LONG – TERM SMASH TISSUE SYNDROME (CRUSH- SYNDROME)
31
LONG – TERM LONG – TERM SMASH TISSUE SMASH TISSUE SYNDROME SYNDROME (CRUSH- (CRUSH- SYNDROME) SYNDROME)
-
Upload
earl-berry -
Category
Documents
-
view
241 -
download
3
Transcript of LONG – TERM SMASH TISSUE SYNDROME (CRUSH- SYNDROME)
LONG – TERM LONG – TERM SMASH TISSUE SMASH TISSUE
SYNDROMESYNDROME(CRUSH-(CRUSH-
SYNDROME) SYNDROME)
Long – term smash tissue syndrome is a Long – term smash tissue syndrome is a kind of traumatic pathology, which arises kind of traumatic pathology, which arises after long – term crushing soft tissues of after long – term crushing soft tissues of limbs by destroyed buildings, stones, limbs by destroyed buildings, stones, ground. There are other synonyms: long-ground. There are other synonyms: long-term crumple syndrome, crush-syndrome, term crumple syndrome, crush-syndrome, traumatic compress, also – recirculative traumatic compress, also – recirculative syndrome.syndrome.
The are following versions of the long-term The are following versions of the long-term smash tissue syndrome :smash tissue syndrome :
1.1. By influence mechanism:By influence mechanism:- crush;- crush;- direct pressing;- direct pressing;- positional pressing;- positional pressing;
2.2. By localization of force:By localization of force:- Thorax;- Thorax;- Abdomen;- Abdomen;- Pelvis;- Pelvis;- Hand;- Hand;- Forearm;- Forearm;- Brachium;- Brachium;- Foot;- Foot;- Crus;- Crus;- Femur;- Femur;
3. By combinations of injures:3. By combinations of injures:- Internal organs;- Internal organs;
- Bones;- Bones;
- Joints;- Joints;
- Main arteries;- Main arteries;
- Nerves;- Nerves;
4. By complications:4. By complications:- Limb ischemia (compensative, non-compensative, non-- Limb ischemia (compensative, non-compensative, non-
reverse);reverse);
- Inner organs and systems (pneumonia, heart infarction, - Inner organs and systems (pneumonia, heart infarction, lungs swelling, fat embolism, etc).lungs swelling, fat embolism, etc).
5. By degree of critically:5. By degree of critically: Easy;Easy; Middle;Middle; Hard;Hard;
6. By periods of compression:6. By periods of compression: Early;Early; Middle;Middle; Late.Late.
7. By present of combined injuries:7. By present of combined injuries: Blood loss;Blood loss; Burns, frostbite;Burns, frostbite; Barotraumas;Barotraumas; Radiation sickness;Radiation sickness; Intoxication (poisoning) of chemical substances.Intoxication (poisoning) of chemical substances.
There are three periods of There are three periods of long-term smash tissue long-term smash tissue
syndrome, those are syndrome, those are distinguished in a clinics:distinguished in a clinics:
►Early – shock manifestation (till third Early – shock manifestation (till third day after trauma);day after trauma);
►Intermediate manifestates by acute Intermediate manifestates by acute renal insufficiencia;renal insufficiencia;
►Late, or a period of convalence (a Late, or a period of convalence (a beginning of second week till 1 – 2 beginning of second week till 1 – 2 month).month).
After shock an intermidiate or light After shock an intermidiate or light period begins. It can be also in a hard period begins. It can be also in a hard form, and those can lead to death. A form, and those can lead to death. A condition of a patient getting better, condition of a patient getting better, there is no pain, normalization of a there is no pain, normalization of a pulse and blood pressure are observed, pulse and blood pressure are observed, body temperature is 37,6 – 38,5 body temperature is 37,6 – 38,5 °°C; an C; an olyguria registates.olyguria registates.
Next period of long-term smash tissue syndrome Next period of long-term smash tissue syndrome manifestates till 4 – 5 day after trauma with manifestates till 4 – 5 day after trauma with acute renal insufficient (dyshydria, acute renal insufficient (dyshydria, hyperazotemia, hyperpotassiumemia, hyperazotemia, hyperpotassiumemia, increasing of metabolic acidosis). Diuresis increasing of metabolic acidosis). Diuresis gets shorter till critical level (30 – 20 ml/h). gets shorter till critical level (30 – 20 ml/h). Also there are anemia, hyposodiumemia, Also there are anemia, hyposodiumemia, hypocalciumemia, and albumen contents get hypocalciumemia, and albumen contents get down till 5 ± 0,1 g%. An acute renal down till 5 ± 0,1 g%. An acute renal insufficient can be observed also at those insufficient can be observed also at those cases, when there is no shock.cases, when there is no shock.
►At the end of long-term smash tissue At the end of long-term smash tissue syndrome during a convalence period syndrome during a convalence period functions of kidney renew other organs, a functions of kidney renew other organs, a water-electrolytic balance are normalizes.water-electrolytic balance are normalizes.
►Anaesthetization should be given at first Anaesthetization should be given at first medical care, before getting out from ruins and medical care, before getting out from ruins and stones. Ketaminum is used very often in stones. Ketaminum is used very often in prehospitalic anaesthetization; it combines prehospitalic anaesthetization; it combines with seduxenum effectively; an analgesic with seduxenum effectively; an analgesic effect manifests in a doses 0,1 – 1 mg/kg per effect manifests in a doses 0,1 – 1 mg/kg per body weight after intravenous introduction.body weight after intravenous introduction.
The first specialist who had singled out The first specialist who had singled out
shock was shock was Le Dran (1737)Le Dran (1737). He . He described the symptoms and described the symptoms and introduced the term “shock” (stroke, introduced the term “shock” (stroke, shake, jolt) and treated the patients shake, jolt) and treated the patients with rest, alcohol and opium.with rest, alcohol and opium.
There are two mechanisms in the There are two mechanisms in the pathogenesis of the long – term pathogenesis of the long – term smash tissue syndrome: first is smash tissue syndrome: first is forced crumpling of soft tissues forced crumpling of soft tissues with long-term ischemia and second with long-term ischemia and second is destroying of anatomic structures is destroying of anatomic structures closed or opened types.closed or opened types.
The syndrome belongs to one of traumatic The syndrome belongs to one of traumatic diseases and it has universal nonspecific diseases and it has universal nonspecific reactions of organism on a trauma. The reactions of organism on a trauma. The reaction of central nervous system and reaction of central nervous system and violation of microcirculation, which in the violation of microcirculation, which in the hardest cases develop as a shock are on hardest cases develop as a shock are on the first place. They develop on the very the first place. They develop on the very beginning of factor activity and continue beginning of factor activity and continue after its cessation; a toxemia and after its cessation; a toxemia and plasmorrhagia increasing.plasmorrhagia increasing.
Generalized and long-term process of micro Generalized and long-term process of micro circulative violations cause globules formation circulative violations cause globules formation of fat and micro thrombus in the micro vessels of fat and micro thrombus in the micro vessels gap, after resuming of hemodynamics a large gap, after resuming of hemodynamics a large quantity of this globules spread with blood quantity of this globules spread with blood flowing in different organs and tissues. The flowing in different organs and tissues. The obstruction of tissue micro circulative system obstruction of tissue micro circulative system promotes a disorganization of brain, lungs, promotes a disorganization of brain, lungs, liver, kidneys work – long-term smash tissue liver, kidneys work – long-term smash tissue syndrome is many-sided, intricate for syndrome is many-sided, intricate for diagnosis.diagnosis.
Pathological result of direct cells destroying appears Pathological result of direct cells destroying appears immediately, but during ischemic injuring of muscle immediately, but during ischemic injuring of muscle result appears some hours later. Since middle term of result appears some hours later. Since middle term of ischemic death of striated muscles is near six hours, so ischemic death of striated muscles is near six hours, so the cause of early necrosis (first hours) is mechanical the cause of early necrosis (first hours) is mechanical factor, but in the later period is factor, but in the later period is hypoxyahypoxya. Because of . Because of direct tissue destruction intra cellular substances get into direct tissue destruction intra cellular substances get into blood; during the compressive-ischemic muscle injuring blood; during the compressive-ischemic muscle injuring in the most cases ischemic toxin penetrate into system in the most cases ischemic toxin penetrate into system of blood flowing (metabolites of anaerobic glycolysis). of blood flowing (metabolites of anaerobic glycolysis). In both cases appears destroying of blood circulation In both cases appears destroying of blood circulation and breathing, but symptoms of ischemic toxins and breathing, but symptoms of ischemic toxins influence increase slowly.influence increase slowly.
Over dosage causes not desired anesthesia till time Over dosage causes not desired anesthesia till time of patients getting into the hospital. It hardens of patients getting into the hospital. It hardens diagnostics by loss of contact with patients, diagnostics by loss of contact with patients, changing of clinical picture of possible changing of clinical picture of possible craniocerebral trauma, intracavital injuries. In craniocerebral trauma, intracavital injuries. In specialized «emergency» car it is possible to specialized «emergency» car it is possible to provide blockades (conductive) using local provide blockades (conductive) using local anesthetics and also inhalation of nitrogenium anesthetics and also inhalation of nitrogenium oxydulatum with oxygen (through the mask), oxydulatum with oxygen (through the mask), trichlorineethylene, inhalation (through special trichlorineethylene, inhalation (through special sets). In case of opened injuries local anesthesia sets). In case of opened injuries local anesthesia is provided; to solution of novocainum there is provided; to solution of novocainum there might be added modern antibiotics of wide action might be added modern antibiotics of wide action spectrum. It considerably improves fight with spectrum. It considerably improves fight with infection. elimination. infection. elimination.
In large injuries of soft tissues, and especially in In large injuries of soft tissues, and especially in fractures immobilization of all injured limb is fractures immobilization of all injured limb is necessary. It’s good to use pneumatic necessary. It’s good to use pneumatic immobilizers, which help to prevent plasma immobilizers, which help to prevent plasma loss by moderate pressing on limbs. Last time loss by moderate pressing on limbs. Last time «anti-shock pants» is used with the same aim. «anti-shock pants» is used with the same aim. During their usage pressure in abdomen and During their usage pressure in abdomen and lower limbs is near 80 mm Hg that decreases lower limbs is near 80 mm Hg that decreases blood loss in intra-abdominal bleeding. It is blood loss in intra-abdominal bleeding. It is considered that these pants are effective considered that these pants are effective measure in shockmeasure in shock
First aid at the crush-syndromeFirst aid at the crush-syndrome
1.1. Remove the compressing factorRemove the compressing factor
2.2. Made the proximal tourniquet to Made the proximal tourniquet to prevent prevent spreadingspreading of toxins for all of toxins for all organismorganism
3.3. Prescribe the narcotic Prescribe the narcotic analgeanalgetticics to s to prevent the formation of pain shockprevent the formation of pain shock
Nowadays in system of pre-hospital Nowadays in system of pre-hospital measures during crush syndrome measures during crush syndrome special accent is put on early base special accent is put on early base infusion into the organism. But there infusion into the organism. But there must be excluded solutions containing must be excluded solutions containing potassium (Ringer’s, Hartmann’s potassium (Ringer’s, Hartmann’s solutions, “Lactasolum”).solutions, “Lactasolum”).
Special attention to infusion anti-shock therapy must Special attention to infusion anti-shock therapy must be put during not fast enough transportation of be put during not fast enough transportation of medical group to focus of catastrophe that leads to medical group to focus of catastrophe that leads to late of these measures. It is needed to continue late of these measures. It is needed to continue infusion therapy and during transportation infusion therapy and during transportation (especially long-term). During evacuation by air (especially long-term). During evacuation by air transport it is needed to use special apparatus for transport it is needed to use special apparatus for infusion because during changes of pressure infusion because during changes of pressure infusion therapy in air by usual way practically infusion therapy in air by usual way practically stops. During combination of crush syndrome with stops. During combination of crush syndrome with overcooling infusion therapy must be provided by overcooling infusion therapy must be provided by solutions heated to 38-40solutions heated to 38-40ooC; they provide body and C; they provide body and limbs massage by special tampons with alcohol, use limbs massage by special tampons with alcohol, use hot water bottles.hot water bottles.
On the stage of hospital treatment elimination of On the stage of hospital treatment elimination of hyperkaliemia it is needed to make an urgent hyperkaliemia it is needed to make an urgent intravenous infusion of hypertonic (40%) solution of intravenous infusion of hypertonic (40%) solution of glucose (50 ml) with insulin, 10% solution of glucose (50 ml) with insulin, 10% solution of calcium chloride or gluconate (30 ml for 20 min.) If calcium chloride or gluconate (30 ml for 20 min.) If the level of potassium in blood plasma is more than the level of potassium in blood plasma is more than 7 mmol/liter except glucose with insulin and 7 mmol/liter except glucose with insulin and calcium preparates it is indicated to use absorbents calcium preparates it is indicated to use absorbents (polystiren-sulfonate, haemo- or peritoneal dialisis). (polystiren-sulfonate, haemo- or peritoneal dialisis). Special attention should be paid to diuresis control.Special attention should be paid to diuresis control.
Intensive therapy during crush Intensive therapy during crush syndrome is to be started in the syndrome is to be started in the earliest time, because the earliest time, because the characteristic changes are formed characteristic changes are formed during 5-6 hours after trauma.during 5-6 hours after trauma.
If the response on diuresis stimulation is absent, you If the response on diuresis stimulation is absent, you should not prescribe furosemidum (lasix) or should not prescribe furosemidum (lasix) or mannitum one more time, because there is already mannitum one more time, because there is already tubular necrosis in kidneys. For saving such patient tubular necrosis in kidneys. For saving such patient there are needed haemoabsorbtion, haemodialisis. there are needed haemoabsorbtion, haemodialisis. Large attention is paid to simple and safe method of Large attention is paid to simple and safe method of detoxication – haemo- and lymphosorbtion. During detoxication – haemo- and lymphosorbtion. During sorbtions the content of potassium, magnesium, sorbtions the content of potassium, magnesium, phosphorum and some toxic substances is phosphorum and some toxic substances is decreased. During regional haemosorbtion there are decreased. During regional haemosorbtion there are absorbed “acid” metabolites.absorbed “acid” metabolites.
Crush syndrome of medium and high severity is an Crush syndrome of medium and high severity is an indication for haemosorbtion providing and indication for haemosorbtion providing and development of acute renal insufficiency – to start development of acute renal insufficiency – to start haemodialisis. During treatment of patients with haemodialisis. During treatment of patients with severe form of syndrome it is necessary to provide severe form of syndrome it is necessary to provide both procedures. Absorption helps to eliminate both procedures. Absorption helps to eliminate encephalopathy, improves general condition, but it encephalopathy, improves general condition, but it hardly changes level of urea and kreatinine in blood; hardly changes level of urea and kreatinine in blood; haemodialisis effectively eliminates hyperazotemia haemodialisis effectively eliminates hyperazotemia and hyperhydration. Haemodialisis must be early, and hyperhydration. Haemodialisis must be early, regular and individual depending on catabolism regular and individual depending on catabolism level; dangerous hyperkaliemia and hyperhydration level; dangerous hyperkaliemia and hyperhydration are absolute indications for “artificial kidney” usage.are absolute indications for “artificial kidney” usage.
Usage of hyperbaric oxygenation in complex Usage of hyperbaric oxygenation in complex therapy of crush syndrome helps to eliminate therapy of crush syndrome helps to eliminate blood hypoxia, increase quantity of blood hypoxia, increase quantity of thrombocytes, decrease intoxication, and thrombocytes, decrease intoxication, and improve kidneys’ function. Experience of improve kidneys’ function. Experience of early and wide usage of plasmapheresis in early and wide usage of plasmapheresis in complex treatment says about its high complex treatment says about its high effectiveness of liquidation of DIC-effectiveness of liquidation of DIC-syndrome, providing of organism’s syndrome, providing of organism’s detoxication.detoxication.
Early amputation is to be provided in Early amputation is to be provided in ischemia of limbs of III degree when ischemia of limbs of III degree when there is edema of injured limbs, there there is edema of injured limbs, there are absent all kinds of sensitivity, are absent all kinds of sensitivity, active and passive movements, active and passive movements, despite of kept arterial pulsation. You despite of kept arterial pulsation. You cannot amputate the limb on the place cannot amputate the limb on the place of catastrophe not freeing it, if time of of catastrophe not freeing it, if time of crush is less than 15 hours.crush is less than 15 hours.
From first stages of treatment systematic injection of From first stages of treatment systematic injection of highly effective antibiotics without nephrotoxic highly effective antibiotics without nephrotoxic properties is needed. Effective antibiotic properties is needed. Effective antibiotic prophylaxis may be by usage of equal combinations prophylaxis may be by usage of equal combinations of antibiotics, effective for most causative agents of of antibiotics, effective for most causative agents of wound infection. Combined antibiotic therapy is an wound infection. Combined antibiotic therapy is an important method of effective treatment important method of effective treatment improvement. During crush syndrome there is improvement. During crush syndrome there is recommended usage of two antibiotics combination recommended usage of two antibiotics combination because injection of more remedies may have not because injection of more remedies may have not desired consequences.desired consequences.
The most adequate in crush symdrome are such The most adequate in crush symdrome are such combinations of antibiotics:combinations of antibiotics:
1.1. Modern aminoglycosides (gentamycini sulfas, Modern aminoglycosides (gentamycini sulfas, tobramycinum, sizomycini sulfas, amykacinum) tobramycinum, sizomycini sulfas, amykacinum) with penicillines (benzylpenicillinum-natrium, with penicillines (benzylpenicillinum-natrium, ampicillinum, carbenicillinum, oxacillinum), ampicillinum, carbenicillinum, oxacillinum), cephalosporines (excluding ceporinum), cephalosporines (excluding ceporinum), macrolides (erythromycinum), tetracyclines macrolides (erythromycinum), tetracyclines (rondomycinum), antibiotics of different groups (rondomycinum), antibiotics of different groups (rifampicinum, linkomycinum, laevomycetinum).(rifampicinum, linkomycinum, laevomycetinum).
2.2. Polymixinum B combined with penicillines, Polymixinum B combined with penicillines, cephalosporines (excluding ceporinum), cephalosporines (excluding ceporinum), macrolides, tetracyclines, and antibiotics of macrolides, tetracyclines, and antibiotics of different groups.different groups.
For prophylaxis and fight with secondary For prophylaxis and fight with secondary immunodeficiency there might be used immunodeficiency there might be used immunomodulators like thymalinum, T-activinum, immunomodulators like thymalinum, T-activinum, immunoglobulines.immunoglobulines.
As a result of plasmorrhagia a hem concentration, As a result of plasmorrhagia a hem concentration, decreasing of chemical and osmotic erythrocyte decreasing of chemical and osmotic erythrocyte resistance, intracellular hemolisis and anemia resistance, intracellular hemolisis and anemia appear: very important is an indication of appear: very important is an indication of mioglobinemia, resistance of erythrocytes. mioglobinemia, resistance of erythrocytes. Processes of hem coagulation activate during the Processes of hem coagulation activate during the long-term smash tissue syndrome, the concentration long-term smash tissue syndrome, the concentration of heparin go down, but fibrinogen concentration of heparin go down, but fibrinogen concentration increases. Hyper coagulation aggravates reological increases. Hyper coagulation aggravates reological properties of blood. properties of blood.
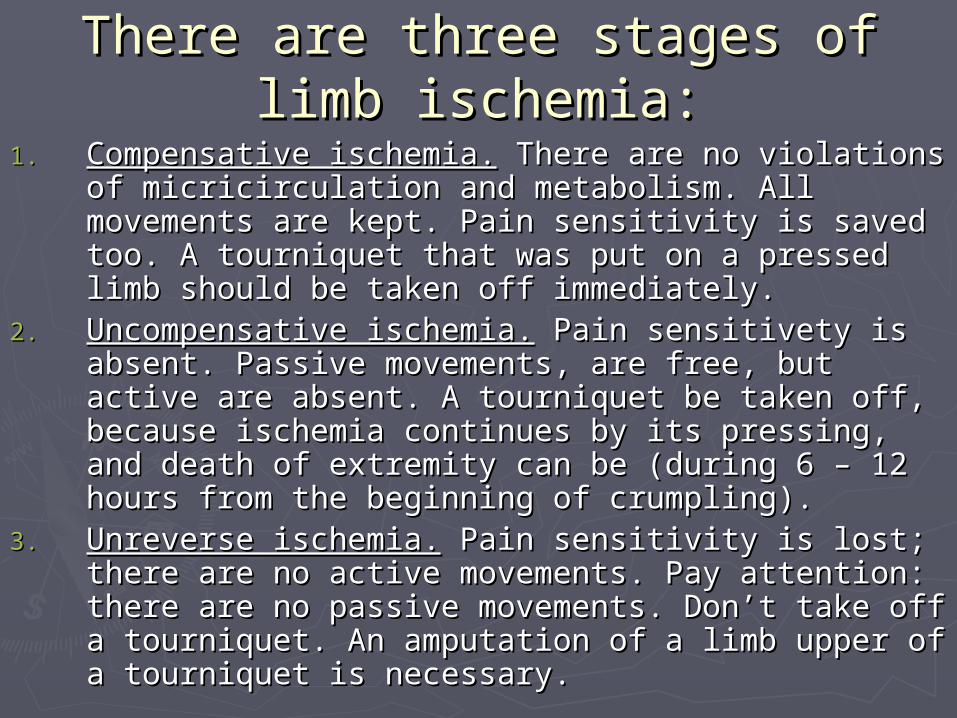
There are three stages of limb There are three stages of limb ischemiaischemia::
1.1. Compensative ischemia.Compensative ischemia. There are no violations of There are no violations of micricirculation and metabolism. All movements are kept. micricirculation and metabolism. All movements are kept. Pain sensitivity is saved too. A tourniquet that was put on a Pain sensitivity is saved too. A tourniquet that was put on a pressed limb should be taken off immediately.pressed limb should be taken off immediately.
2.2. Uncompensative ischemia.Uncompensative ischemia. Pain sensitivety is absent. Passive Pain sensitivety is absent. Passive movements, are free, but active are absent. A tourniquet be movements, are free, but active are absent. A tourniquet be taken off, because ischemia continues by its pressing, and taken off, because ischemia continues by its pressing, and death of extremity can be (during 6 – 12 hours from the death of extremity can be (during 6 – 12 hours from the beginning of crumpling).beginning of crumpling).
3.3. Unreverse ischemia.Unreverse ischemia. Pain sensitivity is lost; there are no Pain sensitivity is lost; there are no active movements. Pay attention: there are no passive active movements. Pay attention: there are no passive movements. Don’t take off a tourniquet. An amputation of a movements. Don’t take off a tourniquet. An amputation of a limb upper of a tourniquet is necessary.limb upper of a tourniquet is necessary.
Usage of pneumatic splint during crush-syndrome.
It’s necessary to distinguish in the crush syndrome a compression period.
The summaryThe summary► Long – term smash tissue syndrome which Long – term smash tissue syndrome which
arises after long – term crushing soft tissues of arises after long – term crushing soft tissues of limbs by destroyed buildings, stones, groundlimbs by destroyed buildings, stones, ground
► First aid: a/ Remove the compressing factor; First aid: a/ Remove the compressing factor; made the proximal tourniquet to prevent made the proximal tourniquet to prevent spreadingspreading of toxins for all organism; prescribe of toxins for all organism; prescribe the narcotic the narcotic analgeanalgetticics to prevent the formation s to prevent the formation of pain shockof pain shock
► Treatment – complex infusion therapy, and Treatment – complex infusion therapy, and sometimes sometimes AMPUTATION OF EXTREMITES AMPUTATION OF EXTREMITES
(the (the worse variant - worse variant - deathdeath))