B cell neoplasms T/NK cell neoplasms Hodgkin lymphoma (disease)

Lymphatic Vessel Density and Vascular Endothelial GrowthFactor-C Expression Correlate with Malignant Behavior inHuman Pancreatic Endocrine Tumors
Laura Rubbia-Brandt,1 Benoit Terris,5
Emile Giostra,2 Bertrand Dousset,6
Philippe Morel,3 and Michael S. Pepper4
Services of 1Clinical Pathology, 2Gastroenterology and Hepatology,and 3Digestive Surgery, Geneva University Hospital, Geneva,Switzerland; 4Department of Morphology, University Medical Center,Geneva, Switzerland; and 5Services d’Anatomie Pathologique and6Surgery, Hopital Cochin, Paris, France
ABSTRACTMetastatic dissemination of tumor cells to regional
lymph nodes is a common early feature of many humancancers including pancreatic adenocarcinoma. In contrast,lymph node metastasis is more variably observed in pancre-atic endocrine tumors. The objective of this study was toassess the lymphatic system of human pancreatic endocrinetumors and correlate this to clinical behavior. Immunohis-tochemistry was performed using antibodies to two recentlyidentified markers of lymphatic endothelium, namely,LYVE-1 and podoplanin, and to the lymphangiogenic factorvascular endothelial growth factor (VEGF)-C. As has beenreported previously, we observed that in the normal pan-creas, islets of Langerhans are devoid of intra-islet lymphat-ics, but that lymphatics are present in connective tissue inassociation with ducts and blood vessels. We found that bothbenign and malignant pancreatic endocrine tumors containintratumoral lymphatic vessels. Lymphatic vessel densitywas related to the size of the tumor in benign tumors and tothe presence of liver metastasis but not to lymph nodemetastasis in malignant tumors. VEGF-C was expressed intumor cells: 4 of 19 (21%) benign tumors were positive,whereas 6 of 9 (67%) borderline tumors and 9 of 11 (82%)carcinomas were positive. These findings strongly suggestthat lymphangiogenesis occurs in pancreatic endocrine tu-mors and that lymphatic invasion and the development ofmetastases are associated with VEGF-C expression.
INTRODUCTIONTumor cell dissemination is mediated by several mech-
anisms, including local invasion, lymphatic or hematogenousspread, and direct seeding of body cavities or surfaces. It isan important indicator of prognosis in human cancers. Withregard to lymphatic spread, it is still unclear whether lymphnode metastasis is dependent on lymphangiogenesis or inva-sion of preexisting lymphatic capillaries (1). Recent studieshave demonstrated a causal role for vascular endothelialgrowth factor (VEGF)-C–induced lymphangiogenesis in me-diating tumor dissemination and the formation of lymph nodemetastases in an experimental pancreatic insulinoma model(2). However, little is known about the lymphatic system inhuman pancreatic endocrine neoplasms (PENs) and the rela-tionship of the lymphatic system to nodal metastasis andprognosis.
A solid, trabecular or glandular arrangement of well-differentiated cells characterizes the histologic pattern ofmost well-differentiated PENs (3). In most cases, these fea-tures are sufficiently distinct to permit recognition of theendocrine nature of the tumor. In other cases, immunhisto-chemical stains for general neuroendocrine markers (e.g.,chromogranin, synaptophysin or neuron-specific enolase) areneeded for tumor identification. In addition, immunohisto-chemical stains for hormones are necessary to characterizetumor cell types and their specific hormonal products, whichmay cause a syndrome of endocrine hyperfunction. Thesetumors are challenging because of the difficulty in predictingbiological behavior when using classical histopathologicalmalignancy criteria (size, cellular atypia, necrosis, mitoticactivity, and angioinvasion). The basis for distinguishinglow-grade endocrine tumors from other well-differentiatedendocrine carcinomas is usually the presence of metastases.The type of endocrine hypersecretion also correlates withbiological behavior of the tumor. Current consensus classifi-cation is the World Health Organization (WHO) internationalhistologic classification (3).
Well-differentiated PENs are also characterized by anabundant vascularity. Little is known, however, about the lym-phatic system in these tumors. One of the main obstacles tostudying tumor-associated lymphatics and lymphangiogenesishas been the lack of specific markers for lymphatic endothelium.We applied antibodies to two recently described lymphaticmarkers to PENs, namely, LYVE-1, a hyaluronan receptor (4),and podoplanin, a podocyte membrane gylocoprotein (5), toinvestigate lymphatic vessels and lymphangiogenesis and theirrelationship to clinicopathological characteristics of these tu-mors. Expression of VEGF-C, a potent lymphangiogenic factor(6, 7), was also evaluated.
Received 2/28/04; revised 4/15/04; accepted 4/29/04.Grant support: Grant 3100-064037.00 from the Swiss National Sci-ence Foundation (M. Pepper).The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely toindicate this fact.Requests for reprints: Laura Rubbia-Brandt, Service de Pathologie Clin-ique, 1 rue Michel Servet, 1211 Geneva 4, Switzerland. Phone: 41-22-3724903; Fax: 41-22-3724920; E-mail: [email protected].
©2004 American Association for Cancer Research.
6919Vol. 10, 6919–6928, October 15, 2004 Clinical Cancer Research
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

MATERIALS AND METHODSPatient Material. Archival paraffin-embedded tissue
from 39 cases of human PENs was retrieved from the files of theService of Clinical Pathology, University Hospital, Geneva,Switzerland (n � 22) and from the Service d’AnatomiePathologique, Hopital Cochin, Paris, France (n � 17). Our studywas performed in accordance with ethical standards of theHelsinki Declaration of the World Medical Association. Thegroup included 18 male and 21 female patients. The mean agewas 51 years (range, 15–81 years). Specimens of surgical duo-denopancreatic resections were selected so that both normalpancreas and tumor tissue were present on the same slide. Thediagnosis was based on hematoxylin and eosin morphologiccharacteristics as well as immunohistochemical positivity forendocrine markers such as chromogranin and synaptophysin.Compatible clinical syndromes associated with elevated serumlevels of the corresponding hormones were used for the diag-nosis of functional tumors. Nonfunctional tumors were notassociated with any clinical syndrome, irrespective of the hor-mone detected in the tumor.
PENs were divided into three groups according to theWHO international histologic classification (3), which was usedto establish clinicopathological correlations (Table 1). The firstgroup consisted of 19 benign PENs characterized by a well-differentiated tumor limited to the pancreas with a size of �2cm, a mitotic count always less than 2 per high-power field(HPF), and no evidence of angioinvasion or metastases. Thesecond group was composed of nine PENs with criteria ofuncertain behavior. They were all confined to the pancreas.They measured �2 cm in size and/or had �2 mitotic figures perHPF and/or presented with angioinvasion. They had no metas-tases. The third group was composed of 11 well-differentiated,low-grade carcinomas that extended into extrapancreatic tissueand presented with lymph node metastases as assessed by theexamination of resected surgical specimens and/or liver metas-tases diagnosed by imaging and confirmed by histologic preop-erative biopsy or from surgical specimens, independent of othercriteria.
Immunostaining. Immunohistochemical stainings wereperformed on 10% neutral buffered formalin-fixed, paraffin-embedded specimens. Briefly, serial 3- to 5-�m sections werecut, mounted on silane-coated glass slides and air dried over-night. Sections were deparaffinized, rehydrated, and pretreatedwith H2O2/methanol to block endogenous peroxidase activity.The following primary antibodies were used: mouse monoclonal
antihuman chromogranin A (1:400; Immunotech, Switzerland),mouse monoclonal antihuman insulin (1:500; Biogenex, Basel,Switzerland), rabbit polyclonal antihuman gastrin (1:1,000; Da-koCytomation, Basel, Switzerland), mouse monoclonal antihu-man serotonin (1:20; DakoCytomation), rabbit polyclonal anti-human glucagon (1:1,000; DakoCytomation), rabbit polyclonalantihuman VIP (1:10; DakoCytomation), rabbit polyclonal an-tihuman LYVE-1 antibody (ref. 4; 1:100), rabbit polyclonalantihuman podoplanin (ref. 5; 1:1,500), mouse monoclonal an-tihuman CD31 (1:100; Dako), mouse monoclonal antihumanCD34 antibody (1:10; Serotec, Dottikon, Switzerland), andpolyclonal goat antihuman VEGF-C (1:80; R&D Systems, BadZurzach, Germany). For anti-chromogranin, anti-VIP, anti-CD31, anti-CD34, anti-LYVE-1 and anti-podoplanin antibod-ies, microwave treatment was used. Sections were incubated for1 hour at room temperature with the diluted primary antibodies,which were then revealed by the avidin-biotin-peroxidase com-plex method (Vectastain; Vector Laboratories, Burlingame,CA). Peroxidase activity was revealed with 30% 3,3�-diamino-benzidine as the chromogen diluted in PBS containing 0.015%H2O2. Sections were weakly counterstained with Mayer’s he-matoxylin and mounted in Eukitt. Negative controls includedomission of the fist antibodies. For LYVE-1 and VEGF-Cimmunostaining, antigen-antibody complexes were revealed bymeans of the rabbit/horseradish peroxidase Envision system(DakoCytomation).
LYVE-1 and podoplanin were considered to be positivewhen staining was intense and diffuse along endothelium.LYVE-1– and podoplanin-positive vessels with erythrocytes inthe lumen were evaluated separately. Lymphatic vessel density(LVD) was determined by counting the number of LYVE-1– orpodoplanin-positive vessels per HPF (�400) in the tumor. Thisincluded both intratumoral and stromal vessels; however, thevast majority of vessels were stromal. Vessels were counted in10 randomly selected fields per section by two independentobservers. VEGF-C was considered positive when staining wascytoplasmic. Staining was graded semiquantitatively as follows:0, absent; 1, focal positive isolated tumor cells; 2, 20% to 50%of tumor cells positive; and 3, �50% of tumor cells positive (8).
Statistical Analysis. Differences in LVD between insu-linomas and other tumors and their relationship to lymph nodemetastasis, liver metastasis, or angioinvasion were evaluatedusing the Mann-Whitney test. The Spearman test was used forestimating the relationship between tumor size and LVD. Thedifferences in LVD among the three groups (benign, borderline,
Table 1 Clinicopathological characteristics of the 39 pancreatic endocrine tumors
Pancreatic endocrine tumor
Benign Uncertain behavior Malignant
Age median (range) (y) 46 (15–81) 61 (41–77) 50 (38–65)Sex m/f 8/11 6/3 4/7Median size (range) (cm) 1.25 (0.4–2) 4.9 (3–7) 4.8 (2–16)Mitotic counts � 2 per HPF 0 4 8Angioinvasion 0 3 8Lymph node metastasis 0 0 9Liver metastasis 0 0 6Total 19 9 11
6920 Lymphatic Status of PENS
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

and malignant) were evaluated using the Kruskal-Wallis test.P � 0.05 was considered to be significant. Tests were per-formed with the SPSS statistical package (SPSS Base 10.0;SPSS Inc., Chicago, IL).
RESULTSLYVE-1 and Podoplanin Antibody Specificity. Immu-
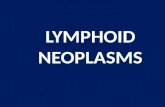
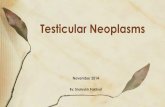
nostaining of normal pancreatic and liver tissues was first usedto assess the specificity of LYVE-1 and podoplanin for lym-phatic vessels. In the pancreas, LYVE-1–positive staining wasseen in vessels devoid of red blood cells with an irregularmorphology. These vessels were located mainly around negativearteries and veins in the interlobular connective tissue and weresparse in the intralobular connective tissue (Fig. 1A). Thesevessels were also podoplanin positive (Fig. 1C). LYVE-1– andpodoplanin-positive vessels were CD31 positive (Fig. 1B) butCD34 negative. No LYVE-1– or podoplanin-positive vesselswere observed within islets of Langerhans (Fig. 2A and B),whereas blood vessels were detected with CD34 (Fig. 2C) andCD31 (Fig. 2D).
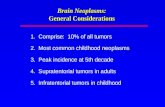
In the liver, LYVE-1–positive vessels were observed inlarge portal tracts (Fig. 3B). Small portal tracts were usuallydevoid of positive vessels (Fig. 3C). Sinusoidal endothelial cells
were also intensely positive, whereas portal arteries and veinsand centrolobular veins were negative (Fig. 3B and C). Podo-planin-positive vessels were seen in all portal tracts, independ-ent of their size (Fig. 3A and D). They were generally small indiameter, with several positive vessels in each portal tract, andwere often localized near to the interlobular bile duct (Fig. 3D).Sinusoids, portal arteries and veins, and centrolobular veinswere negative (Fig. 3A and D).
Lymphatic Vessels in Pancreatic Endocrine Tumors.The 39 PENs included in this study were classified accordingto their pathological characteristics (Table 1). The first groupconsisted of 19 benign well-differentiated PENs. Sixteenwere insulinomas, one was a glucagonoma, and two werenonfunctioning tumors. The second group demonstrated cri-teria of uncertain behavior and consisted of nine cases. Theycorresponded to one insulinoma, one gastrinoma, one seroti-noma, and six nonfunctioning tumors. The third group con-sisted of 11 well-differentiated endocrine carcinomas.Among this group, one secreted glucagon, two secreted gas-trin, and eight were nonfunctioning tumors. No significantdifferences were observed in sex and age between the differ-ent groups (P � 0.05).
To characterize lymphatic vessels in pancreatic endo-
Fig. 1 Immunostaining of normal pancreas. LYVE-1–positive stain-ing (A) and podoplanin-positive staining (C) were seen in vesselsdevoid of red blood cells. These vessels were located mainly aroundnegative arteries and veins in the interlobular connective tissue.LYVE-1– and podoplanin-positive vessels were also CD31 positive(B). Magnification of A�C, �100.
6921Clinical Cancer Research
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

crine tumors, we performed immunostaining with antibodiesto LYVE-1 and podoplanin. The results are summarized inTable 2. LYVE-1– and podoplanin-positive vessels werealways seen in the surrounding normal pancreas. In the PENs,positive lymphatic vessels were variably observed within theintratumoral supporting connective tissue (stroma) next tonegative blood vessels (Fig. 4A) or dispersed between thetumor cells in close contact with them (Fig. 4B and C). Thesevessels were often similar in shape and size to normal pan-creatic vessels. Occasionally, they were distinct, with asmaller, thin or ill-defined lumen (Fig. 4C). Lymphatic ves-sels were randomly distributed within the tumor without hotspots. Occasionally, positive vessels contained tumor cells,which is indicative of lymphatic invasion (Fig. 4D). Vesselspositive for LYVE-1 or podoplanin were negative for CD34on serial sections.
With respect to LYVE-1 immunoreactivity (Table 2), only 4insulinomas of 19 benign tumors had positively staining vesselsthat were localized exclusively in the tumor stroma; in these fourcases, average LVD was 0.14 vessel per HPF (range, 0.1–0.2vessel per HPF). In borderline tumors, four of nine had positive
vessels in the tumor stroma; in these cases, the average LVD was0.15 vessel per HPF (range, 0.1–0.3 vessel per HPF); no positiveintratumoral vessels were seen in any of the cases. In well-differ-entiated carcinomas, 5 of 11 cases had positive tumor stromalvessels. Most strikingly, three of these cases contained positiveintratumoral vessels. In these positive cases, the average LVD was0.6 vessel per HPF [range, 0.1–1.2 vessel(s) per HPF].
With respect to podoplanin immunoreactivity (Table 2), allbenign PENs had positive vessels in the tumor stroma. In addition,8 of 19 benign tumors had positive intratumoral vessels. Theaverage LVD here was 1 vessel per HPF [range, 0.3–2.4 vessel(s)per HPF]. In the borderline tumors, all PENs had positive vesselsin the tumor stroma, and one of nine had positive intratumoralvessels. The average LVD here was 0.7 vessel per HPF [range,0.2–1.4 vessel(s) per HPF]. In well-differentiated carcinomas, allhad positive vessels in the tumor stroma, and 6 of 11 had positiveintratumoral vessels. The average LVD here was 2.5 vessels perHPF [range, 0.7–3.1 vessel(s) per HPF].
Correlations between LVD and WHO Classification.The WHO classification separates PENs into different catego-ries according to their clinical behavior. LVD evaluated by
Fig. 2 Immunostaining of normal pancreatic islets of Langerhans. No LYVE-1–positive (B) or podoplanin-positive (A) vessels were observed withinislets, whereas blood vessels were detected with CD34 (C) and CD31 (D). Magnification of A�D, �400.
6922 Lymphatic Status of PENS
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

podoplanin immunostaining was significantly higher in well-differentiated endocrine carcinomas than in borderline or benigntumors (P � 0.009, Kruskal-Wallis test). No correlation wasfound when LVD was evaluated by LYVE-1 immunostaining(P � 0.204, Kruskal-Wallis test). The different histoprognosticfeatures defining the WHO classification for PENs were thencompared to LVD (Table 3). LVD evaluated by podoplaninimmunostaining (Table 3) was significantly correlated to the
size of the tumor in benign PENs (r � 0.589; P � 0.008). LVDwas not correlated to size in borderline tumors (r � 0.452; P �0.05) or carcinomas (r � �0.09; P � 0.05). No correlation waspresent between LVD and size in the benign group (r � 0.191;P � 0.05), borderline group (r � �0.421; P � 0.05), orcarcinomas (r � 0.05; P � 0.05) when LYVE-1 immuno-staining was considered (Table 3). There was no relationshipbetween the image of angioinvasion and LVD with podoplanin
Fig. 3 Immunostaining of normal liver. LYVE-1–positive vessels (B) were observed in large portal tracts (PT). Small portal tracts were usuallydevoid of positive vessels (C). Sinusoidal endothelial cells in the lobules (L) were also intensely positive (B and C). Podoplanin-positive vessels wereseen in all portal tracts, independent of their size (A and D). Sinusoids in the lobules were negative (A and D). In the tumor metastasis (T) seen inthis image, positive vessels were identified with podoplanin (B) but not with LYVE-1 (B). Magnification: A and B, �100; C and D, �400.
6923Clinical Cancer Research
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

(P � 0.488) or LYVE-1 (P � 0.346) immunostaining. Therewas no relationship between the presence of lymph node me-tastasis and LVD with podoplanin (P � 0.07) or LYVE-1 (P �0.635). There was a modest correlation between the presence ofliver metastasis and LVD with podoplanin (P � 0.02) andLYVE-1 (P � 0.019).
Inflammation/Stroma. LYVE-1– and podoplanin-posi-tive vessels were occasionally seen to contain red blood cells intheir lumen. These positive vessels were essentially observed inareas of inflammation in peritumoral pancreatic tissue and cor-responded to venules (data not shown)
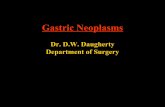
VEGF-C Expression in PENs. Nineteen of 39 tumorsdemonstrated VEGF-C–positive immunolabeling in the cyto-plasm of tumor cells (Fig. 5). With respect to different tumorbehavior categories, 4 of 19 benign tumors had positive tumorcells (Table 4). Only 1 of the 16 insulinomas was positive,whereas the glucagonoma and 2 nonfunctioning tumors ex-pressed VEGF-C. Expression was present in 20% to 50% ofcells in one case and was diffuse in the three other cases (Fig. 5).In borderline tumors, six of nine tumors had positive VEGF-Cexpression in tumor cells. VEGF-C expression was limited toscattered cells in two cases (Fig. 5), present in 20% to 50% of
Fig. 4 Immunostaining of PENs. Podoplanin-positive lymphatic vessels were present within the intratumoral supporting connective tissue (stroma)next to negative blood vessels (A) or dispersed between the tumor cells in close contact with them (B and C). D. Occasionally, podoplanin-positivevessels contained tumor cells, which is indicative of lymphatic invasion Magnification: A and B, �100; C and D, �600.
Table 2 LYVE-1 and podoplanin expression in pancreatic endocrine tumors
No. ofcases
LYVE-1–positive staining Podoplanin-positive staining
Vessels innormal pancreas
Intratumoralstromal vessels
Intratumoralvessels
Vessels innormal pancreas
Intratumoralstromal vessels
Intratumoralvessels
Benign tumorInsulinoma 16 16 4 0 16 16 6Noninsulinoma 3 3 0 0 3 3 2
Borderline tumor 9 9 4 0 9 9 1Well-differentiated endocrine carcinoma 11 11 5 3 11 11 6Total 39 39 13 3 39 39 15
6924 Lymphatic Status of PENS
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

cells in three cases, and diffuse in one case. In well-differenti-ated carcinomas, 9 of 11 cases had positive tumor cells.VEGF-C expression was limited to scattered cells in one case,present in 20% to 50% of the cells in five cases, and diffuse inthree cases.
VEGF-C was more frequently expressed in carcinomaswhen compared with borderline or benign tumors (P � 0.003;Kruskal-Wallis). There was no correlation between the intensityof VEGF-C expression and clinical behavior (P � 0.4; Kruskal-Wallis test). There was no correlation between VEGF-C expres-sion and LVD as evaluated by podoplanin (P � 0.355) andLYVE-1 (P � 0.1) immunostaining.
DISCUSSION
Tumor cell spread via lymphatic capillaries is an earlyfeature of many carcinomas, and the presence of metastases inregional lymph nodes is critical for the staging of these tumorsand for determining prognosis and subsequent therapeutic mo-dalities. Unlike pancreatic adenocarcinomas, PENs variably me-tastasize to regional lymph nodes and may occasionally metas-tasize at first to the liver. The staging of these tumors takes thisinto account and does not rely only on lymph node status(metastatic versus nonmetastatic). The reason for this character-istic behavior has not been established. Until recently, tumor
Fig. 5 In PENs, VEGF-C–positive immunolabeling was detected in the cytoplasm of tumor cells. Expression was focal (A) or diffuse (B).Magnification, �400.
Table 3 Correlation between LVD (as evaluated by LYVE-1 and podoplanin immunostaining) and histological data
LYVE-1–positive staining Podoplanin-positive staining
Benign PENs Uncertain behavior Malignant PENs Benign PENs Uncertain behavior Malignant PENs
Median size (cm) P � 0.05 P � 0.05 P � 0.05 P � 0.008 P � 0.05 P � 0.05Mitotic counts � 2 per HPF NA P � 0.05 P � 0.05 NA P � 0.05 P � 0.05Angioinvasion NA P � 0.05 P � 0.05 NA P � 0.05 P � 0.05Lymph node metastasis NA NA P � 0.05 NA NA P � 0.05Liver metastasis NA NA P � 0.019 NA NA P � 0.02Total 19 9 11 19 9 11
Abbreviation: NA, not available.
6925Clinical Cancer Research
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

cell dissemination to regional lymph nodes was generally be-lieved to be a passive process involving tumor spread viapreexisting afferent lymphatic channels that follows naturalroutes of lymphatic drainage. Recently, evidence for the de novoformation of lymphatic capillaries (lymphangiogenesis) hasraised the possibility that cells within primary tumors can con-tribute actively to lymphatic dissemination through the induc-tion of a lymphangiogenic process. A recent transgenic mousemodel combining pancreatic endocrine tumorigenesis and lym-phangiogenesis demonstrated that development of lymph nodemetastasis was directly related to VEGF-C expression and thedevelopment of lymphatic vessels (2). These observations un-derline the essential role of lymphangiogenesis in the progres-sion from benign to malignant behavior in experimental pancre-atic endocrine tumors. In light of these clinical and experimentalfeatures, we thought it important to assess the lymphatic systemin human PENs, in which a wide spectrum of clinical behavioris characteristically observed.
Studies on lymphangiogenesis rely on the use of specificmarkers of lymphatic endothelial cells. A debate exists as towhich is the best marker of lymphatic vessels (9). LYVE-1, ahyaluronan receptor of the link protein superfamily is, in mostinstances, a specific marker for lymphatics (4). However, sev-eral elements may complicate the use of LYVE-1 in certainsituations. We, like others, have observed expression of thismarker in the endothelium of liver sinusoids. Podoplanin, an-other lymphatic endothelial marker, appears to be restricted tolymphatics; liver sinusoids were negative (5). Moreover, in ourstudy, LYVE-1 appears to stain only a subset of lymphaticswhen compared with podoplanin. In the normal liver, LYVE-1–positive lymphatics were identified only in large portalspaces, whereas with podoplanin, portal spaces of all sizes hadpositive lymphatic vessels. In the normal pancreas, LYVE-1 andpodoplanin revealed a similar pattern in serial sections. Lym-phatics were observed in connective tissue in association withblood vessels and ducts, whereas intra-islet lymphatics werenever observed. This is in accord with previously publishedstudies in a variety of species. In striking contrast, a significantproportion of PENs contained lymphatics in the intratumoralstroma or in direct contact with tumor cells. Surprisingly, thesefeatures, which have not been reported previously, were moreapparent when podoplanin was used as the marker of lymphaticendothelium than with LYVE-1. Moreover, the LVD in PENswas higher with podoplanin than with LYVE-1. The reasons forthese differences are not known.
Because lymphatics are absent from normal islets, thepresence of lymphatic vessels within PENs is strongly sugges-tive of the presence of lymphangiogenesis. However, conclusionby cooption of existing lymph vessels by invading tumor cannotbe excluded. When quantitated with the anti-podoplanin anti-body, all PENs contained lymphatics in the intratumoral stroma,and a proportion of benign, borderline, and malignant PENs hadlymphatics dispersed between tumor endocrine cells. The pres-ence of these lymphatics highlights the fact that lymphangio-genesis in human PENs is a phenomenon that already occurs inbenign tumors and is insufficient to promote the development ofendocrine malignancy. Furthermore, LVD was related to theclinical behavior of the tumors. In fact, our study illustrates agreat variability in LVD among PENs. LVD quantitated bypodoplanin (but not LYVE-1) immunostaining was significantlyhigher in well-differentiated endocrine carcinomas than in be-nign or borderline PENs. LVD as assessed by podoplanin andLYVE-1 immunostaining correlated modestly with the presenceof liver metastasis. Remarkably, however, the density of lym-phatic vessels was unrelated to the image of angioinvasion orlymph node metastasis. These findings strongly suggest thatfactors other than mere access to an increasing number oflymphatic vessels are required for some tumors to metastasize toregional lymph nodes.
Our results on PENs are in accordance with reports fromothers on carcinoma of head and neck (10–12), thyroid (13), andmalignant melanomas (14), in which proliferating intratumorallymphatics and LVD have been identified as a markers of poorprognosis. Our study is in contrast to results on breast cancer, inwhich metastatic dissemination appears to occur in the absenceof lymphangiogenesis and the LVD was inversely correlated totumor aggressiveness (15). Our present observations, combinedwith our previous report on murine insulinomas, point to a majorrole for peritumoral/stromal vessels in tumor cell dissemination.The notion that intratumoral lymphatics, which were relativelyrare in human tumors and absent from murine tumors, arenonfunctional was not addressed in this study.
Few lymphangiogenic factors have been identified thus far.The best characterized are members of the VEGF family. Inparticular, VEGF-C has been shown to promote lymphangio-genesis both in vitro and in vivo through binding to the VEGF-Ctyrosine kinase receptor, VEGFR-3 (16), which, in normal adulttissues, is expressed on lymphatic endothelium (6). The possi-bility that VEGF-C might promote tumor lymphangiogenesishas received much attention. Several studies on animal modelshave directly demonstrated the existence of tumor lymphangio-genesis (17). However, there is as yet little evidence for directlymphangiogenesis in human tumors. Nonetheless, a number ofclinical studies have reported VEGF-C expression in humantumors and illustrated a significant association betweenVEGF-C levels of primary tumors and lymph node metastasis(11, 18–28). This suggests that although VEGF-C may inducetumor lymphangiogenesis, it is also likely to have other func-tions. These include angiogenesis and the autocrine stimulationof tumor cell growth.
In addition, and of specific interest to our studies, is thehypothesis that VEGF-C could activate preexisting lymphatics,which in turn become directly involved in tumor cell chemo-taxis, intralymphatic infiltration, and distant dissemination. This
Table 4 VEGF-C expression in pancreatic endocrine tumors
No. ofcases
Tumor cell VEGF-Cstaining
Positive Negative
Benign tumorInsulinoma 16 1 15Noninsulinoma 3 3 0
Borderline tumor 9 6 3Well-differentiated endocrine
carcinoma11 9 2
Total 39 19 20
6926 Lymphatic Status of PENS
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

would imply the existence of a reciprocal dialogue betweentumor and lymphatic endothelial cells, which leads to the for-mation of lymph node metastases. Normal endocrine cells con-stitutively express VEGF (6). In PENs, VEGF expression ismaintained, but at variable levels (6, 29). To evaluate the role ofVEGF-C in the metastatic process, immunohistochemistry wasperformed. In our series, VEGF-C was variably expressed inPENs, and VEGF-C expression was correlated to malignantclinical behavior. A similar variable expression of VEGF-C inPENs has recently been reported by another group (30). Takentogether with our observation that LVD is unrelated to lymphnode metastasis, these data point to the requirement for a secondelement for the development of lymphogenous metastases,namely, activities of VEGF-C that are unrelated to lymphangio-genesis. This mechanism is illustrated in the WHO classifica-tion, in which the presence of angioinvasion determines uncer-tain behavior but does not imply a malignant metastatic state.
Our data on LVD contrast with the results on blood vesselintratumoral density on PENs evaluated by CD34 immuno-staining, in which microvascular density was inversely corre-lated with behavior (29). Moreover, these authors report a lowerVEGF expression in endocrine carcinomas compared with ahigher expression in benign well-differentiated endocrine tu-mors; this is also in contrast with our observation of an increasein VEGF-C expression with malignant evolution. Taken to-gether, these results suggest the existence of a switch from ablood vessel angiogenic to a lymphangiogenic state during theevolution of PENs toward malignancy, possibly through modi-fication of levels of expression of members of the VEGF family.This possible angiogenic switch has been illustrated in theadenoma–carcinoma sequence during colorectal cancer progres-sion (31). These results also suggest the existence of lymphaticdrainage from the pancreas to the liver that would play a role inthe development of liver metastasis.
The intratumoral localization of lymphatics in our humanPEN series is in contrast to the double transgenic RipTag2 �Rip VEGF-C mouse model combining pancreatic endocrinetumorigenesis and lymphangiogenesis (2), in which VEGF-Cinduced lymphatics surrounding the tumor nodule but did notextend into the tumor itself. However, with respect to the othervariables, our results in human PENs are similar to this animalmodel: peritumoral lymphatics and the image of intralymphatictumoral angioinvasion were occasionally seen in Rip1Tag2mice, but lymph node metastases were never seen in theseanimals. The VEGF-C–induced increase in peritumoral lym-phatic density in double transgenic Rip1Tag2 � RipVEGF-Cmice resulted in dissemination of tumor cells to regional lymphnodes in approximately 40% of animals. It is noteworthy thatthis animal lymphangiogenesis model based on VEGF-C over-expression highlights, in a manner similar to our results inhumans, the important role of VEGF-C in the development of amalignant phenotype via a possible two-step mechanism.
In conclusion, tumor cell metastasis to lymph nodes is akey event in disease outcome and is frequently used as aprognostic factor. Our findings strongly suggest that lym-phangiogenesis occurs in human PENs and that LVD is corre-lated to clinical behavior, but not to lymph node status. Factorsother than mere access to an increasing number of lymphaticvessels may thus be required for some tumors to metastasize to
regional lymph nodes. LVD is correlated to liver metastasis,suggesting the existence of a lymphatic drainage from the pan-creas to the liver. Moreover, we provide evidence for a rolefor VEGF-C in the development of endocrine malignancy.Our results also confirm the validity of double transgenicRip1Tag2 � RipVEGF-C mice as a model of human PENs, inwhich the mechanisms of lymphangiogenesis and lymphatictumor metastasis can be dissected and in which potential inhib-itors of these processes can be tested.
ACKNOWLEDGMENTSWe thank Dr. D. G. Jackson (MRC Human Immunology Unit,
Institute of Molecular Medicine, John Radcliffe Hospital, Oxford,United Kingdom) for kindly providing the rabbit polyclonal antihumanLYVE-1 antibody and Prof. D. Kerjaschki (Department of ClinicalPathology, University of Vienna, Vienna, Austria) for kindly providingthe rabbit polyclonal antihuman podoplanin antibody. We thank PatriciaGendre and Carole Verdun for performing the immunohistochemicalanalysis.
REFERENCES1. Pepper MS. Lymphangiogenesis and tumor metastasis: myth or re-ality? Clin Cancer Res 2001;7:462–8.2. Mandriota SJ, Jussila L, Jeltsch M, et al. Vascular endothelial growthfactor-C-mediated lymphangiogenesis promotes tumor metastasis.EMBO J 2001;20:672–82.3. Solcia E, Kloppel G, Sobin LH. Histological typing of endocrinetumors. International histological classification of tumors WHO, 2nd ed.Springer Verlag; Berlin: 2000.4. Banerji S, Ni J, Wang SX, et al. LYVE-1, a new homologue of theCD44 glycoprotein, is a lymph-specific receptor for hyaluronan. J CellBiol 1999;144:789–801.5. Breiteneder-Geleff S, Soleiman A, Kowalski H, et al. Angiosarcomasexpress mixed endothelial phenotypes of blood and lymphatic capillar-ies: podoplanin as a specific marker for lymphatic endothelium. Am JPathol 1999;54:385–94.6. Kukk E, Lymboussaki A, Taira S, et al. VEGF-C receptor bindingand pattern of expression with VEGFR-3 suggests a role in lymphaticvascular development. Development (Camb) 1996;122:3819–27.7. Veikkola T, Karkkainen M, Claesson-Welsh L, Alitalo K. Regulationof angiogenesis via vascular endothelial growth factor receptors. CancerRes 2000;60:203–12.8. Terris B, Soazec JY, Rubbia L, et al. Expression of vascular endo-thelial growth factor in digestive neuroendocrine tumors. Histopathol-ogy 1998;32:133–8.9. . Jackson DG. New molecular markers for the study of tumorlymphangiogenesis. Anticancer Res 2001;21:4279–83.10. Maula SM, Luukkaa M, Grenman R, et al. Intratumoral lymphaticsare essential for the metastatic spread and prognosis in squamous cellcarcinomas of the head and neck region. Cancer Res 2003;63:1920–6.11. Sedivy R, Beck-Mannagetta J, Haverkampf C, Battistutti W, Honig-schnabl S. Expression of vascular endothelial growth factor-C correlateswith the lymphatic microvessel density and the nodal status in oralsquamous cell cancer. Oral Pathol Med 2003;32:455–60.12. Beasley NJ, Prevo R, Banerji S, et al. Intratumoral lymphangiogen-esis and lymph node metastasis in head and neck cancer. Cancer Res2002;62:1315–20.13. Hall FT, Freeman JL, Asa SL, Jackson DG, Beasley NJ. Intratu-moral lymphatics and lymph node metastases in papillary thyroid car-cinoma. Arch Otolaryngol Head Neck Surg 2003;129:716–9.14. Straume O, Jackson DG, Akslen LA. Independent prognostic im-pact of lymphatic vessel density and presence of low-grade lymphangio-genesis in cutaneous melanoma. Clin Cancer Res 2003;9:250–6.
6927Clinical Cancer Research
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

15. Williams CS, Leek RD, Robson AM, et al. Absence of lymphangio-genesis and intratumoural lymph vessels in human metastatic breastcancer. J Pathol 2003;20:195–206.16. Joukov V, Pajusola K, Kaipainen A, et al. A novel vascular endo-thelial growth factor, VEGF-C, is a ligand for the Flt4 (VEGFR-3) andKDR (VEGFR-2) receptor tyrosine kinases. EMBO J 1996;15:290–8.17. Pepper MS, Tille JC, Nisato R, Skobe M. Lymphangiogenesis andtumor metastasis Cell Tissue Res 2003;314:167–77.18. Neuchrist C, Erovic BM, Handisurya A, et al. Vascular endothelialgrowth factor C and vascular endothelial growth factor receptor 3expression in squamous cell carcinomas of the head and neck. HeadNeck 2003;6:464–74.19. Niki T, Iba S, Tokunou M, et al. Expression of vascular endothelialgrowth factors A, B, C, and D and their relationships to lymph nodestatus in lung adenocarcinoma. Clin Cancer Res 2000;6:2431–9.20. Bunone G, Vigneri P, Mariani L, et al. Expression of angiogenesisstimulators and inhibitors in human thyroid tumors and correlation withclinical–pathologic features. Am J Pathol 1999;55:1967–76.21. Tsurusaki T, Kanda S, Sakai H, et al. Vascular endothelial growthfactor-C expression in human prostatic carcinoma and its relationship tolymph node metastasis. Br J Cancer 1999;80:309–13.22. Ohta Y, Nozawa H, Tanaka Y, Oda M, Watanabe Y. Increasedvascular endothelial growth factor and vascular endothelial growthfactor-C and decreased expression associated with microdisseminationin the lymph nodes in stage I non-small cell lung cancer. J ThoracCardiovasc Surg 2000;119:804–13.23. Ohta Y, Shridhar V, Bright RK, et al. VEGF and VEGF type C playan important role in angiogenesis and lymphangiogenesis in humanmalignant mesothelioma tumours. Br J Cancer 1999;81:54–61.
24. Akagi K, Ikeda Y, Miyazaki M, et al. Vascular endothelial growthfactor-C (VEGF-C) expression in human colorectal cancer tissues. Br JCancer 2000;83:887–91.
25. Yonemura Y, Endo Y, Fujita H, et al. Role of vascular endothelialgrowth factor C expression in the development of lymph node metas-tasis in gastric cancer. Clin Cancer Res 1999;5:1823–9.
26. Arinaga M, Noguchi T, Takeno S, et al. Clinical significance ofvascular endothelial growth factor C and vascular endothelial growthfactor receptor 3 in patients with nonsmall cell lung carcinoma. Cancer(Phila) 2003;97:457–64.
27. Van Trappen PO, Steele D, Lowe DG, et al. Expression of vascularendothelial growth factor (VEGF)-C and VEGF-D, and their receptorVEGFR-3, during different stages of cervical carcinogenesis. J Pathol2003;201:544–54.
28. Skobe M, Hawighorst T, Jackson DG, et al. Induction of tumorlymphangiogenesis by VEGF-C promotes breast cancer metastasis. NatMed 2001;7:192–8.
29. Marion-Audibert AM, Barel C, Gouysse G, et al. Low microvesseldensity is an unfavorable histoprognostic factor in pancreatic endocrinetumors. Gastroenterology 2003;125:1094–104.
30. Hansel DE, Rahman A, Hermans J, et al. Liver metastases arisingfrom well-differentiated pancreatic endocrine neoplasms demonstrateincreased VEGF-C expression. Mod Pathol 2003;16:652–9.
31. Hanrahan V, Currie MJ, Gunningham SP, et al. The angio-genic switch for vascular endothelial growth factor (VEGF)-A,VEGF-B, VEGF-C, and VEGF-D in the adenoma-carcinoma se-quence during colorectal cancer progression. J Pathol 2003;200:183–94.
6928 Lymphatic Status of PENS
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2004;10:6919-6928. Clin Cancer Res Laura Rubbia-Brandt, Benoit Terris, Emile Giostra, et al. Human Pancreatic Endocrine TumorsFactor-C Expression Correlate with Malignant Behavior in Lymphatic Vessel Density and Vascular Endothelial Growth
Updated version
http://clincancerres.aacrjournals.org/content/10/20/6919
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/10/20/6919.full#ref-list-1
This article cites 30 articles, 9 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/10/20/6919.full#related-urls
This article has been cited by 9 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/10/20/6919To request permission to re-use all or part of this article, use this link
Research. on June 5, 2020. © 2004 American Association for Cancerclincancerres.aacrjournals.org Downloaded from