lumbar disc prolapse clinical manifestation and localizatioin
39
CLINICAL MANIFESTATION, CLINICAL EVALUATION AND LOCALISATION OF PIVD By Dr Tejaswi Dussa PG In MS Ortho Gandhi Medical College Secunderabad
-
Upload
tejaswidussa -
Category
Education
-
view
473 -
download
3
description
Transcript of lumbar disc prolapse clinical manifestation and localizatioin

CLINICAL MANIFESTATION,CLINICAL EVALUATION AND LOCALISATION OF
PIVD
By Dr Tejaswi DussaPG In MS Ortho
Gandhi Medical CollegeSecunderabad

CLINICAL MANIFESTATIONS
1. Symptoms related to disc itself -discogenic pain2. Symptoms related to nerve root compression -root pain, radiculopathy3. Symptoms of myelopathy - Compression of spinal cord

• Cervicalgia - intermittent neck pain, medial scapular pain, shoulder pain
-compression of the sinuvertebral nerves and medial branches of the dorsal rami in the cervical region

• Disc compressing the nerve roots• Cervicalgia• Sensation of constriction around the trunk
(girdle pain)• Low back pain• Parasthesias• muscle weakness• sensory impairment

• Prolapse is large enough and causing central compression of spinal cord
- quadriplegia - paraplegia
- Anterior cord syndrome- conus medullaris syndrome- cauda equina syndrome
bladder disturbance dimnished perineal sensation

Hisrory &Spine Examination
• More common in middle aged group• Male > female• Onset of pain - acute - chronic• Site of pain• Sharp stabing /shooting pain• Radiation along the roots affected

• Trauma-Flexion type of injury• h/o evening rise of temp• h/o weight Loss • Look for deformities• Stiffness of back• other symptoms for gynaecological genito-urinary` vascular disease

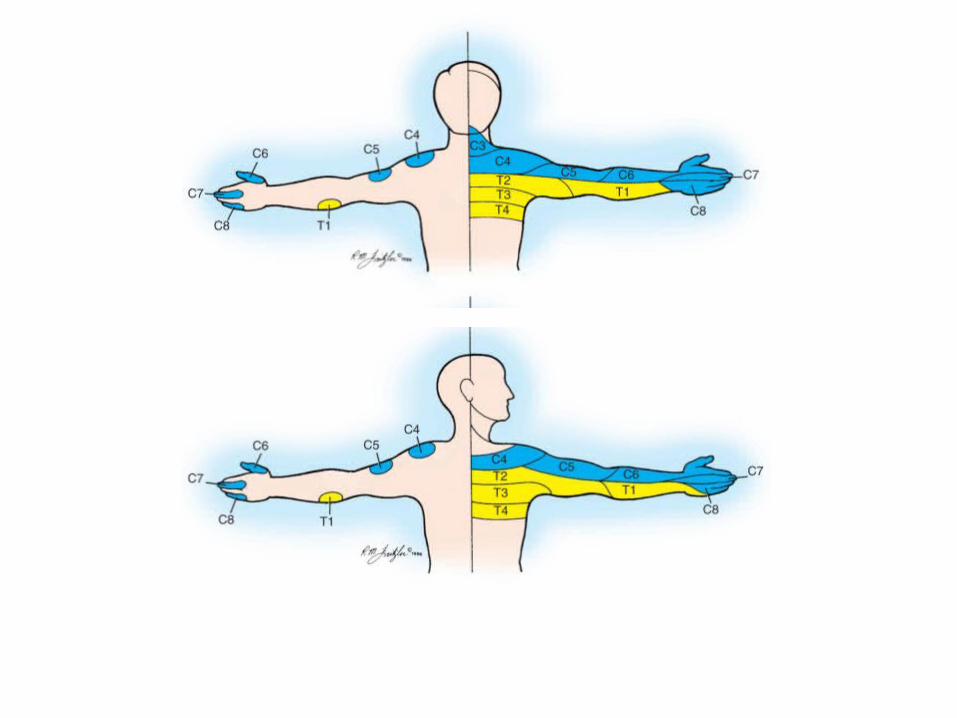
• Radiculopathy – pain radiating to thigh / leg / foot – root irritation
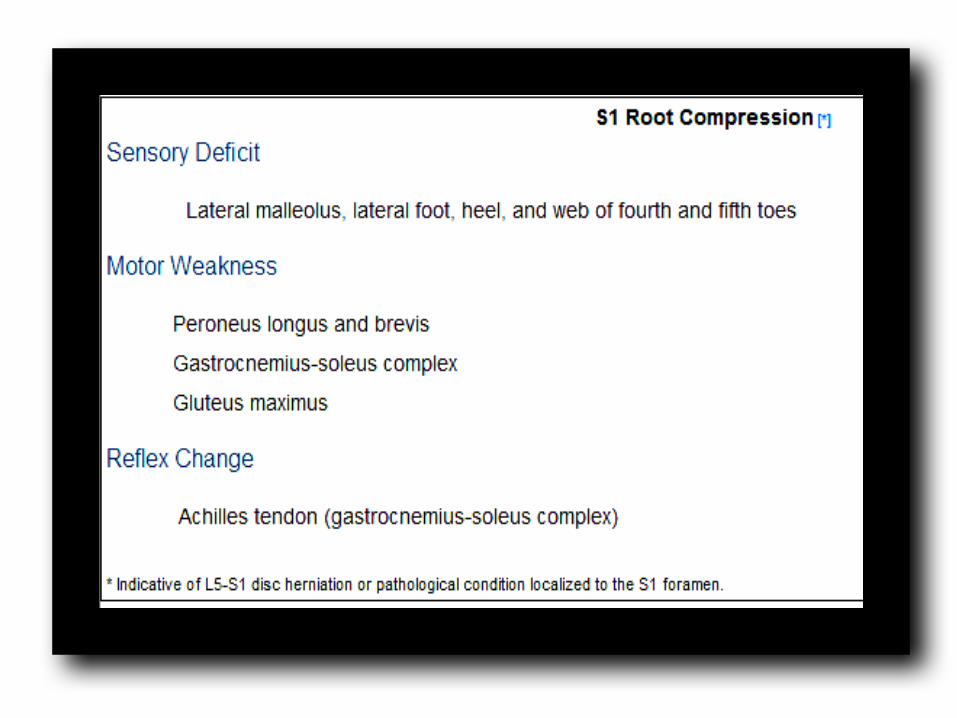
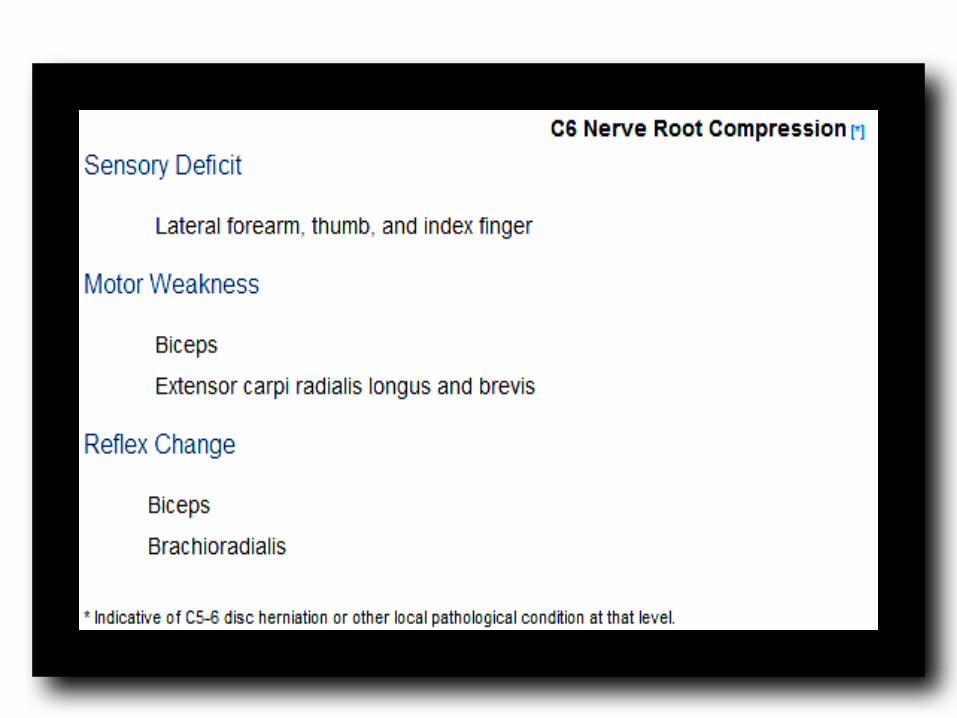
• Neurological deficits – root compression – motor, sensory, reflex
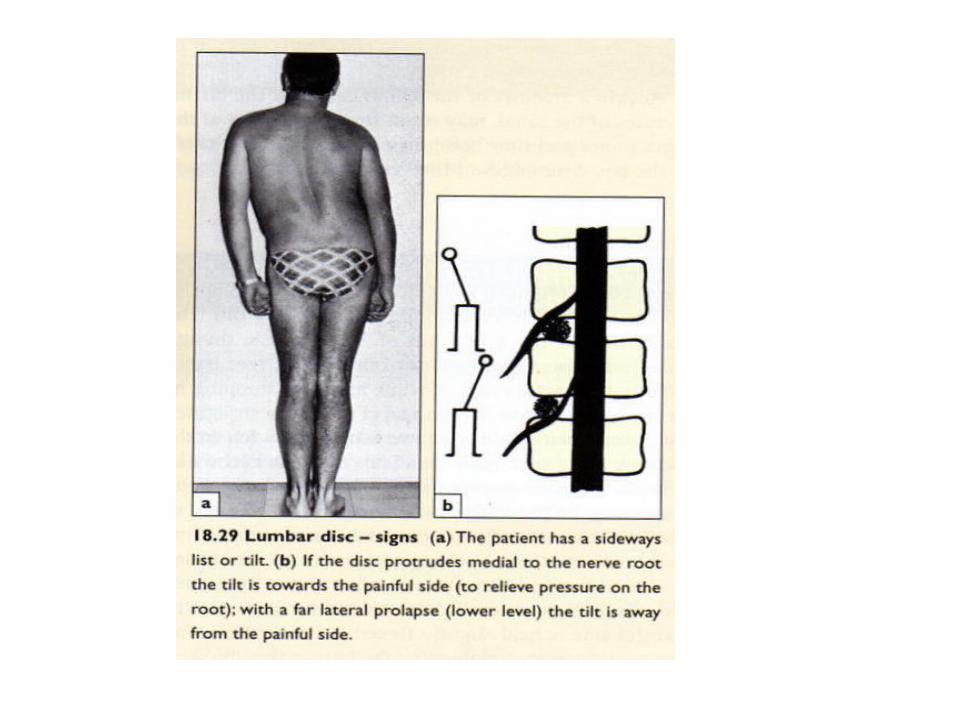
• Loss of lumbar lordosis• Scoliosis due to muscle spasm• Paraspinal muscle tenderness

• Low back ache – Typical H/O LBA relieved by rest – indicates degeneration of disc
• Sudden acute pain on lifting weight – H/O snapping sensation – acute PIVD-
Rupture of annulus• Pain increases on forward bending.



CLINICAL EVALUATION

• Special Tests: • Anvil test• Lhermitte’s test• Naffziger test• Valsalva test• Milgram test
Lumbar disc disease
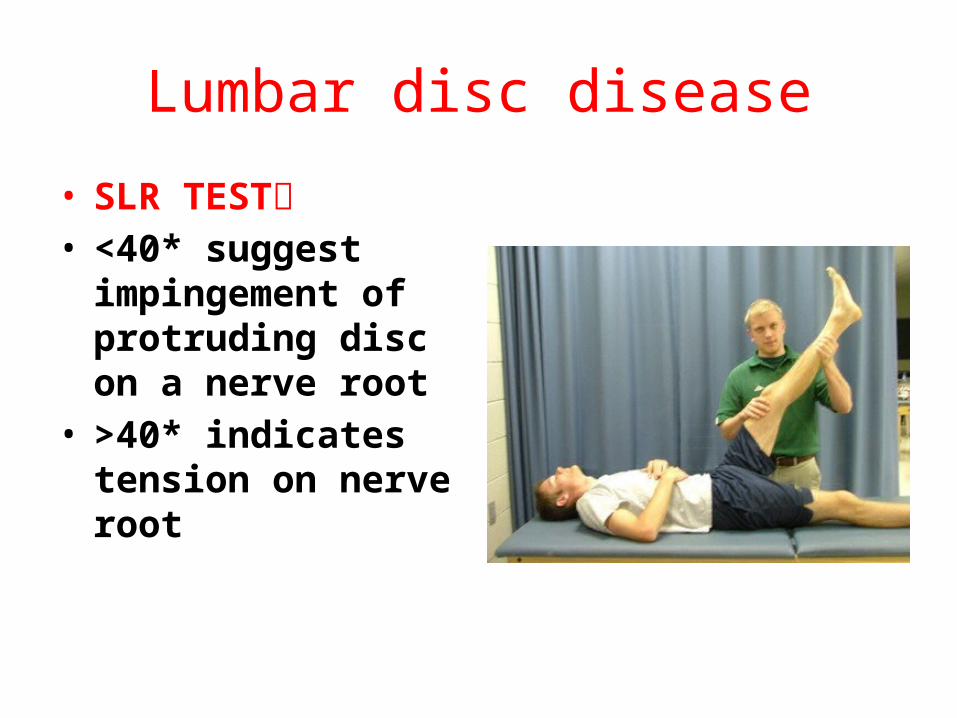
• SLR TEST• <40* suggest
impingement of protruding disc on a nerve root
• >40* indicates tension on nerve root

• LASEGUE’S TEST:• Used to differentiate sciatica from sacro iliac
joint disease

• Slump Test:• Sciatic pain• Impingement of
the dural lining, spinal cord, or nerve roots
• CROSSED SLR TEST:• Large disc prolapse close to midline

• BOWSTRING TEST:• -most reliable sign of nerve root compression
do SLR test At the point where the patient experiences pain, relax the tension by flexing the knee slightly; the pain should disappear. •Then apply firm pressure behind the lateral hamstrings to tighten the common peroneal nerve- the pain recurs in +ve test

• FEMORAL NERVE STRETCH TEST:•

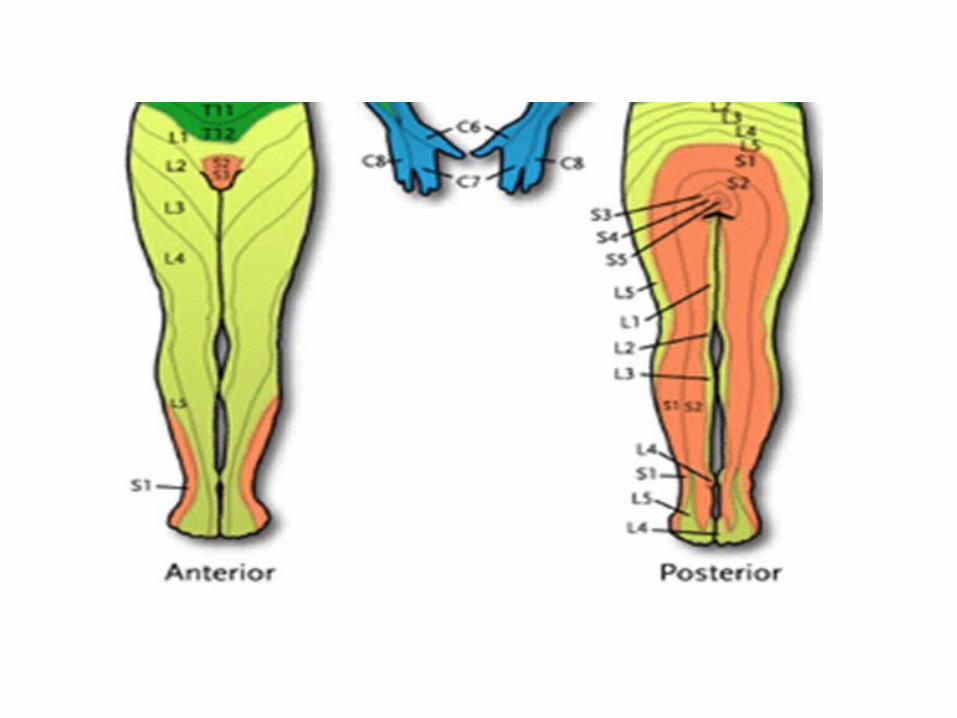
LOCALIZATION OF DISC PROLAPSE

• Spinal nerves C2-7 exit above the pedicle of respective vertebrae
- Eg:C6 nerve root exit the foramen between the C5 and C6
-The C8 nerve root exits the foramen between C7 and T1 pedicle
• All spinal nerves distal to C8 exit the foramen below the pedicle for which they are named
- Eg:L4 nerve root exits the foramen between the L4 and L5 pedicle
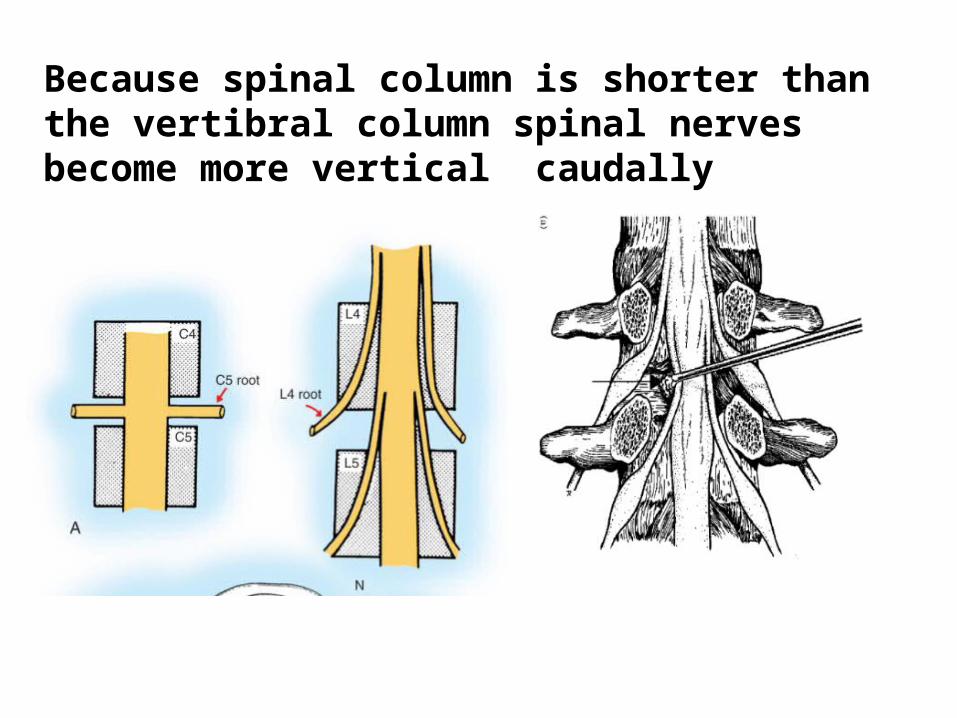
Because spinal column is shorter than the vertibral column spinal nerves become more vertical caudally




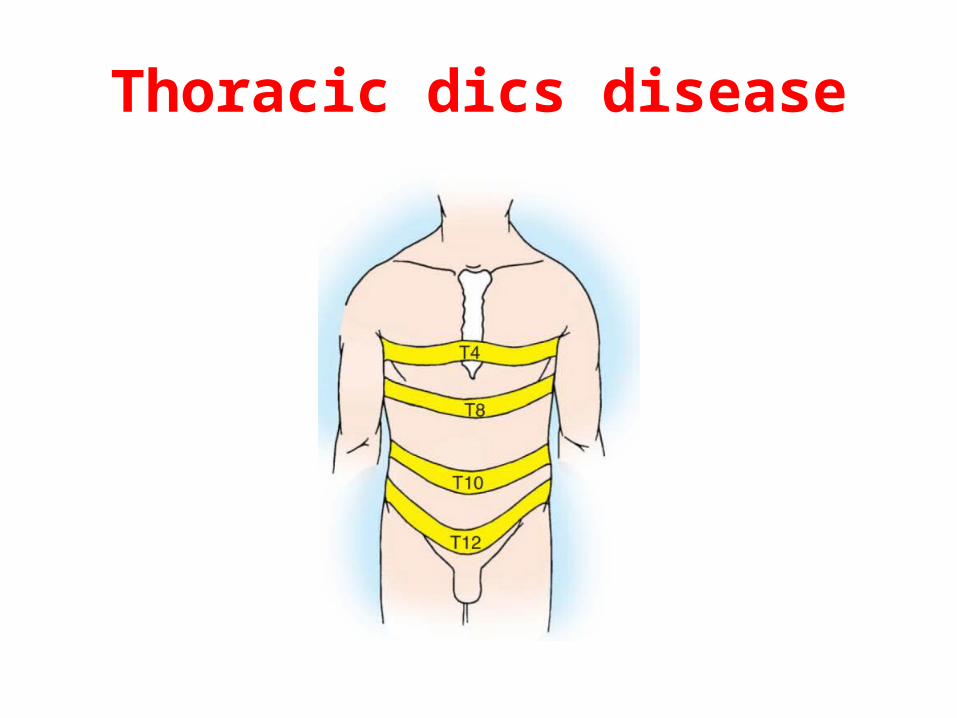
Thoracic dics disease

• Ex:Abdominal musculature:• Pt attempt to lift his head up from the pillow
against the resistance• paralysed lower segment moves upwards• when the upper segment paralysed the
umbilicus moves downwards (Beevor’s sign)

Lumbar disc disease
• Motor testing nerve Root Level
• L1 Hip flexion• L2 Hip flexion• L3 Knee extension• L4 Dorsiflexion ankle• L5 Great toe extension• S1 Plantarflexion