproduced from http://www.radiologyassistant.nl

Hypotensive Abdominal
trauma
Surgical registrar review asks for:
CXR
Lateral lumbar spine
What other injuries are likely?
Upper abdominal visceral injury
What further investigations do you require?
What does the patient need?

Hypotensive Abdominal
trauma
Surgical registrar review asks for:
CXR
Lateral lumbar spine
What other injuries are likely?
What further investigations do you require?
CT
What does the patient need?
Hypotensive Abdominal
trauma
Surgical registrar review asks for:
CXR
Lateral lumbar spine
What other injuries are likely?
What further investigations do you require?
What does the patient need?
Adequate fluid resuscitation – Crystalloid and Blood
Theatre?

Chance fracture
Fracture of L1 hyperflexion
Transverse fracture through posterior
elements +/- body
Associated injury to
pancreas
duodenum 4th part
kidney
liver/spleen
retroperitoneal haemorrage

Hypotensive Abdominal
trauma
Investigation
CT abdomen dual contrast
Additional treatment
NGT, IDC
Tetanus toxoid/Antibiotics if required
police bloods
next of kin
Disposition

Questions?
next case . . .
Trauma scenario 3
A 20 yr old presents via ambulance after
falling from his motorcycle. He is conscious,
complains of neck discomfort and shortness
of breath.
What is your approach?

Approach to trauma
• Primary survey
• AcBC
• CXR, C-Spine, Pelvis XRs
• Secondary survey
• head to toe
• include log roll (if not already done)
• IDC
• NGT

Primary survey
Airway - intact
Cervical collar and sand bags
Breathing - limited chest expansion but equal
air entry
Circulation
HR 70 BP90/50 RR 30
What is the likely cause of this patient’s
hypotension?

Hypotensive trauma
Loss-haemorrhage
internal/external
Redistribution eg vasodilatation 2° spinal shock
Pump failure
cardiac contusion
loss cardio-accelerator
Substance use/abuse

Hypotensive trauma response
Exclude obstruction to venous return
Fluid bolus
CXR normal
What now?

Hypotensive trauma
Repeat fluid bolus if no response Re-do 1° survey, include ‘D’ in assessment of ‘C’
Debility GCS 15/15
flaccid paralysis of both legs
sensory level at level of upper chest
Priapism
BP 100/50 HR 80
What do you do next?

Hypotensive trauma
Trauma series X-rays?
Cervical spine
CXR
Pelvis

Hypotensive trauma
Trauma series X-rays?
Cervical spine
CXR
Pelvis
CX spine/CT shows # dislocation at C6/7

Reproduced from JBJS Journal of Bone and Joint Surgery Br June 2006 vol 88-B No.6 771-775

Franz T et al. Br J Sports Med 2008;42:55-58
Copyright © BMJ Publishing Group Ltd & British Association of Sport and Exercise Medicine. All rights reserved.
Hypotensive trauma
Trauma series X-rays?
Cervical spine
CXR
Pelvis
CX spine/CT shows # dislocation at C6/7
What are the priorities with this patient?

Spinal trauma
Treatment priorities
breathing loss of intercostals exhaustion
spinal shock
temperature control
fluid balance important risk of over-filling
IDC important
Steroids
controversial increases morbidity
Referral to specialist unit

Referral
Be familiar with specialist unit provision
Consider moving to Major Trauma Service
provider early
Engage retrieval service early with
appropriate detail

http://docs.health.vic.gov.au/docs/doc/6A955B0E117A3E7FCA257B630021EA74/$FILE/cervical_spine_guidelines.pdf

http://docs.health.vic.gov.au/docs/doc/6A955B0E117A3E7FCA257B630021EA74/$FILE/cervical_spine_guidelines.pdf

Reproduced from Radiopaeia.org

Reproduced from JBJS Journal of Bone and Joint Surgery Br June 2006 vol 88-B No.6 771-775

Questions?

Trauma scenario 4
47 yr old woman presents via ambulance she
was trapped between her car and a car that
reversed into her in the supermarket car park.
She is conscious but confused, complaining
of pain in her “tummy”.
What is your approach?

Primary survey
ABCx normal
C HR120 BP 80/60 RR 32
Approach to hypotension?

Hypotensive trauma
Fluid bolus
CXR & CX spine normal
Pelvic Xray shows
# body pubis with separation anteriorly
# through sacrum
no response to initial fluid bolus
What is the cause of the hypotension?
What is your assessment & management?

Pelvic Fracture
Open book AP compression pelvic fracture
Hypotension due to haemorrhage
pelvic veins
other abdominal injury

Approach to pelvic fracture
secondary survey
Including AMPLE history
abdominal examination
tender and guarding lower abdomen
approach ?
PV blood at meatus
IDC blood
Log roll sacral pain and tender
Pelvic # and Hypotension
Call orthopaedic Reg ASAP Repeat fluid bolus +/- blood
close # MAST suit
wrap
“C” clamp
Exclude other abdominal organ injury
CT abdomen dual contrast
US “FAST”

Summary
You are all part of a trauma network
Education saves lives
Reassess, reassess, and reassess again
(and intervene if required of course . . .
And then reassess)

Further reading
More cases http://lifeinthefastlane.com/tag/trauma-tribulation/
Online education resource
http://www.surgicaltutor.org.uk/defaulthome.htm?core/trauma/spinal.htm~rig
ht

Resources
ARV Medical Reference Manual http://www.ambulance.vic.gov.au/Media/docs/ARV%20Reference%20Manual_Jan2011-16629a6b-ddd2-4886-97ed-
ad5c6cdb52a6-1.PDF
Vicotrian State Trauma Committee 2010 Adult pre Hospital Major trauma
Criteria http://docs.health.vic.gov.au/docs/doc/9382EC200E82017BCA25784000739B22/$FILE/Prehospital%20triage%20Victo
rian%20State%20Trauma%20Committee%202010.pdf
http://docs.health.vic.gov.au/docs/doc/6A955B0E117A3E7FCA257B630021EA74/$FILE/cervical_spine_guidelines.pdf
The Royal Children’s Hospital Melbourne – Cervical Spine Assessment http://www.rch.org.au/clinicalguide/guideline_index/Cervical_Spine_Injury/
Life in the Fastlane http://lifeinthefastlane.com/ortho-library/open-fractures/
Radiology Assistant http://www.radiologyassistant.nl/

Thankyou
End


















