Macro/micronutrients and Development
79
Macro/micronutrients and Development Dr Julian Eason Chair NICU Corniche Hospital, Abu Dhabi
Transcript of Macro/micronutrients and Development

Macro/micronutrients and Development
Dr Julian Eason
Chair NICU
Corniche Hospital, Abu Dhabi

Corniche Hospital
• 62 Bed NICU
• 8000 deliveries
• Tertiary referral for Fetal medicine and High Risk Maternity
• 1000 NICU admissions/year
• Vermont-Oxford since 1998, 250 infants <1500g
• 12 Consultants and 27 Specialists – UK Model of care
• 145 nurses and increasing
• Stand alone Maternity Hospital
• Paediatric facility Sheik Khalifa Medical City 3 miles away

Macronutrients
• LC-PUFA’s
• Nucleotides

Vitamin A
Thiamin
Riboflavin
Niacin
Folate
Manganese
Magnesium
Iron
Iodine
CobalaminCobalt
Zinc
Vitamin C
Vitamin E
Vitamin D
Vitamin K
Vitamin B6
Vitamin B12
Selenium
Chromium Phosphorus
Micronutrient deficiencies are common throughout the world not
just in developing countries

Effects from Defficiency
1. environment aspects
2. timing of deprivation
3. degree of defficiency
4. possibility of recovery

Statement
• Children who are not adequately nourished are at risk for failing to reach their developmental potential in cognitive, motor, and socio-emotional abilities.
• These abilities are strongly linked to academic achievement and economic productivity.

DHA and ARA
• LCPUFA are important for neuronal membrane integrity and function, and as well as vision may protect in BPD and NEC
• LCPUFAs, especially DHA, are involved in cell signalling, regulation of gene expression and neuronal growth
• Accretion is rapid in last trimester to support rapid growth and brain development
• Premature infants are deficient and remain so due to ineffective conversion, low stores and low supplies

Evidence
• Studies in animals show that lack of the long-chain polyunsaturated fatty acid docosahexaenoic acid (DHA) during periods of rapid brain growth may lead to impaired neurodevelopment
• Trials of the effect of DHA-fortified formula in babies have produced conflicting results.

Omega-3 and Omega-6 LCPUFA synthesis from precursor essential fatty acids
Vegetable oilsNutsSeeds
FlaxseedCanolaWalnutsSoy
Oily Fish
MeatEggs

Early Studies
• 1992 Lucas demonstrates breast fed infants have higher IQ than formula fed. 8.3 point advantage. Lancet 1992; 339(8788): 261–
264
• (Although these results could be explained by differences between groups in parenting skills or genetic potential (even after adjustment for social and educational factors), our data point to a beneficial effect of human milk on neurodevelopment)
• Fleith’s review of studies in 2005 says fewer than half of all studies have found beneficial effects of LCPUFA on visual, mental, or psychomotor functions. Crit Rev Sci Nutr 2005;45 (3) 205-29

Breast-feeding and cognitive development: a meta-analysis.
Anderson JW, Johnstone BM, Remley DT. Am J Clin Nutr 1999;70:525–35.
• Most studies have found that breastfeeding is associated with better cognition, but few adjusted for the confounding effect of maternal education and socio-economic status
• i.e. The educated breast feed so of course they score higher

Meta-analysis
• Mean difference in cognitive function between breast and formula fed infants
• 20 studies initially with 11 controlled
• Unadjusted benefit 5.32 (CI 4.51-6.16) increase in cognitive points
• Adjusted benefit 3.16 (2.35-3.98) increase
• Low birth weight infants showed a larger difference than normal birth weight 5.18 v 2.66 suggesting greater benefit in less mature infants
• Differences observed from 6 months to 15 years

Visual, cognitive and language assessments at 39 months: a follow up study of children fed formulae containing long-chain
polyunsaturated fatty acids to 1 year of age. Scott et al. Pediatrics 2003;112:e177-83
• In 276 term-born children
• Followed up at 39 months
• No differences were found in IQ, visual-motor skills or visual acuity between children randomised to LCPUFA-fortified formula in infancy than those randomised to unfortified formula and a breastfed comparison.

Randomized, double-blind trial oflong-chain polyunsaturated fatty acid supplementation with fish
oil and borage oil in preterm infants.Fewtrell MS, Abbott RA, Kennedy K, et al. J Pediatr 2004;144:471–9.
• 238 preterm infants
• LCPUFA-fortified formula was associated with higher scores on the Mental Development Index of the Bayley Scales at 18 months,
• only in boys
• overall there were no differences in neurodevelopment between the formula groups

Growth and development of preterm infants fed infant formulae containing docosahexaenoic acid andarachidonic acid. Clandinin MT, Van Aerde JE, Merkel KL, et al. J Pediatr 2005;146:461–8.
• 179 preterm infants
• LCPUFA-fortified formula was linked with significantly higher Bayley Scales scores at 18 months.
Effects of maternal docosahexaenoic acid intake on visual function and neurodevelopment in breastfed
term infants. Jensen CL, Voigt RG, Prager TC, et al. Am J Clin Nutr 2005;82:125–32.
• Trial examined the effect of supplementing breastfeeding women with DHA
• Children of supplemented women scored significantly higher than those of a control group on the Psychomotor Development Index of the Bayley Scales at age 30 months
• No difference in score on the Mental Development Index

Cognitive function in 18-month-old term infants of the DIAMOND study: a randomized, controlled clinical trial with
multiple dietary levels of docosahexaenoic acid. Drover et al. Early Hum Dev 2011; 87(3): 223–230.
• Double masked, randomised, controlled prospective trial
• 181 infants 1-9 days randomly assigned to 1 of 4 formulae:
• Control (0%DHA), 0.32% DHA, 0.64% DHA, 0.96% DHA
• All contained 0.64% ARA
• 12 months assignment
• 141 infants completed
• 131 children assessed at 18 months of age
Results
• No diet group differences on MDI, PDI or Behaviour Rating Scale (BSID 11)
• But when scores combined comparing supplemented to controls then significant MDI difference found
• 104.1 v 98.4 p=0.02
• Conclude need 0.32% DHA conc to make a difference

LCPUFA supplementation in infants born at term
Simmer Ke et al. Cochrane Library Dec 2011
• Conclusions
• Majority of the RCTS have not shown beneficial effects of LCPUFA supplementation on the neurodevelopmental outcomes of term infants. The beneficial effects on visual acuity have not been consistently demonstrated. Routine supplementation of term infant milk formula with LCPUFA can not be recommended.

Beyond Building better brains: bridging the
docohexanoic acid (DHA) gap of prematurityHarris et al. J Perinat (2015) 35, 1-7
• Selected conclusions:
• Pregnant and lactating women should take 200mg/day DHA via diet or supplement
• Formula should contain between 0.2 and 0.5% as DHA and ARA
• More DHA provision is required for preterm infants but exact dose not known

Nucleotides• Non-protein nitrogenous compounds found in high
concentrations in breast milk
• Conditionally essential nutrients in infancy
• Building blocks of nucleic acids
• Often thought to be a reason breast feeding confers benefits over formula feeding

Nucleotides supplementation and the growth of SGA infants. Cosgrove et al Arch Dis Child 1996; 74 F122-125
• Double blind RCT to see if catch up growth is improved with nucleotide supplementation
• 74 infants. 39 supplemented (4mg/100ml)
• From birth to 2 months
• Mean wt gain better in nucleotide supplemented group
• 106.3 v 94.7 g/kg baseline wt/week
• Continued over next 6 months

Dietary nucleotides and early growth in formula fed infants: A randomised controlled trial.
Singhal et al. Pediatrics 2010; 126e946
• OFC, weight and length
• Healthy singletons >37 weeks
• Nucleotide supplemented formula 37mg/l n=100 (birth – 20 wks)
• Control formula – no nucleotide n=100
• Breast fed reference group n=101
• Nucleotide group had increased OFC at 8, 16 and 20 weeks
• Weight and OFC greater in nucleotide group
• Supported hypothesis that nucleotides enhance weight gain and head growth in formula fed infants

Nucleotides
• Additional research is needed to test the hypothesis that the benefits of nucleotide supplementation for early head growth, a critical period for brain growth, have advantages for long-term cognitive development.

Iron
• Infants who experience iron deficiency during the first 6-12 mo of life are likely to experience persistent effects of the deficiency that alter functioning in adulthood.
• A lack of sufficient iron intake may significantly delay the development of the central nervous system as a result of alterations in morphology, neurochemistry, and bioenergetics.

Iron Deficiency Anaemia
• 2 Billion anaemic people (30% of global population) in the world are anaemic
• ID affects more people than any other condition in the world
• It remains silent despite more severe consequences than some other common conditions
• Haemoglobin, Ferritin, Enzymes

1.6
2.0
0.8
Population at Risk of Deficiency – GlobalUNICEF 2002

Preschool and pregnancy Iron defficiency UNICEF 2005
Pre-school Pregnancy
Mild 5-19% Moderate 20-39% Severe >40%Lebanon 20-30% 2008 study
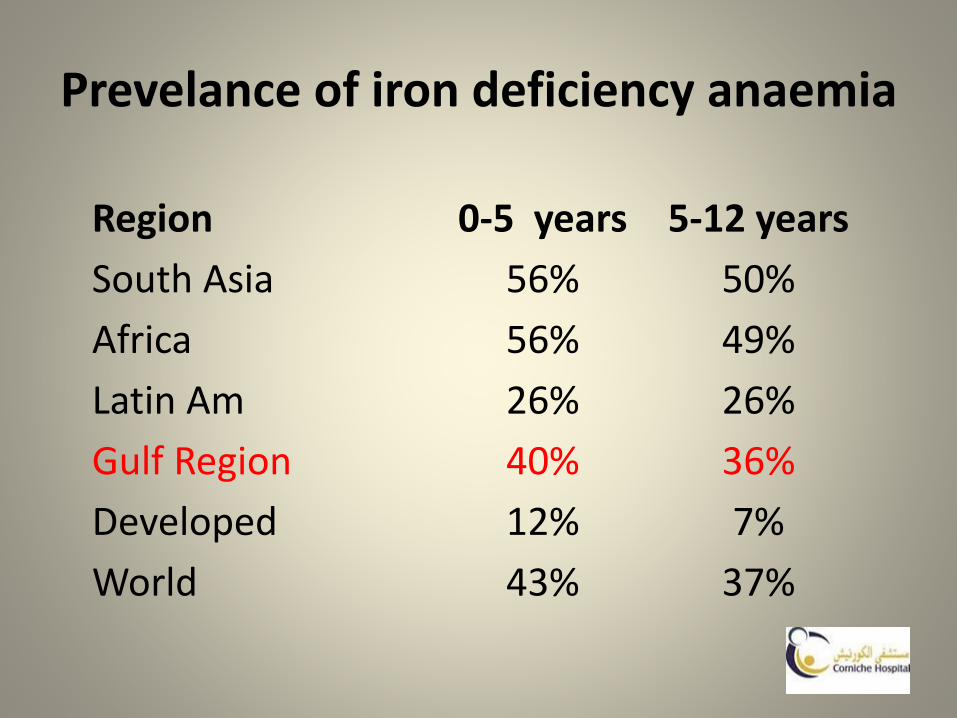
Prevelance of iron deficiency anaemia
Region 0-5 years 5-12 years
South Asia 56% 50%
Africa 56% 49%
Latin Am 26% 26%
Gulf Region 40% 36%
Developed 12% 7%
World 43% 37%

Newborn Iron Stores
• 75 mg/kg of iron at birth
• Dependent on haemoglobin concentration at birth (majority of iron in circulating RBCs)
• Minimally dependent on maternal iron status
• Depleted by 3 months in low birth weight infants without supplementation
• Depleted by age 5-6 months in term infants
• Delayed cord clamping (by 2 minutes) leads to higher ferritin and iron stores at 6 months of age

Cows Milk and Iron Defficiency
• Poor source of iron
• Poor absorption (5-10%)
• Reduces consumption of other foods, especially with overconsumption
• Can cause microscopic GI bleeding

Recent evidence from human and animal studies regarding iron status and infant development.
J Nutr. 2007 Feb;137(2):524S-530S.
• Infants are at risk for iron deficiency as breast milk or formula is replaced by semisolid foods during weaning
• A lack of sufficient iron intake may significantly delay the development of the central nervous system because of alterations in morphology, neurochemistry, and bioenergics.
• Depending on the stage of development at the time of iron deficiency, there may be an opportunity to reverse adverse effects, but the success of repletion efforts may be time dependent.

Conclusions
• Data in monkeys show significant effects on neurodevelopment with dietary iron deficiency.
• Findings in human infants are consistent with altered myelination and changes in monoamine functioning.
• Rodent studies show that effects of iron deficiency during gestation and lactation persist despite restoration of iron status at weaning.
• These cross-species studies indicate a vulnerable period in early development that may result in long-lasting damage

Why iron deficiency is important in infant development.Beard JL. J Nutr. 2008 Dec;138(12):2534-6.
• Depending on the stage of development at the time of iron deficiency, there may be an opportunity to reverse adverse effects, but the success of repletion efforts appear to be time dependent.
• Publications in the past several years describe the emerging picture of the consequences of iron deficiency in both human and animal studies.
• The data in human infants are consistent with altered myelination of white matter, changes in monoamine metabolism in striatum, and functioning of the hippocampus.
• These studies indicate that gestation and early lactation are likely critical periods when iron deficiency will result in long-lasting damage.
Iron supplements reduce impaired neurodevelopment in LBW babies
Berglund et al. Pediatrics 2012
• RCT 285 marginally LBW infants (<2,500 g)
• Placebo or either 1 mg/kg or 2 mg/kg of ferrous succinate per day
• 6 weeks to 6 months.
• A 3.5-year follow-up, psychometric test to determine verbal, performance, and full-scale IQ. Parents completed a checklist questionnaire for behaviouraland emotional problems.

Results
• No significant differences in cognitive scores among the 3 groups of LBW infants compared with controls.
• Infants who received the 1 mg/kg and 2 mg/kg iron supplements were significantly less likely (2.9% and 2.7%, respectively) to score above the subclinical cutoff for behaviour problems than infants given placebo (12.7%).
• The rates for LBW infants given supplements were similar to the rate for babies of normal birth weight (3.2%).
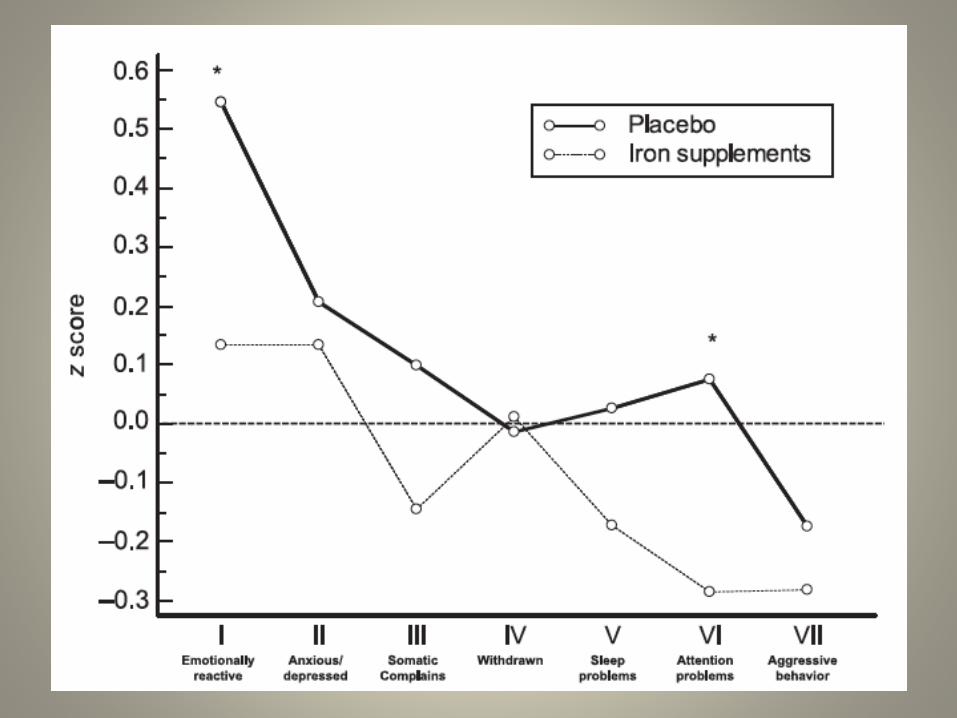

Conclusion
• Early iron supplementation of marginally LBW infants does not affect cognitive functions at 3.5 years of age but significantly reduces the prevalence of behavioural problems.
• The study suggests a causal relation between infant iron deficiency and later behavioral problems.

Enteral iron supplementation in preterm and low birth weight infants.
Mills R, Davies M. Cochrane Database of Systematic Reviews 2012; Issue 3.
• To evaluate the effect of prophylactic enteral iron supplementation on growth and neurodevelopmental outcomes in preterm and low birth weight infants.
• 26 studies, 2672 infants
• 21 studies comparing iron with controls did not look at neurodevelopment
• 1 of 13 looking at growth found a week correlation
• 1 study looking at high and low dose iron found no neurodevelopmental difference
• No haematological difference between 2 or 3 mg/kg/day

Prevention?
• Delayed cord clamping
• Breastfeeding for the first 6 months of life
• Iron fortified formula/cereals
• Iron supplementation for preterm infants
• Iron supplementation for breastfeeding infants at 4 months of age
• Avoid cows milk before 1 year of age ? longer
• Limit cows milk intake to 500mls/day after 12 months of age

Conclusion
• It remains unclear whether iron supplementation in preterm and low birth weight infants has long term benefits in terms of neurodevelopmental outcome and growth.
• Infants who receive iron supplementation have a slightly higher haemoglobin level, improved iron stores and a lower risk of developing iron deficiency anaemia when compared with those who are unsupplemented

Vitamin A
• Fat soluble vitamin with multiple roles
• Roles in cell differentiation, vision, immune function, reproduction, bone formation and growth
• Animal and plant sources

Vitamin A
• Vit A defficiency associated with childhood morbidity, mortality but well know as leading cause of preventable blindness
• 500 million children blinded and many die within one year of blindness

0.0
0.5
1.0
1.5
2.0
2.5
Iodine Iron Vitamin A
People(billions)
1.6
2.0
0.8
Population at Risk of Deficiency – GlobalUNICEF 2002
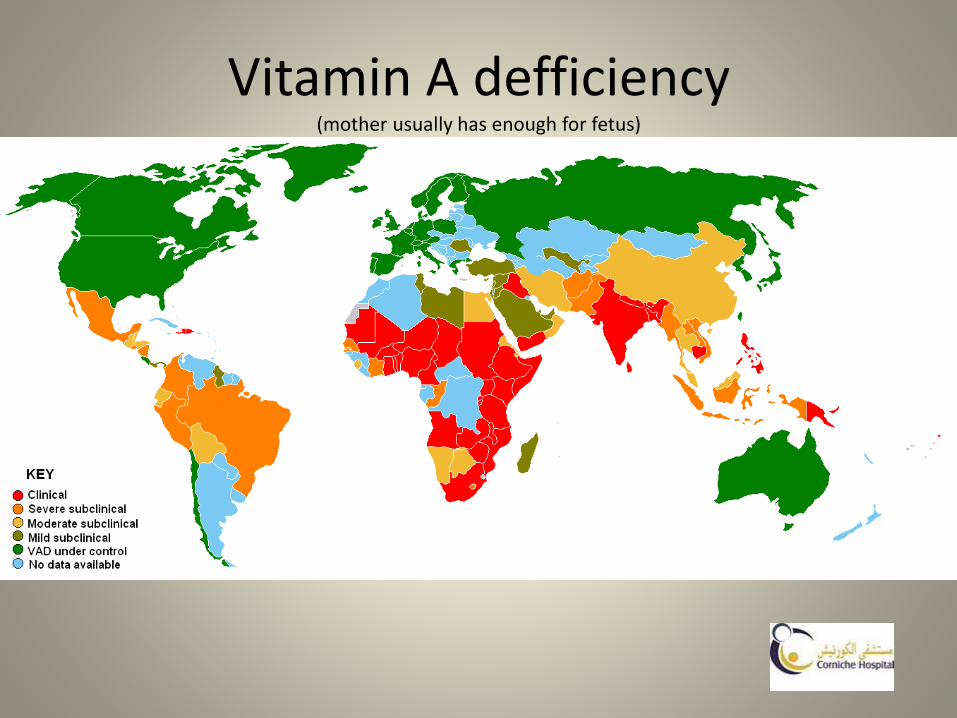
Vitamin A defficiency(mother usually has enough for fetus)

Cochrane reviewDarlow et al 2011
• Nine trials reviewed
• Vit A IM or in formula associated with trend reducing death and oxygen requirement at 1 month of age
• Some associated with reduced ROP
• One trial show no difference in neurodevelopment at 18 months

Iodine
• Defficiency is a cause of mental retardation
• Iodized salt still not universal
• Iodine essential for T4 production and is crucial for brain development
• Thyroid hormone regulates basic metabolism :energy consumption, cellular activity, growth and in particular brain development.

Spectrum of Disease
The Spectrum of Iodine Deficiency Disorders, IDD.
Fetus Abortions
Stillbirths
Congenital anomalies
Increased perinatal mortality
Endemic cretinism
Neonate Neonatal goitre
Neonatal hypothyroidism
Endemic mental retardation
Increased susceptibility of the thyroid gland
to nuclear radiation
Child and Goitre
adolescent (Subclinical) hypothyroidism
Impaired mental function
Retarded physical development
Increased susceptibility of the thyroid gland
to nuclear radiation
Adult Goitre with its complications
Hypothyroidism
Impaired mental function
Spontaneous hyperthyroidism in the elderly
Iodine-induced hyperthyroidism
Increased susceptibility of the thyroid gland
to nuclear radiation
Adapted from Hetzel , Laurberg et al. and Stanbury et al.

Iodine deficiency and the foetus
• Brain development fast between 3-5 months pregnancy and from third trimester till end of second year
• Maternal T4 essential for first 24 weeks
• Foetal T4 starts at 24 weeks
• 30% cord blood is of maternal origin

Iodine and the neonate
• Perinatal mortality
• Infant mortality
• Low birth weight
• Brain development needs T4
• Iodine deficiency mental retardation, retarded motor development.
• General IQ decrease of 15 Points

Implementation of Salt Iodisation

THORN study
• Thyroid Hormone Replacement in Neonates• Biswas et al Pediatric Research (2003) 53 48-56
• 250 infants
• Administration of triiodothyronine (T3) and hydrocortisone would decrease mortality and respiratory morbidity in preterm infants of less than 30 wk gestation
• Raised FT3 and TT3 levels by T3 supplementation but in doing so, suppressed FT4, TT4, and TSH levels
• No beneficial effects

I2S2 A randomised controlled trial of iodine supplementation in preterm infants. 2015
• I2S2 trial is a multi-centre randomised controlled trial of iodine supplementation in extreme preterm infants. It aims to answer whether iodine supplementation of parenterally or entrally fed infants can improve neurodevelopmental outcome at 2.0 years corrected age.
• Supplementation of parenterally or entrally fed infants with sodium iodide or placebo (sodium chloride) supplied by the study (0.4 ml/kg/dose/day; 30 micrograms iodide/chloride per kg/day); randomised within 42 hrs of birth; individual infants will be involved from birth until 34 corrected weeks gestation
• All infants born <31 weeks gestation, up to 42 hours old
Results
• Results being presented at REaSoN meeting UK July 2016

Zinc Deficiency
Zinc is essential for the function of many enzymes and
metabolic processes
Zinc deficiency is common in developing countries with high
mortality
Zinc is commonly the most deficient nutrient in
complementary food mixtures fed to infants during weaning
Zinc interventions are among those proposed to help reduce
child deaths globally by 63% (Lancet, 2003)

Distribution
• Whole body: 1.5g (female)-2.5g (male)
– Skeletal Muscle 57%
– Bone 29%
– Skin 6%
– Liver 5%
– Brain 1.5%
– Kidneys 0.7%
– Heart 0.4%
– Hair ~0.1%
– Blood Plasma ~0.1%

Overview• Approximately 300 enzymes are associated with zinc• Biological functions of Zn are divided into three
categories– Catalytic, Structural, Regulatory
• Role in metabolism– Protein synthesis– Nucleic acid metabolism– Carbohydrate and energy metabolism– Lipid– Epithelial tissue integrity– Cell repair and division– Vitamin A and E transport and utilization– Immune function– Reproductive hormones

Deficiency
Malformations in Zn deficiencyCleft lipCleft palateBrain(Hydrocephaly, anencephaly or exencephaly)
Micro- or agnathiaMicro- or anopthalmiaClubbed feetA- or syndactylyCurly or stubby tailDorsal herniationHeart (abnormal position)
Lung (missing lobes)
Urogentital(Hydronephrosis, absent kidney, or malposition)

Zinc Deficiency- Signs & Symptoms
Hair loss
Skin lesions
Diarrhoea
Poor growth
Acrodermatitis enteropathica
Death

Zinc Deficiency- Treatment
Regular zinc supplements can greatly reduce common infant
morbidities in developing countries
• Adjunct treatment for diarrhoea
• Pneumonia
• Stunting
Zinc deficiency commonly coexists with other micronutrient
deficiencies including iron, making single supplements
inappropriate

Zinc, Copper and Manganese blood levels in preterm infants
Marriott et al Arch Dis Child Neo Ed. 2007; 92: F494-97
• 68 infants
• Levels at EDD and 6 months later
• Mean wt 1.47kg and gestation 31.4 weeks
• New levels defined
• Helps manufacturers and those on TPN

Vitamin D
• Rickets
• Osteoporosis
• Fractures
• Maternal depression and PET
• Developed Arab Gulf countries carry a high prevalence of hypo-vitaminosis D, a finding possibly explained by cultural practices and skin pigmentation Bone 39 (2006) 1136-43
Vitamin D
• Vit D during pregnancy essential for skeletal development, tooth enamel as well as general growth and developmentIf a mother is deffiecientthen so is the infant.
• Cord 25 OH D asoc with inc OFC at 3 and 6 mo
• Defficiency worse in breast fed, no supplementation and limited sunlight
• 400IU, 600IU, 800IU, 1200IU
• Ref IJMR 2011 Mar; 133(3): 2560-52

Effects of Micronutrient supplementation on linear growth of children
• Br J Nutr 2001 – review showing small or no benefits in supplementation
• Am J Clin Nutr 2008 – review looking at <5years age. Little iron and Vit A effect but some with zinc
• BMJ Open 2014 – metanalysis of zinc and iron showing little or no differences in mortality, illness and side-effect
The Long Term Impact of Micronutrient Supplementation during Infancy on Cognition and Executive Function Performance in Pre-
School Children Warthon-Medina M et al. Nutrients 2015 7; 7 (8) 6606-6627
• RCT Multiple nutrient supplementation compared to Iron alone
• Lima, Peru 2010 902 infants 6-17 months getting either Iron or MMN (multiple micronutrients inc Zinc)
• 6 months treatment
• 2012 184 subsample randomly selected to look at intelligence, memory, inhibition and exec function
• No differences between groups but gender differences in that girls better at all except more males with problem behaviours
• So no effect or wrong time to supplement?

children go blind or die
each year from
vitamin A deficiency
1.1 million
600,000stillbirths due to
iron deficiency
18 millionbabies born mentally
impaired due to maternal
iodine deficiency
of world population
estimated to be
vitamin D deficient
40-75%
38 million
women estimated to
be affected by
osteoporosis worldwide
200 million
deaths due to
noncommunicable diseases
Micronutrient Deficiencies:The Impact in Numbers

• 38 million global deaths in 2012 due to NCDs predicted to be 58 million in 2030
• (CVS, Chronic Resp, Cancer, Diabetes)• Worldwide:
– 366 million people have diabetes– 200 million people have osteoporosis– 1.6 billion people are overweight
• 80% of premature heart disease, stroke & diabetes can be prevented
• Diet is an important modifiable factor
Micronutrient Deficiencies:Link to Noncommunicable Diseases

Summary
• Major risk factors for micronutrient deficiency diseases around the world include poor dietary intake, infection, disease and sanitation
• The 4 major MDDs are iron (folate), iodine, vitamin A, and zinc
• Treatment for MDD include dietary diversification, supplementation, and food fortification
Thank you
• Research continues to help fine tune appropriate recommendations for supplementation in vulnerable infants

Does correcting a deficiency correct the underling developmental problem?
A. Always
B. Never
C. Sometimes
D. If given at the correct time
A. B. C. D.
0% 0%0%0%
10

Accretion of LC PUFA’s is greatest in which trimester supporting brain growth and development?
A. First Trimester
B. Second Trimester
C. Third Trimester
D. Second and Third Trimester
A. B. C. D.
0% 0%0%0%
10

Which are a natural source of precursors for LC PUFA’s?
A. Meat and eggs
B. Fish
C. Seeds and nuts
D. Cereals
A. B. C. D.
0% 0%0%0%
10

Early onset iron deficiency has knock-on effects into adult life?
A. Is rare
B. Is easily corrected
C. Has no clinical consequences
D. Can be associated with behavior
A. B. C. D.
0% 0%0%0%
10
The prevalence of Iron deficiency worldwide is?
A. >30%
B. >40%
C. >50%
D. >60%
A. B. C. D.
0% 0%0%0%
10

Vitamin A is available from?
A. Plants only
B. Animals only
C. Plants and Animals
D. Sunlight
A. B. C. D.
0% 0%0%0%
10

Supplementing Thyroxine in the preterm infant can improve cognition?
A. Always
B. Sometimes
C. Never
D. If given before 34 weeks gestation
A. B. C. D.
0% 0%0%0%
10
Iodine is best supplemented in?
A. Flour
B. Water
C. Salt
D. Pepper
A. B. C. D.
0% 0%0%0%
10

Vitamin D deficiency:
A. Is uncommon
B. Affects more males
C. Is common in equatorial countries
D. Has no long term effects
A. B. C. D.
0% 0%0%0%
10

Food fortification examples include:
A. Magnesium
B. Selenium
C. Folate
D. Copper
A. B. C. D.
0% 0%0%0%
10

![6[1].9 macro & micronutrients in plants](https://static.fdocuments.net/doc/165x107/548911f8b47959d80c8b584f/619-macro-micronutrients-in-plants.jpg)