
Maintenance” - Atlantic Health · Maintenance” 2011 Annual CAN Conference ... Svetkey LP t al,...
36
“The Reduced Obese State: The Challenge of Weight Maintenance” 2011 Annual CAN Conference November 17, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics Charles A. Boettcher II Chair in Atherosclerosis University of Colorado Anschutz Medical Campus
Transcript of Maintenance” - Atlantic Health · Maintenance” 2011 Annual CAN Conference ... Svetkey LP t al,...
“The Reduced Obese State: The Challenge of Weight
Maintenance”
2011 Annual CAN Conference November 17, 2011
Robert H. Eckel, M.D.
Professor of Medicine
Professor of Physiology and Biophysics
Charles A. Boettcher II Chair in Atherosclerosis
University of Colorado Anschutz Medical Campus
Duality of Interests – Advisory Boards
• Amylin • Esperion • Genentech • Genfit • GTC Nutrition • Johnson & Johnson • Lilly • Merck • Pfizer • Regulus • sanofi-aventis
– Grants/Research Fellowships • Diadexus • GSK • sanofi-aventis
– Educational Venues • AccelMed
• Cardiometabolic Health Congress
• Vindico
• VoxMed

Prevention of Weight Gain
• It’s all a matter of energy balance!
– In the absence of edematous disorders, if you’re burning less than you’re eating you gain weight
E Out < E In
And it’s much less than the 100 kcal/day estimated by Hill JO et al (Science, 2003)
WT

Obesity Incidence Based on
Energy Balance Calculations
• BMI – 25.0 kg/m2, Ht - 68”, Wt – 164 lb
vs.
• BMI – 30.0 kg/m2, Ht – 68”, Wt – 197 lb
over 20 years is
13 kcal/day excess

Body Weight Regulation
SET OR SETTLING POINT?

Body Weight
Time
years months years
therapeutic space prevention
Schematic Representation of the
Natural History of Obesity
Eckel RH, Kahn S et al: Diabetes Care 34:1424 and JCEM 96:1654, 2011
Once obesity occurs, body fat is
defended!
Why is the Defense of Body Fat So Important?
• Body weight (fat mass) is a predictor of
survival in
– Animals
• Mammals
• Birds
• Insects
– Drosophila larvae
– Unfortunate circumstances in humans
• WWII
– Dutch famine, Leningrad
• IRA starvation
Eckel RH. In: Obesity Mechanisms and Clinical Management. pp. 3-30, 2003

Long-Term Follow-Up of Behavioral Treatment for Obesity
Kramer, F.M. et al, Int J Obes 13:131, 1989

Prevalence of Weight Loss Maintenance in a Biracial Cohort: CARDIA
• n = 1869 overweight/obese subjects
– n = 536 (29%) lost 5% between 1995- 2000
• n = 180 (34%) maintained at least 75% between 2000- 2005
• n = 356 (66%) regained
• Predictors of success – African-American race, T2DM, moderate physical activity,
emotional support, reduced sugar-containing soft drinks
• Overall, 34% x 29% = 9% success in those that may have needed weight reduction
Phelan S et al, Am Jour Prev Med 39:546, 2010

Preservation of Weight Loss by Different Interventions
Svetkey LP t al, JAMA 299:1139, 2008
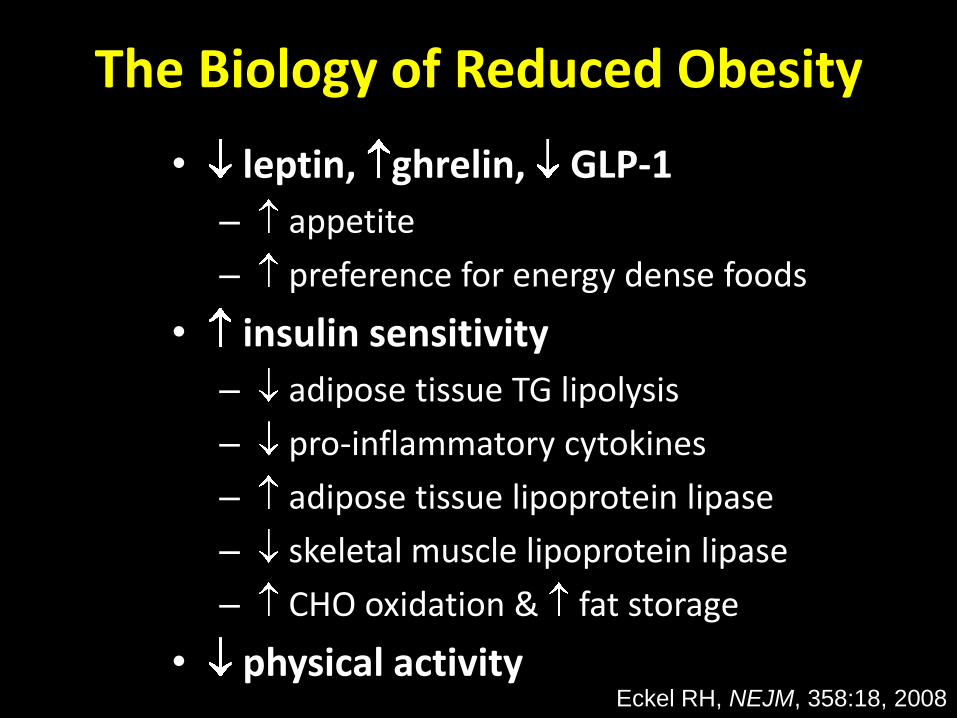
The Biology of Reduced Obesity
• leptin, ghrelin, GLP-1
– appetite
– preference for energy dense foods
• insulin sensitivity
– adipose tissue TG lipolysis
– pro-inflammatory cytokines
– adipose tissue lipoprotein lipase
– skeletal muscle lipoprotein lipase
– CHO oxidation & fat storage
• physical activity Eckel RH, NEJM, 358:18, 2008

Change in Adipose Tissue LPL in
Response to Insulin and/or Corn Oil
Normal Wt Obese Reduced Obese
-2
0
2
4
6
8
10
AT
LP
L (
nm
ol F
FA
/min
/10
6
ce
lls
) Insulin
Insulin + Corn Oil
Eckel RH and Yost TJ, JCI 80:892, 1987

Fasting SMLPL Activity in Normal
Weight and Obese Women
0
2
4
6
SM
LP
L (
nm
ol F
FA
/min
/g)
Normal Obese Weight
before after
p = 0.0001
Eckel RH et al, Eur JCI, 25:396, 1995

ATLPL and SMLPL Responses (0-6h) to a
High-CHO Diet on Changes in Weight and
Fat over 4 Years
Outcome Crude model P Adjusted for sex
and baseline BMI P
Effects of 0-6 h changes in ATLPL activity/cell
Weight change 0.002 0.014 0.751 0.006 0.009 0.332
Fat mass
change
0.049 0.033 0.093 0.040 0.019 0.013
% Fat change 0.049 0.021 0.026 0.036 0.015 0.006
Effects of 0-6 h changes in SMLPL activity/g
Weight change -0.057 0.029 0.060 -0.013 0.019 0.547
Fat mass
change
-0.135 0.067 0.021 -0.048 0.044 0.077
% Fat change -0.077 0.049 0.041 -0.034 0.034 0.056

fMRI, Reduced-Obese > Thin Overfeedng: Hedonic Foods > Basic Objects
Cornier M-Aet al, PLoS ONE, 2009

How much change in AT mass is needed to be
defended?
Let’s ask this question in walking-well normal weight women.

Subject Characteristics
Group Control
(n=18)
Lipectomy
(n=14)
P-value
Race 15C, 2AA,
1H
12C, 1H,
1Asian
NA
Weight (kg) 69.2 6.2 62.3 6.1 <0.005
BMI (kg/m2) 24.8 1.9 23.9 1.7 0.164
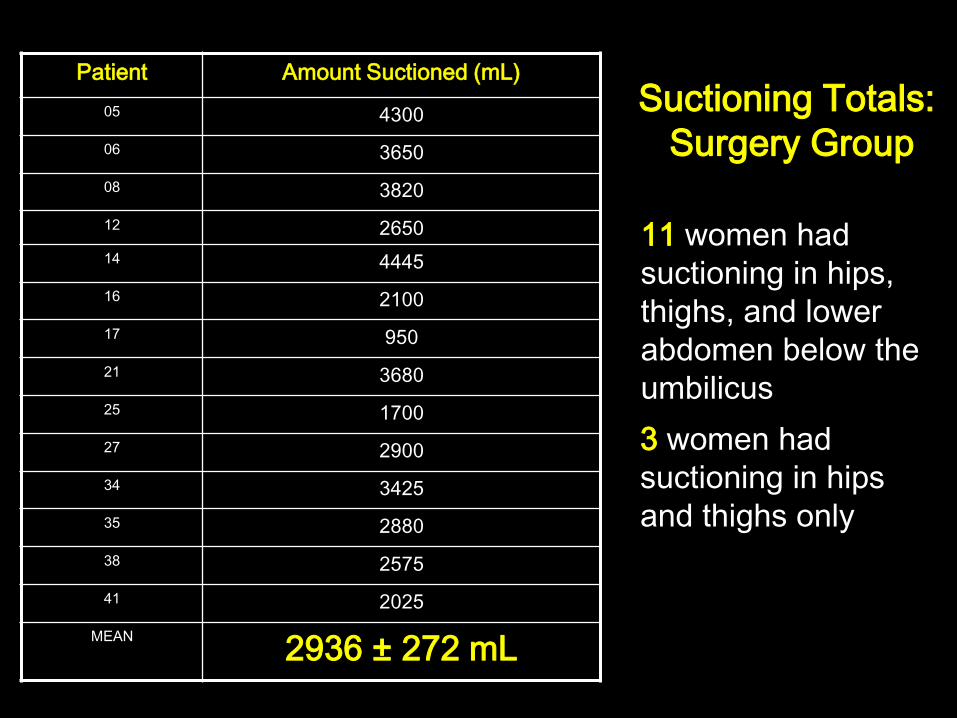
Patient Amount Suctioned (mL)
05 4300
06 3650
08 3820
12 2650
14 4445
16 2100
17 950
21 3680
25 1700
27 2900
34 3425
35 2880
38 2575
41 2025
MEAN
2936 ± 272 mL
Suctioning Totals:
Surgery Group
11 women had
suctioning in hips,
thighs, and lower
abdomen below the
umbilicus
3 women had
suctioning in hips
and thighs only

No Difference in Weight between Baseline and 1-Year
Question 1: Does fat come back?
55
60
65
70
75
Baseline 6 wk 6 mo 1 yr
Time
Weig
ht,
kg
Control (n=18) Liposuction (n=14)

-2.5
-2
-1.5
-1
-0.5
0
0.5
1
Control
Lipectomy
Ch
an
ge f
rom
Baseli
ne (
%)
6 wk 12 mo
Question 2: Where does the fat go?
Total Body % Fat Changes: DXA

Hip Circumference
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
Control
Lipectomy C
han
ge
s f
rom
Ba
se
lin
e (
cm
)
6 wk 12 mo
Thigh Circumference Changes
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
Control
Lipectomy
Ch
an
ge
s f
rom
Ba
se
lin
e (
cm
)
6 wk 12 mo
Mid Thigh Skin Fold Changes
-12
-10
-8
-6
-4
-2
0
2
Control
Lipectomy
Ch
an
ge
s f
rom
Ba
se
lin
e (
mm
)
6 wk 12 mo
Leg % Fat Changes
-4
-3
-2
-1
0
1
2
Control
Lipectomy
Ch
an
ge
s f
rom
Ba
se
lin
e (
%)
6 wk 12 mo
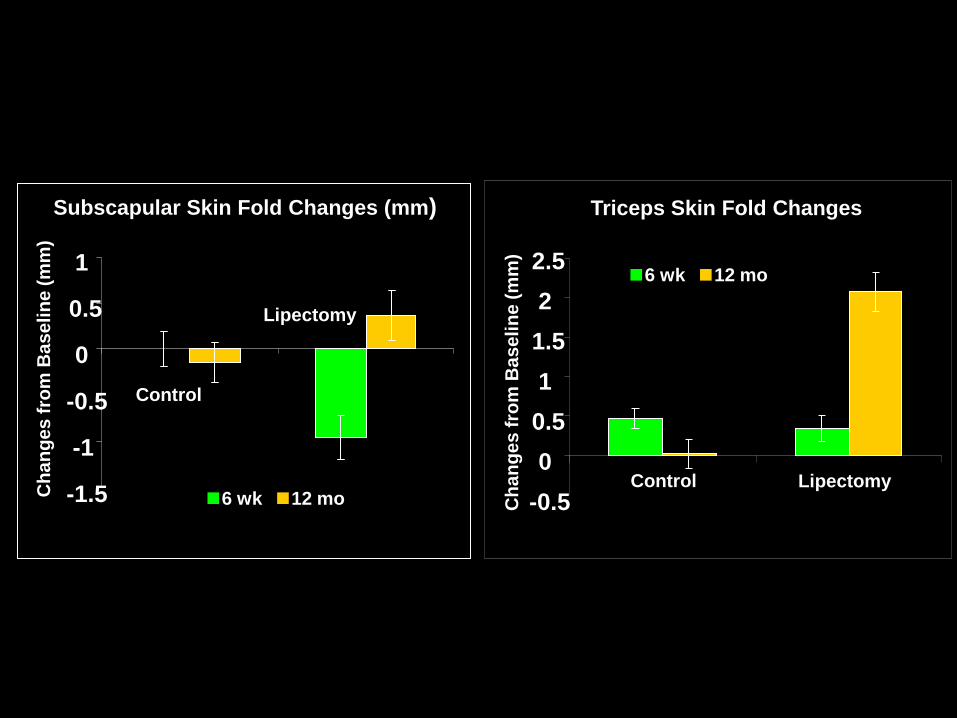
Subscapular Skin Fold Changes (mm)
-1.5
-1
-0.5
0
0.5
1
Control
Lipectomy
Ch
an
ge
s f
rom
Ba
se
lin
e (
mm
)
Triceps Skin Fold Changes
-0.5
0
0.5
1
1.5
2
2.5
Control Lipectomy
Ch
an
ge
s f
rom
Ba
se
lin
e (
mm
)
6 wk 12 mo
6 wk 12 mo

Changes in Fat by MRI
MRI - Pelvis Relative Fat Area
Changes
-5
-4
-3
-2
-1
0
1
6 wk
6 mo 12 mo
Ch
an
ges f
rom
Baseli
ne (
%)
Control Lipectomy
MRI - Thigh Relative Fat Area
Changes
-8
-6
-4
-2
0
2
6 wk 6 mo 12 mo
Ch
an
ges f
rom
Baseli
ne (
%)
Control Lipectomy

Changes in Abdominal Fat by MRI
MRI - Abdominal Subcutaneous
Relative Fat Area Changes
-6
-4
-2
0
2
4
6 wk
6 mo 12 mo
Ch
an
ges f
rom
Baseli
ne (
%)
Control Lipectomy
MRI - Abdomen Visceral Relative
Fat Area Changes
-
1
-
0.
5
0
0.
5
1
1.
5 6 wk
6 mo
12 mo
Ch
an
ges f
rom
Baseli
ne (
%)
Control Lipectomy

So even in walking-well normal weight women,
total body fat is defended one year after suction lipectomy - and perhaps in less favorable
locations!
Hernandez TL et al, Obesity 19:1388-95, 2011

Energy Intake = Energy Expenditure
Maintenance of Reduced Obesity

Weight Loss Maintenance in the National Weight Control Registry
• Self-reported group of 629 women and 155 men – lost an average of 30 kg – maintained a required minimum weight loss of 13.6
kg for 5 yr
• Weight loss achieved by – 50% a formal program – 50% on their own – Both groups reported having used both diet and
exercise – 77% reported a triggering event – 42% of the sample reported that maintaining their
weight loss was less difficult than losing weight.
Klem ML et al, AJCN 66:239, 1997
Predictors of Weight Loss Maintenance: NWCR
• Energy Intake – avoid frying
– substitute low-fat for high-fat
• Leisure Time Exercise – # of strenuous activities/wk
– # of sweat episodes/wk
• Restraint Scale – Concern about dieting
– Weight fluctuation
McGuire, M.T. et al, Obesity Res 7:334, 1999
Where’s the physician in this whole world of
prevention of weight regain after successful treatment of obesity?
Why Nutrition and Physical Activity Are Not Addressed by Physicians
1. Drugs and devices are available
2. Don’t think lifestyle changes work
3. Not enough knowledge about counseling
4. Insufficient time
5. Not reimbursed
6. Lack of staff (dietitians, exercise therapists)
Eckel RH, Circulation 2006, 13:2657

1. Being better informed about why patients are unsuccessful in losing weight
2. Understanding why they regain it
3. Learning about individual patients to help them modify their lifestyles
The Physician’s Ability to Influence
Weight Loss Depends on:
Eckel RH, Circulation 2006, 13:2657
The 3-Minute Physician Interview • Nutrition
– Daily servings of fruits and vegetables
– Daily servings of whole grains
– Weekly servings of fish
– Saturated and trans fat intake
– Snack foods, desserts
– Maximum weight?
– Food intake pattern
– Weight loss experience
– Weight loss desired?

The 3-Minute Physician Interview
• Physical Activity – Activity in the job place
• elevator, escalator, steps
– Planned activity • type and frequency
– Parking habits • close or far
– Limitations on physical activity – Would you like to increase your
physical activity?

Summary and Conclusions • Once obesity occurs, weight loss is
difficult to achieve and more difficult to
maintain.
– There is a strong metabolic basis for this.
– However, success can be achieved.
• The physician in addition to other
members of the health care team must
be involved.


![MECHANISMS IN ENDOCRINOLOGY Regulation of glucose ...Moreover, lowering the (ghrelin):(SST) ratio enhances ghrelin-induced [Ca2C] i mobilization. These data indicate that conditions](https://static.fdocuments.net/doc/165x107/6020a23db0143d6f48200891/mechanisms-in-endocrinology-regulation-of-glucose-moreover-lowering-the-ghrelinsst.jpg)















