
M7: Managing Conflict on Health Care Teams -...
36
3/15/2015 1 M7: Managing Conflict on Health Care Teams Institute for Health Care Improvement March 15, 2015 Nan Cochran, MD Neil Baker, MD Calvin Chou, MD, PhD These presenters have nothing to disclose. Objectives 1. Explain how to build relationships while negotiating 2. Define differences between interests and positions 3. Identify ways to separate fact from assumptions and stories 4. Practice identifying and using emotions during conflict 5. Demonstrate how to negotiate in the face of differences in authority
Transcript of M7: Managing Conflict on Health Care Teams -...

3/15/2015
1
M7: Managing Conflict on
Health Care TeamsInstitute for Health Care Improvement
March 15, 2015
Nan Cochran, MD
Neil Baker, MD
Calvin Chou, MD, PhD
These presenters have nothing to disclose.
Objectives
1. Explain how to build relationships while negotiating
2. Define differences between interests and positions
3. Identify ways to separate fact from assumptions and
stories
4. Practice identifying and using emotions during conflict
5. Demonstrate how to negotiate in the face of differences in
authority

3/15/2015
2
Gawande, A. Cowboys and Pit Crews The New Yorker, 2011
Staffing on hospital teams to care for one patient:
1970’s 2.5 FTE
“Medicine’s complexity has exceeded our individual capabilities as doctors.”
Increased complexity in care
1990’s 15 FTE
Conflict
• “Real or apparent
incompatibility of
parties’ needs or
interests”
• How much of health
care workers’ time is
spent in conflict?Rosenstein et al, Am J Nursing 2005;
O’Mara, Emerg Med Clin N Am 1999

3/15/2015
3
Negative consequences of conflict
• Lower job satisfaction
• Decreased well-being
• Higher perceived stress
• Sleep deprivation
• Use of alcohol and
medications as coping
strategies
Conflict affects patient safety
• Dysfunctional team dynamics
lead to more than 70% of
medical errors
• Disruptive behavior leads to
– Poor patient satisfaction
– Increased costs of care
– Decreased staff retention rates

3/15/2015
4
I experienced conflict that I found
difficult in the last month
A. True
B. False
I experienced conflict that could have
compromised patient care in the last
month
A. True
B. False

3/15/2015
5
Exercise – what is most
challenging about conflict?
• Take 2 minutes to think about what is most
challenging about conflict to you
• Share with a partner, 4” each
• Then, share at your table
• Large group debrief
Relational Task
Different kinds of conflict
Process

3/15/2015
6
Conflict Styles
Thomas-
Kilmann
Conflict
Styles

3/15/2015
7
A story

3/15/2015
8
Why is conflict so hard?
Reactivity
Ladder of Inference
CONCLUSIONS, ACTIONS
JUDGMENTS, ASSUMPTIONS, OPINIONS
SELECTION OF DATA
OBSERVABLE DATA AND EXPERIENCE

3/15/2015
9
Ladder of InferenceCONCLUSIONS, ACTIONSI can’t work with Chris; he is totally unmotivated; it’s time to get rid of him.
JUDGMENTS, ASSUMPTIONS, OPINIONSChris is slacking off, totally disengaged and does not care about our team.
SELECTION OF DATAChris is constantly late to our staff meeting and never apologizes or explains.
OBSERVABLE DATA AND EXPERIENCEI have worked with Chris for 2 years. I see he comes to a staff meeting late for the third time in a row. This last week I have worked until about 9 pm every night.
Climb Down the Ladder
Take a step back:
• What was the observable data?
• Do we agree on the data?
• What assumptions did I make?
• What conclusions did I draw?
• How did those conclusions influence my subsequent
observations?

3/15/2015
10
Caution! Flawed assumption:Feelings don’’’’t matter.
Watch for body language
Created by Neil Baker M.D. for AACH

3/15/2015
11
Watch for “I feel that….…you have poor judgment.””””
(judgments)
…it’s your fault!””””(blame)
…you are attacking me!””””(attributions)
…you are passive-aggressive.””””(generalizations)
…the answer is…””””(cognitive)
Bundles of
feelings and
thoughts
Created by Neil Baker M.D. for AACH
Name feelings - modulate your intensity
High intensity
Pissed off
Angry
Shocked
Low intensity
Concerned
Unsettled
Puzzled
Created by Neil Baker M.D. for AACH

3/15/2015
12
Self-reflective practices
• PAUSE to observe within
• Create a habit of using self-reflective questions
• Find ways to relax
• Practice meditation
• Try journaling
• Know your dominant conflict styles
• Consult with colleagues
• Prepare for difficult conversations
Ladder of Inference Exercise
• Choose an interpersonal situation that was difficult for you - perhaps the relationship you have with the other person is challenging or you regret something you said or did
• Choose a situation that felt important, that is likely to recur and that you are willing to learn from
Potential conflicts:• you can't reach agreement with your colleagues or with a patient
• someone is not pulling his or her weight on a team
• you believe you are being treated unfairly by your boss or supervisor
• you believe your point of view is being ignored

3/15/2015
13
Ladder of Inference Exercise
• What assumptions did you make that contributed
to the conflict?
• Seek disconfirming data!
Perspective

3/15/2015
14
Relationship affects conflict and vice versa
• Conflict in medical teams and in patient care often involve interpersonal incompatibilities
• Detracts from effective functioning
Greer et al, 2012; Kalishman et al, 2012
Negotiating Differences
Ask
Respond
Tell
Summarize

3/15/2015
15
Negotiating Differences
ARTS of Communication
• Ask the other’s perspective – use active listening
• Respond with empathy and reflective listening
• Tell your perspective and your interests
• Summarize your understanding of the other’s perspective, their interests
• Seek solutions--generate options
Negotiating Differences:
ARTS of Communication
• Ask the other’s perspective – use active listening
Distinguish interests from positions
• Respond with empathy and use reflective listening
• Tell your perspective and your interests– Beware of assumptions
• Summarize your understanding of the other’s perspective, their interests and focus on shared interests
• Seek solutions - generate options
3/15/2015
16
Goals of Active
Listening
• Help a speaker feel heard, understood
• Encourage exploration at a deeper level
• Strengthen the relationship
• Understand different perspectives
• Show respect
Listen, don’t reload!
And listen to yourself
• Understand your anger and other feelings beforeengaging in a difficult conversation
• Negotiate with your feelings • What assumptions am I making?
• What story am I telling myself about their intentions?
• Describe your feelings carefully, and gently
• Use “I” statements - “You …” statements often heard as blaming
“I feel angry” vs “ You make me so angry”

3/15/2015
17
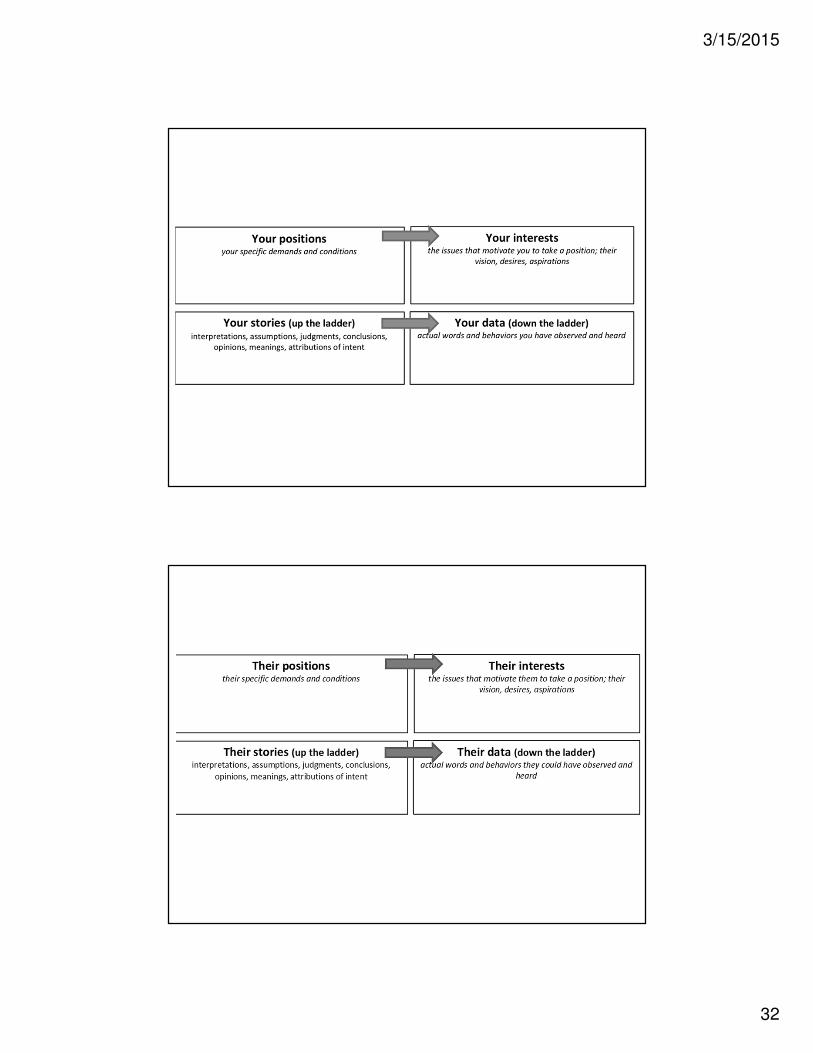
Interests
Positions
Relational Task
Different kinds of interests
Interests
Process
3/15/2015
18
Ask about positions and underlying
interestsPositions
• What we want, need, think,
or feel
• Drawing a line in the sand
• Basis for debate
“I can’t let Bobby transition to
the adult team”
“ Why 4 mandatory visits per
year?”
Interests
• The motivations for our
positions: our needs,
desires, concerns, fears,
aspirations
• Basis for dialogue
“I’m afraid the adult team won’t
understand how to work with
Bobby.”
“I worry they won’t provide the same
level of flexibility and care.”
Example
In a clinic process improvement meeting, a ground rule had
been set to "arrive early to start on time." Dr. X consistently
arrives 15-30 minutes late, typically entering the room with
apologies, along with a statement that "patient care comes
first." Even though the group had developed guidelines for
team members, including not scheduling patients for 15
minutes before the meeting and identifying a time that
really worked for everyone, Dr. X enters expecting to have a
recap of what has been discussed. Many times, Dr. X
intervenes to change decisions the group made before he
arrived.

3/15/2015
19
Positions and Interests: group
Positions and Interests: Dr X

3/15/2015
20
Negotiating Differences:
ARTS of Communication
• Ask the other’s perspective – use active listening
• Respond with empathy, reflective listening
• Tell your perspective and your interests
• Summarize your understanding of the other’s perspective, their interests and focus on shared interests
• Seek solutions - generate options

3/15/2015
21
Listening
Filters that affect our listening (that we don’t notice)
•Culture
•Language
•Values
•Beliefs
•Expectations
•Intentions
What you
mean to say
What is understood
What you say
What is heard
Reflective Response
Potential Pitfalls in Communication
Adapted from Health Behavior Change by Stephen Rollnick
“The single biggest problem in communication is the illusion that it
has taken place.” George Bernard Shaw

3/15/2015
22
Relationship as a conflict transformation tool
PEARLS:
• Partnership
• Emotions
• Acknowledgement (or Apology)
• Respect
• Legitimization
• Support
Marvel et al, JAMA 1999; Langewitz et al, BMJ 2002
PEARLS statements
Partnership: “I’d like to work with you, not against you.”
Empathy: “You seem pretty frustrated.”
Acknowledgement/apology: “What I’m hearing is that you are finding it difficult to interact well with the physicians on the team.”
Respect: “I see how much thought and work you have put into this.”
Legitimation: “Most people I know would also feel troubled after an event like that.”
Support: “What can I do in the next team meeting to support you?”

3/15/2015
23
Convey empathy nonverbally and verbally
Use:
• Pause
• Touch
• Facial expression
• Tone of voice
• SpaceAmbady et al, Surgery 2002
Attending to Relationship:
Skills Practice
Skills
1. Make at least one empathic statement
2. Convey empathy nonverbally
3. Be aware of your own reactions

3/15/2015
24
Reflective Listening
• Listen, express interest, and understand the
meaning of what the speaker is saying – with a
minimum of preconceived agenda
• Reflect the speaker’s words:
- repeat what you heard, including nonverbal
messages
- short summaries
• Non-verbally remain attentive, open, non-
judgmental
Reflective Listening Demo

3/15/2015
25
Skills Practice 6 minute exercise, then 6 minute debrief
• Work in pairs
• You will be in two different roles for 3 min each
1. Storyteller: Describe a challenge in a working relationship – with a patient, colleague, supervisor, etc.
2. Interviewer: Do NOT ask questions, share your stories, or problem-solve. Use only reflection and empathic statements.
“Mm hmm … Sounds like you were angry … That’s really tough …”
Negotiating Differences:
ARTS of Communication
• Ask the other’s perspective – use active listening
• Respond with empathy, reflective listening
• Tell your perspective and your interests
• Summarize your understanding of the other’s perspective, their interests and focus on shared interests
• Seek solutions - generate options
3/15/2015
26
Identify Shared Interests
• Uncover and highlight shared interests
• Remember that you and colleagues
are allies and have many shared goals
• Incompatible interests do exist…
Practice a conflict scenario in pairs10”
• Identify a current conflict in which you are faced
with a person who is entrenched in a position
• Describe the situation briefly to your partner
• Your goal is to identify their interests and find
shared interests
• Group debrief

3/15/2015
27
1.Stay Balanced: successful negotiators are calm, patient,
observant.
2.Be attuned to your counterpart: if they are feeling defensive
and hostile, everyone will be dragged down.
1.Influence your counterparts’ emotions
1.Resilient: self-awareness is key
Goal - emotional self-awareness, self
management
What is power?• Power as ““““legitimized”””” authority
– Positional power
– Professional or “expert” power
– Cultural power
• Power as the ability to produce intended effects
– Experience and knowledge
– Ability to build healthy relationships
– Ability to resolve differences
– Ability to influence others

3/15/2015
28
Why is POWER so hard?
Reactivity
Power
• Those with formal authority
– Less listening
– More talking
– Harder time getting into
others shoes
• Those with less formal authority
– Withdrawal
– Criticism or attack

3/15/2015
29
Long term influencing strategiesBuild relationships
• Identify opinion leaders and those with formal authority
• Get to know their interests, challenges
• Build allies and stay engaged with opponents
• Help others with their challenges
• Use PEARLS, ARTS, INTERESTS vs. POSITIONS
Power
• Those with formal authority
– Less listening
– More talking
– Harder time getting into
others shoes
• Those with less formal authority
– Withdrawal
– Criticism or attack
• Those with formal authority
– Self-management, courage
– More listening, less talking
– ACBD
• Those with less formal authority
– Self-management, courage
– Use long term influencing
strategies
– Focus on ARTS

3/15/2015
30
ARTS--up the power gradient
• Ask the other’s perspective – use active listening– Begin by understanding their interests, barriers, and challenges
• Respond with empathy and reflective listening– Assure they know you want and care about their success.
• Tell your perspective and your interests– Explain how your ideas impact their interests.– Check their reactions to your ideas and their concerns.
• Summarize your understanding of the other’s perspective, their interests– and your understanding of their reaction to your position.
• Seek solutions--generate options– Make sure you meet again.
Prepare for conflict
• Be clear about your goals for:
- the relationship
- the substance of conflict
• Distinguish interests vs. positions
• Distinguish feelings from thoughts
• Check your assumptions

3/15/2015
31
Example
In a clinic process improvement meeting, a ground rule had
been set to "arrive early to start on time." Dr. X consistently
arrives 15-30 minutes late, typically entering the room with
apologies, along with a statement that "patient care comes
first." Even though the group had developed guidelines for
team members, including not scheduling patients for 15
minutes before the meeting and identifying a time that
really worked for everyone, Dr. X enters expecting to have a
recap of what has been discussed. Many times, Dr. X
intervenes to change decisions the group made before he
arrived.
3/15/2015
32

3/15/2015
33
Demo
• Team Leader Role
– Has done the preparation and takes the lead with
ARTS
– Goal to find mutual interests
• MD Role
– Not prepared
– Does not know what to expect in the conversation
Consultation groups
• Form triads
• Think of a conflict at work
• 3 rounds: in each round:
– One person shares a question
– Consultants ask clarifying questions
– Client then turns back on consultants
– Consultants discuss ideas, suggestions, 5 min
– Client returns, shares take-homes

3/15/2015
34
Summary
• Seek to understand and demonstrate your
understanding before seeking to be understood
• Make the goal of “understanding” a collaborative
effort
• Develop a strong working relationship
• Embrace differences
Summary
• Explore the data, reveal your reasoning
• Discuss how each of you has interpreted the data
and reached conclusions
• Explore the interests underlying positions to
expand the pie
• Seek to be “unconditionally constructive”

3/15/2015
35
ReferencesBooks:
1. Getting to Yes by Roger Fisher, William Ury and Bruce Patton 3rd edition 2011 Penguin Books
2. Difficult Conversations, How to Discuss What Matters Most by Douglas Stone, Bruce Patton and
Sheila Heen. 2010 Penguin Books
3. Thanks for the Feedback by Douglas Stone and Sheila Heen. 2013 Penguin Books
4. Nonviolent Communication by Marshall Rosenberg, 2008
5. Dialogue: The Art of Thinking Together by William Isaacs, 1999
Articles:
Aschenbrener, CA et al. Managing Low to Mid Intensity Conflict in the Health Care Setting The
Physician Executive, July/Aug 1999; pp 44-50.
Greer, LL et al. Conflict in medical teams: opportunity or danger? Medical Education 2012: 46: 935–
942
Janss, R. et al. What is happening under the surface? Power, conflict and the performance of medical
teams. Medical Education 2012: 46: 838–849
Rosenstein, AH. A Survey of the Impact of Disruptive Behaviors and Communication Defects on
Patient Safety, JCAHO, 8-08
ExercisePreparation for conflict; interests vs. positions
• Case scenario
You have recently been promoted from nurse manager of a primary
care clinic to be the Chief Nursing Officer for a large integrated health
system with 20 primary care clinics and more than 15 specialty clinics.
There is a huge backlog of patients from primary care waiting for
appointments in many specialty clinics. You have been appointed by
the CEO to chair a steering committee to guide an improvement effort.
The CEO has said there is NO additional money for solutions.
3/15/2015
36
Demo
• CNO Role
– Has done the preparation and takes the lead with
ARTS
– Goal to find mutual interests
• MD Role
– Not prepared
– Does not know what to expect in the conversation


















