Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm...
6
Original Article Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants Jacqueline Bauer a, * , Joachim Gerss b a University Children’s Hospital of Muenster, Department of Pediatrics, Albert-SchweitzerStr. 33, D-48149 Muenster, Germany b Department of Medical Informatics and Biomathematics, University of Muenster, Germany article info Article history: Received 27 January 2010 Accepted 7 August 2010 Keywords: Human milk composition Analysis Preterm infant summary Background & aims: The primary objective of this study was to investigate the composition of breast milk of mothers with extremely preterm infants (<28 weeks) for their nutrient content over the first 8 weeks of lactation, and to compare premature to term milk. Methods: Breast milk from 102 mothers who had delivered preterm infants and from 10 mothers who had delivered term infants were collected longitudinally. Fat, protein, carbohydrate, minerals and energy content were estimated weekly in each participant. Milk samples were representative of complete 24-h cycles. Results: Carbohydrate, fat and energy concentrations were significantly higher in preterm than in term milk (p < 0.05). Protein content of both preterm and term milk decreased with the progress of lactation demonstrating significantly higher values in extremely preterm milk (<28 weeks) than in moderately preterm and term milk (p < 0.0001). The sodium levels of preterm milk were significantly elevated (p < 0.05) only in the first week. Other changes in mineral content were detected neither in preterm nor term milk. Conclusions: Our data provide new information on the macronutrient content of milk in mothers of extremely preterm infants with possible implications for the nutrition of this population. Ó 2010 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved. 1. Introduction Introduction of therapeutic measures such as surfactant replacement and antenatal steroid administration have led to dramatically improved survival rates of premature infants. There- fore, recent research focus has shifted towards factors influencing long-term outcome. Adequate nutritional supply during the first weeks of life has a major impact on neurodevelopment in prema- ture infants. 1,2 The appropriate nutrition for term neonates during the first 4e6 months of life is universally considered to be their own mother’s milk. Human milk provides not only the substrates needed for growth but also a large number of bioactive components that modulate neonatal development. 2 The provision of human milk to premature neonates has demonstrated many beneficial effects including improvements in host defense digestion, absorp- tion of nutrients, gastrointestinal function, neurodevelopment, and psychological effects for the mother. 1,2 Feeding of mother’s milk to rapidly growing preterm infants, especially those who are extremely premature with a gestational age below 28 weeks, often results in suboptimal weight gain and nutritional deficits, due to premature infants need for large amounts of protein and energy to achieve appropriate growth. 3,4 Additionally, inadequate substrate provision is associated with delays in long-term growth and in neurodevelopmental outcome until at least school age. 1,2 Recent investigations on the effect of early postnatal nutrition indicate that the rate of weight gain in premature infants is influenced by the quantity of calories given. Gains in length and head circumferences on the other hand are affected by the amount of protein in the diet. 4 Therefore, information about precise protein and energy contents of each individual mother’s milk are highly desirable when feeding premature infants. Studies focusing on the macronutrient content of human milk fractions from mothers of extremely immature neonates are scarce and often cross-sectional. 5,6 Various reports have revealed that protein concentrations of both preterm and term human milk decline through lactation, whereas the contents of fat, lactose and carbohydrate show no significant changes over time. 5,6 In addition, considerable inter- and intra-individual variations have been detected in the course of lactation. 5,6 In extremely premature * Corresponding author. Tel.: þ49 251 8347810. E-mail address: [email protected] (J. Bauer). Contents lists available at ScienceDirect Clinical Nutrition journal homepage: http://www.elsevier.com/locate/clnu 0261-5614/$ e see front matter Ó 2010 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved. doi:10.1016/j.clnu.2010.08.003 Clinical Nutrition 30 (2011) 215e220
-
Upload
jacqueline-bauer -
Category
Documents
-
view
219 -
download
0
Transcript of Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm...

lable at ScienceDirect
Clinical Nutrition 30 (2011) 215e220
Contents lists avai
Clinical Nutrition
journal homepage: ht tp: / /www.elsevier .com/locate/c lnu
Original Article
Longitudinal analysis of macronutrients and minerals in human milk producedby mothers of preterm infants
Jacqueline Bauer a,*, Joachim Gerss b
aUniversity Children’s Hospital of Muenster, Department of Pediatrics, Albert-SchweitzerStr. 33, D-48149 Muenster, GermanybDepartment of Medical Informatics and Biomathematics, University of Muenster, Germany
a r t i c l e i n f o
Article history:Received 27 January 2010Accepted 7 August 2010
Keywords:Human milk compositionAnalysisPreterm infant
* Corresponding author. Tel.: þ49 251 8347810.E-mail address: [email protected]
0261-5614/$ e see front matter � 2010 Elsevier Ltd adoi:10.1016/j.clnu.2010.08.003
s u m m a r y
Background & aims: The primary objective of this study was to investigate the composition of breast milkof mothers with extremely preterm infants (<28 weeks) for their nutrient content over the first 8 weeksof lactation, and to compare premature to term milk.Methods: Breast milk from 102 mothers who had delivered preterm infants and from 10 mothers whohad delivered term infants were collected longitudinally. Fat, protein, carbohydrate, minerals and energycontent were estimated weekly in each participant. Milk samples were representative of complete 24-hcycles.Results: Carbohydrate, fat and energy concentrations were significantly higher in preterm than in termmilk (p < 0.05). Protein content of both preterm and term milk decreased with the progress of lactationdemonstrating significantly higher values in extremely preterm milk (<28 weeks) than in moderatelypreterm and term milk (p < 0.0001). The sodium levels of preterm milk were significantly elevated(p < 0.05) only in the first week. Other changes in mineral content were detected neither in preterm norterm milk.Conclusions: Our data provide new information on the macronutrient content of milk in mothers ofextremely preterm infants with possible implications for the nutrition of this population.
� 2010 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved.
1. Introduction
Introduction of therapeutic measures such as surfactantreplacement and antenatal steroid administration have led todramatically improved survival rates of premature infants. There-fore, recent research focus has shifted towards factors influencinglong-term outcome. Adequate nutritional supply during the firstweeks of life has a major impact on neurodevelopment in prema-ture infants.1,2 The appropriate nutrition for term neonates duringthe first 4e6months of life is universally considered to be their ownmother’s milk. Human milk provides not only the substratesneeded for growth but also a large number of bioactive componentsthat modulate neonatal development.2 The provision of humanmilk to premature neonates has demonstrated many beneficialeffects including improvements in host defense digestion, absorp-tion of nutrients, gastrointestinal function, neurodevelopment, andpsychological effects for the mother.1,2 Feeding of mother’s milk to
(J. Bauer).
nd European Society for Clinical N
rapidly growing preterm infants, especially those who areextremely premature with a gestational age below 28 weeks, oftenresults in suboptimal weight gain and nutritional deficits, due topremature infants need for large amounts of protein and energy toachieve appropriate growth.3,4 Additionally, inadequate substrateprovision is associated with delays in long-term growth and inneurodevelopmental outcome until at least school age.1,2 Recentinvestigations on the effect of early postnatal nutrition indicate thatthe rate of weight gain in premature infants is influenced by thequantity of calories given. Gains in length and head circumferenceson the other hand are affected by the amount of protein in the diet.4
Therefore, information about precise protein and energy contentsof each individual mother’s milk are highly desirable when feedingpremature infants.
Studies focusing on the macronutrient content of human milkfractions from mothers of extremely immature neonates are scarceand often cross-sectional.5,6 Various reports have revealed thatprotein concentrations of both preterm and term human milkdecline through lactation, whereas the contents of fat, lactose andcarbohydrate show no significant changes over time.5,6 In addition,considerable inter- and intra-individual variations have beendetected in the course of lactation.5,6 In extremely premature
utrition and Metabolism. All rights reserved.

J. Bauer, J. Gerss / Clinical Nutrition 30 (2011) 215e220216
infants, below 28 weeks of gestation, the lack of information aboutmilk’s macronutrient composition implies an obvious risk ofundernutrition or overnutrition. However, the decision on how tofortify mother’s milk for premature infants is arbitrary. Therefore,an individualized analysis of the composition of human milk isdesirable to minimize tolerance problems and to prevent sideeffects related to fortification.
The main objective of our present study was to analysemacronutrients, energy and minerals in human milk samples frommothers with preterm infants (mean gestational age: 28.4 � 3weeks) and to compare the results with full-term milk samplesover the first 8 weeks of lactation.
2. Subjects and methods
Breast milk samples were obtained from 113 healthy mothersgiving birth prematurely between 23 and 33weeks of gestation andhaving enough milk for their infants including a minimum of 3 mLmilk extra for the study. Only participants that completed the entirestudy period of 8 weeks of lactation were evaluated for the study.Therefore, 11 mothers were later excluded from the study forvarious reasons; 2 were translated to other hospitals after delivery,4 had insufficient milk supply, 4 mothers completed the milkproduction after 2 weeks for personal motives, and 1 moved faraway. The analyses of these milk samples were not used for thecalculations. Consequently, a total 102 participants were evaluatedfor the investigation: 4 mothers of 23 weeks of gestation, 8mothersof 24 weeks, and 10 women per each gestational age group from 25to 33 weeks, respectively. For comparison participants weredivided in 3 groups according their gestational duration in:1. extremely premature (below 28 weeks of gestation), 2. severelypremature (28e31 weeks), and 3. moderately premature (32e33weeks), respectively. The milk of additionally 10 term mothers wasalso analyzed. Milk specimens were collected longitudinally, atweekly intervals from the first to the eighth postpartum week. Atadmission all mothers received information about advantages ofhuman milk nutrition for the infant, and were encouraged toinitiate lactation immediately after delivery. Each woman obtaineda comprehensive instruction of milk collection proceduresincluding pumping and breastfeeding techniques by certificatedlactation consultants (e.g. principal investigator, J.B). Extendedsupport was initiated to sustain and maintain milk productionduring the complete study period, as well as to avoid different waysof collecting samples that could influence milk nutrient content. Allparticipants delivering prematurely and at term were visited athome weekly after discharge from the hospital to ensure a goodadherence to the study protocol. Mothers at home were requestedto collect once aweek for 24 h their milk for analyses. To control forpossible diurnal variations in human milk pooled probes onlya collection period of 8:00 AM to 8:00 AM was used for analyses.Milk samples were collected from each participant on the same dayeach week. During the 24-h period mothers assemble their milkevery 4 h. The collection of the 24-h samples started as soon astherewas sufficient milk to feed the infant and to take an additionalof 3 mL sample for analysis. Mothers pumped their breastmechanically (electric double-breast pump, Medela�, Germany)and collected the milk probes in sterile bottles until the end of the24-h collection period. Probes were pooled and stored in a refrig-erator at 4 �C until the end of the 24 h collection period. Samples foranalyses were taken from an entire 24-h collection period, andstored immediately at �70 �C until analyzed. Daily milk volumeoutput was recorded in each participant. The Ethical Committees ofthe Medical Faculties of the Universities of Muenster and Heidel-berg have approved the investigation and parental consent wasobtained before studying each individual infant.
2.1. Laboratory methods
Breast milk samples stored at �70 �C were analyzed for caloriccontent in duplicate for each sample, using a ballistic bomb calo-rimeter (Parr� 6200 Oxygen Bomb Calorimeter, Parr InstrumentCompany, USA). The protein concentration in milk samples wasdetermined according to the method of Lowry and later modifiedby Petersen.7,8 Carbohydrate content of the milk was analyzed bymeans of the Orcinol carbohydrate assay as detailed described byPolberger et al.9 Creamatocrit values were determined using thetechnique presented by Lucas et al.10Well mixedmilk aliquots wereplaced into 2 glasses capillary tubes (75 mL), which were sealed atone end and centrifuged in a hematocrit centrifuge for 5 min at12,000 rpm. The creamatocrit was expressed as a percentage of thelength of the milk column in the tube. With the described tech-niques a minimum of 3 mL milk per week was needed for analysis.Minerals concentration was measured by an absorption spec-trometer and colorimetric assay with endpoint determination andsample blank (Roche� GmbH, Germany).
2.2. Statistical methods
Data were analyzed with the SPSS statistical software (Version17.0 for Windows, SPSS Inc, Chicago, IL, USA) and SAS (Version 9.2forWindows, SAS Institute Inc., Cary, NC, USA). Means and standarddeviations (SD) of target parameters were calculated for eachgestational age and lactation week. Correlations between targetparameters and gestation as well as lactation week were describedusing Pearson’s correlation coefficient. In order to test for signifi-cant differences between gestational age groups, multivariateanalyses were performed. The milk of extremely preterm infantswere correlated against the severely, moderately and term milk. Amixed linear model was established for each target parameter thatincluded a normally distributed random intercept (i.e., subjecteffect) as well as the fixed co-variables lactation week and gesta-tional age group. Themixedmodel approachwas chosen in order toaccount for intra-individual correlations among repeated obser-vations collected from the same subject (longitudinal or clustereddata). Data within each cluster (i.e., subject) cannot be regardedstochastically independent, in contrast to inter-individual datacollected from different subjects. The model was fitted usinga Restricted Maximum Likelihood approach. All statistical analyseswere intended to be rather exploratory than confirmatory. P-valueswere considered statistically significant in the case of p < 0.05. Noadjustment for multiple testing was carried out.
3. Results
All participants were healthy without suffering from hyperten-sive disorders or diabetes mellitus before, during or after preg-nancy, and none of them was vegetarian or followed a specialnutritional diet. Mother’s delivering prematurely had a meangestational age of 28.4 � 3.0 weeks (median 28 weeks), and theterm group of 39 � 0.9 weeks (median 39 weeks), respectively. Thefirst collection started in all participants 6 � 3 days after birth.
3.1. Human milk content
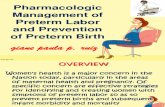
3.1.1. ProteinProtein values of both preterm and term human milk decreased
linearly with progressive week of lactation (Fig. 1). The differenceon protein content between the sub-groups of preterm milksamples is demonstrated on Table 1 showing remarkable higherprotein values in the extremely immature milk in contrast withmore mature human milk. A comparison between protein average

Fig. 1. Protein concentration (g/dl) in preterm and term milk during lactation. Boxplots illustrating median, quartiles, range and outliers (B) and extremes (*).
J. Bauer, J. Gerss / Clinical Nutrition 30 (2011) 215e220 217
values from the preterm groups and term human milk wasdemonstrated in Table 2. The Pearson’s correlation coefficient wasused for comparing protein concentration between target param-eters presenting a closed relation to lactation week (r ¼ �0.626),but only a weak relation to gestational age (r ¼ �0.377). Multi-variate analyses showed that protein decreased by 0.12 g/dl perlactation week (p < 0.0001, 95% CI 0.113, 0.124). Protein content inextremely preterm human milk versus severely preterm humanmilk differed by 0.193 g/dl (p < 0.0001, 95% CI 0.104, 0.282), versusmoderately preterm human milk by 0.452 g/dl (p < 0.0001, 95% CI0.344, 0.562), and in contrast to term human milk by 0.73 g/dl(p < 0.0001, 95% CI 0.589, 0.871), respectively.
3.1.2. FatAverage fat values of preterm milk were significantly higher
compared to term human milk as demonstrating in Table 2. Lipidconcentrationswere related to lactationweek (r¼ 0.670), but not togestational week (r¼ 0.152). During the observation period averagelipid concentration increased significantly (p < 0.001) in pretermmilk from initially 2.9 � 0.1 g/dl to 6.8 � 0.3 g/dl at 8 weeks oflactation, and in term milk from 2.9 � 0.3 g/dl to 4.9 � 0.2 g/dl,respectively. Lipid content in extremely preterm human milkversus term human milk increased by 0.382 g/dl (95% CI 0.226,0.537, p< 0.05). In the comparison of severely preterm humanmilk
Table 1Protein content (g/dl) of human milk from 112 women delivering premature and at term
Lactation weeks Gestational age (weeks)
23 24 25 26 27
1 Mean 2.8 3.0 3.0 2.7 2.9SD 0.2 0.2 0.2 0.2 0.1
2 Mean 2.9 2.8 2.8 2.3 2.8SD 0.1 0.1 0.1 0.1 0.1
3 Mean 2.7 2.9 2.5 2.0 2.6SD 0.1 0.1 0.1 0.1 0.1
4 Mean 2.7 2.7 1.9 2.0 2.4SD 0.1 0.1 0.1 0.1 0.1
5 Mean 2.6 2.6 1.9 1.7 2.3SD 0.1 0.1 0.1 0.1 0.1
6 Mean 2.6 2.6 1.7 1.7 2.1SD 0.2 0.1 0.1 0.1 0.1
7 Mean 2.5 2.5 1.8 1.7 2.1SD 0.1 0.1 0.2 0.1 0.1
8 Mean 2.0 2.6 1.7 1.7 2.0SD 0.1 0.1 0.1 0.1 0.1
Results are expressed as Mean � SD.
versus term human milk lipid values differed by 0.375 g/dl (95% CI0.219, 0.532, p< 0.05), and versus moderately preterm humanmilkby 0.765 g/dl (95% CI 0.594, 0.937, p < 0.05), respectively.
3.1.3. CarbohydrateThe carbohydrate average concentration of preterm milk was
significantly higher compared to term milk values (p < 0.05, asshowing in Table 2), and increased significantly (p < 0.001) in thepreterm and term milk during the observation period. In thepreterm milk the minimal concentration was measured at the first2 weeks with a mean of 6.3� 0.1 g/dl increasing to 8.5� 0.2 g/dl. Interm milk a minimum of 5.0 � 0.2 g/dl of carbohydrate concen-tration was detected in the first week reaching a maximum of7.4 � 0.3 g/dl at the end of the study. No pronounced correlation tolactation week (r ¼ 0.295) and to gestation week (r ¼ 0.021) wasfound during the study period. Extremely preterm human milkversus term human milk differed by 1.43 g/dl (95% CI 1.21, 1.65,p < 0.0001).
3.1.4. EnergyPositive correlations between lipid and energy values were
detected in all lactation weeks in both preterm and term milkgroups. Energy density increased in the preterm milk from64.8 � 0.5 in the first study week to 86.6 � 1.9 kcal/dl during thestudy period, and from 65.3 � 3.1 kcal/dl to 71.0 � 3.5 kcal/dl in theterm milk, respectively. Average energy content in preterm humanmilk showed significantly higher values than term milk during thestudy period (p < 0.05, see Table 2). No differences were observedbetween premature groups.
3.1.5. MineralsMineral contents were higher in the extremely immature milk
compared to the moderately pretermmilk, but without statisticallysignificance (see Table 2). Sodium values of preterm milk aredemonstrated in Fig. 2 showing higher values in the first studyweek than in the 8th week of lactation (p < 0.05). No differences inthe concentrations of potassium, phosphate, magnesium andcalcium were established between the different preterm groupsand the term milk group (see Table 2).
3.1.6. Milk outputIn the first lactation week preterm mothers produced on
average 254 � 125 mL/d and on the eighth week a volume of759 � 325 mL/d, term mothers of 396 � 258 mL/d at the first and
.
28 29 30 31 32 33 Term
2.7 2.6 2.5 2.5 2.3 2.2 2.20.1 0.1 0.2 0.1 0.2 0.2 0.22.3 2.5 2.2 2.5 2.2 2.1 1.90.1 0.2 0.2 0.1 0.1 0.1 0.32.1 2.3 2.2 2.5 2.1 2.0 1.70.1 0.2 0.2 0.1 0.2 0.1 0.11.8 2.4 2.1 2.4 1.8 2.0 1.70.1 0.1 0.1 0.1 0.1 0.1 0.22.0 2.3 2.1 2.2 1.8 1.8 1.50.2 0.1 0.1 0.2 0.1 0.1 0.21.2 2.1 2.0 2.1 1.6 1.8 1.30.1 0.1 0.2 0.1 0.2 0.1 0.21.5 2.1 2.0 2.0 1.6 1.6 1.20.1 0.1 0.2 0.1 0.2 0.2 0.21.5 2.1 1.9 2.0 1.6 1.4 1.10.1 0.3 0.2 0.2 0.2 0.1 0.1

Table 2Comparison between preterm and term human milk nutrient components during 8 weeks of lactation.
Extremely PretermHuman Milk(<28 weeks)
Severely PretermHuman Milk(28e31 weeks)
Moderately PretermHuman Milk(32e33 weeks)
Term Human Milk
Protein (g/dl) 2.3 � 0.5 2.1 � 0.3 1.9 � 0.3 1.6 � 0.4*Carbohydrates (g/dl) 7.6 � 0.6 7.5 � 0.6 7.5 � 0.5 6.2 � 0.9*Fat (g/dl) 4.4 � 0.9 4.4 � 0.8 4.8 � 1.0 4.1 � 0.7*Energy (kcal/dl) 77.8 � 8.4 77.6 � 5.9 76.7 � 6.5 67.7 � 3.9*Sodium (mmol/l) 10.6 � 1.9 10.6 � 2.2 10.4 � 1.9 11.2 � 2.1Potassium (mmol/l) 14.0 � 2.2 13.1 � 2.5 12.1 � 1.8 11.5 � 1.9Calcium (mmol/l) 6.2 � 1.4 6.5 � 1.0 7.4 � 1.1 5.4 � 0.8Magnesium (mmol/l) 1.6 � 0.3 1.5 � 0.3 1.7 � 0.2 1.3 � 0.2Chloride (mmol/l) 10.2 � 2.3 12.5 � 3.0 10.2 � 1.5 10.9 � 1.0Phosphate (mmol/l) 2.2 � 0.5 2.1 � 0.3 2.0 � 0.3 1.9 � 0.3
Preterm milk (average concentration) compared to term human milk, *p < 0.00.05, results are expressed as mean � SD.
J. Bauer, J. Gerss / Clinical Nutrition 30 (2011) 215e220218
985 � 327 mL/d at the last study week, respectively. Comparingmilk output of mothers of extremely preterm gestation to milkvolume of women delivering at a moderately preterm gestation nosignificant difference was detected (p ¼ 0.15).
4. Discussion
In the present investigation we confirmed as previously indi-cated in the literature that preterm human milk shows consider-able differences in the macronutrient composition compared toterm milk.11 Furthermore, we detected a significant difference inmilk protein levels between women delivering extremely early(<28 weeks) compared to mothers giving birth moderatelypremature (32e33 weeks). This indicates an inverse relationshipbetween protein content and gestation. It is remarkable thatmothers of extremely premature infants are in fact able to producehigher protein levels despite the exceptionally short gestation. Thepresent data reveal a pronounced effect of gestational age andlactation week on protein content in preterm human milkcompared to values indicated in the literature.12 It is not a newobservation that preterm human milk differs from term milk, butwe detected a surprisingly high variation in milk protein content ofmothers with infants born extremely prematurely and moreadvanced gestation.
Preterm milk contains protein levels between 1.8 and 2.4 g/dlduring the first month of lactation, as previously reported.11,13,14Wefound higher protein concentrations of 2.7e3.0 g/dl in the milk ofwomen delivering early at 23e24 weeks, whereas in mothers of
1 2 3 4 5 6 7 8
0
5
10
15
20
Lactation weeks
So
diu
m valu
es (m
mo
l/l)
Fig. 2. Sodium values of preterm human milk (23e33 weeks of gestation). Box plotsillustrating median, quartiles, range and outliers (B) and extremes (*).
more advanced gestation (32e33 weeks) concentrations rangedfrom 1.8 to 2.3 g/dl. Only few studies investigating the milk proteincontent of extremely immature milk (below 28 weeks) demon-strated a relation between milk composition and the degree ofprematurity.15 Most investigators have analyzed more mature milk(over 28 weeks of gestation) indicating protein concentrations from2.8 to 1.5 g/dl,11,13e16 which are similar to our results detected inseverely and moderately preterm human milk during the firstmonth of lactation. Theses compositional differences can onlypartly be explained by a compensation for the reducedmilk volumeproduced by women giving birth prematurely. In fact, the proteinproduction per 24-h sampling period is higher in mother’s milk ofextremely premature infants suggesting an adaptation to thehigher protein requirements of these infants.
In the present study, carbohydrate concentration of humanmilkincreased gradually during the postpartum weeks of lactation, aswell as fat content independent of milk volume. Faerk et al.15
demonstrated that carbohydrate and fat concentrations increasedafter 2 weeks of lactation reaching a constant level after this period.Preterm milk contained significantly more fat than term milk andshowed a further increase during lactation. The high fat contentwas responsible for the high energy density of preterm milk.Changes in electrolyte compositionwere only seen in the first weekof lactation. Especially a decline in sodium concentrationwas notedstarting in the second week of lactation in all preterm groups. If theinitial high sodium concentration simply reflects an adaptation tothe small breast milk volume produced in the first days after birth,one would expect electrolyte concentrations to be altered in everywoman with minimal milk output independent of the length ofgestation. Accordingly, an inverse relationship between milkvolume and sodium levels has been observed and reported byseveral researchers.17 The finding that mothers who had low breastmilk sodium concentrations on day 3 of lactation had a greatchance of nursing successfully was explained by low milk sodiumconcentrations, whichmight be amarker of milk production.18 Milkvolumes from both preterm and term mothers were not signifi-cantly different in our study, and no differences in sodiumconcentration were detected when comparing preterm term andterm human milk at any week of lactation. This stresses that ourunderstanding of the physiological processes responsible for thenutrient composition in human milk is still limited. Despiteincreasing evidence that a lactogenic hormone complex is requiredfor the initiation of lactation at parturition, the origin of higherprotein content and variations in mineral content in pretermhuman milk is not completely understood.19,20 It seems likely thatthe discrepancies are due to differences in hormonal balance andmetabolic regulation associated with shorter gestational periodand certain aspects of immaturity of the mammary gland.19e21

J. Bauer, J. Gerss / Clinical Nutrition 30 (2011) 215e220 219
Studies in this field still yield conflicting results, and furtherresearch in hormonal regulation of lactation in prematurity isneeded before a more precise picture of this complex process mayarise. It may be suggested that the mammary gland of the motherdelivering prematurely is functionally developed and undergoesregular maturational processes, which are responsible for changesin milk composition.19e25
Inadequate protein intake due to declining levels in humanmilkmay lead to inappropriate growth in premature infants,22,23
therefore a supplement is routinely added. At the same time, thecurrently available milk fortifiers need to be improved to bettermimic human milk.24 The higher protein levels found in ourpreterm human milk samples might be of advantage to the rapidlygrowing premature infant, whose protein requirement has beenestimated to be greater than that of the more mature infant.4
Furthermore, our results of a high variability in milk proteincontent from mothers of both extremely short gestational age andof more advanced pregnancy should guide us towards more indi-vidualized nutritional regimens. With the recognition thatextremely preterm human milk (<28 weeks) has initially highernutrient concentrations (e.g. protein, carbohydrate, fat) thanpreviously estimated together with recently published recom-mendations on nutrient needs of premature infants,25 new calcu-lations for supplementation will be useful. Recent studies indicatethat the rate of weight again in preterm infants is affected by theamount of calories, whereas gains in length and head circumfer-ence are dependent upon the quantity of protein in the nutrition.4
Consequently, inadequate substrate supply results in changes inbody composition, which might have effects on later life.26 Thisintriguing observation of higher human milk protein levelssuggests that milk of mothers of extremely premature infants areadapted to the growth requirements of these neonates. The prac-tical significance of this finding in view of nutritional or immuno-logical and metabolic properties of the produced proteins remainsto be established.
Human milk protein represents a heterogeneous mixture ofcompounds and no assay can satisfactorily measure all of itscomponents. Therefore, we are well aware that our method ofestimating protein content has its limitations. The Lowry methodhad low variability for whey and skimmed milk samples, but thismethod yielded analytical values closest to Kjeldahl proteinvalues.27 Another limitation of the present study is the high degreeof subjectivity regarding the creamatocrit using a caliper. Thisconcern leads to our decision to determine energy density inhuman milk.
Several factors such as weeks of lactation, breastfeeding time,gestational age, genetic factors and dietary habits are responsiblefor inter-individual changes found in human milk components.3,5,6
Studies comparing preterm and term human milk have showndifferences for a number of nutrients, although some of the resultsare contradictory.12,28 Different sampling and processing methodscan result in variations in the quantity and in the composition ofhuman milk.3,12,16 To minimize variables (e.g. sampling methods)that may affect milk composition, each participant receivedprofessional support by lactation consultants providing instructionin sampling milk during the entire investigation including homevisits after discharge. Frommacronutrient analyses it is known thathumanmilk shows a large change in protein and fat content duringlactation.29,15 Studies focusing on the nutrient composition ofhuman milk from mothers of extremely preterm neonates, partic-ularly under 28 weeks of gestation, are limited due to hormonaland psychological factors that cause insufficient milk output.Clearly, mothers experience a greater degree of psychologicaldistress after giving birth to a premature infant who remainshospitalized for a long period of time compared to mothers who
deliver a healthy term neonate. In general, it is quite difficult to findan adequate number of mothers who are not only able to feed theirpreterm infants for an extended period and are also willing toparticipate in a clinical study when undergoing an enormouslystressful experience. Trials have demonstrated that maternalanxiety and stress during puerperium have a negative impact onbreastfeeding outcome suggesting that counseling and supportinganxious mothers of high-risk infants may contribute to increasedlactation initiation and maintenance.30 Lactation consultants takeon a very important role for the promotion of human milk feedingin modern medicine providing special support to high-risk groupswho have not been breastfeeding in recent decades. Our studypointed out that appropriate management of lactation and infor-mation about the essential role of human milk in the nutrition ofpreterm infants are helpful to ensure lactation inwomen deliveringextremely early. The professional support for all lactating mothersand the effort to promote skin-to-skin care in our unit facilitatedthemilk production after birth. Non-nutritive suckling at the emptybreast and oral stimulation initiated as soon as possible contributedfavorable to establish milk supply during the entire study period.
In summary, a longitudinal collection of milk samples from thesame preterm and term mothers allowed us to observe composi-tional pattern changes for specific nutrients with progressingweeks of lactation. Individualized protein fortification of breastmilk is highly desirable to improve nutritional management invulnerable premature infants and facilitates a more precisesupplementation of human milk than currently possible. Thesedata provide a more detailed insight into nutrient intake of preterminfants fed breast milk, whereas further research is needed on thetopic of nutrient utilization in this area.
Conflict of interest statementNone of the authors have a conflict of interest.
Acknowledgments
We particularly thank the participating mothers, without whomthis studywould not have been possible, for generous contributionsand understanding at time when they were undergoing an enor-mously stressful experience.
The authors gratefully acknowledge the technical support ofThorstenMarquardt from the University Children’s Hospital ofMuenster, of Michael C. Frühwald for manuscript review from theKlinikum Augsburg, Pediatrics 1, and of ManfredFobker and Jerzy-Roch Nofer from the Institute of Clinical Chemistry and LaboratoryMedicine, University of Muenster, Germany.
The authors’ responsibilities were as follows e JB: responsiblefor the overall study design, involved in subjects’ recruitment, datacollection and analysis, performed the measurements, and wrotethe manuscript. JG: performed the statistical analysis of the data,participated in the discussion of the results, and in the correction ofthe manuscript.
References
1. Isaacs EB, Morley R, Lucas A. Early diet and general cognitive outcome atadolescence in children born at or below 30 weeks gestation. J Pediatr2009;155:229e34.
2. Lawrence RM. Breastfeeding. Host-resistance factors and immunologicsignificance of human milk. In: Lawrence RA, Lawrence RM, editors. Breast-feeding. A guide for the medical profession. 6th ed. Philadelphia: Elsevier, Mosby;2006. p. 171e214.
3. Mikkola K, Ritari N, Tommiska V, Salokorpi T, Lehtonen L, Tammela O, et al.Neurodevelopmental outcome at 5 years of age of a national cohort ofextremely low birth weight infants who were born in 1996e1997. Pediatrics2005;116:1391e400.
4. Sauer PJ. Can extrauterine growth approximate intrauterine growth? Should it?Am J Clin Nutr 2007;85:608Se13S.

J. Bauer, J. Gerss / Clinical Nutrition 30 (2011) 215e220220
5. Wojcik KY, Rechtman DJ, Lee ML, Montoya A, Medo ET. Macronutrient analysisof a nationwide sample of donor breast milk. J Am Diet Assoc 2009;109:137e40.
6. Maas YG, Gerritsen J, Hart AA, Hadders-Algra M, Ruijter JM, Tamminga P, et al.Development of macronutrient composition of very preterm human milk.Br J Nutr 1998;80:35e40.
7. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with thefolin phenol reagent. J Biol Chem 1951;193:265e75.
8. Peterson GL. A simplification of the protein assay method of Lowry et al. whichis more generally applicable. Anal Biochem 1977;83:346e56.
9. Polberger S, Lönnerdal B. Simple and rapid macronutrient analysis of humanmilk for individual fortification: basis for improved nutritional management ofvery-low-birth-weight infants? JPGN 1993;17:283e90.
10. Lucas A, Gibbs JA, Lyster RL, Baum JD. Creamatocrit: simple clinical techniquefor estimating fat concentration and energy value of human milk. Br Med J1978;22(1):1018e20.
11. Anderson DM, Williams FH, Merkatz RB, Schulman PK, Kerr DS, Pittard 3rd WB.Length of gestation and nutritional composition of human milk. Am J Clin Nutr1983;37:810e4.
12. Lubetzky R, Mimouni FB, Dollberg S, Salomon M, Mandel D. Consistent circa-dian variations in creamatocrit over the first 7 weeks of lactation: a longitu-dinal study. Breastfeed Med 2007;2:15e8.
13. Beijers RJ, Graaf FV, Schaafsma A, Siemensma AD. Composition of prematurebreast-milk during lactation: constant digestible protein content (as in fullterm milk). Early Hum Dev 1992;29:351e6.
14. Atkinson SA, Bryan MH, Anderson GH. Human milk feeding in prematureinfants: protein, fat, and carbohydrate balances in the first two weeks of life.J Pediatr 1981;99:617e24.
15. Faerk J, Skafte L, Petersen S, Peitersen B, Michaelsen KF. Macronutrients in milkfrom mothers delivering preterm. Adv Exp Med Biol 2001;501:409e13.
16. Pamblanco M, Ten A, Comín J. Proteins in preterm and term milk from mothersdelivering appropriate or small-for-gestational age infants. Early Hum Dev1986;14:267e72.
17. Lang S, Lawrence CJ, Orme RL. Sodium in hand and pump expressed humanbreast milk. Early Hum Dev 1994;38:131e8.
18. Morton JA. The clinical usefulness of breast milk sodium in the assessment oflactogenesis. Pediatrics 1994;93:802e6.
19. Pang WW, Hartmann PE. Initiation of human lactation: secretory differentia-tion and secretory activation. J Mammary Gland Biol Neoplasia 2007;12:211e21.
20. Hill PD, Aldag JC, Demirtas H, Naeem V, Parker NP, Zinaman MJ, et al. Associ-ation of serum prolactin and oxytocin with milk production in mothers ofpreterm and term infants. Biol Res Nurs 2009;10:340e9.
21. Chatterton Jr RT, Hill PD, Aldag JC, Hodges KR, Belknap SM, Zinaman MJ.Relation of plasma oxytocin and prolactin concentrations to milk production inmothers of preterm infants: influence of stress. J Clin Endocrinol Metab2000;85:3661e8.
22. Arslanoglu S, Moro GE, Ziegler EE. Preterm infants fed fortified human milkreceive less protein than they need. J Perinatol 2009;29:489e92.
23. Simmer K, Metcalf R, Daniels L. The use of breastmilk in a neonatal unit and itsrelationship to protein and energy intake and growth. J Pediatr Child Health1997;33:55e60.
24. Doege C, Bauer J. Effect of high volume intake of mother’s milk with an indi-vidualized supplementation of minerals and protein on early growth ofpreterm infants <28 weeks of gestation. Clin Nutr 2007;26:581e8.
25. Agostoni C, Buonocore G, Carnielli VP, De Curtis M, Darmaun D, Decsi T, et al.Enteral nutrient supply for preterm infants: commentary from the EuropeanSociety of Paediatric Gastroenterology, Hepatology and Nutrition Committeeon Nutrition. J Pediatr Gastroenterol Nutr 2010;50:85e91.
26. Barker DJ. Obesity and early life. Obes Rev 2007;8(Suppl. 1):45e9.27. Lönnerdal B, Woodhouse LR, Glazier C. Compartmentalization and quantization
of protein in human milk. J Nutr 1987;117:1385e95.28. Polberger S, Alexlsson IA, Raiha NC. Growth of very low birth weight infants on
varying amounts of human milk protein. Pediatr Res 1989;25:414e9.29. Wojcik KY, Rechtman DJ, Lee ML, Montoya A, Medo ET. Macronutrient analysis
of a nationwide sample of donor breast milk. J Am Diet Assoc 2009;109:137e40.30. Sisk PM, Lovelady CA, Dillard RG, Gruber KJ, O’Shea TM. Maternal and infant
characteristics associated with human milk feeding in very low birth weightinfants. J Hum Lact 2009;25:412e9.