Long case pregnancy with mitral stenosis sandeep kumar kar
80
Dr Sandeep Kumar Kar Dr Sandeep Kumar Kar RMO –CUM CLINICAL TUTOR RMO –CUM CLINICAL TUTOR {Cardiac Anesthesiology} {Cardiac Anesthesiology} I.P.G.M.E&R KOLKATA I.P.G.M.E&R KOLKATA PREGNANCY WITH PREGNANCY WITH MITRAL STENOSIS MITRAL STENOSIS ANESTHETIC ANESTHETIC CONSIDERATIONS CONSIDERATIONS (LONG CASE FORMAT) (LONG CASE FORMAT)
-
Upload
isakakinada -
Category
Healthcare
-
view
515 -
download
2
description
Pregnancy with MS
Transcript of Long case pregnancy with mitral stenosis sandeep kumar kar

Dr Sandeep Kumar KarDr Sandeep Kumar KarRMO –CUM CLINICAL TUTORRMO –CUM CLINICAL TUTOR{Cardiac Anesthesiology}{Cardiac Anesthesiology}
I.P.G.M.E&R KOLKATAI.P.G.M.E&R KOLKATA
PREGNANCY WITH PREGNANCY WITH MITRAL STENOSIS MITRAL STENOSIS
ANESTHETIC ANESTHETIC CONSIDERATIONS CONSIDERATIONS
(LONG CASE FORMAT)(LONG CASE FORMAT)

PARTICULARS OF THE PARTICULARS OF THE PATIENTPATIENT
Name – Mrs. XName – Mrs. X Age- 25 years.Age- 25 years. Sex-Female.Sex-Female. Religion-Humanity.(above all Religion-Humanity.(above all
religions)religions) Social status-Poor.Social status-Poor. Occupation-Housewife.Occupation-Housewife.

CHIEF COMPLAINTSCHIEF COMPLAINTS
• Patient is admitted with Patient is admitted with active labour pain at full active labour pain at full term for institutional delivery term for institutional delivery
• Shortness of breath for last 6 Shortness of breath for last 6 weeks.weeks.

HISTORY OF PRESENT HISTORY OF PRESENT ILLNESSILLNESS
The breathlessness gradually The breathlessness gradually progressive, exertional, non seasonal, progressive, exertional, non seasonal, grade III in severity.grade III in severity.
Cough not associated with any fever .Cough not associated with any fever . No H/O chest pain, swelling of leg, No H/O chest pain, swelling of leg,
syncope, squatting, pain in leg, syncope, squatting, pain in leg, neurodeficit.neurodeficit.
H/O acute respiratory distress in night 1 H/O acute respiratory distress in night 1 week back. week back.
contd..contd..

HISTORY OF PRESENT HISTORY OF PRESENT ILLNESS ILLNESS
• It is her first pregnancy.It is her first pregnancy.• She experienced only mild She experienced only mild
exertional dyspnea during her exertional dyspnea during her non pregnant state.non pregnant state.
• She was a diagnosed case of She was a diagnosed case of mitral stenosis since her early mitral stenosis since her early adult hood (15 yrs. Of age).adult hood (15 yrs. Of age).
• She had definite history of fever She had definite history of fever with joint pain in her childhood (5 with joint pain in her childhood (5 yrs of age).yrs of age).

Treament historyTreament history The patient was on Tab. Digoxin The patient was on Tab. Digoxin
(0.25mg) 1 OD for 5 days/week(0.25mg) 1 OD for 5 days/week Tab. Lasix (40mg) 1 bdTab. Lasix (40mg) 1 bd Syrup Pot chlor 2 tsf tdsSyrup Pot chlor 2 tsf tds prophylactic Inj. Penidura every prophylactic Inj. Penidura every
21 days.21 days.

PHYSICAL EXAMINATIONPHYSICAL EXAMINATION• GENERAL SURVEYGENERAL SURVEY
Pt. is alert, conscious and co-operative.Pt. is alert, conscious and co-operative. Build-Build- average,average, State of nutrition-State of nutrition- poor,poor, Decubitus-Decubitus- of choiceof choice,(preferably left lateral),(preferably left lateral) FaciesFacies- - normalnormal Pallor-Pallor- mildmild Icterus- Icterus- absentabsent Cyanosis-Cyanosis- absentabsent Clubbing-Clubbing- absent.absent.

GENERAL SURVEYGENERAL SURVEY
Pulse -Pulse - Rate-74/min,Rate-74/min, Rhythm-regular,Rhythm-regular, Volume- low,Volume- low, all peripheral pulses are all peripheral pulses are
palpable,palpable, condition of arterial wall-normal.condition of arterial wall-normal.
no radio radial or radio femoral no radio radial or radio femoral delaydelay
Blood pressure - Blood pressure - 100/76 mm of Hg.100/76 mm of Hg.

CVSCVS• InspectionInspection – – no deformityno deformity..• Palpation –Palpation – Apex beat in the left 5Apex beat in the left 5thth
ICS ½ inch in side the left MCL. ICS ½ inch in side the left MCL. Tapping in character.Tapping in character.
• Diastolic thrillDiastolic thrill is palpable in the is palpable in the mitral area which is best felt in left mitral area which is best felt in left lateral position at the end of lateral position at the end of expiration.expiration.
• Auscaltation – Auscaltation – S1-- short, sharp, S1-- short, sharp, accentuated. accentuated. S2 – audible. S2 – audible. P2 – P2 – Loud in pulmonary areaLoud in pulmonary area
contd…contd…

Opening snap heard just after S2.Opening snap heard just after S2. Low pitched mid diastolic rumbling Low pitched mid diastolic rumbling
murmur of intensity IV/VI with murmur of intensity IV/VI with presystolic accentuation in the presystolic accentuation in the mitral mitral area without any radiation. area without any radiation. Best heard with the bellBest heard with the bell of the of the stethoscope, in stethoscope, in left lateral positionleft lateral position, , at the at the height of expiration height of expiration and and after doing mild exercise. after doing mild exercise.

EXAMINATION OF RESPIRATORY EXAMINATION OF RESPIRATORY SYSTEMSYSTEM
Bilateral vesicular breath Bilateral vesicular breath sound.sound.
No adventitious sound.No adventitious sound.

EXAMINATION OF GASTROINTESTINAL EXAMINATION OF GASTROINTESTINAL SYSTEMSYSTEM
Abdomen -soft, 36 weeks as fundal Abdomen -soft, 36 weeks as fundal
heightheight -umbilicus central in -umbilicus central in
position.position. -no other palpable lump, -no other palpable lump, -fluid shift-absent.-fluid shift-absent. -peristaltic sound-present. -peristaltic sound-present.

EXAMINATION OF NERVOUS SYSTEMEXAMINATION OF NERVOUS SYSTEM::
No tremor, muscle wasting.No tremor, muscle wasting. Power + TonePower + Tone upper limb-right-normal. upper limb-right-normal. -left-normal.-left-normal. lower limb-right-normal.lower limb-right-normal. -left-normal.-left-normal. Deep tendon reflexes-normal.Deep tendon reflexes-normal.
Examination of cranial nerves-normal.Examination of cranial nerves-normal.

Obstetrical examinationObstetrical examination
Uterine size – 36 wks.Uterine size – 36 wks. Position – left occipito-Position – left occipito-
anterioranterior FHS – 160/min.FHS – 160/min.

AIRWAY EXAMINATIONAIRWAY EXAMINATION::
• Mouth opening-3 fingers.Mouth opening-3 fingers.
• No loose tooth/artificial denture.No loose tooth/artificial denture.• Mallampati- grade II.Mallampati- grade II.
• Thyromental distance-6 fingers.Thyromental distance-6 fingers.• Neck movement-within normal limits.Neck movement-within normal limits.

PROVISIONAL DIAGNOSISPROVISIONAL DIAGNOSIS::
Mitral stenosis of rheumatic Mitral stenosis of rheumatic origin without any evidence of origin without any evidence of congestive heart failure and in congestive heart failure and in sinus rhythm in a primi para sinus rhythm in a primi para term mother posted for CS. term mother posted for CS.

Etiology of MS Etiology of MS • Almost always rheumatic in our setting.Almost always rheumatic in our setting.• Rarely congenital, SLE, carcinoid Rarely congenital, SLE, carcinoid
syndrome, endocarditis, CVD, syndrome, endocarditis, CVD, mucopolysccharoidosis.mucopolysccharoidosis.
• Pure MS approximately in 40% Pure MS approximately in 40% rheumatic heart disease.rheumatic heart disease.
• Two – third of the all MS pt. are female.Two – third of the all MS pt. are female.• Time gap of development symptoms Time gap of development symptoms
from rheumatic fever – two decade in from rheumatic fever – two decade in developed country but 5 – 15 yrs in developed country but 5 – 15 yrs in developing countrydeveloping country..

PathologyPathology• Valve leaflets are diffusely thickenedValve leaflets are diffusely thickened• Mitral commisure and cordae Mitral commisure and cordae
tendineae fused and shorten, valve tendineae fused and shorten, valve cusp become rigid –cusp become rigid – fish mouth valve. fish mouth valve.
• Initial insult is rheumatic but later Initial insult is rheumatic but later changes may be a process resulting changes may be a process resulting from trauma to the valve caused by from trauma to the valve caused by altered flow pattern due to initial altered flow pattern due to initial deformity.deformity.
• Thrombus formation and arterial Thrombus formation and arterial embolisation can occur.embolisation can occur.

Mitral stenosisMitral stenosisPathophysiologyPathophysiology
Mitral valve area (MVA):Mitral valve area (MVA):
Normal Normal 4 -- 6 sq. cm 4 -- 6 sq. cm Mild MS Mild MS 1.5 – 2.5 sq. cm 1.5 – 2.5 sq. cm Moderate MS Moderate MS 1.1– 1.5 sq. cm 1.1– 1.5 sq. cm Severe MS Severe MS <1 sq. cm <1 sq. cm Critical MS Critical MS < 0.6 sq. cm< 0.6 sq. cm

Mitral stenosisMitral stenosisPathophysiologyPathophysiology
Diastolic trans-mitral pressure Diastolic trans-mitral pressure gradient: gradient:
Mild MS -- <5 mm Hg.Mild MS -- <5 mm Hg. Moderate MS – 5 –12 mm Hg.Moderate MS – 5 –12 mm Hg. Severe MS -- > 12 mm Hg.Severe MS -- > 12 mm Hg.

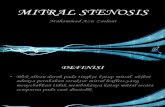
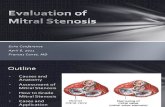
PATHOPHYSIOLOGYPATHOPHYSIOLOGYMITRAL STENOSIS
Obstruction to LA emptying ↓LV filling
↑LA pressure↑LA size
↑pulm venous pressure
↑pulm artery pressure
↓COPulm HTN
↑pulm vas resistance
RV overload
TR
Perivascular edema, Pulm. Pulm.
Arteriolar constriction, Arteriolar constriction, organic organic
obliterative changes in obliterative changes in the the
pulm vascular bedpulm vascular bedObstruction to pulm blood flow
↓lung compliance↑work of breathing


Mitral stenosisMitral stenosisPathophysiologyPathophysiology
• MVA < 2 sq. cm MVA < 2 sq. cm increased increased pressure gradient between LA & LV pressure gradient between LA & LV in diastole.in diastole.
• Increased pressure gradient across Increased pressure gradient across MV – with decreased MVA or with MV – with decreased MVA or with increased flow across MV.increased flow across MV.
• Increased flow across MV Increased flow across MV increasing pressure gradient in an increasing pressure gradient in an exponential manner exponential manner ( as pressure ( as pressure gradient varies with the square of gradient varies with the square of the flow).the flow).
• Therefore, exercise and pregnancy Therefore, exercise and pregnancy (increased blood volume & thus (increased blood volume & thus increased flow) can cause significant increased flow) can cause significant increase in LA pressureincrease in LA pressure. .

Mitral stenosisMitral stenosisPathophysiologyPathophysiology
Increased HR (sinus tachycardia, AF) Increased HR (sinus tachycardia, AF) shortened diastolic filling period shortened diastolic filling period diminished time for LA emptying diminished time for LA emptying increased pressure gradient across increased pressure gradient across MV and increased LA pressure.MV and increased LA pressure.
AF – additionally causes loss of AF – additionally causes loss of ‘atrial kick’(contributes 30% to LV ‘atrial kick’(contributes 30% to LV filling) filling) further reduction of LV further reduction of LV filling filling reduced cardiac out put. reduced cardiac out put.

Mitral stenosisMitral stenosisPathophysiologyPathophysiology
• Increased LA pressure Increased LA pressure increased increased pulmonary venous, capillary, arterial pulmonary venous, capillary, arterial pressure pressure risk of pulmonary edema. risk of pulmonary edema.
• Persistently elevated pulmonary arterial Persistently elevated pulmonary arterial pressure (pulmonary hypertension, PAH) pressure (pulmonary hypertension, PAH) increased RV after load increased RV after load RVH RVH RVF RVF right sided CHF.right sided CHF.
• LV function is normal in most patients of LV function is normal in most patients of MS but poor LV function may be seen in MS but poor LV function may be seen in 25% of patients 25% of patients because of LV fibrosis in because of LV fibrosis in longstanding MS.longstanding MS.

Is LV function normal in Is LV function normal in mitral stenosis mitral stenosis (controversy)(controversy)
According to Bolen etal. According to Bolen etal. Fibrosis of the myocardium Fibrosis of the myocardium
secondary to rheumatic fever in secondary to rheumatic fever in the posterobasal region of the the posterobasal region of the ventricle may be responsible for ventricle may be responsible for SWMA and decreased systolic SWMA and decreased systolic function.function.

Is LV function normal in Is LV function normal in mitral stenosis mitral stenosis (controversy)(controversy)
Gash etal Gash etal “ Under loaded “ Under loaded ventricle’s fixed stroke volume ventricle’s fixed stroke volume activates a reflex sympathetic activates a reflex sympathetic response and increases the SVR response and increases the SVR thereby decreasing the ejection thereby decreasing the ejection phase indices.”phase indices.”
““Inotropically normal myocardium is Inotropically normal myocardium is simultaneously under loaded( ms) simultaneously under loaded( ms) and afterload stressed(high SVR) and afterload stressed(high SVR) that is afterload mismatched.”that is afterload mismatched.”

Modified New York Association Modified New York Association Functional Classification of Heart Functional Classification of Heart
DiseaseDisease..
Class I: Asymptomatic except Class I: Asymptomatic except during severe exertion.during severe exertion.
Class II: Symptomatic with Class II: Symptomatic with moderate activity. moderate activity.
Class III: Symptomatic with Class III: Symptomatic with minimal activity. minimal activity.
Class IV: Symptomatic at rest.Class IV: Symptomatic at rest.

Age - usually younger population < 12 yrsSex – F (66 %) > M (34 %)Symptoms: 1. SOB – commonest (in mild MS, by sudden change in
HR, vol-status, or CO e.g. severe exertion, excitement, fever, severe anemia, paroxysmal AF or other Tachycardia, Preg, thyrotoxicosis. As MS progress, lesser stress ppt. dyspnea & also orthopnea, PND)
2. Palpitations, 3. Cough, 4. Haemoptysis (from rupture of pulm. Bronchial venous
connections 2ndary to PVH/ never fatal ), 6. Attacks of ac. Resp. distress ( pulm. edema) cont.

Atypical presentationsAtypical presentations
• Atypical anginaAtypical angina, , Chest pain in 10–Chest pain in 10–15% of pts, even 15% of pts, even in the absence of in the absence of atherosclerosis;atherosclerosis; etiology often etiology often remains unexplained but may be remains unexplained but may be emboli in the coronary circulation or emboli in the coronary circulation or ac. RV pr. overload.ac. RV pr. overload.
• Pts may developPts may develop hoarseness hoarseness as a as a
result of compression of the lt. result of compression of the lt. recurrent laryngeal nv. by the recurrent laryngeal nv. by the enlarged LA enlarged LA (Oatner syndrome )(Oatner syndrome )

• LV function is normal in the majority LV function is normal in the majority with pure MS, but with pure MS, but impaired LV impaired LV functionfunction may be encountered in may be encountered in up up to 25%to 25% of pts & of pts & presumably presumably represents residual damage from represents residual damage from rheumatic myocarditis or coexistent rheumatic myocarditis or coexistent hypertensive or IHD.hypertensive or IHD.
• 9.9.Malar flushMalar flush in face (pinched & in face (pinched & blue facies).rare in indians blue facies).rare in indians
• 10.10.Repeated pulm. Infection.Repeated pulm. Infection.

ExaminationGeneral DECUBITUSDECUBITUS: may be orthopnoeic: may be orthopnoeicCYANOSIS: Present in severe MS with ac. pulm. CYANOSIS: Present in severe MS with ac. pulm.
edemaedemaOEDEMAOEDEMA: Bilateral pedal edema, accentuated in : Bilateral pedal edema, accentuated in
CCFCCFNECK VEIN: Engorged in CCFNECK VEIN: Engorged in CCF Prominent ‘a’ wave in pulm. HTNProminent ‘a’ wave in pulm. HTN1. Pulse - low volume. Rhythm- usually regular, Rhythm- usually regular,
irregular in AFirregular in AF2. BP: usually low. BP: usually low. Cold extremities.3.3. RESPIRATION: may be tachypnoeic RESPIRATION: may be tachypnoeic3. Engorged pulsatile neck veins, pedal edema,
tender hepatomegaly (Signs of RV failure). In pt. with sinus rhythm & severe PH or associated TR, JVP reveals prominent ‘a’ wave due vigorous rt. atrial contraction && a a gradual pr. gradual pr. ddecline after MV opening ecline after MV opening (Y-(Y-descent).descent).

SystemicSystemic CVS- CVS- InspectionInspection-- no deformity of precordium, no deformity of precordium, - no venous prominence seen, - no venous prominence seen, - visible pulm. Art. pulsation in - visible pulm. Art. pulsation in
left 2nd ICS in left 2nd ICS in pulm. HTN.pulm. HTN.PALPATION:PALPATION: **Apex beat- Apex beat- Lt 4th ICS, Lt 4th ICS,
outside MCL, tapping in character. outside MCL, tapping in character. *Thrill- *Thrill- Diastolic thrill over apical area, Diastolic thrill over apical area,
best palpable in left lateral position at best palpable in left lateral position at the height of exp.the height of exp.
**Left parasternal heave- Left parasternal heave- in pulmonary in pulmonary HTN.HTN.
*Left parasternal impulse (rt *Left parasternal impulse (rt ventricular tap). ventricular tap).
*Palpable S2*Palpable S2

Auscultation- S1- short, sharp, accentuated Opening snap - - audible just after S2 (just medial to apex) Mitral area- low pitched mid-diastolic rumbling murmur with presystolic accentuation of varying intensity without any radiation and best heard in left lateral position at the height expiration with the bell of the stethoscope. Pulmonary area- Pulmonary ejection click with ejection systolic murmur in pulmonary pulmonary HTNHTN (due to relative obstruction).(due to relative obstruction).•P2 accentuated•Closely split S2 •Systolic murmur - due to TR following RV dilatation

Pulmonary changesPulmonary changes
VC, TLC, Max breathing capacity VC, TLC, Max breathing capacity & O2 uptake /unit of ventilation – & O2 uptake /unit of ventilation – may reduced. may reduced.
Also the elevated pulm. Venous Also the elevated pulm. Venous pr. & PAWP: ↓ Cpr. & PAWP: ↓ CL L , contribute to , contribute to exertional dyspnea.exertional dyspnea.

Clinical assessment of Clinical assessment of severityseverity
• Assessing the AAssessing the A22 - OS gap. - OS gap.
• Assessing the severity of PAH.Assessing the severity of PAH.
• duration of the diastolic murmur.duration of the diastolic murmur.

ECGECG
LA enlargement – wide and LA enlargement – wide and notched P wave (P mitrale) – notched P wave (P mitrale) – most prominent in lead IImost prominent in lead II
RVHRVH Right axis deviationRight axis deviation f wave replacing P wave if atrial f wave replacing P wave if atrial
fibrillation developsfibrillation develops

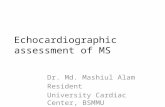
CXRCXR• Slight increase in the transverse diam. of Slight increase in the transverse diam. of
heartheart• Straightening of the left border of heartStraightening of the left border of heart• Double contour of the right border of Double contour of the right border of
heartheart• Evidence of PAH- dilated pulmonary Evidence of PAH- dilated pulmonary
artery at hilum with peripheral prunningartery at hilum with peripheral prunning• Dilatation of upper lobe pulmonary veinDilatation of upper lobe pulmonary vein• Kerly’s B lineKerly’s B line• Mitral valve calcificationMitral valve calcification• Elevation of left upper lobe bronchusElevation of left upper lobe bronchus• Multiple opacities due to hemosiderosis Multiple opacities due to hemosiderosis

Lt. Border - Lt. Border - Auricular Auricular appendage of LA. appendage of LA. But mainly by LV.But mainly by LV.
Rt. Border – RARt. Border – RA
In MS: hypoplastic aortic knuckleenlarged pulmonary bayLA enlargementReduced LV size

Cephalization
Straightening of left heart

Convexity from enlarged left atrial appendage

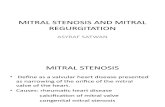
Echocardiogram
•Transvalvular peak & mean gradient•Mitral orifice size •Presence and severity of MR•Extent of restriction of valve leaflets •Degree of distortion of subvalvular apparatus•Anatomic suitability of percutaneous mitral balloon valvotomy (PMBV).•Asses the ventricular chamber, LV function, PAP
[TEE is superior & use when TTE is inadequate. TEE is especially indicated to exclude atrial thrombi before PMBV].

Modified Duckett Jones Modified Duckett Jones criteria for diagnosing criteria for diagnosing Rheumatic heart diseaseRheumatic heart disease

Major criteria• Carditis• Arthritis• Subcutaneous nodules• Chorea• Erythema Marginatum
Minor Criteria• Clinical-
FeverArthralgia
• Laboratory - Acute phase reactants Prolonged PR interval in ECG

Essential criteria
Evidence for recent streptococcal infection as indicated by•Increased ASO titer (> 250 todd units in west bengal)•Positive throat culture•Recent scarlet fever
Diagnosis consists of :Essential criteria + 2 major/ 1 major + 2 minor criteria

Why does pregnancy Why does pregnancy aggravate the symptoms of aggravate the symptoms of
mitral stenosis?mitral stenosis? Decrease in Decrease in SVRSVR Increase in HR 10-20 beats/min – Increase in HR 10-20 beats/min –
reduced diastolic filling time of LVreduced diastolic filling time of LV Increase in CO by 30-50% Increase in CO by 30-50% - increase - increase
in transvalvular gradient – rise in LA in transvalvular gradient – rise in LA pressure pressure
Increase in blood volume by 30-Increase in blood volume by 30-50% 50% -increase in capillary -increase in capillary hydrostatic pressure – pulmonary hydrostatic pressure – pulmonary edema.edema.

Why does pregnancy Why does pregnancy aggravate the symptoms of aggravate the symptoms of
mitral stenosis?mitral stenosis? During labour and delivery During labour and delivery
sympathetic stimulation – sympathetic stimulation – rise in rise in HR and COHR and CO
Sudden rise in venous return Sudden rise in venous return due due to auto transfusion and IVC to auto transfusion and IVC compression –decompensationcompression –decompensation

Why does pregnancy Why does pregnancy aggravate the symptoms of aggravate the symptoms of
mitral stenosis?mitral stenosis?
Atrial enlargement in pregnancy Atrial enlargement in pregnancy – atrial fibrilation– atrial fibrilation
Hypercoagulability – Hypercoagulability – thromboembolic riskthromboembolic risk
During pregnancy pts During pregnancy pts symptomatic status increases by symptomatic status increases by 1 or 2 NYHA class. 1 or 2 NYHA class.

Just thinkJust think
Why tachycardia is detrimental to
the patient?

• According to Gorlin formula: According to Gorlin formula: Pr. Pr. gradient across valve is proportional gradient across valve is proportional to the square of blood flowto the square of blood flow
• Flow = CO / diastolic filling timeFlow = CO / diastolic filling time• Tachycardia (↓ diastolic filling time) Tachycardia (↓ diastolic filling time)
increases increases the pressure gradient by the pressure gradient by the square of the original value.the square of the original value.
• Acute elevation of LAP is rapidly Acute elevation of LAP is rapidly transmitted back to the pulm. transmitted back to the pulm. capillaries.capillaries.
• If pulm. capillary pr. rises above 25 If pulm. capillary pr. rises above 25 mm Hg, mm Hg, transudation of capillary fluid transudation of capillary fluid results in pulm. edema.results in pulm. edema.

In shortIn short↑↑HR→ ↓diastolic HR→ ↓diastolic filling time→ ↑flow → filling time→ ↑flow → ↑pr. gradient across ↑pr. gradient across mitral valve → ↑LAP mitral valve → ↑LAP → pulm. edema.→ pulm. edema.

Therapeutic ApproachTherapeutic Approach Therapeutic approach is to Therapeutic approach is to
reduce the heart rate and reduce the heart rate and decrease left atrial pressuredecrease left atrial pressure– Restrict physical activityRestrict physical activity– Restrict salt intake Restrict salt intake – diureticsdiuretics– Beta blockersBeta blockers– Digoxin (if patient is Digoxin (if patient is in a. fib)in a. fib)

During pregnancy clinical and During pregnancy clinical and echocardiographic follow up echocardiographic follow up to be done to be done at 3 and 5 months at 3 and 5 months and every months thereafterand every months thereafter
In pt unresponsive to medical In pt unresponsive to medical therapy therapy PMC/BMV PMC/BMV to be to be considered considered after 20after 20thth week week of of gestationgestation

CMC during pregnancy still CMC during pregnancy still practised in developing worldpractised in developing world
CPB during pregnancy risk is CPB during pregnancy risk is same to mother as non same to mother as non pregnant state pregnant state but fetal but fetal mortality is high. mortality is high.

Anti coagulationAnti coagulation Indications for anticoagulationIndications for anticoagulation
Patient with AF(> 48 hrs)Patient with AF(> 48 hrs)Prior embolic eventPrior embolic eventSevere MS with left atrial dimension 55 Severe MS with left atrial dimension 55
mm on ECHOmm on ECHO Heparin for first trimesterHeparin for first trimester Warfarin 12-36 weeksWarfarin 12-36 weeks After 36 weeks changed to After 36 weeks changed to
heparin titrated to APTT levelheparin titrated to APTT level

Anaesthesia management – Anaesthesia management – Principles Principles
• Maintain sinus rhythm Maintain sinus rhythm and prevent rapid and prevent rapid ventricular rates. ventricular rates.
• Atrial fibrillation Atrial fibrillation and tachycardia can and tachycardia can also precipitate worsening cardiac also precipitate worsening cardiac function. Aggressively treat new onset function. Aggressively treat new onset atrial fibrillation pharmacologically or atrial fibrillation pharmacologically or with with direct cardioversion especially in direct cardioversion especially in the hemodynamically compromised the hemodynamically compromised patient .patient .
• Avoid large, rapid falls in SVR. Avoid large, rapid falls in SVR. This is This is compensated for by increasing HR, which compensated for by increasing HR, which can worsen cardiac function.can worsen cardiac function.

Prevent increases in central blood Prevent increases in central blood volumevolume. Careful fluid management . Careful fluid management and diuresis may be necessary.and diuresis may be necessary.
Avoid factors that may increase Avoid factors that may increase pulmonary artery pressure (PAP). pulmonary artery pressure (PAP). Prostaglandins, Prostaglandins, which may be which may be useful in treating uterine atony,useful in treating uterine atony, can precipitate increases in can precipitate increases in pulmonary vascular pressure.pulmonary vascular pressure.
LA filling to be kept high, but LA filling to be kept high, but pulmonary edema to be avoided. pulmonary edema to be avoided. PA pressure monitoring desirable.PA pressure monitoring desirable.


Effects of altered Effects of altered hemodynamicshemodynamics
Adverse effects
Result Mechanism
Bradycardia CO Low cardiac output
Tachycardia CO filling time AF CO LV
filling/no atrial kick
Preload CO LV filling SVR CO stroke
volume SVR CO SV (due to
tachycardia related filling time)

Anesthetic optionAnesthetic option• Evidence-based data on the ideal Evidence-based data on the ideal
anesthetic and analgesic for the anesthetic and analgesic for the parturient with MS is lacking.parturient with MS is lacking. Management must be Management must be individualized to individualized to optimize patient outcome. optimize patient outcome.
• The degree of monitoring should be The degree of monitoring should be based on the based on the severity of the disease and severity of the disease and the parturient”:s condition.the parturient”:s condition.
• The concomitant use of invasive The concomitant use of invasive hemodynamic monitorshemodynamic monitors is recommended is recommended in symptomatic parturients with critical in symptomatic parturients with critical stenosisstenosis..

Analgesia Analgesia
• It is important to It is important to minimize pain minimize pain and catecholamine release during and catecholamine release during labor.labor.
• A carefully titrated A carefully titrated EpiduralEpidural for for labor and delivery addresses all labor and delivery addresses all the desired hemodynamic goals.the desired hemodynamic goals.

Hemodynamic advantages Hemodynamic advantages of epidural anesthesiaof epidural anesthesia
• Epidural analgesia Epidural analgesia during the first during the first stage of labor canstage of labor can
• reduce PVR and SVR, reduce PVR and SVR, • lower PAP, andlower PAP, and• decrease CO to baseline levels.decrease CO to baseline levels.• Rapid prehydration should be avoidedRapid prehydration should be avoided..• slow titration of local anesthetic slow titration of local anesthetic
solution solution is recommended to minimise is recommended to minimise hemodynamic changes.hemodynamic changes.

Phenylephrine or Phenylephrine or ephedrine?ephedrine?
Unresolved controversyUnresolved controversy When treating hypotensionWhen treating hypotension, ,
phenylephrine is preferred over phenylephrine is preferred over ephedrine as ephedrine may ephedrine as ephedrine may increase the HR. increase the HR.
Epinephrine-containing local Epinephrine-containing local anesthetic solutions are best anesthetic solutions are best avoidedavoided due to concerns about due to concerns about potential tachycardia.potential tachycardia.

Evidences and logicEvidences and logic Ephedrine and dopamine act on the CV Ephedrine and dopamine act on the CV
system in a manner almost exactly system in a manner almost exactly reciprocal to the effects of sympathectomy reciprocal to the effects of sympathectomy associated with high spinal or epidural associated with high spinal or epidural anesthesiaanesthesia (Butterworth JFT, Austin JC, Johnson MD, et al. Effect of total (Butterworth JFT, Austin JC, Johnson MD, et al. Effect of total spinal anesthesia on arterial and venous responses to dopamine and dobuta-spinal anesthesia on arterial and venous responses to dopamine and dobuta-
mine. Anesth Analg 1987;66(3):209–214.)mine. Anesth Analg 1987;66(3):209–214.)
Phenylephrine also increases peripheral Phenylephrine also increases peripheral vascular resistance and decreases venous vascular resistance and decreases venous capacitance, but capacitance, but unlike ephedrine or unlike ephedrine or dopamine, it has minimal effects on dopamine, it has minimal effects on myocardial contractility and heart rate.myocardial contractility and heart rate.

Evidences contd…Evidences contd… Placental vessels are usually maximally Placental vessels are usually maximally
dilated so placental perfusion is highly dilated so placental perfusion is highly dependent on maternal BP.dependent on maternal BP.
Phenylephrine induced Phenylephrine induced vasoconstriction of placental vessel is vasoconstriction of placental vessel is not clinically significant because of not clinically significant because of large vascular reserve in a normal large vascular reserve in a normal placenta.placenta.
Moran DH, Perillo M, La Porta RF, et al. Phenylephrine in the prevention of Moran DH, Perillo M, La Porta RF, et al. Phenylephrine in the prevention of hypotension following spinal anesthesia for cesarean deliery. J Clin Anesth hypotension following spinal anesthesia for cesarean deliery. J Clin Anesth 1991;3(4):301–3051991;3(4):301–305..

The best strategy:The best strategy:
Combined spinal–epidural (CSE) Combined spinal–epidural (CSE) with an intrathecal opioid with an intrathecal opioid combined with a dilute epidural combined with a dilute epidural infusion minimizes sympathetic infusion minimizes sympathetic block and concomitant block and concomitant hypotension may be a good hypotension may be a good option.option.

Considerations in GAConsiderations in GA• If GA is required, avoid drugs that If GA is required, avoid drugs that
produce tachycardia such as produce tachycardia such as atropine, pancuronium, ketamine, atropine, pancuronium, ketamine, and meperidine.and meperidine.
• Vasodilating induction agents Vasodilating induction agents and volatile agents to be used and volatile agents to be used with great caution, as these tend with great caution, as these tend to to reduce SVR greatly.reduce SVR greatly.
• Nitrous oxide to be avoided in Nitrous oxide to be avoided in established PAH.established PAH.

Best GA StrategyBest GA Strategy• High dose narcotic (fentanyl 25 -30 High dose narcotic (fentanyl 25 -30
mcg/kg)+ muscle relaxant (avoid mcg/kg)+ muscle relaxant (avoid pancuronium) + ventilation with air-pancuronium) + ventilation with air-oxygen mixture is a preferred option.oxygen mixture is a preferred option.
• Remifentanil may be the preferred Remifentanil may be the preferred opioid in the peripartum setting due to opioid in the peripartum setting due to its short context-sensitive half-life its short context-sensitive half-life
• Neonatal resuscitation should be ready Neonatal resuscitation should be ready in hand.in hand.

Post- operative care Post- operative care • The The intrapartum and immediate intrapartum and immediate
postpartum postpartum periods are high risk as periods are high risk as the PCWP increases in the presence of the PCWP increases in the presence of severe MS (functional class III and IV).severe MS (functional class III and IV).
• Postoperative ventilation and Postoperative ventilation and intensive care may be necessary.intensive care may be necessary.
• The The lowest possible dose of uterotonic lowest possible dose of uterotonic agent agent is recommended as it may is recommended as it may produce significant adverse produce significant adverse cardiovascular effects. cardiovascular effects.

• Patients may need inotropic Patients may need inotropic support as well as a pulmonary support as well as a pulmonary vasodilator such as nitroglycerin vasodilator such as nitroglycerin or sodium nitroprusside .or sodium nitroprusside .(Milrinone can be a good option).(Milrinone can be a good option).
• In the appropriate patient, C/S In the appropriate patient, C/S may be followed by immediate may be followed by immediate corrective surgery, for example corrective surgery, for example closed mitral valvotomy..closed mitral valvotomy..

Are prophylactic antibiotics Are prophylactic antibiotics needed?needed?
The use of prophylactic antibiotics is not The use of prophylactic antibiotics is not recommended for an uncomplicated recommended for an uncomplicated elective cesarean delivery in a woman elective cesarean delivery in a woman who is not in labor and has intact who is not in labor and has intact membranes. membranes.
Indicated for procedures that cause Indicated for procedures that cause bacteremia when the patients are at bacteremia when the patients are at increased risk of I.E due to surgically increased risk of I.E due to surgically constructed systemic – pulmonary shunts constructed systemic – pulmonary shunts prosthetic valves RHD or previous I.Eprosthetic valves RHD or previous I.E

ASRA guidelineASRA guideline

THANK YOUTHANK YOUTHANK YOU FOR YOUR PATIENCE