Lymphangioma involving the urogenital system in childhood · Lymphangioma involving the urogenital...
4
Lymphangioma involving the urogenital system in childhood Michael Yap a, * , Robert Newbury b , Denise Malicki b , George Chiang a a Division of Pediatric Urology, Rady Children’s Hospital, 7920 Frost Street, Suite 200, San Diego, CA 92123, USA b Department of Pathology, Rady Children’s Hospital, 3020 Children’s Way, San Diego, CA 92123, USA article info Article history: Received 16 July 2015 Received in revised form 19 August 2015 Accepted 20 August 2015 Key words: Lymphangioma Bladder Scrotum Childhood abstract Lymphangioma of the urogenital system is extremely rare and we present two cases treated at our institution over a one year period. The first case is a 3 year-old boy who presented with scrotal swelling and was initially thought to have a complex hydrocele. On surgical exploration, an extratesticular multiloculated cystic mass was discovered and testis-sparing excision of the mass was performed. Pa- thology revealed lymphangioma. The second case is a 5 year-old male who initially presented with gross hematuria. Ultrasound was unremarkable but cystoscopy revealed varicosities extending from the bladder wall. On transurethral resection, histology showed non-specific benign vascular malformation. Magnetic resonance imaging (MRI) was obtained because of persistent hematuria and showed multiple bladder lesions suggestive of lymphatic malformation. Partial cystectomy was ultimately performed and histology confirmed lymphangioma. To the author’s knowledge, this represents the fifth reported case of lymphangioma of bladder. Ó 2015 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Lymphangioma is a benign lymphatic malformation, most commonly seen in the neck and axillary regions. Lymphangioma involving the urogenital system is extremely rare. Herein, we describe one case involving the bladder and another case involving the scrotum. 1. Case report 1 A 3 year-old boy initially presented with a 1-year history of painless, progressive swelling in his left scrotum. Physical exami- nation showed bilaterally descended testes and a non-tender, soft, compressible mass in the left hemiscrotum suggestive of hydrocele. Ultrasound of the testes was done and demonstrated fluid around the left testis containing low-level echoes due to debris and mul- tiple septae (Fig. 1). Based on clinico-radiological findings, a pro- visional diagnosis of complex left hydrocele was suggested. The swelling was initially explored via a left inguinal incision. A mul- ticystic lesion separate from the left testis but densely adhered to the scrotal wall and perineum was identified (Fig. 2). The left testis and spermatic cord were easily separated from the lesion. The left testis was normal in size and appearance. No hydrocele or hernia were identified. Complete excision of the lesion was performed and the overlying scrotal skin spared. Macroscopy showed tan to dark brown to black nodular tissue measuring 4 3.8 2.7 cm. Sectioning revealed multicystic compartments, some of which contained clear serous fluid, hemorrhagic dark brown material, and clear gelatinous material. Dilated cystic spaces were lined by bland endothelial cells, with small amounts of smooth muscle within the walls of vascular structures (Fig. 3). Immunostaining was positive for CD31 and D2-30, consistent with a diagnosis of lymphangioma. At follow up 1 month later, there was no evidence of recurrence. 2. Case report 2 A 5 year-old boy initially presented with penile pain and blood at the urethral meatus. Physical examination was unremarkable, urinalysis was negative, and a diagnosis of probable meatitis was given. The patient subsequently re-presented three years later at the age of 8 with intermittent gross hematuria. He had no addi- tional complaints. Physical exam was again unremarkable. Urinal- ysis showed blood but was otherwise negative. Urine culture was negative for bacteria and ultrasonography showed no abnormal- ities. Cystoscopy under anesthesia was performed, which revealed a lesion with varicosities at the right lateral bladder wall (Fig. 4). Bilateral retrograde pyelograms revealed no upper tract abnor- malities. Transurethral resection of the bladder lesion was per- formed and histology revealed benign vascular malformation. The specimen showed submucosa with varying-sized vascular channels * Corresponding author. Tel.: þ1 858 9668446. E-mail address: [email protected] (M. Yap). Contents lists available at ScienceDirect Journal of Pediatric Surgery CASE REPORTS journal homepage: www.jpscasereports.com 2213-5766/Ó 2015 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). http://dx.doi.org/10.1016/j.epsc.2015.08.012 J Ped Surg Case Reports 3 (2015) 419e422
Transcript of Lymphangioma involving the urogenital system in childhood · Lymphangioma involving the urogenital...

Contents lists available at ScienceDirect
J Ped Surg Case Reports 3 (2015) 419e422
Journal of Pediatric Surgery CASE REPORTS
journal homepage: www.jpscasereports .com
Lymphangioma involving the urogenital system in childhood
Michael Yap a,*, Robert Newbury b, Denise Malicki b, George Chiang a
aDivision of Pediatric Urology, Rady Children’s Hospital, 7920 Frost Street, Suite 200, San Diego, CA 92123, USAbDepartment of Pathology, Rady Children’s Hospital, 3020 Children’s Way, San Diego, CA 92123, USA
a r t i c l e i n f o
Article history:Received 16 July 2015Received in revised form19 August 2015Accepted 20 August 2015
Key words:LymphangiomaBladderScrotumChildhood
* Corresponding author. Tel.: þ1 858 9668446.E-mail address: [email protected] (M. Yap).
2213-5766/� 2015 The Authors. Published by Elsevierhttp://dx.doi.org/10.1016/j.epsc.2015.08.012
a b s t r a c t
Lymphangioma of the urogenital system is extremely rare and we present two cases treated at ourinstitution over a one year period. The first case is a 3 year-old boy who presented with scrotal swellingand was initially thought to have a complex hydrocele. On surgical exploration, an extratesticularmultiloculated cystic mass was discovered and testis-sparing excision of the mass was performed. Pa-thology revealed lymphangioma. The second case is a 5 year-old male who initially presented with grosshematuria. Ultrasound was unremarkable but cystoscopy revealed varicosities extending from thebladder wall. On transurethral resection, histology showed non-specific benign vascular malformation.Magnetic resonance imaging (MRI) was obtained because of persistent hematuria and showed multiplebladder lesions suggestive of lymphatic malformation. Partial cystectomy was ultimately performed andhistology confirmed lymphangioma. To the author’s knowledge, this represents the fifth reported case oflymphangioma of bladder.� 2015 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND
license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Lymphangioma is a benign lymphatic malformation, mostcommonly seen in the neck and axillary regions. Lymphangiomainvolving the urogenital system is extremely rare. Herein, wedescribe one case involving the bladder and another case involvingthe scrotum.
1. Case report 1
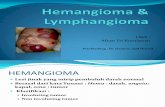
A 3 year-old boy initially presented with a 1-year history ofpainless, progressive swelling in his left scrotum. Physical exami-nation showed bilaterally descended testes and a non-tender, soft,compressible mass in the left hemiscrotum suggestive of hydrocele.Ultrasound of the testes was done and demonstrated fluid aroundthe left testis containing low-level echoes due to debris and mul-tiple septae (Fig. 1). Based on clinico-radiological findings, a pro-visional diagnosis of complex left hydrocele was suggested. Theswelling was initially explored via a left inguinal incision. A mul-ticystic lesion separate from the left testis but densely adhered tothe scrotal wall and perineumwas identified (Fig. 2). The left testisand spermatic cord were easily separated from the lesion. The lefttestis was normal in size and appearance. No hydrocele or herniawere identified. Complete excision of the lesionwas performed and
Inc. This is an open access article u
the overlying scrotal skin spared. Macroscopy showed tan to darkbrown to black nodular tissue measuring 4 � 3.8 � 2.7 cm.Sectioning revealed multicystic compartments, some of whichcontained clear serous fluid, hemorrhagic dark brownmaterial, andclear gelatinous material. Dilated cystic spaces were lined by blandendothelial cells, with small amounts of smooth muscle within thewalls of vascular structures (Fig. 3). Immunostaining was positivefor CD31 and D2-30, consistent with a diagnosis of lymphangioma.At follow up 1 month later, there was no evidence of recurrence.
2. Case report 2
A 5 year-old boy initially presented with penile pain and bloodat the urethral meatus. Physical examination was unremarkable,urinalysis was negative, and a diagnosis of probable meatitis wasgiven. The patient subsequently re-presented three years later atthe age of 8 with intermittent gross hematuria. He had no addi-tional complaints. Physical exam was again unremarkable. Urinal-ysis showed blood but was otherwise negative. Urine culture wasnegative for bacteria and ultrasonography showed no abnormal-ities. Cystoscopy under anesthesiawas performed, which revealed alesion with varicosities at the right lateral bladder wall (Fig. 4).Bilateral retrograde pyelograms revealed no upper tract abnor-malities. Transurethral resection of the bladder lesion was per-formed and histology revealed benign vascular malformation. Thespecimen showed submucosa with varying-sized vascular channels
nder the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

Fig. 1. Scrotal ultrasound showing lymphangioma of scrotum with air-fluid levels.
Fig. 3. Scrotal lymphangioma. Large thin-walled vascular space lined by endothelialcells with small amount of smooth muscle and focal collections of lymphocytes in wall.
M. Yap et al. / J Ped Surg Case Reports 3 (2015) 419e422420
lined by flat endothelial cells and filled with blood/proteinaceousmaterial. Immunostaining was strongly positive for CD31 and rarefor D2-40. Urine cytology was negative. Follow up magnetic reso-nance imaging (MRI) was performed and revealed multiple nodularand serpiginous areas of T1 and T2 signal abnormality, extensivelyinvolving the right lateral wall, left anterolateral wall, dome, andbladder base (Fig. 5). The lesions exhibited inconsistent signalchanges but the bulk appeared bright on T1 and T2 sequences anddid not enhance. The dominant bladder lesion measured approxi-mately 26 � 9 � 21 mm. On magnetic resonance angiogram (MRA),no arterial or venous contribution, early draining vein, or earlyarterial enhancement were seen to suggest venous malformation,arteriovenous malformation (AVM), or hemangioma. Surgicaltreatment was undertaken because of the patient’s persistent he-maturia. Open partial cystectomy was successfully performed. Thelesion had poorly defined borders and consisted of many cystsseparated from each other by solid partitions and containingtransparent fluid. The lesion was primarily located at the bladderdome and anterior wall but also extended to both lateral walls andthe posterior bladder wall. The lesions involved the perivesicalspace and also protruded full-thickness through the bladder atvarious locations. Histologic examination revealed that the cysticmass was composed of numerous transmural cavernous vascularlesions, some with rare thickened hyalinized or myxoid walls butthe majority lined with a single layer of flattened endothelium.Many of the vascular channels contained lightly eosinophilic lymph,while many others were filled with red cells (Fig. 6). Immuno-staining was positive for both CD43 and D2-40. The presence of
Fig. 2. Intraoperative view showing multiloculated cystic mass delivered throughscrotal incision.
peripheral blood within some of the lesional vessels raised thediagnostic consideration of a venous component; however, D2-40labeled the majority of the vessels, supporting the clinical impres-sion of a lymphangioma. The boy had an uneventful post-operativecourse and was discharged from the hospital 2 days after the pro-cedure. At follow-up 7 months later, patient reported intermittenthematuria that was significantly improved from prior to surgery. Arepeat MRI showed residual lesions at the right anterolateral walldecreased from prior to surgery and no new masses. He is beingobserved for now with plans for possible endoscopic interventionshould his hematuria persist.
3. Discussion
Lymphangiomas are benign vascular lesions that usually arisefrom embryologic disturbances in the development of thelymphatic system [1]. Whereas the majority of these lesions arecongenital due to insufficiency or atresia of the efferent lymphaticsand venous channels, they can also be acquired after infection,inflammation, or degeneration [2]. Symptoms of lymphangiomasare related to the anatomical location of these lesions, as well as tothe extent of involvement of the local anatomical structures. Theycan be seen in any anatomic region but are more commonly seen inlymphatic-rich areas, such as the neck (75%) and axilla (20%) [3].Histologically, there are three primary types: capillary, cavernous,and cystic. The cystic form is the most common variety [4]. Lesionsare composed of vascular spaces filled with eosinophilic and pro-tein-rich fluid. A single layer of flattened endothelium lines the
Fig. 4. Cystoscopic view of lymphangioma of the bladder consisting of mucosalvaricosities.

Fig. 5. A) MRI showing lymphangioma of the bladder at right lateral wall. B) MRI showing lymphangioma of the bladder at anterior wall in the midline and left anterolateral wall. C)MRI showing lymphangioma of the bladder at right anterolateral wall.
M. Yap et al. / J Ped Surg Case Reports 3 (2015) 419e422 421
walls of lymphatic channels. Hemorrhagewithin the cystic spaces iscommon and indicates recent trauma or spontaneous intralesionalbleeding. The majority of lymphangiomas (90%) develop during thefirst two years of life and 50% are present at birth [5]. Unlikehemangiomas, lymphangiomas persist throughout life, grow pro-portionately with the size of the patient, and do not undergoinvolution [1].
3.1. Lymphangioma of the scrotum
The intrascrotal presentation of lymphangiomas is rare at anyage. Loberant et al. estimated less than fifty cases reported in theliterature as of 2002 [6]. The most typical locations are the scrotalwall and tunics [7], although the testis, epididymis, spermatic cord,and Colles fascia may also be involved [2]. Most present as painless,indolent scrotal masses but can sometimes be associatedwith acutescrotum due to enlargement or pain following infection or hem-orrhage [8,9]. High resolution ultrasonography is highly accurate indelineating the type and extent of lesions in most cases.
Fig. 6. A) Lymphangioma of the bladder. Submucosal cavernous thin-walled channels. B)extending into surrounding connective tissue. C) Lymphangioma of the bladder. Cavernous
Ultrasonography reveals a cystic mass with multiple septations andlocules filled with low level internal echoes that may bemobile. Theechoes may be due to internal hemorrhage or debris. Septationsoften show low velocity and high resistance vascular flow, charac-teristic of benign lesions [6]. Computed tomography and magneticresonance imaging may also be helpful in evaluating for extensioninto the pelvis or retroperitoneum. As cystic lymphangiomas do notcommunicate with the lymphatic system, lymphangiography is notrecommended [10]. The differential diagnosis of scrotal lym-phangioma includes hernia, hydrocele, pyocele, hematocele, sper-matocele, varicocele, and primary tumor of the testis [8]. Presenceof septal flow differentiates cystic lymphangioma from hydrocele,pyocele, and hematocele; whereas, absence of color flow in thecystic spaces differentiates lymphangioma from varicocele. Despitepreoperative imaging, they are often misdiagnosed before surgery[11e13]. Hurwitz et al. reported seven cases of scrotal lym-phangioma over a ten-year period, all of which were misdiagnosedprior to surgery [13]. As in our case, the patient was thought to havea complex hydrocele based on clinical and radiologic findings prior
Lymphangioma of the bladder. Cavernous thin-walled channels containing lymph andthin-walled channels traversing through mural smooth muscle.

M. Yap et al. / J Ped Surg Case Reports 3 (2015) 419e422422
to surgery. Local recurrence is common and complete surgicalexcision along with overlying skin has been recommended. Othertreatment modalities such as injection of sclerosants, extensivefulguration, and cryotherapy have been reported but without muchsuccess.
3.2. Lymphangioma of the bladder
Lymphangioma only rarely occurs in the urinary tract. About 40cases have been described involving the kidney and 2 cases havebeen reported involving the urethra [14e16]. Only 4 cases of lym-phangioma of the bladder have been reported worldwide since1983. Bolkier et al. reported the first case in a boy who presentedwith macroscopic painless hematuria and was treated with partialcystectomy [17]. Wyler et al. reported the second case in a 49 year-old male presenting with irritative voiding symptoms. Cystoscopyshowed a non-papillary lesion located between the two ureteralorifices. The patient was managed with transurethral resection andhistology revealed lymphangioma of the bladder. Three monthsafter the procedure, the irritative voiding symptoms had improvedand therewas no evidence of residual tumor on cystoscopy [18]. Niuet al. reported on two additional cases of bladder lymphangioma inchildren. The first was an 8 year-old girl who presented with ter-minal hematuria accompanied and intermittent fever. Imagingrevealed a sharply defined 0.5-cm mass in the right lateral bladderwall. On cystoscopy, the tumor was red and found to be bulging intothe bladder. A partial cystectomy was performed and histologyrevealed lymphangioma involving the full-thickness of the bladder.She had no evidence of recurrence at 3 years of follow up [19]. Theother case reported by Niu et al. was a 5 year-old boy who pre-sented with abdominal pain and palpable pelvic mass. Computedtomography and magnetic resonance imaging revealed a 12-cmcystic lesion anterior to the rectum, occupying the pelvic cavity, anddisplacing the bladder downward and laterally. Mass partial cys-tectomywas performed and histology revealed lymphangioma. Themass was located extraperitoneally and was firmly attached tothe superior and posterior walls of the bladder. It penetrated thedetrusor muscle but did not protrude into the bladder cavity. Theboy was recurrence-free at 3 months [20]. While not specificallydescribed for treatment of bladder lymphangiomas, endoscopiclaser ablation may be an option based on reports of successfulcontrol of bladder hemangiomas, mainly using the neo-dymium:yttrium aluminum garnet (Nd:YAG) laser. It is importantto know that when laser ablation has been used for bladder hem-angiomas, treatments were often carried out several occasions[21e23].
4. Conclusion
In summary, although the scrotum is a very rare site for lym-phangioma, it should be considered in the list of differential diag-nosis of multiloculated, benign-appearing scrotal lesions. Althoughultrasonography can be useful in establishing a preoperative diag-nosis, misdiagnosis is relatively common. Awareness of these le-sions is integral in making a correct diagnosis, to avoidmismanagement and reduce recurrences.
Lymphangioma of the bladder is also a benign lesion and does notregress. Its symptoms are generally related to infection and hemor-rhage, as well as to the size of the malformation and perturbation ofadjacent tissues altering structure and function. Open resection isideal for the disease; however, because the lesion is benign, anextensive operation is not warranted. Endoscopic laser ablation maybe an option when partial cystectomy is precluded but may requiremultiple procedures for initial control and repeat procedures forrecurrences. Preoperative diagnosis may be difficult because of therarity of this lesion and it’s non-specific presentation clinically andradiologically. Ultrasound has been suggested as a useful tool forfollow up in children and prognosis is generally good after resection.
Conflict of interestNone.
References
[1] Elleru RG, Balakrishnan K, Padua HM. Lymphatic malformations: diagnosis andmanagement. Semin Pedaitr Surg 2014;23:178e85.
[2] Koshy A, Tandon RK, Kapur BM, Rao KV, Joshi K. Retroperitoneal lym-phangioma: a case report with review of the literature. Am J Gastroenterol1978;69:485e90.
[3] De Perrot M, Rostan O, Morel P, Le Coultre C. Abdominal lymphangioma inadults and children. Br J Surg 1998;85:395e7.
[4] Cutillo DP, Swayne LC, Cucco J, Dougan H. CT and MR imaging in cysticabdominal lymphangiomatosis. J Comput Assist Tomogr 1989;13:534e6.
[5] Mulcahy JJ, SChileru G, Donmezer M, Bhathena D. Lymphangioma of thescrotum. Urology 1979;14:64e5.
[6] Loberant N, Chernihovski A, Goldfeld M. Role of Doppler sonography in thediagnosis of cystic lymphangioma of the scrotum. J Clin Ultrasound 2002;30:384e7.
[7] Millan RW, Donald BR, Alpern HD. Scrotal lymphangioma. Urology 1984;33:79e80.
[8] Wiedman ED, Cendron M, Schned AR, Harris RD. Scrotal lymphangioma: anuncommon cause for a scrotal mass. J Ultrasound Med 2002;21(6):669e72.
[9] Hacker A, Hatzinger M, Grobholz R, Alken P, Hoang-Bohm J. Scrotal lym-phangioma: a rare cause of acute scrotal pain in childhood. Aktuelle Urol2006;37:445e8.
[10] Chung SE, Frush DP, Fordham LA. Sonographic appearance of extratesticularfluid and fluid containing scrotal masses in infants and children: clues todiagnosis. AJR Am J Roentgenol 1999;173:741e5.
[11] Ratan SK, Rattan KN, Sehgal T, Maggu S. Spermatic cord lymphangioma in a 7year old child masquerading as a hydrocele. Br J Urol Int 2003;10:4046.
[12] Parakh A, Dubey AP, Garg A, Khurana N, Aggarwal SK. Cystic lymphangiom-atous hamartoma masquerading as massive ascites. Indian J Pediatr 2009;76:753e4.
[13] Hurwitz RS, Shapiro E, Hulbert WC. Scrotal cystic lymphangioma: the mis-diagnosed scrotal mass. J Urol 1997;158:1182e5.
[14] Honma Y, Takagi Y, Shigyo M, Sunaoshi K, Wakabayashi J, Harada O, et al.Lymphangioma of the kidney. Int J Urol 2002;9:178e82.
[15] Jadeja NA, Yadav SP. Lymphangioma of the urethra. Urol Int 1994;53:104e6.[16] Tahtali N, Yazicioglu A, Dalva I, Sargin S, Cetin S. An unusual cause of urethral
stricture: urethral lymphangioma. Eur Urol 1994;26:347e8.[17] Bolkier M, Ginesin Y, Lichtig C, Levin DR. Lymphangioma of bladder. J Urol
1983;129:1049e50.[18] Wyler SF, Bachmann a, Singer G, Gasser TC, Sulser T. First case of lym-
phangioma of the bladder in an adult. Urol Int 2004;73(4):374e5.[19] Niu ZB, Yang Y, Hou Y, Chen H, Liu X, Wang CL. Lymphangioma of bladder.
Urology 2010;76(4):955e7.[20] Niu ZB, Ying H, Sun RG, et al. Cystic lymphatic malformation of bladder pre-
senting as a pelvic mass. J Pediatr Surg 2011;46:1284e7.[21] Takemoto J, Yamazaki Y, Sakai K. A case of large bladder hemangioma suc-
cessfully treated with endoscopic yttrium aluminum garnet laser irradiation.Int J Urol 2011;18:854e6.
[22] Vicente J, Salvador J. Neodymium:YAG laser treatment of bladder hemangi-omas. Urology 1990;36:305e8.
[23] Smith Jr JA, Dixon JA. Neodymium:YAG laser irradiation of bladder heman-gioma. Urology 1984;24:134e6.