
Lorne Community Hospital Service Plan Discussion Paper ... · PDF fileLorne Community Hospital...
18
1 Lorne Community Hospital Service Plan Discussion Paper – March 2011 Lorne Community Hospital is seeking the development of a service plan to guide the development of its services over the next five to ten years. This paper provides a basis for discussion with selected key stakeholders in relation to the important issues that are likely to impact on the service profile of Lorne Community Hospital both now and into the future. The identified issues are not intended to be extensive but intended to be ‘thought starters’ and act as prompts for considered discussion on this future direction. There is no expectation that stakeholders will address all the questions in the paper, different questions will resonate with different stakeholders. There will be other matters that are important to different stakeholders that should be raised in the context of the development of this report. Part of the paper provides background information as an overview to the current service profile, configuration and important demographic data that will help inform the service plan. In addition to the meetings being conducted by the consultants, written comments will be most welcome. Written comments may be submitted to either: Janelle Bryce CEO Lorne Community Hospital Albert Street, Lorne, 3232 [email protected] OR Amanda Singleton Inside Health Management 85 Vine Street, Moonee Ponds, 3039 [email protected] Verbal feedback is also encouraged and can be made by contacting Janelle Bryce, CEO, on 03-52894310 (direct) during business hours.
Transcript of Lorne Community Hospital Service Plan Discussion Paper ... · PDF fileLorne Community Hospital...
1
Lorne Community Hospital
Service Plan
Discussion Paper – March 2011
Lorne Community Hospital is seeking the development of a service plan to guide the development of its services over the next five to ten years.
This paper provides a basis for discussion with selected key stakeholders in relation to the important issues that are likely to impact on the service profile of Lorne Community Hospital both now and into the future. The identified issues are not intended to be extensive but intended to be ‘thought starters’ and act as prompts for considered discussion on this future direction. There is no expectation that stakeholders will address all the questions in the paper, different questions will resonate with different stakeholders. There will be other matters that are important to different stakeholders that should be raised in the context of the development of this report.
Part of the paper provides background information as an overview to the current service profile, configuration and important demographic data that will help inform the service plan.
In addition to the meetings being conducted by the consultants, written comments will be most welcome. Written comments may be submitted to either:
Janelle Bryce CEO Lorne Community Hospital Albert Street, Lorne, 3232 [email protected] OR Amanda Singleton Inside Health Management 85 Vine Street, Moonee Ponds, 3039 [email protected]
Verbal feedback is also encouraged and can be made by contacting Janelle Bryce, CEO, on 03-52894310 (direct) during business hours.
2
1. Background information
Lorne Community Hospital (LCH) is a public hospital under the Health Services Act. It receives funding as a Small Rural Health Service. It provides acute, residential and primary care services for Lorne and the surrounding areas.
There is a one medical practice that provides the medical input into the residential aged care and acute services.
1.1. Population profile
The estimated resident population of the Lorne area based on the 2006 census was 967. This was 10.7 % of the overall population of 9004 in the Surf Coast (West) SLA. Due to the nature of the tourist population, the number of persons staying in Lorne at any time can vary quite significantly depending on the season.
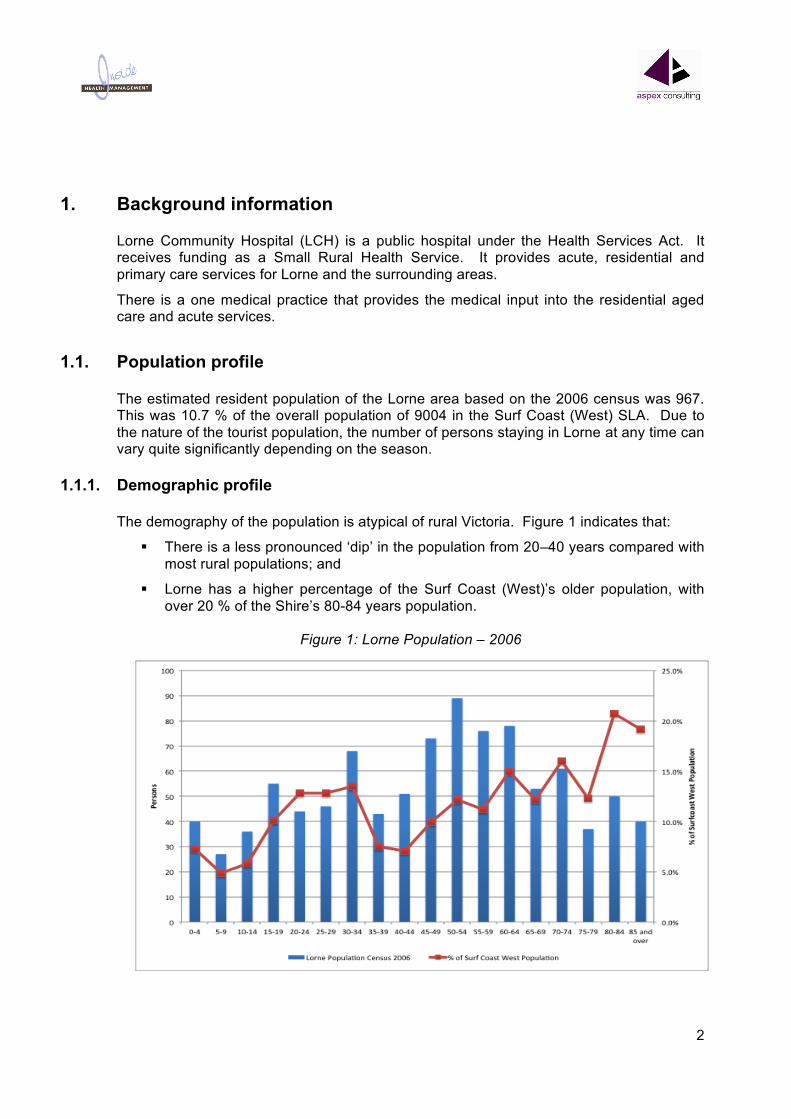
1.1.1. Demographic profile
The demography of the population is atypical of rural Victoria. Figure 1 indicates that:
There is a less pronounced ‘dip’ in the population from 20–40 years compared with most rural populations; and
Lorne has a higher percentage of the Surf Coast (West)’s older population, with over 20 % of the Shire’s 80-84 years population.
Figure 1: Lorne Population – 2006
3
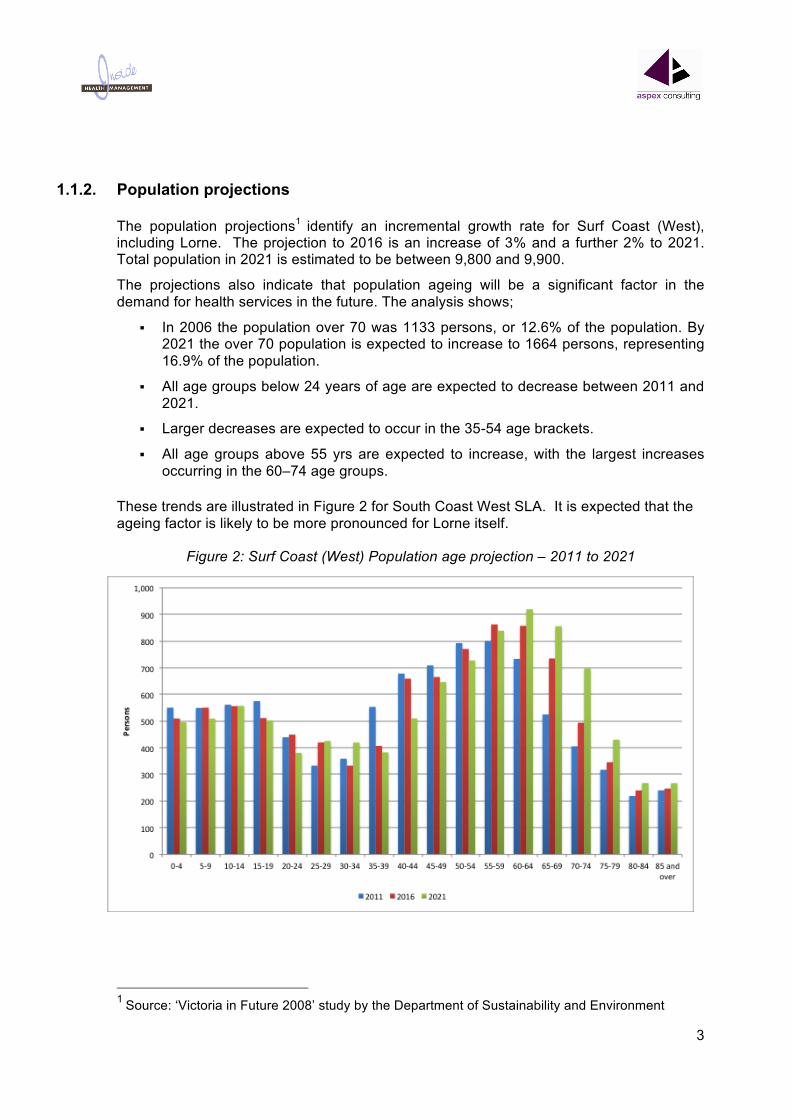
1.1.2. Population projections
The population projections1 identify an incremental growth rate for Surf Coast (West), including Lorne. The projection to 2016 is an increase of 3% and a further 2% to 2021. Total population in 2021 is estimated to be between 9,800 and 9,900.
The projections also indicate that population ageing will be a significant factor in the demand for health services in the future. The analysis shows;
In 2006 the population over 70 was 1133 persons, or 12.6% of the population. By 2021 the over 70 population is expected to increase to 1664 persons, representing 16.9% of the population.
All age groups below 24 years of age are expected to decrease between 2011 and 2021.
Larger decreases are expected to occur in the 35-54 age brackets.
All age groups above 55 yrs are expected to increase, with the largest increases occurring in the 60–74 age groups.
These trends are illustrated in Figure 2 for South Coast West SLA. It is expected that the ageing factor is likely to be more pronounced for Lorne itself.
Figure 2: Surf Coast (West) Population age projection – 2011 to 2021
1 Source: ‘Victoria in Future 2008’ study by the Department of Sustainability and Environment

4
Figure 3 demonstrates the population distribution expected from 2011 – 2021, showing the changes by age group.
Figure 3: Surf Coast (West) Population age distribution changes – 20011 to 2021
1.2. Catchment Lorne Community Hospital is located in the coastal town of Lorne in Victoria’s south west. The town of Lorne lies between Aireys Inlet (19km north east) and Apollo Bay (44km south west). The town is nestled between the coast and the Otway ranges, meaning road access is limited to the coastal Great Ocean Road and the road travelling north through the Otway Ranges to Deans Marsh. Lorne Community Hospital forms part of the Barwon South West health region, and is situated 67km from the regional referral hospital at Geelong, with metropolitan Melbourne a further 80km north east.

5
Figure 4: Nominal Catchment
1.2.1. Nominal and refined catchment
Lorne Community Hospital nominally serves a permanent catchment population of approximately 2,500 if Aireys Inlet is included. Lorne has a seasonal fluctuation of up to 35,000 population. There a significant number of persons over 50 years represented within the permanent and seasonal populations
For the purpose of this Service Plan, the primary catchment may be more appropriately defined as Lorne and surrounds. The primary catchment is based on the geographic spread of actual Lorne Community Hospital’s acute patient profile. A secondary catchment exists in the rural areas surrounding Lorne itself and in the communities nearby along the Great Ocean Road.
6
2. Areas for consideration in service planning
2.1. Role and strategic direction
It is important that all health services understand their role within the health system. The strategic direction and vision for Lorne Community Hospital over the next five to ten years needs to be established in the context of the broader government policy direction.
Lorne Community Hospital is the designated local health care provider for the Lorne catchment. It refers patients to sub-regional and regional health care providers, such as Barwon Health, Geelong or Colac Area Health for patients requiring a level of clinical care or support that they are unable to provide.
What should be the priority areas at Lorne Community Hospital over the coming years?
What is Lorne Community Hospital’s core role in the delivery of health care?
What is the appropriate catchment area of Lorne Community Hospital?
How does/should Lorne Community Hospital relate to other health services in the sub-region such as Barwon Health and Colac Area Health?
What are the important ‘interface’ issues with other health care providers for Lorne Community Hospital in undertaking its role?
What are the core services, or priority areas for Lorne Community Hospital? What are the gaps that need to be addressed?
Are the demographics and socio-economic factors key drivers of service need in the future? How are they reflected in service demand?
Are there other key factors that impact on service demand?
Are there other changes anticipated in Lorne Community Hospital ‘s catchment that may significantly impact on the capacity of Lorne Community Hospital to fulfill its role?
Is Lorne Community Hospital’s strategic direction consistent with policy?
How will technology changes impact on the service profile at Lorne Community Hospital?
What is an appropriate level of self-sufficiency for Lorne Community Hospital? How does this compare with similar organisations and show should this be factored into future service planning?
Is the disease profile a key driver of future service need? Why/Why not?

7
2.2. Acute services
Lorne Community Hospital has six acute beds and a 24-hour urgent care service. There is also a two-chair renal dialysis service that has no permanent clients (currently). Dialysis is essentially a holiday service.
Lorne Community Hospital acute activity indicates:
There were 183 separations2 excluding dialysis recorded in 2009/10, an increase of 11% compared to the previous year and following a 22% decrease in 2007/08.
An additional 210 renal dialysis separations were recorded in 2009/10. Renal activity has fallen from a high of 417 in 2007/08.
Increase in multi-day separations from 2005/06 – 2009/10 and a reduction in same day separations.
81% of separations in 2009/10 were for public patients. Private patients accounted for 7.7% of separations in 2009/10 up from 3.4% in 2005/06.
77% of separations in 2009/10 were classified as emergency with 22.4% planned. This compares to 85% planned and 15% emergency in 2005/06, with close to a 50/50 split in 2007/08 and 2008/09. The variation reflects changes in clinical practice.
There is an increase in separations during peak holiday season, particularly January generally these are non-residents.
There was a 5% decrease in urgent care presentations3 in 2009/10. 2085 presentations were recorded. The triage mix has seen a decrease in category 5 presentation, with a corresponding increase in category 3 and 4.
See Appendix A for a more detailed analysis.
What are the key priorities for development of acute services over the next five years?
Are there any services that are “over-provided”? Could these be delivered in a different way?
What is Lorne Community Hospital’s future role in relation to bed based services in the future?
Is the renal dialysis service a high priority service?
What is the potential for Lorne Community Hospital to work with other health care providers in different ways to meet increasing/changing demand?
2 Separations: the term given for discharges from a health service (discharges include deaths and transfers of admitted acute patients to other health services) 3 No. of patients attending the urgent care

8
Do the medical imaging, pharmacy and pathology services provide the necessary range of modalities and support for Lorne Community Hospital acute and urgent care activity?
2.3. Primary health & community care
Generally community-based services have developed in an ad hoc manner over many years in response to service demand, funding opportunities and policy directions. These services have historically been seen as peripheral to bed-based services but with an increasing emphasis on substitution and diversion away from bed based services there will be opportunities for service development and enhancement in the delivery of community based services.
With the increasing expectations that will be placed on community-based services over the next five years in response to policy and changing models of care, the strategies developed in this area will be important to meet service demand.
Within this context, Lorne Community Hospital, together with the Surf Coast Shire could potentially play a more significant role in the access and coordination of the primary care and community health services for the community of Lorne. The role of these community-based services is both restorative and preventative; it substitutes for hospital admissions and enables access to health care services that consumers may not otherwise receive.
What is Lorne Community Hospital’s role in relation primary and community based care services?
Are there sufficient and appropriate community based services in Lorne? If not, what are the gaps?
How can community-based services be delivered more effectively to reduce demand on other services?
What is the role of Lorne Community Hospital’s in health promotion, early intervention and care for more complex patients related to inpatient services?
Are community based service coping with demand?
Are community based services well integrated with other health service providers, including GPs? Is there service duplication? Are there opportunities for more effective integration and collaboration of services?
How does Lorne Community Hospital interface with other community-based services in surrounding towns?
9
2.4. Residential aged care 9Lorne Nursing Home)
Residential aged care is a core service for Lorne Community Hospital. Lorne Community Hospital operates a 19 bed high care facility in additional to one respite bed. The residential aged care service is the single largest service stream provided by Lorne Community Hospital.
However, the residential aged care sector is changing significantly with demand for residential low care services reducing as home based packages become more attractive. This means people are choosing to enter residential care later. Residents therefore enter with more complex needs, requiring palliation and often experiencing quite short lengths of stay. In addition, there have been changes to the funding model in the last two years with other bodies of work suggesting that there may be further changes by the Commonwealth Government. Similar to many small rural health services, Lorne Community Hospital is experiencing some difficulties with the financial viability of the residential aged care.
The main issues for residential aged care include:
Resident dependency levels against the new funding regime; and
Decreasing occupancy rates only over relatively recent time (relating to declining demand), notwithstanding the increasing ageing of the catchment population.
This service plan will also examine the financial performance of the health service, including residential aged care funding. The financial analysis is underway but yet to be completed.
How does the residential aged service fit with the future role and strategic objectives of Lorne Community Hospital?
Does there need to be a re-balancing between bed-based and community based residential aged care service?
Should there be an expansion, maintenance or contraction of residential aged care service capacity? Why?
Does Lorne Community Hospital have an appropriate business model to sustain the service? What needs to change?
2.5. Model of care
The model of care essentially describes how services are delivered in order to provide care to the right people at the right time with the right set of skills.
What are the models of care that Lorne Community Hospital should explore in areas including acute inpatient, non-admitted patient services, aged care and community-based services?
To what extent is the model of care being influenced by outside factors? What are these factors?
10
Is the trend toward delivering more services in a community setting the right model for Lorne Community Hospital? If so, how should this be undertaken?
Are there practices that inhibit better patient outcomes, patient access, timely care/treatment, and/or operational efficiencies? Explain.
Are service risks adequately managed through the current means of delivering care?
Are patients receiving effective continuum of care, or are there barriers which are due to the involvement of different service providers?
2.6. Clinical governance and service quality
Health Services together with the Department of Health and the community demand the provision of consistent high quality services. There are systems in place to ensure that Lorne Community Hospital is monitoring their performance and being measured against an acceptable set of standards. Lorne Community Hospital holds nationally accredited status with the Australian Council of Healthcare Standards (ACHS) Equip 4 and with the Aged Care Standards and Accreditation Agency. Despite the cost associated with accreditation there is an ongoing commitment from the Board and the executive to maintain this process throughout the organisation.
In addition, the level of safety within an organisation can be directly dependent on the skills and capability of the staff that work in it and the resources available to them.
How is quality of service delivery measured at Lorne Community Hospital?
Are there effective measures in place to demonstrate that a high quality service is actually being delivered?
Do the clinical support and corporate support services have a strong ‘customer’ orientation?
Is there a strong ‘customer’ approach at Lorne Community Hospital? Does the culture of the organisation, unit, or department enhance or inhibit service quality?
What risk management system is in place? Is there also an active risk mitigation approach to the identified high-risk areas?
Are the risk mitigations systems and processes effective? If not, what are the barriers to more effective systems?
11
2.7. Partnerships and alliances
Consistent with policy directions at both the State and Commonwealth levels, partnerships and alliances by Lorne Community Hospital will be an important component in delivering services more effectively to patients in the catchment.
Who are Lorne Community Hospital main partnerships and alliances?
Are there any existing problems with current partnerships/arrangements?
Are there successful partnerships or alliances? If so, what are the main ‘ingredients’ of successful partnerships?
Do any of the current partnerships and alliances need to be modified? Why/Why not?
What are the partnerships and alliances that need to be developed in the future? Why?
2.8. Workforce
The workforce is one of the most critical components in delivering of health care in general. Notwithstanding the critical nature of an adequate and skilled workforce, there are unambiguous signs of future shortages.
What are likely to be the most pressing areas of skill shortage that should be considered in the development of this plan?
What is currently being done to address these issues?
What initiatives does Lorne Community Hospital have in place to support local development of staff?
What is the availability for the local teaching of a prospective workforce? What alliances and relationships are in place or need to be developed?
2.9. Infrastructure development
It is important to ensure that facilities and equipment available at Lorne Community Hospital match the requirements of current and future service developments.
What are the areas of infrastructure that most inhibit the effective delivery of services, or lead to inefficiency?
What physical or capital infrastructure is the most urgent for over the next five years?

12
What are the most pressing information technology issues confronting the region to provide services?
Is infrastructure in some way impeding service development?
13
Appendix A: Service Profile Summary
Acute Lorne Community Hospital has 6 acute beds and a 24-hour urgent care service. There is a renal dialysis service that has no permanent clients (currently) providing essentially a holiday service.
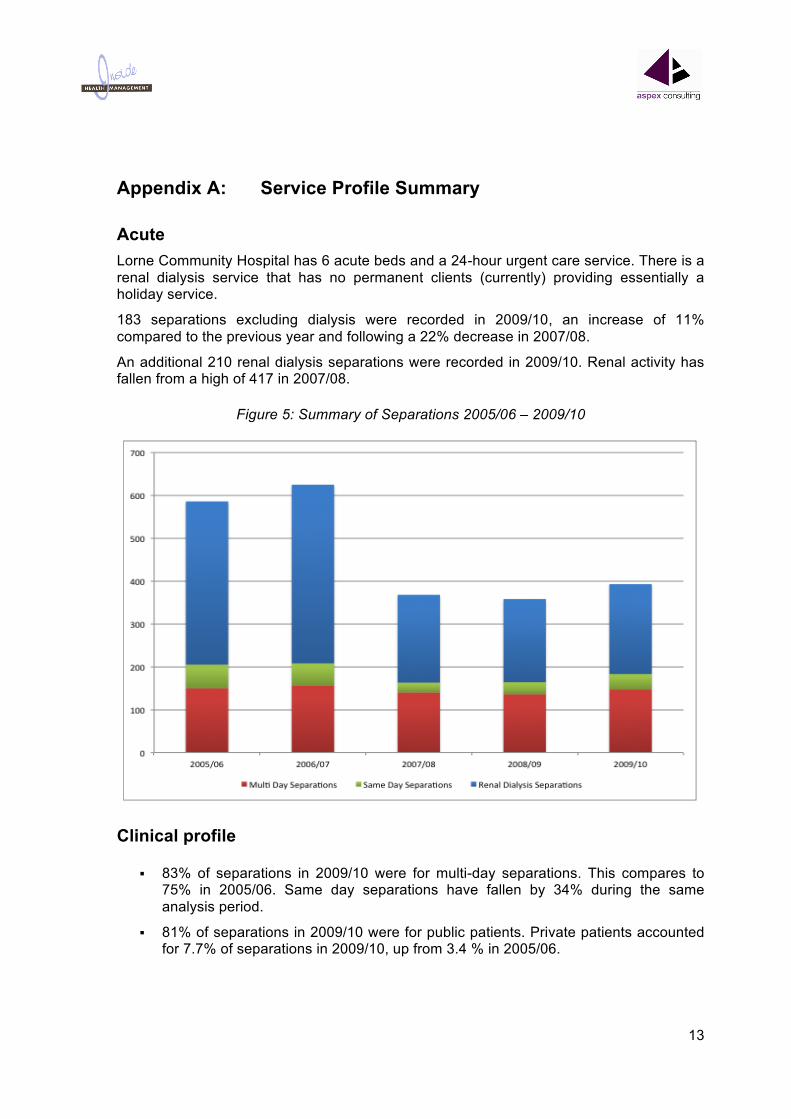
183 separations excluding dialysis were recorded in 2009/10, an increase of 11% compared to the previous year and following a 22% decrease in 2007/08.
An additional 210 renal dialysis separations were recorded in 2009/10. Renal activity has fallen from a high of 417 in 2007/08.
Figure 5: Summary of Separations 2005/06 – 2009/10
Clinical profile
83% of separations in 2009/10 were for multi-day separations. This compares to 75% in 2005/06. Same day separations have fallen by 34% during the same analysis period.
81% of separations in 2009/10 were for public patients. Private patients accounted for 7.7% of separations in 2009/10, up from 3.4 % in 2005/06.

14
77% of separations in 2009/10 were classified as emergency, with 22% planned. This compares to 85% planned and 15% emergency in 2005/06, with close to a 50/50 split in 2007/08 and 2008/09.
Figure 6: Bed day activity
In addition to the change in the bed day profile of the hospital there has been subsequent change in the length of stay.
Figure 7: Length of stay
15
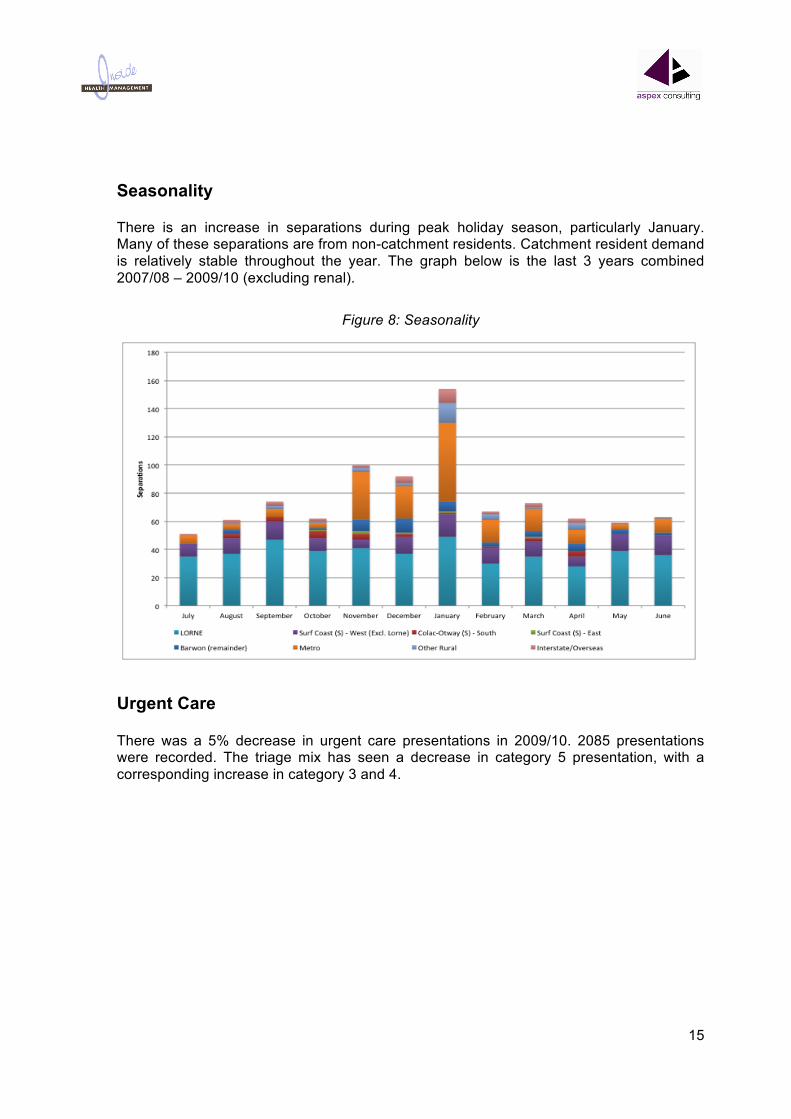
Seasonality
There is an increase in separations during peak holiday season, particularly January. Many of these separations are from non-catchment residents. Catchment resident demand is relatively stable throughout the year. The graph below is the last 3 years combined 2007/08 – 2009/10 (excluding renal).
Figure 8: Seasonality
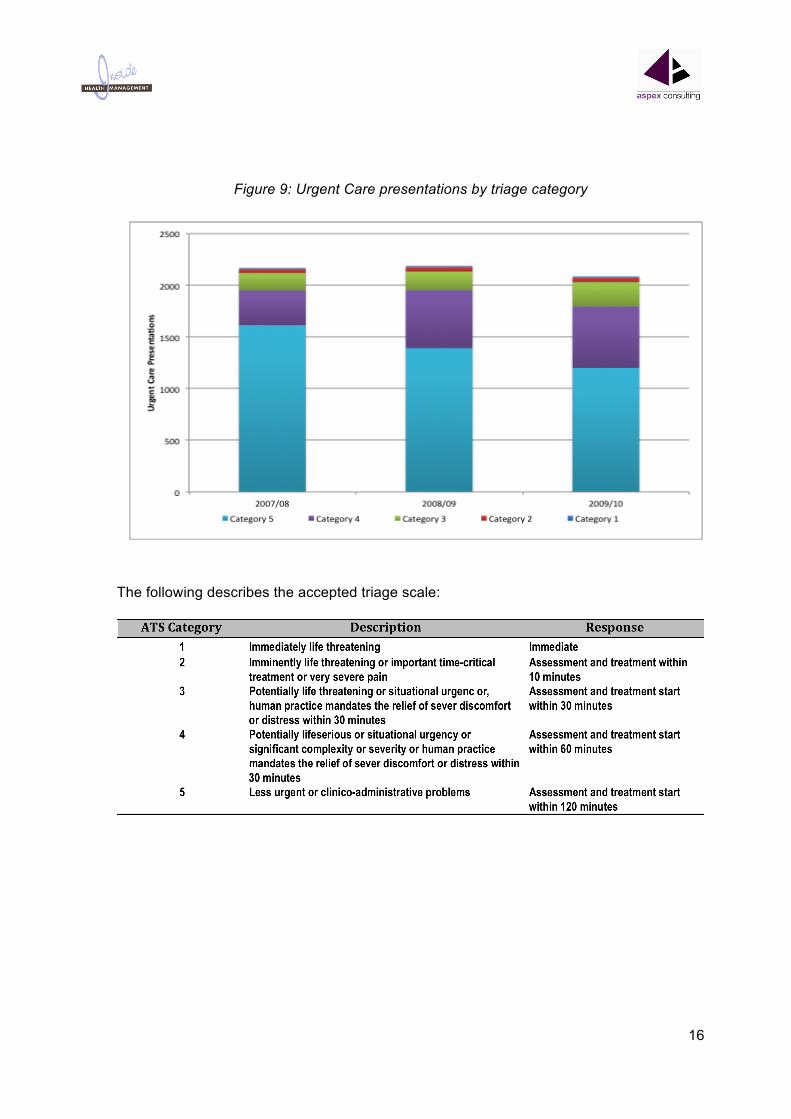
Urgent Care
There was a 5% decrease in urgent care presentations in 2009/10. 2085 presentations were recorded. The triage mix has seen a decrease in category 5 presentation, with a corresponding increase in category 3 and 4.
16
Figure 9: Urgent Care presentations by triage category
The following describes the accepted triage scale:

17
Residential aged care The activity analysis of the residential aged care services is summarised below.
Occupancy by month in terms of bed days and percentages is shown in Figure . Occupancy for the first 5 months of FY 11 is 89.6% compared with 98.7% in FY 10 and 91.4% in FY 09.
Figure 10: Bed days x month – July 08 to Nov 10
In FY 09, occupancy was only 84% in the first half compared with 98.7% in the second half of the year. The FY 09 occupancy pattern was not repeated in FY 10, which recorded 99% in the first half and 98.7% in the second half. The first half of FY 11 however is trending more like FY 09 with occupancy falling to 89.6 % after the first 5 months.
Details of the number of individual residents and the duration of their stay in each period are shown in Table .
Table 1: Residents and LOS – FY 09 to FY 11
LOS FY 09 FY 10 LOS FY 11
No. No. No.365 12 8 153 10300‐364 1 5 124‐152 3240‐299 2 1 93‐123 4180‐239 4 5 63‐92 2120‐179 1 4 32‐62 260‐119 0 2 0‐31 10‐59 4 3
Total 24 28 22
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
250
300
350
400
450
500
550
600
650
Jul‐0
8Au
g‐08
Sep‐08
Oct‐08
Nov‐08
Dec‐08
Jan‐09
Feb‐09
Mar‐09
Apr‐09
May‐09
Jun‐09
Jul‐0
9Au
g‐09
Sep‐09
Oct‐09
Nov‐09
Dec‐09
Jan‐10
Feb‐10
Mar‐10
Apr‐10
May‐10
Jun‐10
Jul‐1
0Au
g‐10
Sep‐10
Oct‐10
Nov‐10
Bed Days Occupancy %
18
Occupancy was higher in FY 10 than FY 09 despite a higher turnover of residents in that year which indicates that vacancies were filled promptly. During FY 10, there were 9 new residents and 13 departures.
A total of 15 residents has carried forward from FY 10 into FY 11 however, 5 of these residents have departed in the first 5 months of FY 11. There have been 7 new admissions in FY 11 but the lower occupancy in FY 11 suggests that there have been longer vacancies compared to FY 10.


















