
M health_Farhad
24
Reducing Maternal and Newborn Death (ReMiND) - use of m health technology Sharing experiences , April 9, 2015 Farhad Ali Technical Expert Health CRS, NEW DELHI [email protected]
-
Upload
farhad-ali -
Category
Documents
-
view
82 -
download
3
Transcript of M health_Farhad

Reducing Maternal and Newborn Death (ReMiND) - use of m health technologySharing experiences , April 9, 2015
Farhad AliTechnical Expert HealthCRS, NEW [email protected]

Project Duration: 4 Years (FY12 – FY15)
Partners: Vatsalya, Sarthi Development Foundation, Dimagi Inc. & Government of Uttar Pradesh
Area of Intervention: 8 blocks of Kaushambi & 1 block on Lucknow district
Beneficiaries: 13428 women & 12,308 children through 257 ASHAs in two blocks Total beneficiaries – around 1,42,000
Donors: CRS private fund, USAID small contribution DIV 2.0
Reducing Maternal & Newborn Deaths-ReMiND

3

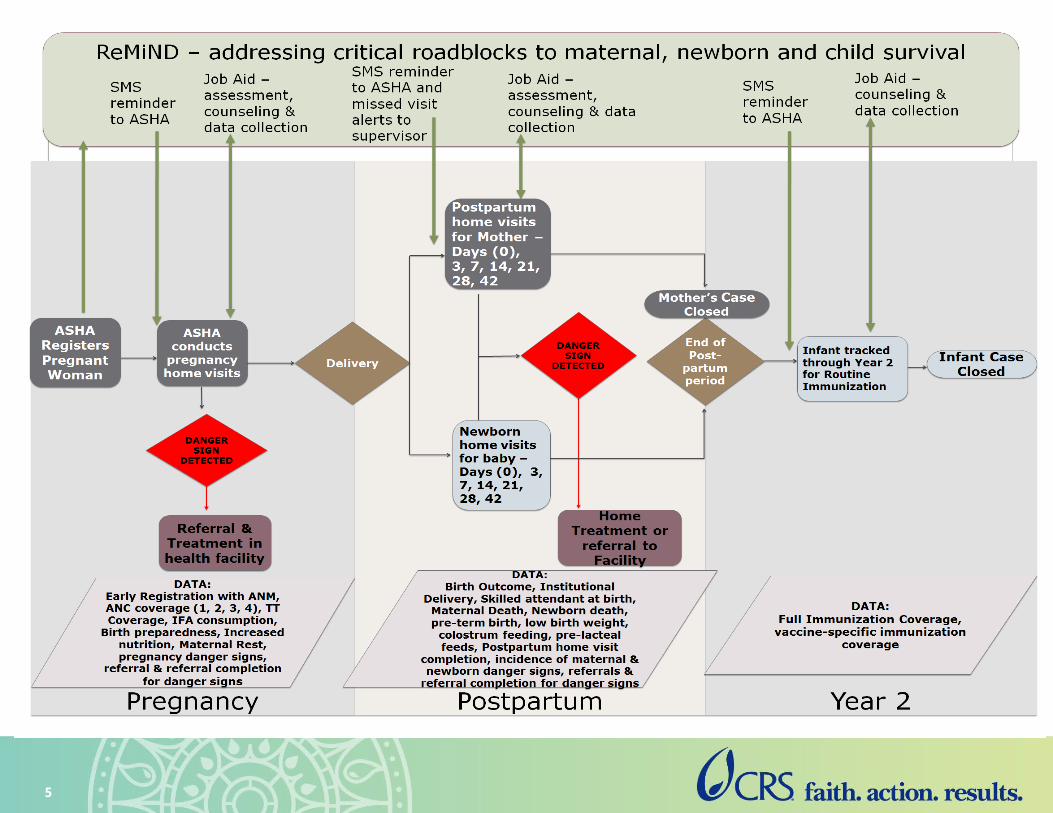
ReMiND – What is it?
CommCare as a Job Aid for ASHA:• Track and support woman through Pregnancy and
Postpartum periods
• Track and support baby from birth through first 2 years of life
• Localized and designed for ASHA use
Combines audio and still images for counseling and assessment content based on ASHA Modules 2, 6 and 7
CommCare as a Decision Support tool:• Helps the ASHA identify Danger Signs and make the
appropriate referral
CommCare as a supportive supervision tool• Helps ASHA supervisors to manage ASHA performance
and provide constructive feedback.
4
5
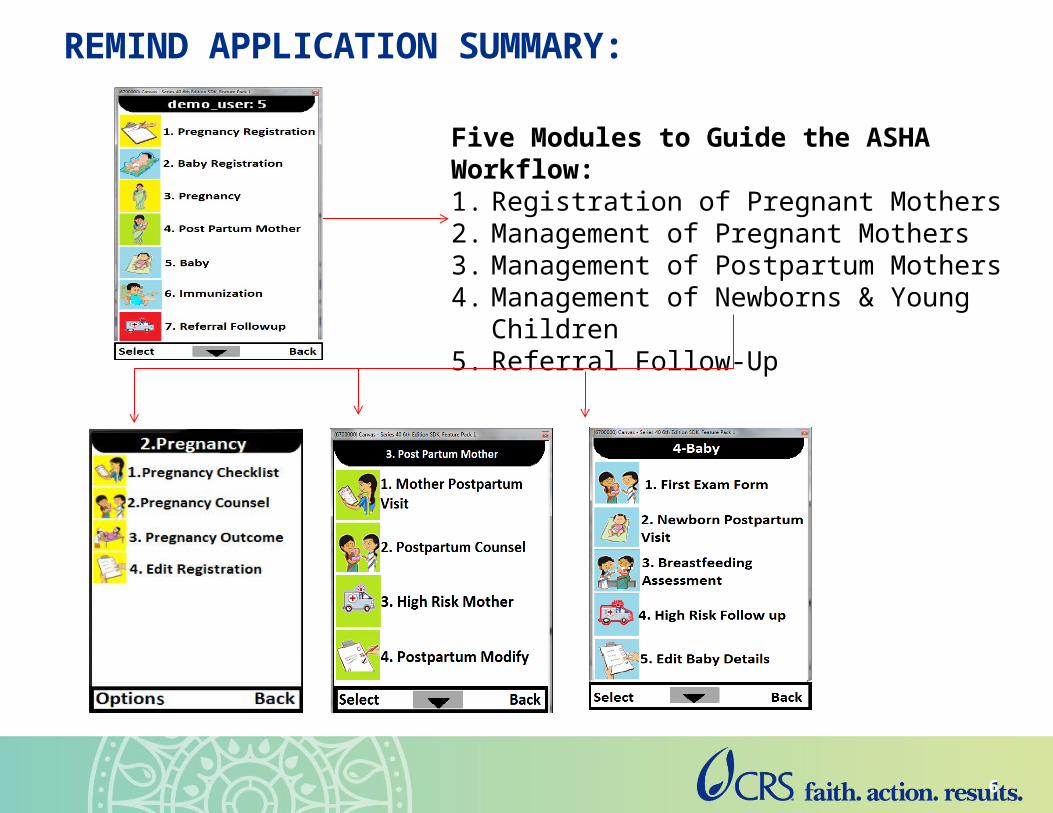
REMIND APPLICATION SUMMARY:
Five Modules to Guide the ASHA Workflow:1. Registration of Pregnant Mothers2. Management of Pregnant Mothers3. Management of Postpartum Mothers4. Management of Newborns & Young Children5. Referral Follow-Up
6

- Pregnancy Checklist- Completion of ANC check-ups and Tetanus
Immunizations, Assess Use of Health Services, Assess High Risks Signs in Pregnancy
- Pregnancy Counseling- Information about High Risks and Pregnancy
Danger Signs, Antenatal Care, Nutrition, Rest and IFA, Pregnancy Danger Signs, Birth Planning and Preparedness, Essential Newborn Care
- Pregnancy Outcome- Delivery information, Pregnancy outcome,
Newborn and mother’s health after delivery
- Modify Pregnant Woman Info- Modify identification info for woman, and update
EDD/LMP information
PREGNANT MOTHERS:
7

- Mother Postpartum Visit- Completion of Postpartum home visits,
Assessment of High Risks, Visit scheduling
- Postpartum Counseling- Information about High Risks and Postpartum
Danger Signs
- High Risk Follow up- Follow-up on high risks identified, Decision support
for assessing high risks
- Postpartum Review - Review information about status and health of
postpartum mother, high risks identified, and next scheduled home visit
- Close Postpartum- To be filled 42 days post delivery once postpartum
phase is complete
POSTPARTUM MOTHERS:
8
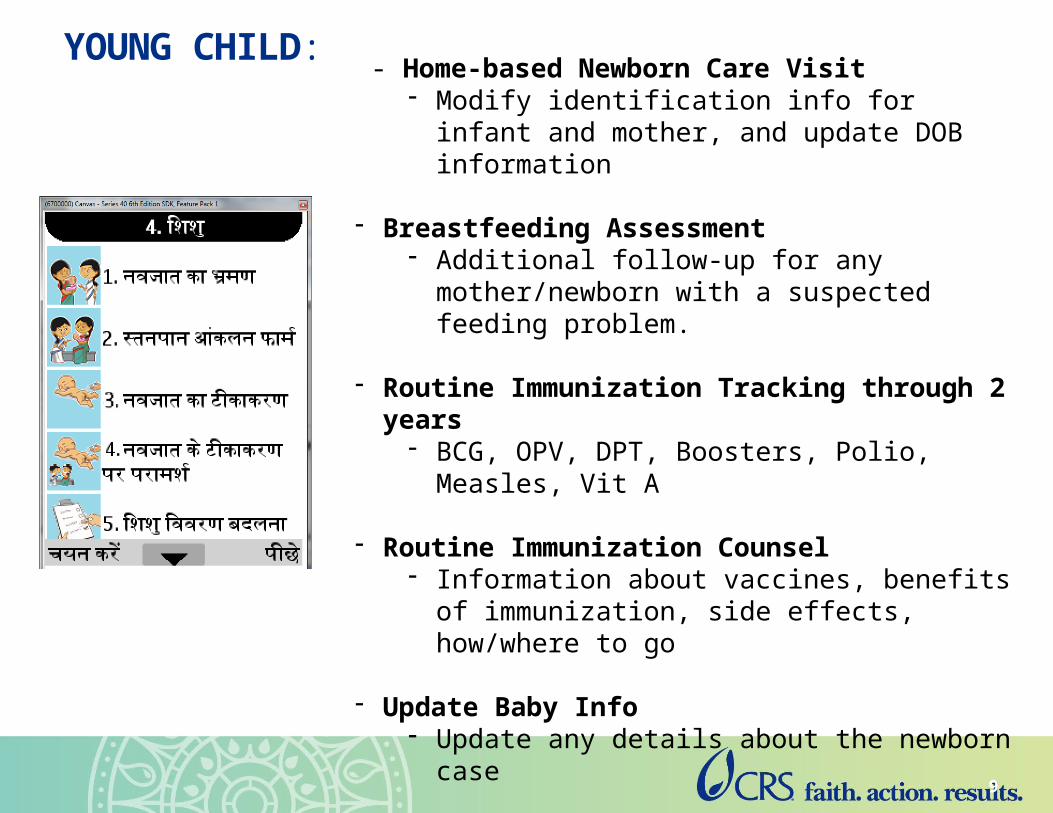
- Home-based Newborn Care Visit- Modify identification info for infant and mother, and
update DOB information
- Breastfeeding Assessment- Additional follow-up for any mother/newborn with a
suspected feeding problem.
- Routine Immunization Tracking through 2 years- BCG, OPV, DPT, Boosters, Polio, Measles, Vit A
- Routine Immunization Counsel- Information about vaccines, benefits of
immunization, side effects, how/where to go
- Update Baby Info- Update any details about the newborn case
- Close Baby- To be filled to close the baby case after 2 years of
care and full immunization
YOUNG CHILD:
9
Mohini
Did the govt want to track until 5 years? Because we can make this 5 years as well. Note that currently, there the newborn module isn't deployed, but its developed and we have much more content. We'll be ready to launch pilot testing in June - delayed about a month with Sri's injury.

Supportive Supervision & Monitoring
Analysis & use of
ASHAs’ real-time data
Outcome:Maternal, newborn & child health outcomes
CommCare HQ
Supportive Supervision Application
Quality:IPC & counseling skills,
Mobile skills
Analysis & use of real-
time supervision
data
Active Data Management
Reports
Output: Frequency & timeliness of ASHA home visits
SMS reminders & missed visit alerts
10
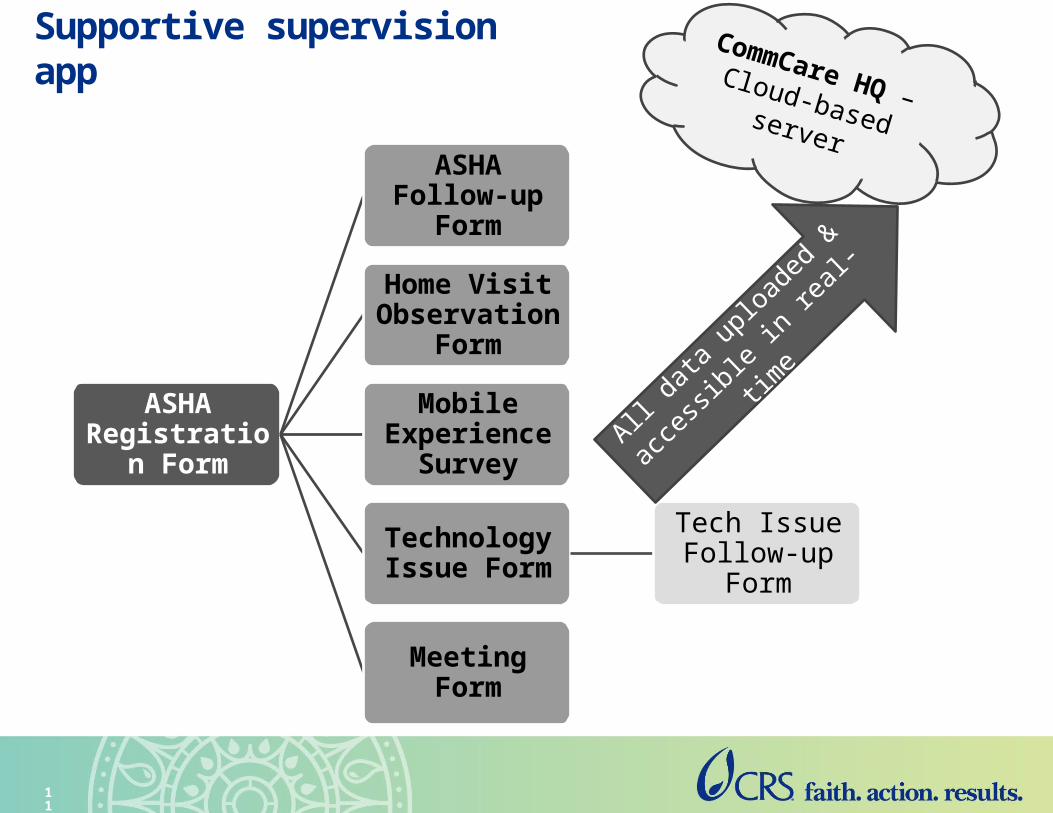
Supportive supervision app
ASHA Registration
Form
ASHA Follow-up Form
Home Visit Observation
Form
Mobile Experience
Survey
Technology Issue Form
Tech Issue Follow-up Form
Meeting Form
CommCare HQ – Cloud-based server
All data
uploaded &
accessi
ble in re
al-time
11

Program Impacts !
©CR
S/In
dia2
014/
DIM
AGI

Quality of counseling by ASHA has improved significantly
ASHA talked about her next home visit.
ASHA encouraged woman to use next recommended health service.
Families who asked any questions.
Clients who asked any questions.
ASHA encouraged client to speak or ask questions.
ASHA waited for client to respond before moving to next audio message.
ASHA expanded on any of the CommCare audio messages/questions.
ASHA greeted woman
79%
100%
35%
77%
96%
94%
94%
100%
41%
50%
11%
24%
58%
59%
59%
85%
Improvements in ASHA counseling tracked through facilitators’ observations
Sept-12 14-Sep

14
ASHA Activities: Home Visit Coverage

15
Shift from low to high coverage ASHAs

16
ASHA Activities: Counseling and Knowledge

17
Targeted Health Behaviors: Ante-natal Care
• Multi-media app help them more credibility with clients—validates key health messages
• Improved confidence levels in working in the community and improved acceptability by the beneficiaries they serve.
• Half of the functionally
illiterate ASHAs can now type
in Hindi on their mobile
phones.
©CR
S/In
dia2
014/
Satis
h
Positioning ASHAs in the community

• Birth preparedness doubled from baseline (43.2% to 80.7%)
• The average number of counseling visits made by an ASHA prior to birth nearly doubled, increasing from an average of 1.18 per woman to 1.95 per women
©CRS/India2014/Satish
Outcome level changes

• Tailored handholding support to ASHAs
• Working with ASHAs who have no functional literacy
• Frequent change in the leadership in government at district level
• Technology related issues
– GPRS problems
– Change in the settings in the hand set
• Engaging government in resolving tech issues
• Putting systems in place vis a vie leveraging technology
– Eg – ensuing ASHA visit & then making it ICT enabled
Challenges

• Make app more localized (such as voice of a local lady) and simple. • With low-literate users, the mobile interface must ensure easy
navigation and training strategies must be adapted to maximize learning.
• Immediate post training follow ups sustains interest and motivates to practice.
• Need based supervision helpful in maximizing ASHA outputs.• Strengthening local resources minimizes time in resolving
technology issues • Understand the context well before launching the app
– Such as understanding capacities of ASHAs
Lessons Learned
• Success of a mobile app for ASHAs is dependent on having sufficient supportive supervision for the ASHAs.
• Engagement of the government functionaries from the inception enables easy uptake of intervention and increase their ownership
• Allow sufficient time at every stage – app development, training, implementation and data analysis as well as its use
• Align with government programs and system
• Having tool is good. However, the purpose of using tool needs to be given more importance than the tool itself.
Lessons Learned

Keep it simple
Test, Test, Test & Then Scale
Invest in building local capacities
It takes a team
Share & learn…learn & share
Summary and Close

Thank You !
Thanks for your attention

















![I · MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMTFP ! O[A]|VFZL Z__& JØ" o _# AZSFT[ bJF• m m m m m m m m m m m m m m m m m m m m …](https://static.fdocuments.net/doc/165x107/5e7ba18c1045a43ff17a2374/i-mmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmtfp-oavfzl-z-j-o-.jpg)
