London New Drugs Group / London Medicines Evaluation ... · London New Drugs Group / London...
12
1 London New Drugs Group / London Medicines Evaluation Network Dolutegravir January 2014 Summary Dolutegravir will be the third integrase inhibitor (INI) to be launched in the UK and the first stand-alone INI with once-daily dosing, with no need for a pharmacokinetic booster. Efficacy and safety have been evaluated in five phase 3 studies. In treatment-naïve patients, efficacy and safety of dolutegravir was shown to be comparable to that of raltegravir, superior to that of boosted darunavir and superior to that of Atripla when combined with ABC/3TC, with respect to the number of patients achieving an HIV-1 RNA level <50 copies/mL. Dolutegravir was more effective with a TDF/FTC backbone than with an ABC/3TC backbone by week 96, with respect to the proportion of patients achieving HIV-1 RNA <50c/mL. In treatment-experienced, INI-naive patients, dolutegravir was superior to raltegravir with respect to the number of patients achieving an HIV-1 RNA level <50 copies/mL. In treatment-experienced patients with INI- resistance, dolutegravir was highly effective in reducing viral load to <50 copies/mL. Dolutegravir was well tolerated, with few patients discontinuing therapy due to adverse effects. Dolutegravir does not inhibit CYP1A2, CYP2B6 or CYP3A4 and would not be expected to affect the pharmacokinetics of drugs that are substrates of these enzymes. 1. Background and introduction Integration of viral DNA into the host chromosome is a vital process in the HIV replication cycle. Key steps are carried out by the viral enzyme integrase, which, along with protease and reverse transcriptase, are encoded by HIV. 1 Dolutegravir is the third HIV integrase strand transferase inhibitor (INI) and the first stand-alone INI with once-daily dosing that does not require boosting with a pharmacokinetic enhancer. 2 British HIV Association (BHIVA) guidelines (2012) recommend that therapy-naive patients start ART containing two nucleotide reverse transcriptase inhibitor (NRTIs) plus one of the following: a ritonavir-boosted protease inhibitor (PI/r), an NNRTI or an integrase inhibitor (INI). 3 BHIVA recommend patients with triple-class resistance switch to a new ART regimen containing at least two and preferably three fully active agents with at least one active PI/r such as darunavir/r (DRV/r) or tipranavir/ ritonavir (TPV/r) and one agent with a novel mechanism (CCR5 receptor antagonist or integrase/fusion inhibitor) with etravirine (ETV) an option based on viral susceptibility. 3 2. Proposed place in therapy ViiV Healthcare anticipates that dolutegravir will be used as first-line therapy in treatment-naïve patients or treatment- experienced, integrase-inhibitor naive patients. Dosing in adults is as follows: 4 Treatment-naïve or treatment-experienced INI-naïve: 50mg once daily. Treatment-naïve or treatment-experienced INI-naïve when co-administered with the following potent UGT1A/CYP3A inducers: efavirenz, fosamprenavir/ritonavir, tipranavir/ritonavir, or rifampicin: 50mg twice daily. INI-experienced with certain INI-associated resistance substitutions or clinically suspected INI resistance: 50mg twice daily. Patients without INI resistance may take DTG with or without food. In the presence of integrase class resistance, DTG should preferably be taken with food to enhance exposure (particularly in patients with Q148 mutations). 5 If efavirenz, fosamprenavir/ritonavir, tipranavir/ritonavir or rifampicin is co-administered, the dose is 50 mg twice daily. Dosing in treatment-naïve or treatment-experienced INI-naïve children aged 12 years and older and weighing at least 40kg is 50mg once daily. 3. Evidence selected for inclusion There are five phase 3 studies in adults; these were identified by a literature search and from information provided by ViiV Healthcare. Three studies have been in treatment-naïve adults: SPRING-2 compared dolutegravir once daily (OD) with raltegravir twice daily (BD) 6;7 , SINGLE compared dolutegravir OD + Kivexa with Atripla 8;9 and FLAMINGO compared dolutegravir OD with darunavir boosted with ritonavir 10 . Two have been in treatment experienced patients: SAILING compared dolutegravir 50mg OD with raltegravir in treatment experienced, integrase naive patients while VIKING-3 assessed the efficacy of dolutegravir 50mg BD in highly treatment experienced patients with resistance to multiple antiretroviral (ARV) classes including integrase inhibitors. 11;12 SPRING-2, SINGLE and SAILING have been fully published. All studies were sponsored by ViiV Healthcare. There is also an on-going phase 1/2 open-label, pharmacokinetic study (IMPAACT) in paediatrics. 13;14 Treatment - naïve adults SPRING-2 SPRING-2 is a 96-week, randomised, double-blind, active-controlled, non-inferiority study in treatment-naïve adults (85%
Transcript of London New Drugs Group / London Medicines Evaluation ... · London New Drugs Group / London...

1
London New Drugs Group / London Medicines Evaluation Network
Dolutegravir
January 2014
Summary Dolutegravir will be the third integrase inhibitor (INI) to be launched in the UK and the first stand-alone INI with once-daily
dosing, with no need for a pharmacokinetic booster.
Efficacy and safety have been evaluated in five phase 3 studies.
In treatment-naïve patients, efficacy and safety of dolutegravir was shown to be comparable to that of raltegravir, superior to that of boosted darunavir and superior to that of Atripla when combined with ABC/3TC, with respect to the number of patients achieving an HIV-1 RNA level <50 copies/mL.
Dolutegravir was more effective with a TDF/FTC backbone than with an ABC/3TC backbone by week 96, with respect to the proportion of patients achieving HIV-1 RNA <50c/mL.
In treatment-experienced, INI-naive patients, dolutegravir was superior to raltegravir with respect to the number of patients achieving an HIV-1 RNA level <50 copies/mL.
In treatment-experienced patients with INI- resistance, dolutegravir was highly effective in reducing viral load to <50 copies/mL.
Dolutegravir was well tolerated, with few patients discontinuing therapy due to adverse effects.
Dolutegravir does not inhibit CYP1A2, CYP2B6 or CYP3A4 and would not be expected to affect the pharmacokinetics of drugs that are substrates of these enzymes.
1. Background and introduction Integration of viral DNA into the host chromosome is a vital process in the HIV replication cycle. Key steps are carried out by the viral enzyme integrase, which, along with protease and reverse transcriptase, are encoded by HIV.
1 Dolutegravir is the third HIV
integrase strand transferase inhibitor (INI) and the first stand-alone INI with once-daily dosing that does not require boosting with a pharmacokinetic enhancer.
2
British HIV Association (BHIVA) guidelines (2012) recommend that therapy-naive patients start ART containing two nucleotide reverse transcriptase inhibitor (NRTIs) plus one of the following: a ritonavir-boosted protease inhibitor (PI/r), an NNRTI or an integrase inhibitor (INI).
3 BHIVA recommend patients with triple-class resistance switch to a new ART regimen containing at least
two and preferably three fully active agents with at least one active PI/r such as darunavir/r (DRV/r) or tipranavir/ ritonavir (TPV/r) and one agent with a novel mechanism (CCR5 receptor antagonist or integrase/fusion inhibitor) with etravirine (ETV) an option based on viral susceptibility.
3
2. Proposed place in therapy ViiV Healthcare anticipates that dolutegravir will be used as first-line therapy in treatment-naïve patients or treatment-experienced, integrase-inhibitor naive patients. Dosing in adults is as follows:
4
Treatment-naïve or treatment-experienced INI-naïve: 50mg once daily.
Treatment-naïve or treatment-experienced INI-naïve when co-administered with the following potent UGT1A/CYP3A inducers: efavirenz, fosamprenavir/ritonavir, tipranavir/ritonavir, or rifampicin: 50mg twice daily.
INI-experienced with certain INI-associated resistance substitutions or clinically suspected INI resistance: 50mg twice daily. Patients without INI resistance may take DTG with or without food. In the presence of integrase class resistance, DTG should preferably be taken with food to enhance exposure (particularly in patients with Q148 mutations).
5
If efavirenz, fosamprenavir/ritonavir, tipranavir/ritonavir or rifampicin is co-administered, the dose is 50 mg twice daily. Dosing in treatment-naïve or treatment-experienced INI-naïve children aged 12 years and older and weighing at least 40kg is 50mg once daily.
3. Evidence selected for inclusion There are five phase 3 studies in adults; these were identified by a literature search and from information provided by ViiV Healthcare. Three studies have been in treatment-naïve adults: SPRING-2 compared dolutegravir once daily (OD) with raltegravir twice daily (BD)
6;7, SINGLE compared dolutegravir OD + Kivexa with Atripla
8;9 and FLAMINGO compared dolutegravir
OD with darunavir boosted with ritonavir10
. Two have been in treatment experienced patients: SAILING compared dolutegravir 50mg OD with raltegravir in treatment experienced, integrase naive patients while VIKING-3 assessed the efficacy of dolutegravir 50mg BD in highly treatment experienced patients with resistance to multiple antiretroviral (ARV) classes including integrase inhibitors.
11;12 SPRING-2, SINGLE and SAILING have been fully published. All studies were sponsored by ViiV Healthcare. There is
also an on-going phase 1/2 open-label, pharmacokinetic study (IMPAACT) in paediatrics.13;14
Treatment - naïve adults SPRING-2
SPRING-2 is a 96-week, randomised, double-blind, active-controlled, non-inferiority study in treatment-naïve adults (85%

2
men) with HIV RNA ≥1000 copies per mL (c/mL) and no primary resistance in reverse transcriptase or protease enzymes; there were no CD4 entry criteria.
6;7 Exclusion criteria were defined laboratory values or medical characteristics such as US
Center for Disease Control and Prevention (CDC) category C disease, except for Kaposi’s sarcoma, pregnancy, moderate or severe hepatic impairment, need for hepatitis C treatment, estimated creatinine clearance <50mL/min, recent or on-going malignancy or HIV-1 vaccine within 90 days of screening or any immunomodulator within 28 days. Patients were randomised to treatment either dolutegravir 50mg once daily (OD) (n=411) or raltegravir 400mg twice daily (BD) (n=411). All patients received a NRTI backbone of tenofovir/emtricitabine (TDF/FTC, 60%) or abacavir/lamivudine (ABC/3TC, 40%); one switch was allowed for management of side effects but those switching after 4 weeks were regarded as non-responders. Patients could only receive abacavir after exclusion of the HLA-B*5701 allele. Randomisation was also stratified according to HIV-1 RNA (≤100,000 or >100,000 c/mL; 28% had baseline levels >100,000 c/mL) and NRTI backbone. The study was powered (90%) with a 10% non-inferiority margin pre-specified for both the 48 (primary endpoint) and 96 week analyses. All safety and efficacy analyses were on the intention-to-treat population (ITT, all patients randomised to treatment groups who took at least one dose of study drug).
The primary endpoint was the proportion of patients with HIV-1 RNA <50c/mL at week 48, by snapshot analysis (i.e. those who had HIV-1 RNA <50c/mL in the analysis window of 48 weeks ± 6 weeks). At week 48, 88% (n=361) on dolutegravir and 85% (n=351) on raltegravir had reached the primary endpoint. Treatment difference was 2.5% (95% CI -2.2% to +7.1%), meeting the non-inferiority criterion.
6 At week 48 in the dolutegravir groups, similar proportions of patients achieved HIV-1
RNA<50c/mL regardless of treatment backbone: 86% in the dolutegravir/ABC/3TC group and 89% in the dolutegravir/TDF/FTC group.
6 By week 96, a difference could be seen, with 74% and 86% respectively achieving HIV-1 RNA
<50c/mL.7
The proportion of patients with virological suppression by week 96 was slightly lower: 81% in the dolutegravir arm and 76% in the raltegravir arm, treatment difference 4.5%, (-1.1% to +10%), and dolutegravir remained non-inferior to raltegravir.
7
Main secondary endpoints were: o Change from baseline in CD4 count: At 48 weeks CD4 counts increased in both groups from a median baseline value
of 360 cells/microL by a median of 230 cells/microL (see Appendix 1a). This increased to +276 cells with dolutegravir and +264 cells with raltegravir by week 96.
6;7
o Virological outcome by baseline stratification: Similar rates of virological response were seen across subgroups stratified by CD4 count, baseline HIV-1 RNA and NRTI backbone at both week 48 and 96 (see Appendix 1a). There were few virological non-responses (viral load not <50c/mL) at week 48: eight patients on dolutegravir and five on raltegravir.
6;7
o Genotypic evidence of resistance: In patients with protocol-defined virological failure (22 in the dolutegravir group and 29 in the raltegravir group by week 96), no patient treated with dolutegravir had developed treatment-emergent integrase or NRTI resistance. In the raltegravir group, one patient developed a resistant mutation to integrase inhibitors and four developed resistant mutations to NRTIs.
7
SINGLE
SINGLE is a 96-week, randomised, double-blind, active-controlled, non-inferiority study in therapy-naïve patients with HIV-1 RNA ≥1000c/mL.
9 There was an option to continue to 144 weeks on open-label therapy. Patients were randomised to
treatment with dolutegravir 50mg OD + abacavir 600mg/lamivudine 300mg (Kivexa) OD (n=414) or efavirenz 600mg /tenofovir 300mg/emtricitabine 200mg (Atripla) OD (n=419). Randomisation was also stratified according to HIV-1 RNA (≤100,000 or >100,000 c/mL) and CD4 count (≤200 or >200 per mL
3). The study was powered (90%) with a 10% non-
inferiority margin. All safety and efficacy analyses were on the intention-to-treat population (ITT, all patients randomised to treatment groups who took at least one dose of study drug).
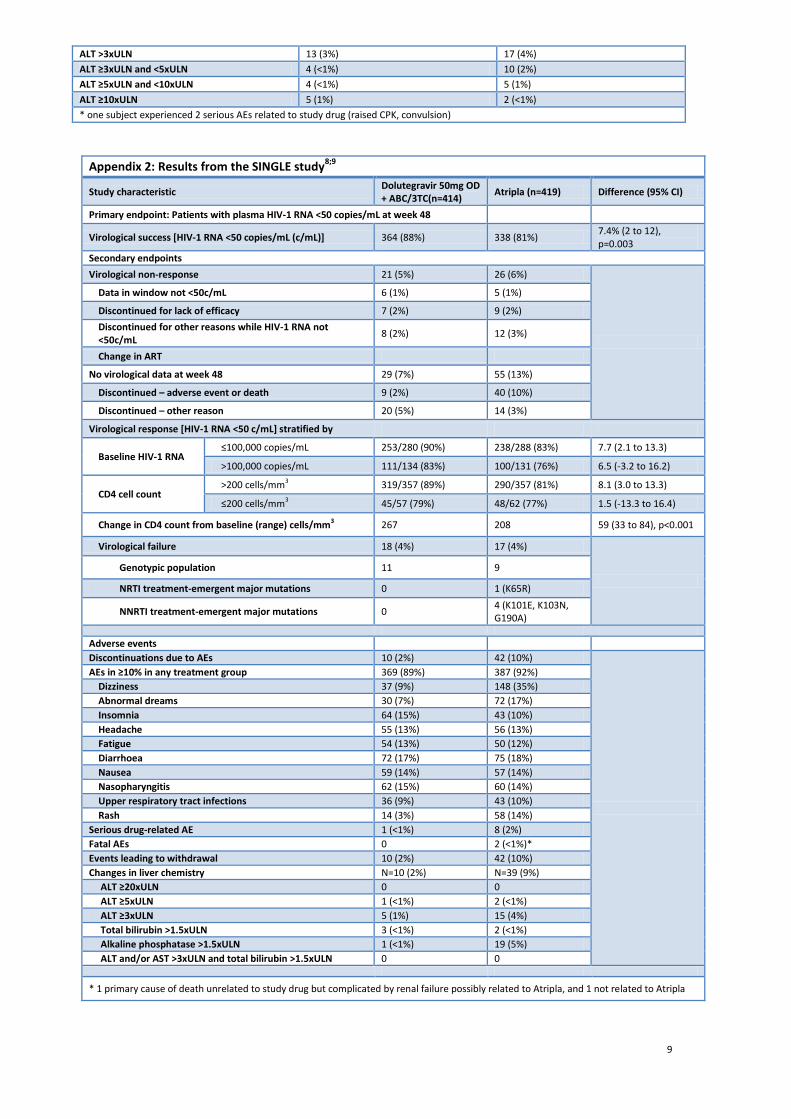
The primary endpoint was the proportion of patients with HIV-1 RNA <50c/mL at week 48, by snapshot analysis (i.e. those who had HIV-1 RNA <50c/mL in the analysis window of 48 weeks ± 6 weeks). At week 48, 88% on dolutegravir + Kivexa and 81% on Atripla had reached the primary endpoint. Treatment difference was +7% and met the predefined criteria for superiority (95% CI +2 to +12, p=0.003). This difference was seen in participants with HIV RNA ≤100,000 c/mL and >100,000 c/mL. Subjects receiving dolutegravir achieved virological suppression faster than Atripla, median time to HIV-1 RNA <50c/mL of 28 days (dolutegravir) vs. 84 days (Atripla), p<0.001 (see Appendix 2). Superiority of dolutegravir was driven by a lower proportion of patients discontinuing dolutegravir because of adverse events compared with Atripla (2% vs. 10%).
There were a number of secondary endpoints: o Change from baseline in CD4 count: At 48 weeks, the change in CD4 counts increased in both groups from a median
baseline value of 338/mL3 by +267 cells/mm
3 with dolutegravir and +208 cells/mm
3 with Atripla; difference 59
cells/mm3, (95% CI 33-84, p<0.001).
o Few patients had protocol defined virological failure: 18 (4%) in the dolutegravir arm and 17 (4%) in the Atripla arm, of which 11 and 9 respectively had baseline genotypic tests. No patient in the dolutegravir arm had developed a reverse transcriptase mutation but five in the Atripla arm did (1 NRTI- and 4 NNRTI-emergent major mutations). No patient developed an integrase inhibitor emergent mutation.
8
FLAMINGO
FLAMINGO is an open-label 96 week, phase 3b/4 non-inferiority study comparing dolutegravir 50mg OD (n=242) with a once-daily regimen containing darunavir (800mg boosted with ritonavir 100mg)(n=242) in treatment-naïve patients with HIV-1.
10 Both treatment arms were administered with investigator-selected dual NRTIs. Data have only been published as a
conference abstract, so cannot be fully evaluated. Exclusion criteria were not stated in the abstract.
The primary objective was to demonstrate the antiviral activity of dolutegravir to darunavir over 48 weeks. At 48 weeks, 90% of patients treated with dolutegravir vs. 83% treated with darunavir/ritonavir (darunavir/r) were virologically suppressed (HIV-1 RNA <50c/mL). Treatment difference was 7.1% and met the predefined criteria for superiority, (95% CI
3
+0.9 to +13.2, p=0.025).
There were a number of secondary endpoints. o Rates of virological non-response were 6% in the dolutegravir arm and 7% in the darunavir/r arm. See Appendix 3 for
more results. Protocol-defined virological failure occurred in 2 patients (<1%) in both groups and no emergent INI, PI or NRTI mutations were seen in either arm.
o When patients were stratified according to HIV-1 RNA (≥ or <100,000 c/mL) and background dual NRTI therapy, dolutegravir was superior to darunavir/r for all groups (see Appendix 3).
o Median CD4 counts increased by 210 cells/mm3 in both groups.
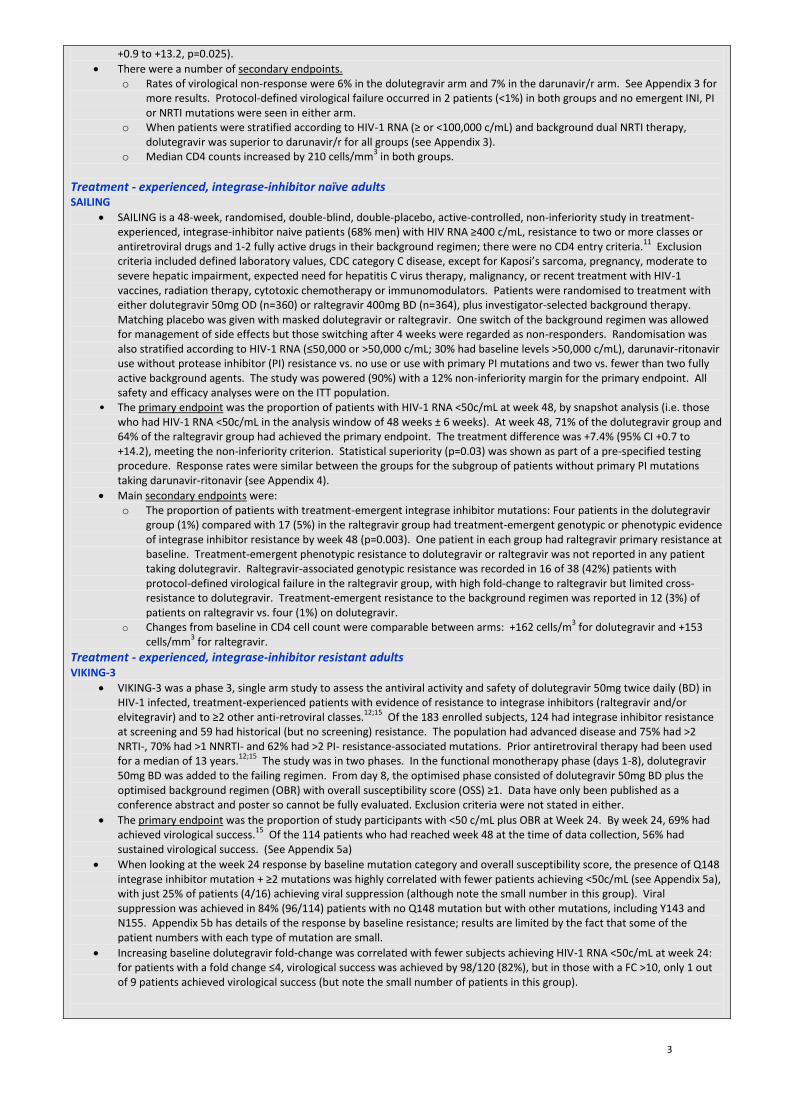
Treatment - experienced, integrase-inhibitor naïve adults SAILING
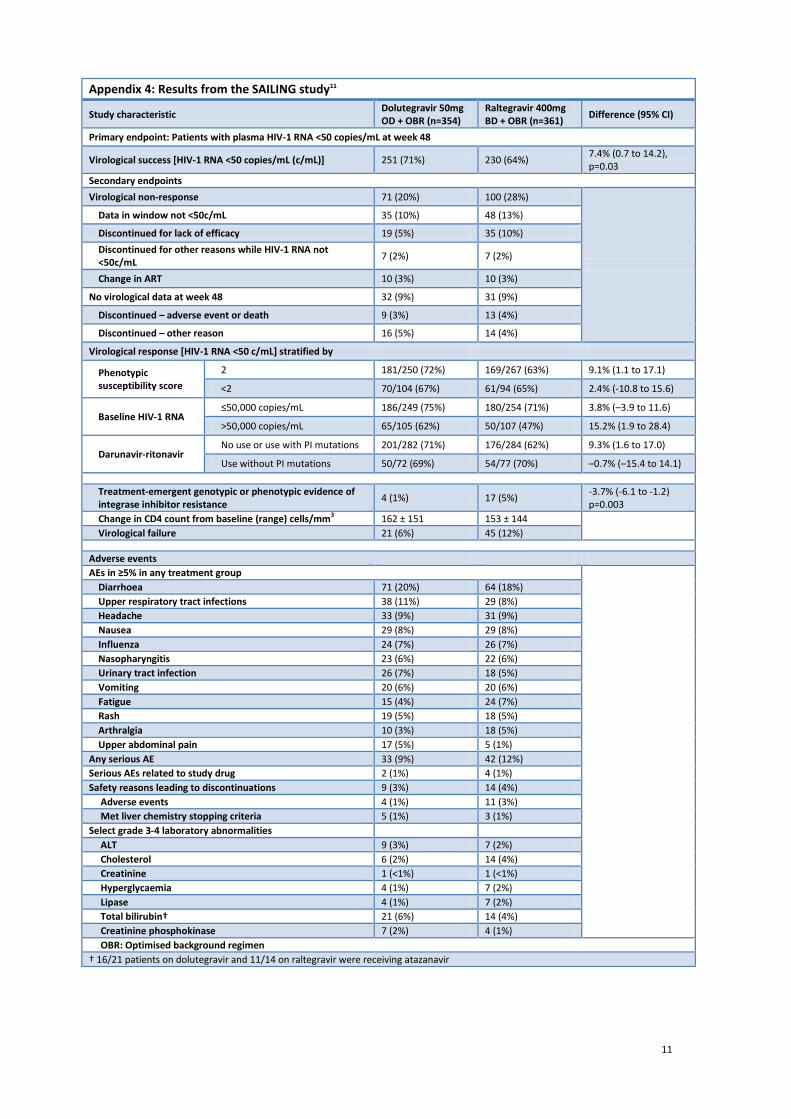
SAILING is a 48-week, randomised, double-blind, double-placebo, active-controlled, non-inferiority study in treatment-experienced, integrase-inhibitor naive patients (68% men) with HIV RNA ≥400 c/mL, resistance to two or more classes or antiretroviral drugs and 1-2 fully active drugs in their background regimen; there were no CD4 entry criteria.
11 Exclusion
criteria included defined laboratory values, CDC category C disease, except for Kaposi’s sarcoma, pregnancy, moderate to severe hepatic impairment, expected need for hepatitis C virus therapy, malignancy, or recent treatment with HIV-1 vaccines, radiation therapy, cytotoxic chemotherapy or immunomodulators. Patients were randomised to treatment with either dolutegravir 50mg OD (n=360) or raltegravir 400mg BD (n=364), plus investigator-selected background therapy. Matching placebo was given with masked dolutegravir or raltegravir. One switch of the background regimen was allowed for management of side effects but those switching after 4 weeks were regarded as non-responders. Randomisation was also stratified according to HIV-1 RNA (≤50,000 or >50,000 c/mL; 30% had baseline levels >50,000 c/mL), darunavir-ritonavir use without protease inhibitor (PI) resistance vs. no use or use with primary PI mutations and two vs. fewer than two fully active background agents. The study was powered (90%) with a 12% non-inferiority margin for the primary endpoint. All safety and efficacy analyses were on the ITT population.
• The primary endpoint was the proportion of patients with HIV-1 RNA <50c/mL at week 48, by snapshot analysis (i.e. those who had HIV-1 RNA <50c/mL in the analysis window of 48 weeks ± 6 weeks). At week 48, 71% of the dolutegravir group and 64% of the raltegravir group had achieved the primary endpoint. The treatment difference was +7.4% (95% CI +0.7 to +14.2), meeting the non-inferiority criterion. Statistical superiority (p=0.03) was shown as part of a pre-specified testing procedure. Response rates were similar between the groups for the subgroup of patients without primary PI mutations taking darunavir-ritonavir (see Appendix 4).
Main secondary endpoints were: o The proportion of patients with treatment-emergent integrase inhibitor mutations: Four patients in the dolutegravir
group (1%) compared with 17 (5%) in the raltegravir group had treatment-emergent genotypic or phenotypic evidence of integrase inhibitor resistance by week 48 (p=0.003). One patient in each group had raltegravir primary resistance at baseline. Treatment-emergent phenotypic resistance to dolutegravir or raltegravir was not reported in any patient taking dolutegravir. Raltegravir-associated genotypic resistance was recorded in 16 of 38 (42%) patients with protocol-defined virological failure in the raltegravir group, with high fold-change to raltegravir but limited cross-resistance to dolutegravir. Treatment-emergent resistance to the background regimen was reported in 12 (3%) of patients on raltegravir vs. four (1%) on dolutegravir.
o Changes from baseline in CD4 cell count were comparable between arms: +162 cells/m3 for dolutegravir and +153
cells/mm3 for raltegravir.
Treatment - experienced, integrase-inhibitor resistant adults VIKING-3
VIKING-3 was a phase 3, single arm study to assess the antiviral activity and safety of dolutegravir 50mg twice daily (BD) in HIV-1 infected, treatment-experienced patients with evidence of resistance to integrase inhibitors (raltegravir and/or elvitegravir) and to ≥2 other anti-retroviral classes.
12;15 Of the 183 enrolled subjects, 124 had integrase inhibitor resistance
at screening and 59 had historical (but no screening) resistance. The population had advanced disease and 75% had >2 NRTI-, 70% had >1 NNRTI- and 62% had >2 PI- resistance-associated mutations. Prior antiretroviral therapy had been used for a median of 13 years.
12;15 The study was in two phases. In the functional monotherapy phase (days 1-8), dolutegravir
50mg BD was added to the failing regimen. From day 8, the optimised phase consisted of dolutegravir 50mg BD plus the optimised background regimen (OBR) with overall susceptibility score (OSS) ≥1. Data have only been published as a conference abstract and poster so cannot be fully evaluated. Exclusion criteria were not stated in either.
The primary endpoint was the proportion of study participants with <50 c/mL plus OBR at Week 24. By week 24, 69% had achieved virological success.
15 Of the 114 patients who had reached week 48 at the time of data collection, 56% had
sustained virological success. (See Appendix 5a)
When looking at the week 24 response by baseline mutation category and overall susceptibility score, the presence of Q148 integrase inhibitor mutation + ≥2 mutations was highly correlated with fewer patients achieving <50c/mL (see Appendix 5a), with just 25% of patients (4/16) achieving viral suppression (although note the small number in this group). Viral suppression was achieved in 84% (96/114) patients with no Q148 mutation but with other mutations, including Y143 and N155. Appendix 5b has details of the response by baseline resistance; results are limited by the fact that some of the patient numbers with each type of mutation are small.
Increasing baseline dolutegravir fold-change was correlated with fewer subjects achieving HIV-1 RNA <50c/mL at week 24: for patients with a fold change ≤4, virological success was achieved by 98/120 (82%), but in those with a FC >10, only 1 out of 9 patients achieved virological success (but note the small number of patients in this group).

4
Paediatrics IMPAACT study
IMPAACT P1093 is an on-going, phase 1/2 open-label pharmacokinetic, dose-finding study in HIV-1 infected children aged 4 weeks to <18 years.
13 Results from Cohort 1, adolescents 12 years to <18 years, have been presented as a conference
abstract.14
The study was in two phases: in stage I, dolutegravir was dosed at 1mg/kg (maximum 50mg once daily) for 48 weeks, either added to stable, failing antiretroviral regimens or started as monotherapy.
14 Stage II assessed long-term
follow-up.13
Ten adolescents (7 females) with mean age 14 years were enrolled, nine received dolutegravir 50mg and one received 35mg daily.
Primary endpoints were safety and pharmacokinetics. Secondary endpoints included measurement of HIV RNA levels and CD4 counts. HIV-1 RNA <40copies/mL was achieved in 7/10 (70%) of subjects after 4 weeks of dosing and median change from baseline was -2.8 log10copies/mL (95% CI -3.1 to -2.6).
4. Critical evaluation 4.1. Clinical application
By the end of 2012, an estimated 98,4000 people were living with HIV in the UK, of whom approximately 22% were undiagnosed.
16 Of the 76,500 patients living with a diagnosed HIV infection, 33,600 (44%) were men who have sex with
men, 14,900 were heterosexual men (19.5%), 24,000 heterosexual women (31.3%). Of the heterosexual men, 8,100 (54.3%) were African-born and of the heterosexual women, 16,400 (68.3%) were African born.
The studies participant demographics may not be representative of the demographics of the UK population living with HIV and could limit extrapolation of study results to other patient groups
Critical evaluation of FLAMINGO and VIKING-3 is limited due to the presentation of the data as conference abstracts.
Due to the double-dummy design of some of the studies, the potential benefits of dolutegravir as a once daily treatment option could not be assessed.
Treatment-naïve adults
In SPRING-2, dolutegravir was shown to be non-inferior to raltegravir with respect to reduction of HIV-1 RNA at 48 weeks and at 96 weeks.
6;7 Most study participants were white (85%), males (85%) and with fairly non-advanced disease.
6 Antiviral
resistance to dolutegravir was not seen in patients with protocol-defined virological failure, but it was seen in some patients taking raltegravir. The week 48 and week 96 results show non-inferiority and no safety differences; the results from SPRING-2 give little incentive for changing therapy from raltegravir to dolutegravir although the once-daily dosing schedule may improve adherence with treatment.
In SINGLE, dolutegravir + ABC/3TC was superior to Atripla in achieving virological success and also had a better side effect profile.
9 Overall differences in response were due primarily to discontinuations because of adverse events (10/414, 2%, in
the dolutegravir group vs. 42/419, 10% in the Atripla group). Most participants were male (84%), but 24% were African American.
In FLAMINGO, overall superiority of dolutegravir was shown over darunavir/r, driven by a lower number of withdrawals [18, (7%) vs. 29 (12%)] and fewer virological non-responders.
10 Detailed critical evaluation is limited by the presentation of the
data as a conference abstract.
Overall, dolutegravir was shown to be as effective in reducing HIV-1 RNA <50c/mL as raltegravir and superior to Atripla and darunavir/r, with a side effect profile comparable to that of raltegravir but better than Atripla and darunavir/r.
To date, no integrase resistance mutations have developed during the dolutegravir studies in treatment-naive patients. Treatment-experienced adults
In SAILING, the population was more diverse with 49% Caucasian, 68% male, 46% with a history of AIDS and 49% with resistance to at least one drug in three or more antiretroviral classes.
11 SAILING is the first study to show superior
virological efficacy of any antiretroviral drug over raltegravir; this was driven by fewer virological non-responders in the dolutegravir group compared with the raltegravir group.
11 There was also significantly less treatment-emergent integrase
inhibitor or background therapy resistance at failure. No integrase resistance mutations developed in treatment-experience patients. Protocol-defined virological failure occurred more frequently and earlier on with raltegravir, reflecting the greater antiviral potency of dolutegravir. Dolutegravir use also led to higher proportions of more difficult-to-treat patients (e.g. those with baseline HIV-1 RNA >50,000c/mL or those not taking darunavir-ritonavir) achieving virological suppression.
VIKING-3 supports the use of dolutegravir in patients with multi-antiretroviral drug resistance, a difficult-to-treat patient population.
12 Not all of the patients had reached week 48 at the time the data was collected and while the current results
show a decrease in the number with virological success from week 24 to 48, this may change as more patients reach this time point.
Paediatrics
There are few published data regarding the efficacy of dolutegravir in children over 12 years of age; this is currently limited
to data from the phase 1/2 IMPAACT study (P1093); the primary endpoints of this were safety and pharmacokinetics.
4.2. Safety and Drug interactions
Adults
Few patients discontinued dolutegravir due to adverse events: around 2% in each study discontinued due to dolutegravir-associated adverse events (n=3-10), compared with 10% taking Atripla (n=42) and 4% taking darunavir (n=9). Discontinuation rates were similar to those seen with raltegravir (n=6-11). Overall, discontinuations due to adverse events

5
were numerically small.
The safety profiles of dolutegravir and raltegravir were shown to be comparable in SPRING-2 and SAILING (see Appendices 1b and 4).
6;11;17 The most frequently reported adverse events (AEs) were headache, nausea, diarrhoea, upper respiratory
tract infections, with most events grade 1 or 2 and occurring at similar rates in both groups. Changes in laboratory parameters were similar in each group in each study. Few patients had drug-induced liver injury. Results from SPRING-2 up to 96 weeks showed that the adverse event profile between dolutegravir and raltegravir was still comparable.
7
In SINGLE, more patients receiving Atripla reported drug-related adverse events than receiving dolutegravir (66% vs. 43%).9
The incidence of dizziness and abnormal dreams was higher with Atripla than with dolutegravir (35% and 17% vs. 9% and 7%, p<0.001 for both comparisons), as would be expected from the side-effect profile of Atripla.
18 The incidence of
insomnia was higher in those treated with dolutegravir (15% vs.10%); this has not been seen in other studies and may be an artifact.
Darunavir was associated with a higher incidence of diarrhoea than dolutegravir (29% vs. 17%) in FLAMINGO, and while more patients discontinued darunavir than dolutegravir, the numbers were low (10 vs. 4) (see Appendix 3).
10
The safety profile of dolutegravir in VIKING-3 was similar to that seen in the other studies. Paediatrics
In the small number of adolescents treated with dolutegravir in IMPAACT, there were no drug discontinuations due to adverse events, no trends in laboratory abnormalities and one grade 3 event (not stated in the conference abstract).
14
Renal effects
Dolutegravir inhibits the organic cation transport OCT2, which decreases tubular secretion of creatinine and therefore increases serum creatinine concentrations, but without affecting glomerular filtration rates.
6 A study in healthy volunteers
has shown that dolutegravir 50mg OD and BD does not affect actual glomerular filtration, as shown by the absence of effect of iohexal clearance.
6 Small increases in serum creatinine and small reductions in creatinine clearance have been reported
in three of the phase 3 studies, occurring early in treatment but remaining stable for the course of the study.6;9;11
Drug interactions
Dolutegravir inhibits OCT2 and may increase plasma concentrations of drugs eliminated by this pathway, i.e. metformin, and an adjustment of the metformin dose may be necessary.
4
Dolutegravir does not induce CYP1A2, CYP2B6 or CYP3A4 and would not be expected to affect the pharmacokinetics of drugs that are substrates of these enzymes.
4
Dolutegravir is metabolised mainly by UGT1A1 with some minor metabolism by CYP3A.4 Darunavir/ritonavir,
lopinavir/ritonavir, rilpivirine, tenofovir, boceprevir, telaprevir, prednisolone, rifabutin and omeprazole had no clinically significant effect on the pharmacokinetics of dolutegravir. Etravirine significantly reduced plasma concentrations of dolutegravir, but these effects of etravirine were mitigated by co-administration of lopinavir/ritonavir or darunavir/ritonavir and are expected to be mitigated by atazanavir/ritonavir.
4
As per other integrase inhibitors, dolutegravir should not be administered concurrently with medication containing polyvalent cations, i.e. magnesium and aluminium-containing antacids or laxatives, oral iron or calcium supplements or sucralfate.
4;19;20 These can form complexes with the integrase inhibitors and reduce absorption.
20 Dolutegravir should be
administered 2 hours before or 6 hours after taking medications containing polyvalent cations.4
The summary of product characteristics should be consulted for the full list of drug interactions.
4.3. Potential advantages and disadvantages over existing technologies 4.3.1. Convenience
Dolutegravir is a once-daily dosing regimen; the advantages of this compared with twice-daily raltegravir has not been assessed in clinical studies.
Several studies have shown higher adherence with once-daily dosing of antiretroviral therapy (ART) than with twice-daily dosing and some have shown that a lower pill burden results in higher adherence.
21 One prospective, observational cohort
study of newly diagnosed patients (n=99) assessed adherence to ART regimens based on pill burden.21
Seventy participants (71%) were taking a once-daily regimen, this included 34 (34%) taking Atripla and 36 (36%) were taking a once-daily regimen that consisted of more than one pill. The rest (n=29) were taking a twice-daily regimen. Of the participants taking more than one pill a day, some took up to 7 pills a day (n=3), but most took 3-5 pills a day (n=48).
Adherence over 30 days was assessed using a subjective visual analogue scale (VAS) and the mean adherence calculated every 3 months for 18 months. Use of a subjective VAS is a study limitation; objective measures such as pharmacy refill data or pill counts were not used. Once-daily dosing was associated with greater mean adherence rates than twice-daily dosing: 99.5% vs. 94% (p=0.01). For patients taking a once-daily regimen, mean adherence for those taking Atripla (100%) was no different to those taking more than one pill (99.3%), suggesting that pill burden is not an important factor in determining adherence. These are all high rates which may be due to patients overstating their adherence and, as stated above, are subjective, not objective.
Viral load data were only available for 76 patients, limiting the ability to detect small differences in adherence and virological suppression. Virological suppression was more likely in those with 99-100% adherence (n=38, 84% suppressed) than in those with <99% adherence (n=36, 64% suppressed, p=0.06). There was no statistically significant difference in virological suppression between those taking once-daily regimens (n=42, 79.3% suppressed) and those taking twice-daily

6
Search strategy: Medline: dolutegravir.af Embase: *DOLUTEGRAVIR/ SIGN grade of evidence: Grade ‘A’ At least one meta-analysis, systematic review, or RCT rated as 1++ and directly applicable to the target population or A systematic review of RCTs or a body of evidence consisting principally of studies rated as 1+ directly applicable to the target population and demonstrating overall consistency of results. Written by Alexandra Denby, London Medicines Information Service, Pharmacy Department, Northwick Park Hospital, Harrow, HA1 3UJ. [email protected]. ViiV Healthcare and specialist HIV pharmacists from London have commented on this review.
References Reference List
(1) Katlama C, Murphy R. Dolutegravir for the treatment of HIV. Expert Opinion on Investigational Drugs
2012; 21(4):523-530.
(2) Boyd MA, Donovan B. Antiretroviral therapy: dolutegravir sets SAIL(ING). Lancet 2013; 382:664-666.
(3) Williams I, Churchill D, Anderson J et al. British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2012. HIV Medicine 2012; 13(Suppl 2):1-85. DOI: 10.1111/j.1468-1293.2012.01029_1.x
(4) Prescribing information: Tivicay. Revised August 2013. GlaxoSmithKline 2013 http://www.viivhealthcare.com/media/58599/us_tivicay.pdf
(5) Personal communication, ViiV Healthcare. 19/12/2013.
(6) Raffi F, Rachlis A, Stellbrink HJ et al. Once-daily dolutegravir versus raltegravir in antiretroviral-naive adults with HIV-1 infection: 48 week results from the randomised, double-blind, non-inferiority SPRING-2 study. Lancet 2013; 381:735-743.
(7) Raffi F, Jaeger H, Quiros-Roldan E et al. Once-daily dolutegravir versus twice-daily raltegravir in antiretroviral-naive adults with HIV-1 infection (SPRING-2 study): 96 week results from a randomised, double-blind, non-inferiority trial. Lancet 2013; dx.doi.org/10.1016/S1473-3099(13)70257-3.
(8) Walmsley S, Antela A, Clumeck N et al. Dolutegravir (DTG; S/GSK1349572) + abacavir/lamivudine once daily statistically superior to tenofovir/emtricitabine/efavirenz: 48-week results - SINGLE (ING114467).
regimens (n=14, 60.9% suppressed, p=0.15), but this may be due to the small sample size. Pill burden did not influence virological suppression with no statistically significant differences between those taking fixed-dose Atripla (n=23, 82.1% suppressed) and those taking >1 pill once daily (n=19, 76% suppressed, p=0.74), and between those taking Atripla and those taking all other regimens (n=33, 68.6% suppressed, p=0.28).
4.3.2. Drug cost
To be confirmed.
5. Likely commissioning and funding pathway Commissioning will be through NHS England and is not in the PbR Tariff.
6. Suggested place in therapy Dolutegravir is the first integrase inhibitor to be available as a stand-alone tablet (as opposed to in a fixed-dose
combination) that is administered once a day, with no need for pharmacokinetic boosting. Dolutegravir offers a treatment option in integrase experienced patients with certain integrase inhibitor mutations and
requiring salvage therapy. Dolutegravir is given twice daily in treatment-experienced patients with integrase resistance, preferably with food.
Dolutegravir has been shown to be non-inferior to raltegravir in clinical studies in treatment-naïve patients and superior in treatment-experienced, integrase naive patients. It has been shown to be superior to Atripla and boosted darunavir in treatment-naïve patients.
To date, no integrase resistance mutations have developed during the dolutegravir studies in treatment-naive patients.
The number of patients who discontinued dolutegravir due to adverse events was low; it has a better adverse event profile than Atripla and darunavir/ritonair
Although adherence to once-daily dolutegravir has not been compared with that with twice-daily raltegravir in clinical studies, adherence to once-daily regimens has been shown to be higher than with twice-daily regimens but for once-daily regimens, pill burden did not affect adherence.

7
Abstract H-556b. 52nd Interscience Conference on Antimicrobials Agents and Chemotherapy, San Francisco, California. September 9-12, 2012
(9) Walmsley SL, Antela A, Clumeck N et al. Dolutegravir plus abacavir-lamivudine for the treatment of HIV-1 infection. N Engl J Med 2013; 369:1807-1818.
(10) Feinberg J, Bonaventura C, Khuong M-A et al. Once-daily dolutegravir (DTG) is superior to darunavir/ritonavir (DRV/r) in antiretroviral-naive adults: 48 week results from FLAMINGO (ING114915). Abstract h-1464a. 53rd Interscience Conference on Antimicrobial Agents and Chemotherapy. Denver, Colorado. September 10-13, 2013
(11) Cahn P, Pozniak A, Mingrone H et al. Dolutegravir versus raltegravir in antiretroviral-experienced integrase-inhibitor-naive adults with HIV: week 48 results from the randomised, double-blind, non-inferiority SAILING study. Lancet 2013; 382:700-708.
(12) Nichols G, Mills A, Grossberg R et al. Antiviral activity of dolutegravir in subjects with failure on an integrase inhibitor-based regimen: week 24 phase 3 results from VIKING-3. J Int AIDS Soc 2012; 15(Suppl 4). http://dx.doi.org.10.7448/IAS15.6.18112
(13) Safety of and immune response to GSK1349572 in HIV-1 infected infants, children, and adolescents. NCT01302847. www.clinicaltrials.gov
(14) Hazra R, Viani R, Acosta E et al. Pharmacokinetics, safety and efficacy of dolutegravir (DTG; S/GSK1349572) in HIV-1-positive adolescents: preliminary analysis from IMPAACT P1093. Abstract no. TUAB0203. 19th International AIDS Conference, Washington DC, July 22-27.: 2012
(15) Nichols G, Lazzarin A, Maggiolo F et al. Phase 3 assessment of dolutegravir (DTG) 50mg twice daily (BID) in HIV-1 infected subjects with raltegravir (RAL) and/or elvitegravir (EVG) resistance in VIKING-3: week 24 results of all 183 subjects enrolled. Poster: TULBPE19. 7th IAS Conference on HIV Pathogenesis, Treatment and Prevention. Kuala Lumpur, Malaysia. June 30 - July 3: 2013
(16) HIV in the United Kingdom: 2013 Report. Health Protection Agency 2013 http://www.hpa.org.uk/Publications/InfectiousDiseases/HIVAndSTIs/1311HIVintheUk2013report/
(17) Raffi F, Rachlis A, Stellbrink HJ et al. Supplementary appendix (SPRING-2). Lancet 2013. http://dx.doi.org/10.1016/S0140-6736(12)61853-4
(18) Supplementary appendix to: Walmsley SL, Antela A, Clumeck N et al. Dolutegravir plus abacavir-lamivudine for the treatment of HIV-1 infection. N Engl J Med 2013; 369:1807-1818.
(19) Summary of Product Characteristics. Isentress 400mg film-coated tablets. Merck Sharp & Dohme Ltd. Date accessed 30/09/2013. Date of revision of the text: August 2013. Accessed via emc.medicines.org.uk.
(20) Summary of Product Characteristics. Stribild 150mg/150mg/200mg/245mg film-coated tablets. Gilead Sciences Ltd. Date accessed 22/11/2013. Date of revision of the text: October 2013. Accessed via emc.medicines.org.uk.
(21) Buscher A, Hartman C, Kallen MA et al. Impact of antiretroviral dosing frequency and pill burden on adherence among newly diagnosed, HAART naive HIV patients. Int J STD AIDS 2012; 23(5):351-355.
8
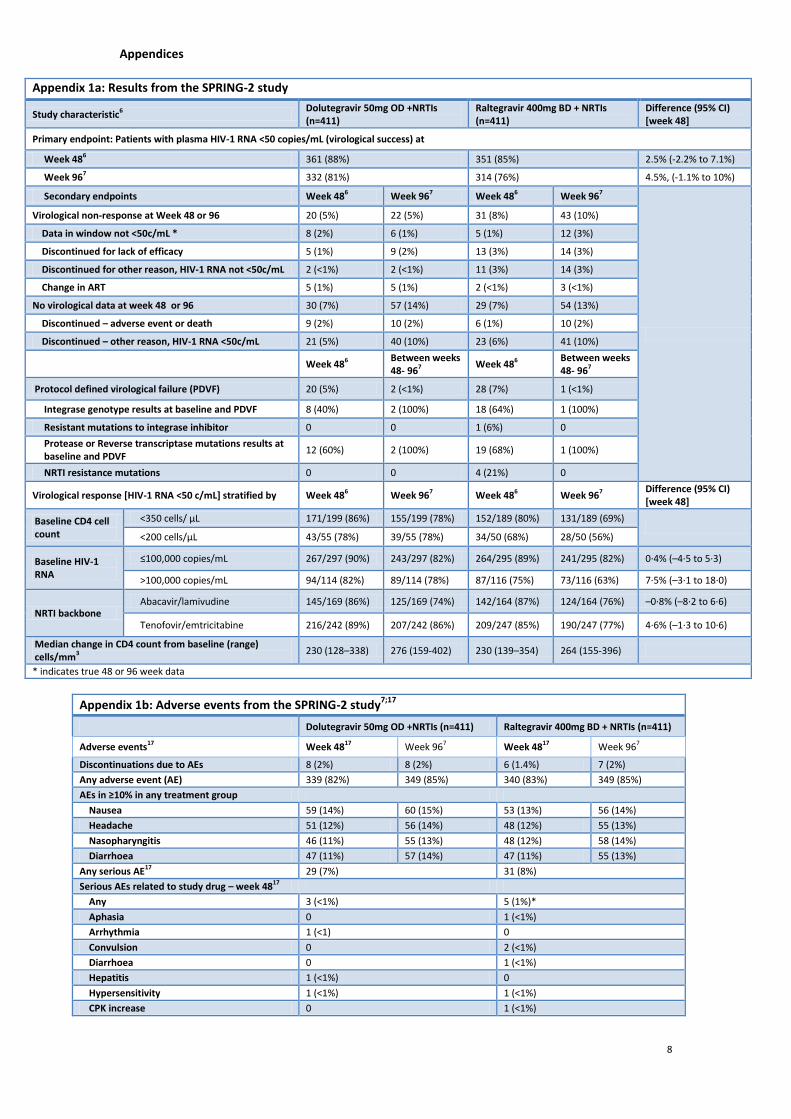
Appendices
Appendix 1a: Results from the SPRING-2 study
Study characteristic6 Dolutegravir 50mg OD +NRTIs (n=411)
Raltegravir 400mg BD + NRTIs (n=411)
Difference (95% CI) [week 48]
Primary endpoint: Patients with plasma HIV-1 RNA <50 copies/mL (virological success) at
Week 486 361 (88%) 351 (85%) 2.5% (-2.2% to 7.1%)
Week 967 332 (81%) 314 (76%) 4.5%, (-1.1% to 10%)
Secondary endpoints Week 486 Week 967 Week 486 Week 967
Virological non-response at Week 48 or 96 20 (5%) 22 (5%) 31 (8%) 43 (10%)
Data in window not <50c/mL * 8 (2%) 6 (1%) 5 (1%) 12 (3%)
Discontinued for lack of efficacy 5 (1%) 9 (2%) 13 (3%) 14 (3%)
Discontinued for other reason, HIV-1 RNA not <50c/mL 2 (<1%) 2 (<1%) 11 (3%) 14 (3%)
Change in ART 5 (1%) 5 (1%) 2 (<1%) 3 (<1%)
No virological data at week 48 or 96 30 (7%) 57 (14%) 29 (7%) 54 (13%)
Discontinued – adverse event or death 9 (2%) 10 (2%) 6 (1%) 10 (2%)
Discontinued – other reason, HIV-1 RNA <50c/mL 21 (5%) 40 (10%) 23 (6%) 41 (10%)
Week 486 Between weeks 48- 967
Week 486 Between weeks 48- 967
Protocol defined virological failure (PDVF) 20 (5%) 2 (<1%) 28 (7%) 1 (<1%)
Integrase genotype results at baseline and PDVF 8 (40%) 2 (100%) 18 (64%) 1 (100%)
Resistant mutations to integrase inhibitor 0 0 1 (6%) 0
Protease or Reverse transcriptase mutations results at baseline and PDVF
12 (60%) 2 (100%) 19 (68%) 1 (100%)
NRTI resistance mutations 0 0 4 (21%) 0
Virological response [HIV-1 RNA <50 c/mL] stratified by Week 486 Week 967 Week 486 Week 967 Difference (95% CI) [week 48]
Baseline CD4 cell count
<350 cells/ μL 171/199 (86%) 155/199 (78%) 152/189 (80%) 131/189 (69%)
<200 cells/μL 43/55 (78%) 39/55 (78%) 34/50 (68%) 28/50 (56%)
Baseline HIV-1 RNA
≤100,000 copies/mL 267/297 (90%) 243/297 (82%) 264/295 (89%) 241/295 (82%) 0·4% (–4·5 to 5·3)
>100,000 copies/mL 94/114 (82%) 89/114 (78%) 87/116 (75%) 73/116 (63%) 7·5% (–3·1 to 18·0)
NRTI backbone Abacavir/lamivudine 145/169 (86%) 125/169 (74%) 142/164 (87%) 124/164 (76%) –0·8% (–8·2 to 6·6)
Tenofovir/emtricitabine 216/242 (89%) 207/242 (86%) 209/247 (85%) 190/247 (77%) 4·6% (–1·3 to 10·6)
Median change in CD4 count from baseline (range) cells/mm3
230 (128–338) 276 (159-402) 230 (139–354) 264 (155-396)
* indicates true 48 or 96 week data
Appendix 1b: Adverse events from the SPRING-2 study7;17
Dolutegravir 50mg OD +NRTIs (n=411) Raltegravir 400mg BD + NRTIs (n=411)
Adverse events17 Week 4817 Week 967 Week 4817 Week 967
Discontinuations due to AEs 8 (2%) 8 (2%) 6 (1.4%) 7 (2%)
Any adverse event (AE) 339 (82%) 349 (85%) 340 (83%) 349 (85%)
AEs in ≥10% in any treatment group
Nausea 59 (14%) 60 (15%) 53 (13%) 56 (14%)
Headache 51 (12%) 56 (14%) 48 (12%) 55 (13%)
Nasopharyngitis 46 (11%) 55 (13%) 48 (12%) 58 (14%)
Diarrhoea 47 (11%) 57 (14%) 47 (11%) 55 (13%)
Any serious AE17 29 (7%) 31 (8%)
Serious AEs related to study drug – week 4817
Any 3 (<1%) 5 (1%)*
Aphasia 0 1 (<1%)
Arrhythmia 1 (<1) 0
Convulsion 0 2 (<1%)
Diarrhoea 0 1 (<1%)
Hepatitis 1 (<1%) 0
Hypersensitivity 1 (<1%) 1 (<1%)
CPK increase 0 1 (<1%)
9
ALT >3xULN 13 (3%) 17 (4%)
ALT ≥3xULN and <5xULN 4 (<1%) 10 (2%)
ALT ≥5xULN and <10xULN 4 (<1%) 5 (1%)
ALT ≥10xULN 5 (1%) 2 (<1%)
* one subject experienced 2 serious AEs related to study drug (raised CPK, convulsion)
Appendix 2: Results from the SINGLE study8;9
Study characteristic Dolutegravir 50mg OD + ABC/3TC(n=414)
Atripla (n=419) Difference (95% CI)
Primary endpoint: Patients with plasma HIV-1 RNA <50 copies/mL at week 48
Virological success [HIV-1 RNA <50 copies/mL (c/mL)] 364 (88%) 338 (81%) 7.4% (2 to 12), p=0.003
Secondary endpoints
Virological non-response 21 (5%) 26 (6%)
Data in window not <50c/mL 6 (1%) 5 (1%)
Discontinued for lack of efficacy 7 (2%) 9 (2%)
Discontinued for other reasons while HIV-1 RNA not <50c/mL
8 (2%) 12 (3%)
Change in ART
No virological data at week 48 29 (7%) 55 (13%)
Discontinued – adverse event or death 9 (2%) 40 (10%)
Discontinued – other reason 20 (5%) 14 (3%)
Virological response [HIV-1 RNA <50 c/mL] stratified by
Baseline HIV-1 RNA ≤100,000 copies/mL 253/280 (90%) 238/288 (83%) 7.7 (2.1 to 13.3)
>100,000 copies/mL 111/134 (83%) 100/131 (76%) 6.5 (-3.2 to 16.2)
CD4 cell count >200 cells/mm3 319/357 (89%) 290/357 (81%) 8.1 (3.0 to 13.3)
≤200 cells/mm3 45/57 (79%) 48/62 (77%) 1.5 (-13.3 to 16.4)
Change in CD4 count from baseline (range) cells/mm3 267 208 59 (33 to 84), p<0.001
Virological failure 18 (4%) 17 (4%)
Genotypic population 11 9
NRTI treatment-emergent major mutations 0 1 (K65R)
NNRTI treatment-emergent major mutations 0 4 (K101E, K103N, G190A)
Adverse events
Discontinuations due to AEs 10 (2%) 42 (10%)
AEs in ≥10% in any treatment group 369 (89%) 387 (92%)
Dizziness 37 (9%) 148 (35%)
Abnormal dreams 30 (7%) 72 (17%)
Insomnia 64 (15%) 43 (10%)
Headache 55 (13%) 56 (13%)
Fatigue 54 (13%) 50 (12%)
Diarrhoea 72 (17%) 75 (18%)
Nausea 59 (14%) 57 (14%)
Nasopharyngitis 62 (15%) 60 (14%)
Upper respiratory tract infections 36 (9%) 43 (10%)
Rash 14 (3%) 58 (14%)
Serious drug-related AE 1 (<1%) 8 (2%)
Fatal AEs 0 2 (<1%)*
Events leading to withdrawal 10 (2%) 42 (10%)
Changes in liver chemistry N=10 (2%) N=39 (9%)
ALT ≥20xULN 0 0
ALT ≥5xULN 1 (<1%) 2 (<1%)
ALT ≥3xULN 5 (1%) 15 (4%)
Total bilirubin >1.5xULN 3 (<1%) 2 (<1%)
Alkaline phosphatase >1.5xULN 1 (<1%) 19 (5%)
ALT and/or AST >3xULN and total bilirubin >1.5xULN 0 0
* 1 primary cause of death unrelated to study drug but complicated by renal failure possibly related to Atripla, and 1 not related to Atripla

10
Appendix 3: Results from the FLAMINGO study10
Study characteristic Dolutegravir + OBR (n=242)
Darunavir/ritonavir + OBR (n=242)
Difference (95% CI)
Primary endpoint: Patients with plasma HIV-1 RNA <50 copies/mL at week 48
Virological success [HIV-1 RNA <50 copies/mL (c/mL)] 217 (90%) 200 (83%) 7.1% (0.9 to 13.2), p=0.025
Secondary endpoints
Virologic non-response 15 (6%) 18 (7%)
Data in window not <50c/mL 6 (2%) 11 (5%)
Discontinued for lack of efficacy 1(<1%) 1 (<1%)
Discontinued for other reasons while HIV-1 RNA not <50c/mL
3 (1%) 5 (2%)
Change in ART 5 (2%) 1 (<1%)
No virological data at week 48 10 (4%) 24 (10%)
Discontinued – adverse event or death 3 (1%) 9 (4%)
Discontinued – other reason 6 (2%) 11 (5%)
Virological response [HIV-1 RNA <50 c/mL] stratified by
Baseline HIV-1 RNA ≤100,000 copies/mL 88% 87%
>100,000 copies/mL 93% 70%
Background dual NRTI therapy
ABC/3TC 90% 85%
TDF/FCT 90% 81%
Treatment-emergent genotypic or phenotypic evidence of integrase inhibitor resistance
Change in CD4 count from baseline (range) cells/mm3
Virological failure 2 (<1%) 2 (<1%)
Treatment-emergent primary mutations (INI,NRTI, PI) 0 0
Adverse events
Discontinuations due to AE / met stopping criteria 4 (2%) 10 (4%)
AEs in ≥10% in any treatment group
Diarrhoea 41 (17%) 70 (29%)
Nausea 39 (16%) 43 (18%)
Headache 37 (15%) 24 (10%)
Serious AEs 11% 5%
Fatal AEs 0 0
Events leading to withdrawal 1% 4%
Maximum post-baseline emergent toxicity grade 3-4
Cholesterol 0 3 (1%)
LDL cholesterol 2 (<1%) 6 (2%)
Alanine aminotransferase 3 (1%) 4 (2%)
Creatine kinase 16 (7%) 9 (4%)
Creatinine 0 0
11
Appendix 4: Results from the SAILING study11
Study characteristic Dolutegravir 50mg OD + OBR (n=354)
Raltegravir 400mg BD + OBR (n=361)
Difference (95% CI)
Primary endpoint: Patients with plasma HIV-1 RNA <50 copies/mL at week 48
Virological success [HIV-1 RNA <50 copies/mL (c/mL)] 251 (71%) 230 (64%) 7.4% (0.7 to 14.2), p=0.03
Secondary endpoints
Virological non-response 71 (20%) 100 (28%)
Data in window not <50c/mL 35 (10%) 48 (13%)
Discontinued for lack of efficacy 19 (5%) 35 (10%)
Discontinued for other reasons while HIV-1 RNA not <50c/mL
7 (2%) 7 (2%)
Change in ART 10 (3%) 10 (3%)
No virological data at week 48 32 (9%) 31 (9%)
Discontinued – adverse event or death 9 (3%) 13 (4%)
Discontinued – other reason 16 (5%) 14 (4%)
Virological response [HIV-1 RNA <50 c/mL] stratified by
Phenotypic susceptibility score
2 181/250 (72%) 169/267 (63%) 9.1% (1.1 to 17.1)
<2 70/104 (67%) 61/94 (65%) 2.4% (-10.8 to 15.6)
Baseline HIV-1 RNA ≤50,000 copies/mL 186/249 (75%) 180/254 (71%) 3.8% (–3.9 to 11.6)
>50,000 copies/mL 65/105 (62%) 50/107 (47%) 15.2% (1.9 to 28.4)
Darunavir-ritonavir No use or use with PI mutations 201/282 (71%) 176/284 (62%) 9.3% (1.6 to 17.0)
Use without PI mutations 50/72 (69%) 54/77 (70%) –0.7% (–15.4 to 14.1)
Treatment-emergent genotypic or phenotypic evidence of integrase inhibitor resistance
4 (1%) 17 (5%) -3.7% (-6.1 to -1.2) p=0.003
Change in CD4 count from baseline (range) cells/mm3 162 ± 151 153 ± 144
Virological failure 21 (6%) 45 (12%)
Adverse events
AEs in ≥5% in any treatment group
Diarrhoea 71 (20%) 64 (18%)
Upper respiratory tract infections 38 (11%) 29 (8%)
Headache 33 (9%) 31 (9%)
Nausea 29 (8%) 29 (8%)
Influenza 24 (7%) 26 (7%)
Nasopharyngitis 23 (6%) 22 (6%)
Urinary tract infection 26 (7%) 18 (5%)
Vomiting 20 (6%) 20 (6%)
Fatigue 15 (4%) 24 (7%)
Rash 19 (5%) 18 (5%)
Arthralgia 10 (3%) 18 (5%)
Upper abdominal pain 17 (5%) 5 (1%)
Any serious AE 33 (9%) 42 (12%)
Serious AEs related to study drug 2 (1%) 4 (1%)
Safety reasons leading to discontinuations 9 (3%) 14 (4%)
Adverse events 4 (1%) 11 (3%)
Met liver chemistry stopping criteria 5 (1%) 3 (1%)
Select grade 3-4 laboratory abnormalities
ALT 9 (3%) 7 (2%)
Cholesterol 6 (2%) 14 (4%)
Creatinine 1 (<1%) 1 (<1%)
Hyperglycaemia 4 (1%) 7 (2%)
Lipase 4 (1%) 7 (2%)
Total bilirubin† 21 (6%) 14 (4%)
Creatinine phosphokinase 7 (2%) 4 (1%)
OBR: Optimised background regimen
† 16/21 patients on dolutegravir and 11/14 on raltegravir were receiving atazanavir

12
Appendix 5a: Results from VIKING-315
Week 24 (n=183) Week 48 (n=114) *
Proportion with HIV-1 RNA <50c/mL over time
HIV-1 RNA <50c/mL 126 (69%) 64 (56%)
Virological non-response 50 (27%) 44 (39%)
No virological data at data cut 7 (4%) 6 (5%)
Discontinued due to AE or death 5 (3%) 5 (4%)
Discontinued due to other reasons 2 (1%) 1 (<1%)
Derived Integrase mutation group
Week 24 response by baseline mutation category and OBR overall susceptibility score (OSS)
No Q148 (Y143, N155, T66, E92 or historical resistance)
OSS=0 4/4 (100)%
OSS=1 35/40 (88%)
OSS≥2 57/70 (81%)
Total 96/114 (84%)
Q148 + 1 (key secondary mutations were G140A/C/S, L741, E138/A/K/T)
OSS=0 2/2 (100%)
OSS=1 8/12 (67%)
OSS≥2 10/17 (59%)
Total 20/31 (65%)
Q148 + ≥2 (key secondary mutations were G140A/C/S, L741, E138/A/K/T)
OSS=0 1/2 (50%)
OSS=1 2/11 (18%)
OSS≥2 1/3 (33%)
Total 4/16 (25%)
Week 24 responses by baseline dolutegravir fold-change category
Total 120/161 (75%)
≤4 98/120 (82%)
>4 to 10 14/25 (56%)
>10 1/9 (11%)
* 114 of the 183 patients enrolled had reached week 48 at the time of data cut-off.
Appendix 5b: Day 8 and week 24 responses by baseline resistance: VIKING-315
Day 8 Mean HIV-1 RNA log10 change from baseline
Week 24 With HIV-1 RNA <50c/mL
Primary integrase inhibitor resistance mutation at baseline
Total (n=183) -1.4 (± 0.61) 69%
No primary mutations (n=60) -1.6 (± 0.55) 78%
T66 (n=1) -1.9 100%
Y143 (n=28) -1.7 (± 0.42) 75%
N155 (n=33) -1.4 (± 0.51) 88%
≥ 2 primary mutations (n=8) -1.4 (± 0.76) 50%
Q148 + 1 secondary mutation (n=32) -1.1 (± 0.51) 59%
Q148 + ≥2 secondary mutations (n=21) -1.0 (± 0.81) 24%
Appendix 5c: Adverse events from VIKING-315
Dolutegravir 50mg BD (n=183)
Drug related (most common ≥5%) 50 (27%)
Nausea 11 (6%)
Diarrhoea 10 (5%)
Headache 9 (5%)
AEs leading to withdrawal 6 (3%)
Serious - any event 31 (17%)
Fatal 1 (<1%) [unrelated to study drug]
Serious drug-related 2 (1%) [hyperbilirubinaemia + elevated ALT + drug eruption; grade 2 syncope]