Lyme disease
43
Lyme Disease Keith Berndtson, MD A Systems Medicine Approach
-
Upload
keith-berndtson -
Category
Health & Medicine
-
view
8.965 -
download
0
description
This presentation tackles the controversy regarding Lyme disease by reviewing the evidence for immune evasion and persistent infection by the Lyme spiorchete, Borrelia burgdorferi. The evidence shows that physicians called upon to assist patients with this potential diagnosis should be open to the possibility of persistent infection even in patients who have already received antibiotic treatment for their condition. Lacking evidence on how best to treat a chronic infection of this kind, physicians should be allowed to rely on their experience and to exercise their best clinical judgment in managing patients with Lyme disease.
Transcript of Lyme disease

Lyme Disease
Keith Berndtson, MD
A Systems Medicine Approach

Lyme Wars, circa 2013
ILADS Is not a persistent infection! vs. Is so a persistent infection!

Underpowered studies that purport to demonstrate universal efficacy must be viewed with circumspection.
Everyone is studying the early stage of this infection; no one is studying the persistent phase of the disease. It is important that those studies occur.
All the bitterness of the debate does not serve the science or the patient...[it] drowns out the complexity and nuance of the work that needs to be done.
The 2011 Institute of Medicine Report
2011

What is the physician’s dutywhen assisting patients with Lyme disease?
Hippocratic Oathon papyrus, 200 AD
Know and teach the evidence for immune evasion and persistent infection in Lyme disease.
Learn the varied clinical presentations of Lyme disease.
Apply evidence-based care strategies within a shared decision-making model that respects patient values.
Monitor and document clinical outcomes.

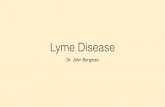
2012 Yale Lyme Risk Map
• Map produced by the Yale School of Public Health
• Released February, 2012
• Includes a high risk “sliver” in Northern Illinois
• Most of Northern Illinois considered a transitional area

July 2012 Illinois Tick survey
56.4% of over 1,067 ticks collected from 17 sites in Cook, Lake, McHenry, and DuPage counties were deer ticks.

Dispersal of Borrelia burgdorferi by songbirds can help account for the dramatic increase in the incidence of tick-borne diseases in North America and Europe over the past 16 years.
Bloated tick on a Cedar Waxwing

In a 2007 tick survey of Lake and Cook counties, 37% of adult deer ticks collected were + for Borrelia burgdorferi. (1)
A 2006 report by this team found that only 3-5% of adult deer ticks in Cook and DuPage counties were + for Bb. (2)
(1) Jobe DA, Nelson JA, Adam MD, Martin SA. Lyme disease in urban areas, Chicago. Emerging Infectious Diseases. 2007;13(11):1799-1800.
(2) Jobe DA, Lovrich SD, Nelson JA, et al. Borrelia burgoderferi in Ixodes scapularis ticks, Chicago area. Emerging Infectious Diseases. 2006;12:1039-1041.
Research shows a 7 to 10-fold increase in Chicago
area Bb-infected deer ticks between 2005 and 2007.
Questing Deer tick
Borrelia burgdorferi

Evidence for Immune Evasion in Lyme Disease
Cross-disciplinary studies

Evidence for Immune Evasion in Lyme Disease
“Borrelia species may well have the most unusual genomes on the planet. No other bacteria have such a large complement of extra-chromosomal elements. They perform an uncommon process known as telomere resolution that can explain the wide-ranging variability in linear plasmid size, content, and sequence scrambling.” - George Chaconas, the Canadian Society for
Microbiology Murray Lecture
A Flexibly Adaptive Genome
Canadian Journal Microbiology 2011;58(3):236-48.

Tick salivary protein (Salp-15) binds to CD4 on T helper cells and to OspC on Bb, which delays the humoral response to Bb, allowing early dissemination into connective tissue and the central nervous system. Salp-15 and OspC collaborate to enhance the virulence of Bb during the early stages of infection.
Evidence for Immune Evasion in Lyme Disease
Bb Commandeers Tick Salivary Protein
Ramamoorthi N, et al. The Lyme disease antigen exploits a tick protein to infect the mammalian host. Nature 2005;436(7050):573-7.
Hovius J, et. al. Tick-host-pathogen interactions in Lyme borreliosis. Trends in Parasitology 2007;23(9):434-438.

Evidence for Immune Evasion in Lyme Disease
Antigen Masking
Bb evades complement-mediated killing by interacting with complement regulators through distinct complement regulator-acquiring surface proteins (CRASPs). CRASP-1 is a multifunctional protein of Bb that binds to several human extracellular matrix proteins and plasminogen. These interactions contribute to adhesion, bacterial colonization, and organ tropism and assist with dissemination of Bb in the host.
Kurtenbach K, et al. Host association of Bb sensu lato - the key role of host complement. Trends in Microbiology. 2002;10(2):74-9.
Kraiczy P, Stevenson B. Complement regulator-acquiring surface proteins of Bb: structure, function, and regulation of gene expression. Ticks and Tick Borne Diseases. 2013 Feb;4(1-2):26-34.
Bb’s Factor H “hall pass”

Bb’s outer membrane protein, OspC, binds to plasminogen, activating the serine protease, plasmin. Plasmin induces the release of collagenases and MMPs (matrix metallproteinases), which enhance Bb’s ability to pass through tight junctions. Bb thus usurps the fibrinolytic pathways of its host to help it penetrate otherwise impermeable tissue barriers. The result: rapid deep tissue invasion.
Toledo A, et al. The enolase of Borrelia burgdorferi is a plasminogen receptor released in outer membrane vesicles. Infection and Immunity. 2012 Jan;80(1):359-68.
The Blood-Brain BarrierPlasmin + MMPs
Bb spirochete able to disrupt tight junctions causing a leaky blood-brain barrier and a portal of entry into the brain.
Bb Usurps the Host’s Plasminogen Activating System
Evidence for Immune Evasion in Lyme Disease
Hu LT, et al. Binding of human plasminogen to Borrelia burgdorferi. Infection and Immunity. 1995 Sep;63(9):3491-6.

Bb Encodes for “Best in Class” Antigenic Variation
Evidence for Immune Evasion in Lyme Disease
Norris SJ. How do Lyme Borrelia organisms cause disease? The quest for virulence determinants. Open Neurology Journal. 2012;6(Suppl 1-M8):119-123.
Ongoing antigenic variation frustrates the host’s antibody response to Borrelia burgdorferi. B-cells become confused, causing excess B-cell traffic in lymph nodes and a weak and delayed marrow plasma cell response. Hastey CJ, et al. Delays and diversions mark the development of B cell responses to Borrelia burgdorferi infections. Journal of Immunology 2012;188(11):5612-22.
The VlsE sequence variants produce different antigen epitopes. Recombination occurs continuously during mammalian infection and plays a key role in immune evasion and the long-term survival of Bb in humans.
15 silent vls casse-es expressed vlsE casse-e

Sources of Immune Evasion in Lyme Disease
Atypical Forms
Mikossly J, et al. Persisting atypical and cystic forms of Borrelia burgdorferi and local inflammation in Lyme borreliosis. J Neuroinflammation 2008;5:40.
A cystic form.Rolled forms
Bb strain B31
Bb strain ADBI thickenedmembrane
The results indicate that atypical extra- and intracellular pleomorphic and cystic forms of Borrelia burgdorferi and local neuroinflammation occur in the brain in chronic Lyme neuroborreliosis. The persistence of these more resistant spirochete forms, and their intracellular location in neurons and glial cells, may explain the long latent stage and persistence of Borrelia infection.

Brorsson O, Brorsson SH. Transformation of cystic forms of Borrleia burgdorferi to normal, mobile spirochetes. Infection 1997;4:241-46.
Miklossy J, et al. Persisting atypical and cystic forms of Borrelia burgdorferi and local inflammation in Lyme borreliosis. J Neuroinflammation 2008;5:40.
Cystic forms of Bb.
Rolled forms of Bb
Cystic forms of Bb. Plasma membrane inside cystic structure (i) thinner than
extracystic plasma membrane (e).
Sources of Immune Evasion in Lyme Disease
Atypical Forms

Gene transfer by bacterial conjugation and by DNA transformation happens efficiently in biofilms, and this process helps stabilize the biofilm structure.
Molin S. Gene transfer occurs with enhanced efficiency in biofilms and induces enhanced stabilization of the biofilm structure. Curremt OPinions in Biotechnology. 2003;14:255-261.
Horizontal Gene TransferSources of Immune Evasion in Lyme Disease
Conjugation Transformation

Evidence for Immune Evasion in Lyme Disease
Advanced Motility Capabilities

Evidence for Immune Evasion in Lyme Disease
High Performance Flagellar Motors

Evidence for Immune Evasion in Lyme Disease
Elite Flagellar Design

Evidence for Immune Evasion in Lyme Disease
Advanced Flagellar Maneuverability

Evidence for Immune Evasion in Lyme Disease
Evasive Chemotaxis and Niche-Seeking Behavior
Moriarty TJ, et al. Real-time high resolution 3D imaging of the Lyme disease spirochete adhering to and escaping from the vasculature of the living host. PLoS Pathogen 2008;4(6).

Evidence for Immune Evasion in Lyme Disease
Movement through Vascular Walls
Moriarty TJ, et al. Real-time high resolution 3D imaging of the Lyme disease spirochete adhering to and escaping from the vasculature of the living host. PLoS Pathogen 2008;4(6).

Evidence for Immune Evasion in Lyme Disease
Rapid Escape from Vascular Compartment into the Extracellular Matrix
Moriarty TJ, et al. Real-time high resolution 3D imaging of the Lyme disease spirochete adhering to and escaping from the vasculature of the living host. PLoS Pathogen 2008;4(6).
Spirochetes would transmigrate through the venule wall, typically at the endothelial cell junctions, and escape into the surrounding extracellular matrix in a process that averaged 10.8 minutes. The speed of the final escape yielded images in which spirochetes appeared to burst away from the vessel. The matrix is like a sanctuary from immune traffic, and Bb escapes to it in a hurry.

Evidence for Immune Evasion in Lyme Disease
Bb Quorum Sensing and Biofilm-Like Behavior
Sapi E, et al. Characterization of biofilm formation by Borrelia burgdorferi In Vitro. PLoS ONE;7(10):e48277.
Babb K, et al. Synthesis of autoinducer-2 by the Lyme disease spirochete. Journal of Bacteriology 2005;187:3079-87.
Bb respond to AI-2 by expressing factor H-binding protein to enhance immune evasion.
Stevenson B, et al. LuxS-mediated quorum sensing in the Lyme disease spirochete. Infection and Immunity 2002;70:4099-4105.

Evidence for Immune Evasion in Lyme Disease
Biofilm-Like Aggregations
Sapi E, et al. Characterization of biofilm formation by Borrelia burgdorferi In Vitro. PLoS ONE;7(10):e48277.
Bb-induced effects included multilevel arrangements of alginates, calcium, and extracellular DNA, highly consistent with biofilm. Bb grown on agarose-coated mica discs. Imaged by atomic force microscopy, measurements made with Nanorule software.

Evidence for Persistent Infection in Lyme Disease
Definitive studies

Evidence for Persistent Infection in Lyme Disease
Barthold, 2010
..
....
..
..
..
..
....
Xenodiagnosis-Bb acquisition
by ticks-Bb transmission
by ticks-Bb survival through tick
life cycle
Allograft-transmissible Bb
RNA transcripts- showing
metabolicallyactive, viable Bb
Forms of proof given for
post-antibioticpersistence of
viable andinfective Bb in this study:

Evidence for Persistent Infection in Lyme Disease
Yrjanainen, 2010
..
..
..
..
..
..
Forms of proof given for
post-antibioticpersistence of
viable Bb in this study:
Culturefrom tissue samplesof mice treated withanti-TNFa 4 weeks
post antibiotictreatment

Evidence for Persistent Infection in Lyme Disease
Embers, 2012
..
....
..
..
Culture
Xenodiagnosisacquisitiontransmission
Immunofluorescence
PCR
C6 antibody
RNA transcripts
Bb antigen
Forms of proof given for
post-antibioticpersistence of
viable andinfective Bb in this study:

Conclusions
2. Bb exploits tick and host proteins, antigen masking and variation, elite motility skills, strategic niche-seeking, horizontal gene transfer, atypical forms, biofilm-like behavior, and antibiotic tolerance to help it persist within mammalian hosts.
1. Bb has an unusually adaptive combined genome that encodes for a powerful set of immune evasion capabilities.
3. In mice and primates, Bb subsets are proven to remain viable and infective despite culture negativity following antibiotic challenge.
4. Immune suppressed mice are more susceptible to the reactivation of viable Bb that persist despite antibiotic challenge.
5. Solid evidence supports the existence of persistent Lyme disease. Health care policy needs to accommodate efforts to prevent, detect, and treat it.

Added Sources of Complexity in Lyme Disease
Clinical Considerations

Sources of Added Complexity in Lyme Disease
Co-infections
AnaplasmosisGranulocytes WBCs, RBCs, plateletsElevated liver enzymesFever, chills, aches Headache, diarrhea
BabesiosisRed blood cellsFever, chills, sweatsHeadache, fatigueRing forms, Maltese crossHowell-Jolly bodies
EhrlichiosisMonocytesFever, chills, body achesConfusion, GI disturbanceHeadacheMorula (colony) forms
BartonellaRed blood cellsEndothelial cellsFever, rash, headacheFatigue, brain fogEndocarditis, sore soles
Borreliaburgdorferi (124 strains), afzellii, garinii (European forms)50+ symptoms reported, invasion of most tissues documented, primarily connective tissue, synovium, liver, testes, pelvic organs, central, peripheral, and autonomic nervous system cells, heart cells, and immune cells.
A new breed of polymicrobial, polyphasic infection?

Deer Tick Co-infection Rates
Assessment of polymicrobial infections in ticks in New York State. Vector Borne Zoonotic Diseases. 2010 Apr;10(3):217-221.
Among 286 Ixodes scapularis ticks collected in this study:
Borrelia Anaplasma Babesia Borrelia +Anaplasma
Borrelia +Babesia
Borrelia +Anaplasma+
Babesia
% positive ticks
182 (64%) 56 (20%) 58 (20%) 45 (16%) 48 (17%) 14 (5%)
Sources of Added Complexity in Lyme Disease

Sources of Added Complexity in Chronic Lyme Disease
Co-morbid Conditions in the Host
AutoimmuneDisease
DegenerativeDisease
PsychosocialStresses
Co-infections
Mood orCognitiveDisorders
MetabolicDisease
ChronicToxicity
AllergicSensitivities
Lyme

Sources of Added Complexity in Chronic Lyme Disease
Host Genetic VariationsThe influence of tumor necrosis factor alpha (TNFa) in Bb infection is well documented. There seems to be a polarity in host reactions, perhaps related to gene polymorphisms in TNFa or in promoter genes for the pro-inflammatory cytokines. This results in weaker or stronger cell-mediated immune responses.
In pathology studies of neurological Lyme disease, the following polarity is seen:
Infiltrative Atrophic
cerebral vasculitismulti-infarct
white matter lesionsinflammation
frontotemporal atrophydementia
hypoperfusionapoptosis
Miklossy J. Biology and neuropathology of dementia in syphilis and Lyme disease. In Handbook of Clinical Neurology, vol. 89, 2008, Elsevier: New York.

Sources of Added Complexity in Chronic Lyme Disease
The Limits of Diagnostic Testing
ILADS• Prefers higher sensitivity on Western Blot• Tolerates a higher false positive rate
• Prefers higher specificity on Western Blot• Tolerates a higher false negative rate
The search is on for biomarkers with better abilities to rule in (ILADS) and rule out (IDSA) cases of persistent Lyme and associated diseases.

Sources of Added Complexity in Chronic Lyme Disease
The Limits of Therapy
There is to date no known therapy for the post-Lyme residual autoimmune condition postulated by IDSA-aligned researchers.
ILADSNIH-sponsored clinical trials were underpowered and likely underestimate the benefits of antibiotic therapy in chronic Lyme patients. There is no surefire way of proving total eradication of viable Lyme spirochetes.
Guidelines for selecting therapies for patients with chronic Lyme continues to rest on a weak evidence base. For this reason, physicians should be allowed to select therapies based on pathophysiologic rationales supported by clinical experience and judgment, with decisions that reflect patient values and preferences.

Sources of Added Complexity in Chronic Lyme Disease
Patients Caught in the Crossfire
Given the lack of reliable biomarkers for use in monitoring responses to therapy for chronic Lyme disease, outcomes evaluation must rely on methods for assessing the subjective dimensions of the patient’s experience with therapy.
Physical Symptoms
Social
Mental
OverallFunction
Outlook ILADS
??
Who will help me?
The Rationalists The Empiricists
Finding reasonsto treat
Finding reasons not to treat

Dimensional Outcomes Assessments
• Quality of Life Score (SF-36)
• Fibromyalgia Impact Questionnaire (FIQ)
• Fatigue Severity Scale (FSS)
• Neurocognitive Dysfunction Index (NDI)
• McGill Pain Questionnaire (MPQ)
• Medical Outcome Scale (MOS)
Dimensional assessment tools used in NIH-funded chronic Lyme treatment studies:*
* Klempner, Krupp, and Fallon
• Review of Systems Scale (ROSS)
Visual analog scale for practice-based outcomes monitoring

• Evidence-based medicine 2.0
• Built to handle complexity
• Patient values respected
• Shared decision-making
• Clinical experience valued
• Empirical trials encouraged
• Dimensional outcome tracking
• Biopsychosocial awareness
• Systems theory and practiceA Systems Medicine Model
We Need a More Integrative
Medical Model

Repairing the Broken Bridge
Physicians must be allowed to use current evidence, experience, and clinical judgment to address the complexity of patients with tick-borne illness.
- Keith Berndtson, MD
All the bitterness of the debate does not serve the science or the patient...all the shouting drowns out the complexity and nuance of the work that needs to be done.
- Institute of Medicine Lyme Report, 2011

15 N. Prospect Park Ridge, IL 60068
847-232-9800www.parkridgemultimed.com
Patient-centeredsystems medicine.