MA STAAR Learning Session Creating an Ideal Transition to Home by Working with Clinical Office...
26
MA STAAR Learning Session Creating an Ideal Transition to Home by Working with Clinical Office Practices, Home Health, and Community Agencies Gail Nielsen, Amy MacNulty, Pat Kelleher, Helen Siegel
-
Upload
marcus-mckinney -
Category
Documents
-
view
217 -
download
1
Transcript of MA STAAR Learning Session Creating an Ideal Transition to Home by Working with Clinical Office...

MA STAAR Learning Session
Creating an Ideal Transition to Home by Working with Clinical Office Practices, Home Health, and
Community Agencies
Gail Nielsen, Amy MacNulty, Pat Kelleher, Helen Siegel

Session Objectives
Participants will be able to: • Describe the role community providers can play
in improving transitions in care• Discuss specific strategies for enhancing care
coordination with clinical office practices, home health, and community agencies

Transitions Home
• Small Group work:─Describe how a patient and/or family member
would (ideally) experience care as they transition home (i.e., what they might want and need?)
─ Identify three things that you will need to do in order to deliver that ideal system for your patients (i.e., processes that you will have to put in place)
• Report out on your discussions

Digging In-Open Mind
Perform an in-depth review of the last five rehospitalizations to identify opportunities for improvement
• Conduct chart reviews of the last five readmissions, transcribing key information onto the data collection sheets (see Worksheet A).
• Conduct interviews with patients recently readmitted and their family members (If possible, interview the same patients whose charts were reviewed). Next, conduct interviews with clinicians in the community who also know the readmitted patient (physicians, nurses in the skilled nursing facility, home care nurse, etc.) to identify problem areas from their perspective. Transcribe information from these interviews onto the data collection sheet (see Worksheet B).

Digging In-Open Mind
Review patient experience data regarding communications and discharge preparations to identify opportunities for improvement
• Evaluate trends in the scores of the communication and discharge preparation questions on your patient satisfaction or patient experience survey for the last year. Assess survey scores both for the hospital and each medical and surgical unit, when possible. Use the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) or tailored hospital survey questions, if equivalent. Refer to www.hcahpsonline.org for the complete list of HCAHPS questions.

Opportunities Discovered through Diagnostics (OP)
• Primary or specialty care physician does not know his or her patient has been admitted or discharged because of the lack of an alert system from hospital to office
• Patient is told to schedule an appointment with his or her primary or specialty care provider, but is confused about whom he or she should see, when, and why
• Failure of the office practice care team to recognize and provide support for patients with a low capacity for self-care due to low health literacy, financial barriers, other social problems, alternative health beliefs, substance abuse, or mental illness
• Home health care agencies, skilled nursing facilities and other supportive services are not provided with an updated care plan for their past/current patients.

Opportunities Discovered through Diagnostics (HH)
• Inadequate completion of comprehensive assessment, problem identification and care plan development
• Patient and family/caregiver unable to overcome challenges to manage self-care and medications-knowledge, cognitive and functional challenges, financial constraints, problem solving
• When primary care physician is designated as the lead clinician, often they are not current on hospitalization, discharge instructions and current status
• Too many ―care managers calling post-discharge, which can be confusing and/or overwhelming to the patient and family caregivers

Transitions Home
• Small Group work:─At your table, identify typical gaps in your
clinical setting (3 or more!)
─What have you seen? What gets in the way of patients getting what they need?
• Report out on your discussions

Working Across the Continuum
By understanding mutual interdependencies at each step of the patient journey across
the care continuum, the team will codesign processes to improve transitions in care. Collectively, team members will explore the ideal flow of information and patient
encounters as the patient moves from one setting to the next and then home.


or
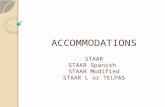
IHI’s Roadmap for Improving Transitions and Reducing Avoidable Rehospitalizations
* Additional Costs for these Services
Improved Transitionsand Coordination of Care
Reduction in Avoidable Rehospitalizations
Patient and Family Engagement
Cross-Continuum Team Collaboration
Evidence-based Care in All Clinical Settings
Health Information Exchange and Shared Care Plans

Improving Transitions to the Clinical Office Practice
1. Provide Timely Access to Care Following a Hospitalization
2. Prior to the Visit: Prepare Patient and Clinical Team
3. During the Visit: Assess Patient and Initiate New Care Plan or Revise Existing Plan
4. At the Conclusion of the Visit: Communicate and Coordinate On-going Care Plan

1. Provide Timely Access to Care Following a Hospitalization
A. Review on a daily basis information received from the hospital about admissions and anticipated discharges
B. Provide appropriate level and type of follow-up for high-risk, medium-risk and low-risk discharged patients

2. Prior to the Visit: Prepare Patient and Clinical Team
A. Review the discharge summary
B. Clarify outstanding questions with sending physician(s)
C. Place a reminder call to patient or family caregiver to help them prepare for the visit
D. Coordinate care with home healthcare nurses and case managers if appropriate

3. During the Visit: Assess Patient and Initiate New Care Plan or Revise Existing Plan
A. Ask the patient about his/her goals for the visit, what factors contributed to hospital admission or ED visit, and what meds he/she is taking and on what schedule
B. Perform med rec with attention to the pre-hospital regimen
C. Determine need to adjust meds or dosages, follow-up on test results, do monitoring or testing, discuss advance directives, discuss specific future treatments
D. Instruct patient in self-management, have patient repeat back
E. Explain warning signs and how to respond, have patient repeat back
F. Provide instructions for seeking emergency and non-emergency after-hours care

4. At the Conclusion of the Visit: Communicate and Coordinate Ongoing Care Plan
A. Print reconciled, dated medication list and provide a copy to the patient, family, home health care nurse, and case manager (if appropriate)
B. Communicate revisions of the care plan to the patient, family caregiver, home health care nurse, and case manager (if appropriate)
C. Ensure that the next appt is made, as appropriate

Improving Transitions to Home Health Care
1. Meet the Patient, Family Caregiver(s), and Inpatient Caregiver(s) in the Hospital and Review Transition Home Plan
2. Assess the Patient, Initiate Plan of Care and Reinforce Patient Self-Management at the First Post-Discharge Home Care Visit
3. Engage, Coordinate, and Communicate with the Full Clinical Team

1. Meet the Patient, Family Caregiver(s), and Inpatient Caregiver(s) in the Hospital and Review Transition
Home Plan
A. Whenever possible, the home health care nurse or liaison meets the patient, family caregivers, and at least one inpatient caregiver in the hospital and reviews the transition home plan. It is important to identify and collaborate with the appropriate responsible caregiver whenever possible.
B. Reinforce to patient, family caregiver(s), and inpatient caregiver(s) that a follow-up appointment be made before discharge to assure timely follow-up after hospitalization with primary care or managing clinician.

2. Assess the Patient, Initiate Plan of Care, and Reinforce Patient Self-Management at
First Post-Discharge Home Care Visit
A. Re-evaluate the patient’s clinical status since leaving the hospital.
B. Reconcile all medications, including all meds in the home.
C. Assess, reinforce, and improve patient and family caregiver’s understanding and ability to manage medications and self-care with Teach Back.
D. Initiate treatments as ordered (e.g. dressing changes, O2 saturation, wound care).

3. Engage, Coordinate, and Communicate with the Full Clinical Team
A. Assure that there is proactive, consistent, real-time consultation with primary care provider or other managing clinician(s).
B. Use a patient-centered health record to communicate to all caregivers.
C. Advocate as necessary to assure referrals are completed and needed services are received.

Identify Opportunities
• Observe patients and staff during discharge handovers
• Seek information on usefulness of handover information
• Exchange visits with community partners: “Go See” and observe together
• Review cases of readmitted patients with community providers
• Interview readmitted patients and their families: what didn’t work well?

Your Turn to Plan
• Create your initial action plan using the ACTION PLANNING FORM
• Document plans for your first test of changes using the PDSA FORM


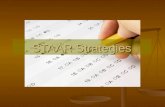
A P
S D
PDSA Worksheet Team Name:__________________Cycle start date:_________ Cycle end date:__________
PLAN: Area to work on: Describe the change you are testing and state the question you want this test to answer (If I do x will y happen?)What do you predict the result will be?What measure will you use to learn if this test is successful or has promise? Plan for change or test: who, what, when, whereData collection plan: who, what, when, where
DO: Report what happened when you carried out the test. Describe observations, findings, problems encountered, special circumstances.
STUDY: Compare your results to your predictions. What did you learn? Any surprises?
ACT: Modifications or refinements for the next cycle; what will you do next?


What is one new thing you learned
today that you would like to test?